Residential Racial Composition and Black-White Obesity Risks: Differential Effects of Neighborhood Social and Built Environment


Abstract
:
1. Introduction
2. Methods
2.1. Data
2.2. Individual-Level Measures
2.3. Neighborhood-Level Measures
2.4. Statistical Analysis

{kind=link}
{kind=link}
{kind=link}
| White Women | White Men | Black Women | Black Men | |
|---|---|---|---|---|
| Individual-level Measures | ||||
| Obese | 20.74% | 24.06% | 40.79% | 31.27% |
| Age | 54.57 (0.18) | 53.65 (0.24) | 49.28 (0.30) | 50.52 (0.48) |
| Married/living with partner | 58.74% | 66.78% | 30.33% | 45.27% |
| US born | 96.40% | 96.12% | 95.07% | 92.35% |
| Educational attainment | ||||
| High school or below | 37.10% | 31.36% | 52.50% | 54.90% |
| Some college | 19.97% | 18.75% | 24.73% | 22.51% |
| College or above | 42.94% | 49.89% | 22.78% | 22.59% |
| Income | ||||
| <100% FPL | 4.54% | 3.04% | 20.03% | 13.14% |
| 100%–200% FPL | 13.33% | 9.61% | 27.29% | 24.91% |
| ≥200% FPL | 82.14% | 87.35% | 52.69% | 61.94% |
| Current smoker | 18.21% | 18.66% | 25.56% | 28.18% |
| Survey year 2008 | 50.78% | 49.51% | 51.89% | 55.24% |
| Sample Size (N) | 8,224 | 4,506 | 3,126 | 1,164 |
| Neighborhood-level Measures | ||||
| Percent black ≥ 25% | 20.75% | 19.05% | 46.29% | 55.28% |
| Social cohesion | 0.06 (0.01) | 0.06 (0.01) | −0.15 (0.02) | −0.18 (0.02) |
| Socioeconomic status | 0.15 (0.03) | 0.20 (0.03) | −0.37 (0.04) | −0.52 (0.05) |
| Street connectivity | 166.51 (4.96) | 163.03 (5.06) | 227.00 (6.59) | 243.40 (7.63) |
| Park accessibility | 1.59 (0.04) | 1.62 (0.04) | 1.16 (0.04) | 1.10 (0.04) |
| Residential stability | 0.58 (0.00) | 0.58 (0.00) | 0.57 (0.01) | 0.57 (0.01) |
| Number of Tracts | 853 | 819 | 553 | 407 |
3. Results
3.1. Descriptive Statistics
| (1) | (2) | (3) | (4) | (5) | |
|---|---|---|---|---|---|
| (1) Percent black ≥ 25% | 1.000 | ||||
| (2) Social cohesion | −0.512 | 1.000 | |||
| (3) Socioeconomic status | −0.635 | 0.657 | 1.000 | ||
| (4) Street connectivity | 0.400 | −0.439 | −0.565 | 1.000 | |
| (5) Park accessibility | −0.365 | 0.376 | 0.404 | −0.495 | 1.000 |
| (6) Residential stability | −0.045 | 0.128 | 0.002 | −0.130 | 0.059 |
3.2. Multivariate Regression Analysis
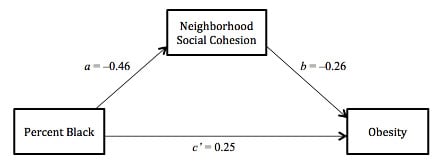
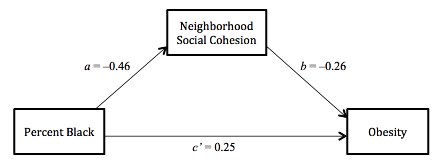
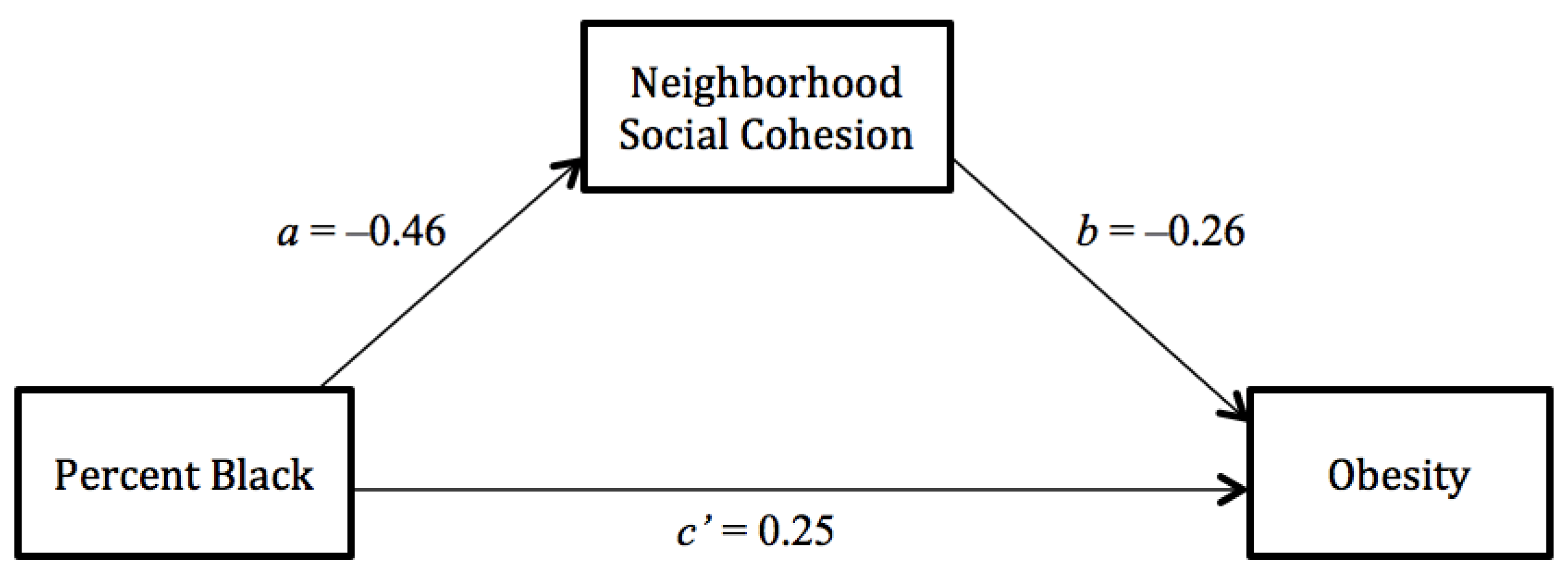
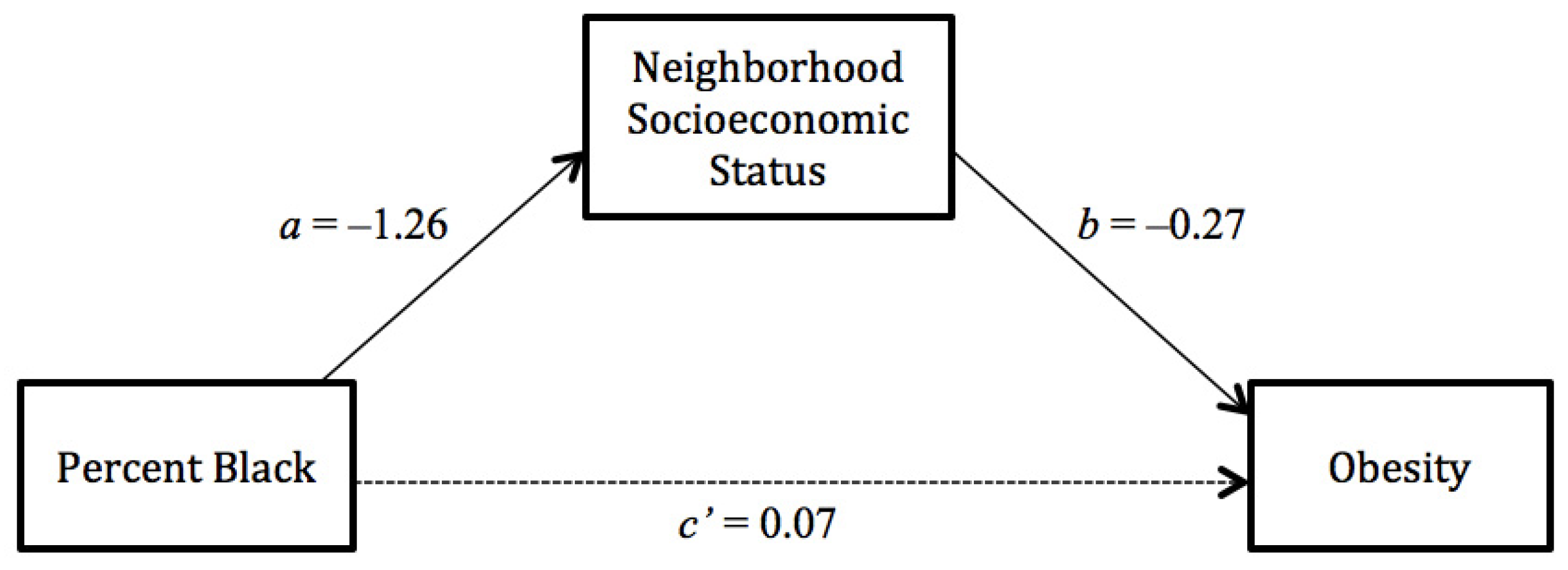
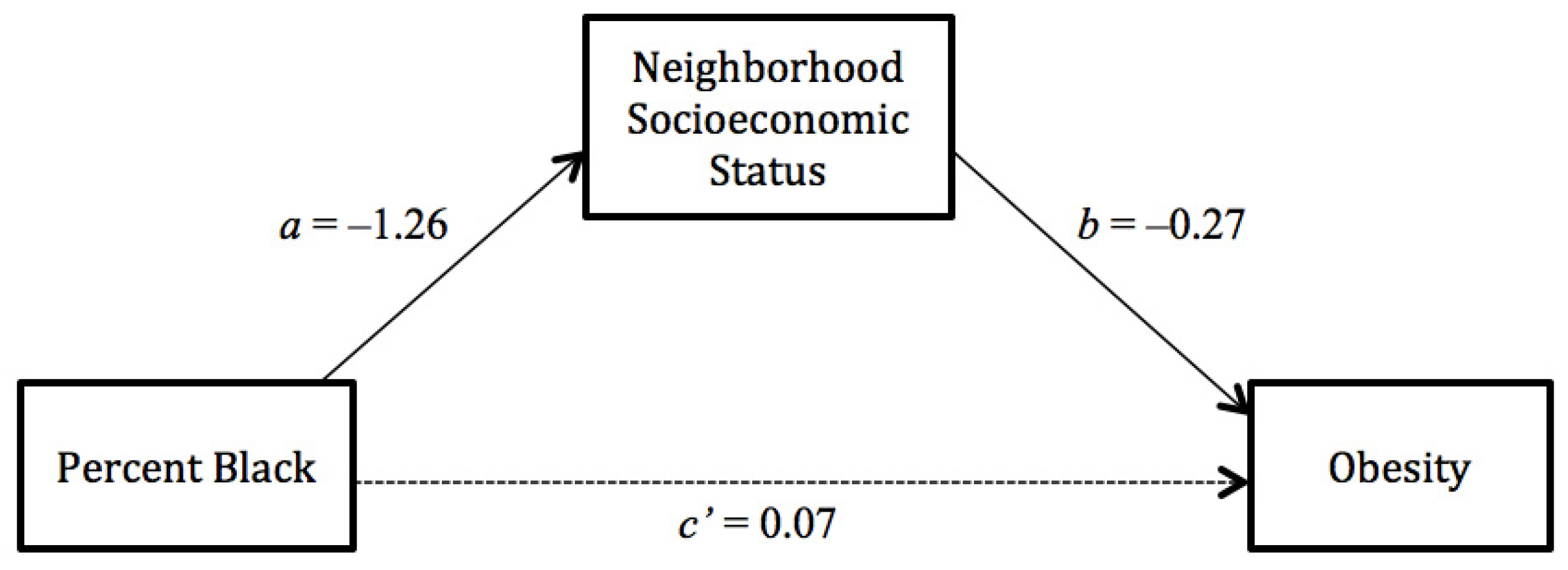
3.3. Mediation Analysis
| White Women (N = 8,224) | White Men (N = 4,506) | |||||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | Model 1 | Model 2 | Model 3 | Model 4 | |
| Neighborhood-level Measures | ||||||||
| Percent black ≥ 25% | 1.43 *** | 1.28 * | 1.09 | 1.09 | 0.89 | 0.74 + | 0.64 * | 0.65 * |
| [1.17–1.75] | [1.02–1.60] | [0.86–1.36] | [0.87–1.38] | [0.66–1.20] | [0.53–1.03] | [0.45–0.92] | [0.46–0.93] | |
| Social cohesion | 0.77 * | 1.11 | 1.08 | 0.67 ** | 0.93 | 0.89 | ||
| [0.62–0.97] | [0.86–1.44] | [0.83–1.41] | [0.50–0.89] | [0.66–1.29] | [0.63–1.24] | |||
| Socioeconomic status | 0.74 *** | 0.72 *** | 0.75 *** | 0.69 *** | ||||
| [0.66–0.83] | [0.64–0.81] | [0.64–0.88] | [0.58–0.81] | |||||
| Street connectivity | 1.00 | 0.99 ** | ||||||
| [1.00–1.00] | [0.99–1.00] | |||||||
| Park accessibility | 1.02 | 0.99 | ||||||
| [0.96–1.09] | [0.91–1.08] | |||||||
| Residential stability | 1.33 | 1.48 | 1.18 | 1.12 | 1.90 | 2.25 + | 1.83 | 1.41 |
| [0.64–2.75] | [0.71–3.1] | [0.57–2.40] | [0.53–2.33] | [0.76–4.77] | [0.88–5.73] | [0.72–4.67] | [0.54–3.66] | |
| Individual-level Measures | ||||||||
| Age | 1.11 *** | 1.11 *** | 1.11 *** | 1.11 *** | 1.14 *** | 1.14 *** | 1.14 *** | 1.14 *** |
| [1.08–1.14] | [1.08–1.14] | [1.08–1.14] | [1.08–1.14] | [1.10–1.18] | [1.10–1.18] | [1.10–1.18] | [1.10–1.18] | |
| Ages quared | 1.00 *** | 1.00 *** | 1.00 *** | 1.00 *** | 1.00 *** | 1.00 *** | 1.00 *** | 1.00 *** |
| [1.00–1.00] | [1.00– 1.00] | [1.00–1.00] | [1.00–1.00] | [1.00–1.00] | [1.00–1.00] | [1.00–1.00] | [1.00–1.00] | |
| Married | 0.69 *** | 0.70 *** | 0.71 *** | 0.70 *** | 1.03 | 0.97 | 0.99 | 0.98 |
| [0.60–0.79] | [0.60–0.80] | [0.61–0.81] | [0.61–0.81] | [0.92–1.16] | [0.80–1.17] | [0.82–1.20] | [0.81–1.18] | |
| US born | 1.72 ** | 1.73 ** | 1.71 ** | 1.71 ** | 1.10 | 1.11 | 1.12 | 1.13 |
| [1.20–2.48] | [1.20–2.50] | [1.19–2.48] | [1.18–2.47] | [0.72–1.68] | [0.73–1.70] | [0.73–1.72] | [0.74–1.72] | |
| Education a | 0.73 *** | 0.74 *** | 0.77 *** | 0.77 *** | 0.79 *** | 0.80 *** | 0.83 *** | 0.84 *** |
| [0.67–0.79] | [0.68– 0.80] | [0.70–0.83] | [0.70–0.84] | [0.72–0.87] | [0.73–0.88] | [0.75–0.92] | [0.76–0.92] | |
| Income b | 0.77 *** | 0.78 *** | 0.80 ** | 0.80 ** | 0.90 | 0.92 | 0.95 | 0.93 |
| [0.68–0.87] | [0.69–0.89] | [0.70–0.91] | [0.70–0.91] | [0.75–1.07] | [0.77–1.10] | [0.79–1.13] | [0.78–1.12] | |
| Individual-level Measures | ||||||||
| Current smoker | 0.69 *** | 0.68 *** | 0.68 *** | 0.68 *** | 0.73 ** | 0.72 ** | 0.71 ** | 0.71 ** |
| [0.57–0.83] | [0.57–0.82] | [0.56–0.82] | [0.56–0.82] | [0.58–0.91] | [0.58–0.91] | [0.57–0.89] | [0.57–0.89] | |
| Year 2008 | 1.00 | 1.00 | 0.99 | 0.99 | 1.19 * | 1.18 * | 1.18 * | 1.18 * |
| [0.88–1.13] | [0.88–1.13] | [0.87–1.12] | [0.87–1.12] | [1.01–1.39] | [1.00–1.38] | [1.01–1.39] | [1.00–1.38] | |
| Level 2 variance | 0.20 *** | 0.20 *** | 0.17 *** | 0.17 *** | 0.35 *** | 0.33 *** | 0.30 *** | 0.28 *** |
| Intraclass correlation | 0.06 | 0.06 | 0.05 | 0.05 | 0.11 | 0.10 | 0.09 | 0.08 |
| AIC | 7,881.35 | 7,877.96 | 7,855.43 | 7,857.40 | 4,828.89 | 4,822.07 | 4,810.86 | 4,804.41 |
| BIC | 7,965.53 | 7,969.15 | 7,953.64 | 7,969.64 | 4,905.85 | 4,905.44 | 4,900.65 | 4,907.02 |
| Black Women ( N = 3,126) | Black Men ( N = 1,164) | |||||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | Model 1 | Model 2 | Model 3 | Model 4 | |
| Neighborhood-level Measures | ||||||||
| Percent black ≥ 25% | 1.10 | 1.03 | 0.95 | 0.93 | 0.90 | 0.87 | 0.87 | 0.95 |
| [0.89–1.37] | [0.76–1.29] | [0.74–1.22] | [0.72–1.20] | [0.64–1.27] | [0.60–1.25] | [0.59–1.28] | [0.63–1.43] | |
| Social cohesion | 0.77 + | 0.92 | 0.93 | 0.92 | 0.91 | 0.87 | ||
| [0.59–1.00] | [0.66–1.27] | [0.67–1.29] | [0.60–1.41] | [0.53–1.56] | [0.51–1.50] | |||
| Socioeconomic status | 0.88 + | 0.90 | 1.01 | 1.01 | ||||
| [0.76–1.01] | [0.77–1.05] | [0.79–1.28] | [0.78–1.29] | |||||
| Street connectivity | 1.00 | 1.00 | ||||||
| [1.00–1.00] | [1.00–1.00] | |||||||
| Park accessibility | 0.93 | 1.21 | ||||||
| [0.77–1.13] | [0.95–1.56] | |||||||
| Residential stability | 0.47 + | 0.53 | 0.44 + | 0.45 + | 1.42 | 1.51 | 1.53 | 1.32 |
| [0.20–1.10] | [0.23–1.24] | [0.18–1.08] | [0.19–1.16] | [0.37–5.44] | [0.40–5.72] | [0.41–5.77] | [0.35–5.00] | |
| Individual-level Measures | ||||||||
| Age | 1.14 *** | 1.14 *** | 1.14 *** | 1.14 *** | 1.17 *** | 1.17 *** | 1.17 *** | 1.17 *** |
| [1.10–1.17] | [1.10–1.17] | [1.10–1.17] | [1.10–1.17] | [1.11–1.24] | [1.11–1.24] | [1.11–1.24] | [1.11–1.24] | |
| Age squared | 1.00 *** | 1.00 *** | 1.00 *** | 1.00 *** | 1.00 *** | 1.00 *** | 1.00 *** | 1.00 *** |
| [1.00–1.00] | [1.00–1.00] | [1.00–1.00] | [1.00–1.00] | [1.00–1.00] | [1.00–1.00] | [1.00–1.00] | [1.00–1.00] | |
| Married | 0.79 * | 0.79 * | 0.79 * | 0.80 * | 0.90 | 1.07 | 1.07 | 1.08 |
| [0.66–0.96] | [0.66–0.96] | [0.66–0.96] | [0.66–0.97] | [0.75–1.08] | [0.79–1.46] | [0.78–1.46] | [0.79–1.47] | |
| US born | 1.86 ** | 1.84 ** | 1.82 ** | 1.81 ** | 2.52 ** | 2.47 ** | 2.48 ** | 2.48 ** |
| [1.25–2.76] | [1.24–2.74] | [1.22–2.71] | [1.21–2.69] | [1.30–4.89] | [1.28–4.78] | [1.28–4.80] | [1.28–4.78] | |
| Education a | 0.78 *** | 0.79 *** | 0.80 *** | 0.80 *** | 0.85 + | 0.86 + | 0.86 + | 0.86 + |
| [0.69–0.87] | [0.71–0.88] | [0.71–0.89] | [0.71–0.90] | [0.71–1.02] | [0.72–1.03] | [0.71–1.03] | [0.72–1.03] | |
| Income b | 0.80 *** | 0.81 *** | 0.81 ** | 0.81 ** | 1.22 + | 1.24 + | 1.24 + | 1.23 + |
| [0.71–0.90] | [0.71–0.91] | [0.72–0.91] | [0.72–0.92] | [0.97–1.53] | [0.99–1.55] | [0.99–1.56] | [0.99–1.55] | |
| Current smoker | 0.67 *** | 0.67 *** | 0.67 *** | 0.66 *** | 0.55 ** | 0.55 *** | 0.55 ** | 0.55 ** |
| [0.55–0.82] | [0.55–0.82] | [0.55–0.81] | [0.54–0.81] | [0.39–0.77] | [0.39–0.77] | [0.39–0.77] | [0.39–0.78] | |
| Year 2008 | 0.91 | 0.91 | 0.92 | 0.92 | 1.02 | 1.03 | 1.03 | 1.01 |
| [0.77–1.08] | [0.77–1.09] | [0.77–1.09] | [0.77–1.09] | [0.76–1.37] | [0.77–1.38] | [0.77–1.38] | [0.76–1.36] | |
| Level 2 variance | 0.17 *** | 0.17 ** | 0.18 ** | 0.17 ** | 0.22 | 0.22 | 0.22 | 0.19 |
| Intraclass correlation | 0.05 | 0.05 | 0.05 | 0.05 | 0.07 | 0.07 | 0.07 | 0.06 |
| AIC | 4,042.83 | 4,041.40 | 4,039.42 | 4,042.17 | 1,376.37 | 1,378.25 | 1,380.25 | 1,381.66 |
| BIC | 4,115.40 | 4,120.02 | 4,124.08 | 4,138.93 | 1,437.09 | 1,444.02 | 1,451.08 | 1,462.62 |

4. Discussion
5. Conclusions
Acknowledgments
Conflicts of Interest
References
- Mokdad, A.H. Prevalence of obesity, diabetes, and obesity-related health risk factors, 2001. JAMA 2003, 289, 76–79. [Google Scholar] [CrossRef]
- Ogden, C.L.; Carroll, M.D.; Curtin, L.R.; McDowell, M.A.; Tabak, C.J.; Flegal, K.M. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA 2006, 295, 1549–1555. [Google Scholar] [CrossRef]
- Griffith, D.M.; Johnson-Lawrence, V.; Gunter, K.; Neighbors, H.W. Race, SES, and obesity among men. Race Soc. Probl. 2011, 3, 298–306. [Google Scholar] [CrossRef]
- Bleich, S.N.; Thorpe, R.J.; Sharif-Harris, H.; Fesahazion, R.; Laveist, T.A. Social context explains race disparities in obesity among women. J. Epidemiol. Community Health 2010, 64, 465–469. [Google Scholar] [CrossRef]
- Wen, M.; Kowaleski-Jones, L. The built environment and risk of obesity in the United States: Racial-ethnic disparities. Health Place 2012, 18, 1314–1322. [Google Scholar] [CrossRef]
- Wen, M.; Maloney, T.N. Latino residential isolation and the risk of obesity in Utah: The role of neighborhood socioeconomic, built-environmental, and subcultural context. J. Immigr. Minor. Heal. 2011, 13, 1134–1141. [Google Scholar] [CrossRef]
- Williams, D.R.; Collins, C. Racial residential segregation: A fundamental cause of racial disparities in health. Public Health Rep. 2001, 116, 404–416. [Google Scholar]
- Bécares, L.; Shaw, R.; Nazroo, J.; Stafford, M.; Albor, C.; Atkin, K.; Kiernan, K.; Wilkinson, R.; Pickett, K. Ethnic density effects on physical morbidity, mortality, and health behaviors: A systematic review of the literature. Am. J. Public Health 2012, 102, e33–e66. [Google Scholar]
- Pickett, K.E.; Wilkinson, R.G. People like us: Ethnic group density effects on health. Ethn. Health 2008, 13, 321–334. [Google Scholar] [CrossRef]
- Kramer, M.R.; Hogue, C.R. Is segregation bad for your health? Epidemiol. Rev. 2009, 31, 178–194. [Google Scholar] [CrossRef]
- Boardman, J.D.; Saint Onge, J.M.; Rogers, R.G.; Denney, J.T. Race differentials in obesity: The impact of place. J. Health Soc. Behav. 2005, 46, 229–243. [Google Scholar] [CrossRef]
- Chang, V.W.; Hillier, A.E.; Mehta, N.K. Neighborhood racial isolation, disorder and obesity. Soc. Forces 2009, 87, 2063–2092. [Google Scholar] [CrossRef]
- Black, J.L.; Macinko, J.; Dixon, L.B.; Fryer, G.E. Neighborhoods and obesity in New York City. Health Place 2010, 16, 489–499. [Google Scholar] [CrossRef]
- Kirby, J.B.; Liang, L.; Chen, H.-J.; Wang, Y. Race, place, and obesity: The complex relationships among community racial/ethnic composition, individual race/ethnicity, and obesity in the United States. Am. J. Public Health 2012, 102, 1572–1578. [Google Scholar] [CrossRef]
- Robert, S.A.; Reither, E.N. A multilevel analysis of race, community disadvantage, and body mass index among adults in the US. Soc. Sci. Med. 2004, 59, 2421–2434. [Google Scholar] [CrossRef]
- Do, D.P.; Dubowitz, T.; Bird, C.E.; Lurie, N.; Escarce, J.J.; Finch, B.K. Neighborhood context and ethnicity differences in body mass index: A multilevel analysis using the NHANES III survey (1988–1994). Econ. Hum. Biol. 2007, 5, 179–203. [Google Scholar] [CrossRef]
- Social Capital and Health; Kawachi, I.; Subramanian, S.V.; Kim, D. (Eds.) Springer: New York, NY, USA, 2008.
- Alba, R.D.; Logan, J.R.; Stults, B.J. The changing neighborhood contexts of the immigrant metropolis. Soc. Forces 2000, 79, 587–621. [Google Scholar]
- Wen, M.; Christakis, N.A. Neighborhood effects on posthospitalization mortality: A population-based cohort study of the elderly in Chicago. Health Serv. Res. 2005, 40, 1108–1127. [Google Scholar] [CrossRef]
- Becares, L.; Stafford, M.; Laurence, J.; Nazroo, J. Composition, concentration and deprivation: Exploring their association with social cohesion among different ethnic groups in the UK. Urban Stud. 2011, 48, 2771–2787. [Google Scholar] [CrossRef]
- Hutchinson, R.N.; Putt, M.A.; Dean, L.T.; Long, J.A; Montagnet, C.A.; Armstrong, K. Neighborhood racial composition, social capital and black all-cause mortality in Philadelphia. Soc. Sci. Med. 2009, 68, 1859–1865. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Perceptions of neighborhood characteristics and leisure-time physical inactivity—Austin/Travis County, Texas, 2004. Morb. Mortal. Wkly. Rep. 2005, 54, 926–928. [Google Scholar]
- Feng, J.; Glass, T.A.; Curriero, F.C.; Stewart, W.F.; Schwartz, B.S. The built environment and obesity: A systematic review of the epidemiologic evidence. Health Place 2010, 16, 175–190. [Google Scholar] [CrossRef]
- Lovasi, G.S.; Neckerman, K.M.; Quinn, J.W.; Weiss, C.C.; Rundle, A. Effect of individual or neighborhood disadvantage on the association between neighborhood walkability and body mass index. Am. J. Public Health 2009, 99, 279–284. [Google Scholar]
- Wen, M.; Zhang, X.; Harris, C.D.; Holt, J.B.; Croft, J.B. Spatial disparities in the distribution of parks and green spaces in the USA. Ann. Behav. Med. 2013, 45 (Suppl. 1), S18–S27. [Google Scholar] [CrossRef]
- Duncan, D.T.; Kawachi, I.; White, K.; Williams, D.R. The geography of recreational open space: Influence of neighborhood racial composition and neighborhood poverty. J. Urban Heal. 2013, 90, 618–631. [Google Scholar]
- Wen, M.; Zhang, X. Contextual effects of built and social environments of urban neighborhoods on exercise: A multilevel study in Chicago. Am. J. Health Promot. 2009, 23, 247–254. [Google Scholar] [CrossRef]
- Kershaw, K.N.; Albrecht, S.S.; Carnethon, M.R. Racial and ethnic residential segregation, the neighborhood socioeconomic environment, and obesity among blacks and Mexican Americans. Am. J. Epidemiol. 2013, 177, 299–309. [Google Scholar] [CrossRef]
- Wen, M.; Lauderdale, D.S.; Kandula, N.R. Ethnic neighborhoods in multi-ethnic America, 1990–2000: Resurgent ethnicity in the ethnoburbs? Soc. Forces 2009, 88, 425–460. [Google Scholar] [CrossRef]
- Borrell, L.N.; Kiefe, C.I.; Diez-Roux, A.V.; Williams, D.R.; Gordon-Larsen, P. Racial discrimination, racial/ethnic segregation, and health behaviors in the CARDIA study. Ethn. Health 2013, 18, 227–243. [Google Scholar] [CrossRef]
- Salinas, J.J.; Rocha, E.; Abdelbary, B.E.; Gay, J.; Sexton, K. Impact of Hispanic ethnic concentration and socioeconomic status on obesity prevalence in Texas counties. Int. J. Environ. Res. Public Health 2012, 9, 1201–1215. [Google Scholar]
- White, K.; Borrell, L.N. Racial/ethnic residential segregation: Framing the context of health risk and health disparities. Health Place 2011, 17, 438–448. [Google Scholar] [CrossRef]
- Roy, A.L.; Hughes, D.; Yoshikawa, H. Exploring neighborhood effects on health and life satisfaction: Disentangling neighborhood racial density and neighborhood income. Race Soc. Probl. 2012, 4, 193–204. [Google Scholar] [CrossRef]
- Wang, F.; Wen, M.; Xu, Y. Population-adjusted street connectivity, urbanicity and risk of obesity in the U.S. Appl. Geogr. 2013, 41, 1–14. [Google Scholar] [CrossRef]
- Zhang, X.; Lu, H.; Holt, J.B. Modeling spatial accessibility to parks: A national study. Int. J. Health Geogr. 2011, 10, 31. [Google Scholar] [CrossRef]
- Krull, J.L.; MacKinnon, D.P. Multilevel modeling of individual and group level mediated effects. Multivar. Behav. Res. 2001, 36, 249–277. [Google Scholar] [CrossRef]
- Jones, A. Segregation and cardiovascular illness: The role of individual and metropolitan socioeconomic status. Health Place 2013, 22, 56–67. [Google Scholar] [CrossRef]
- Warner, E.T.; Gomez, S.L. Impact of neighborhood racial composition and metropolitan residential segregation on disparities in breast cancer stage at diagnosis and survival between black and white women in California. J. Community Health 2010, 35, 398–408. [Google Scholar] [CrossRef]
- Prince, S.A.; Kristjansson, E.A.; Russell, K.; Billette, J.-M.; Sawada, M.; Ali, A.; Tremblay, M.S.; Prud’homme, D. A multilevel analysis of neighbourhood built and social environments and adult self-reported physical activity and body mass index in Ottawa, Canada. Int. J. Environ. Res. Public Health 2011, 8, 3953–3978. [Google Scholar] [CrossRef]
- Rios, R.; Aiken, L.S.; Zautra, A.J. Neighborhood contexts and the mediating role of neighborhood social cohesion on health and psychological distress among Hispanic and non-Hispanic residents. Ann. Behav. Med. 2012, 43, 50–61. [Google Scholar] [CrossRef]
- Singh, G.K.; Kogan, M.D.; Siahpush, M.; van Dyck, P.C. Independent and joint effects of socioeconomic, behavioral, and neighborhood characteristics on physical inactivity and activity levels among US children and adolescents. J. Community Health 2008, 33, 206–216. [Google Scholar] [CrossRef]
- Li, K.; Wen, M. Racial and ethnic disparities in leisure-time physical activity in California: Patterns and mechanisms. Race Soc. Probl. 2013, 5, 147–156. [Google Scholar] [CrossRef]
- Ross, C.E. Walking, exercising, and smoking: Does neighborhood matter? Soc. Sci. Med. 2000, 51, 265–274. [Google Scholar] [CrossRef]
- Weiss, C.C.; Purciel, M.; Bader, M.; Quinn, J.W.; Lovasi, G.; Neckerman, K.M.; Rundle, A.G. Reconsidering access: Park facilities and neighborhood disamenities in New York City. J. Urban Health 2011, 88, 297–310. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Li, K.; Wen, M.; Henry, K.A. Residential Racial Composition and Black-White Obesity Risks: Differential Effects of Neighborhood Social and Built Environment. Int. J. Environ. Res. Public Health 2014, 11, 626-642. https://doi.org/10.3390/ijerph110100626
Li K, Wen M, Henry KA. Residential Racial Composition and Black-White Obesity Risks: Differential Effects of Neighborhood Social and Built Environment. International Journal of Environmental Research and Public Health. 2014; 11(1):626-642. https://doi.org/10.3390/ijerph110100626
Chicago/Turabian StyleLi, Kelin, Ming Wen, and Kevin A. Henry. 2014. "Residential Racial Composition and Black-White Obesity Risks: Differential Effects of Neighborhood Social and Built Environment" International Journal of Environmental Research and Public Health 11, no. 1: 626-642. https://doi.org/10.3390/ijerph110100626