Overweight and Obesity in Portuguese Children: Prevalence and Correlates

 , and
, and
Abstract
:1. Introduction
2. Methods
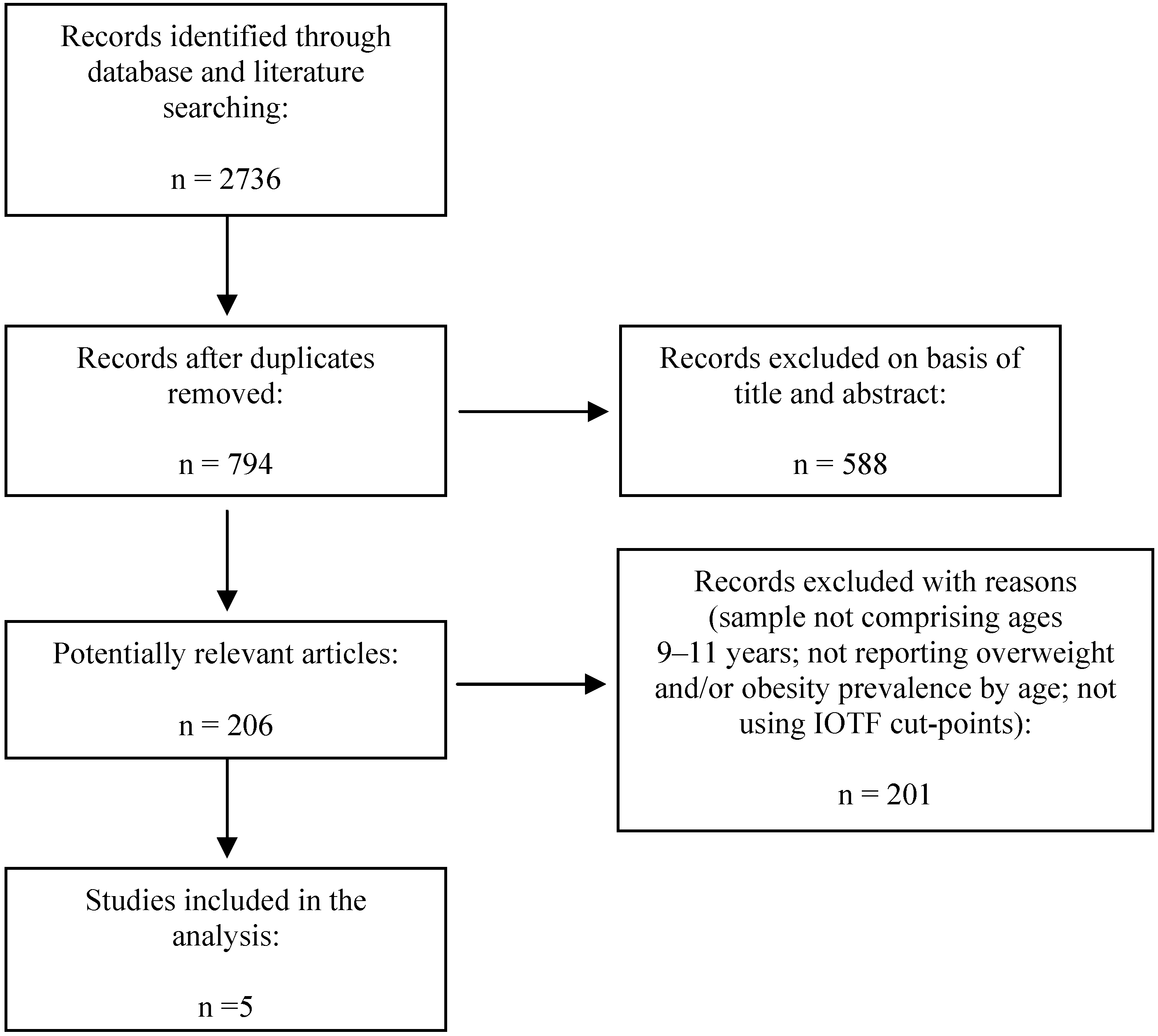
2.1. Part I: Meta-Analysis of Obesity Prevalence among Portuguese Children
2.2. Part II: Correlates of Childhood Overweight and Obesity
2.2.1. Sample
2.2.2. Anthropometry
2.2.3. Family Data
2.2.4. Biological Maturity
2.2.5. Nutritional and Behavioural Habits
2.2.6. Physical Activity, Sedentary Time and Sleep
2.2.7. School Environment
2.2.8. Statistical Analysis
3. Results
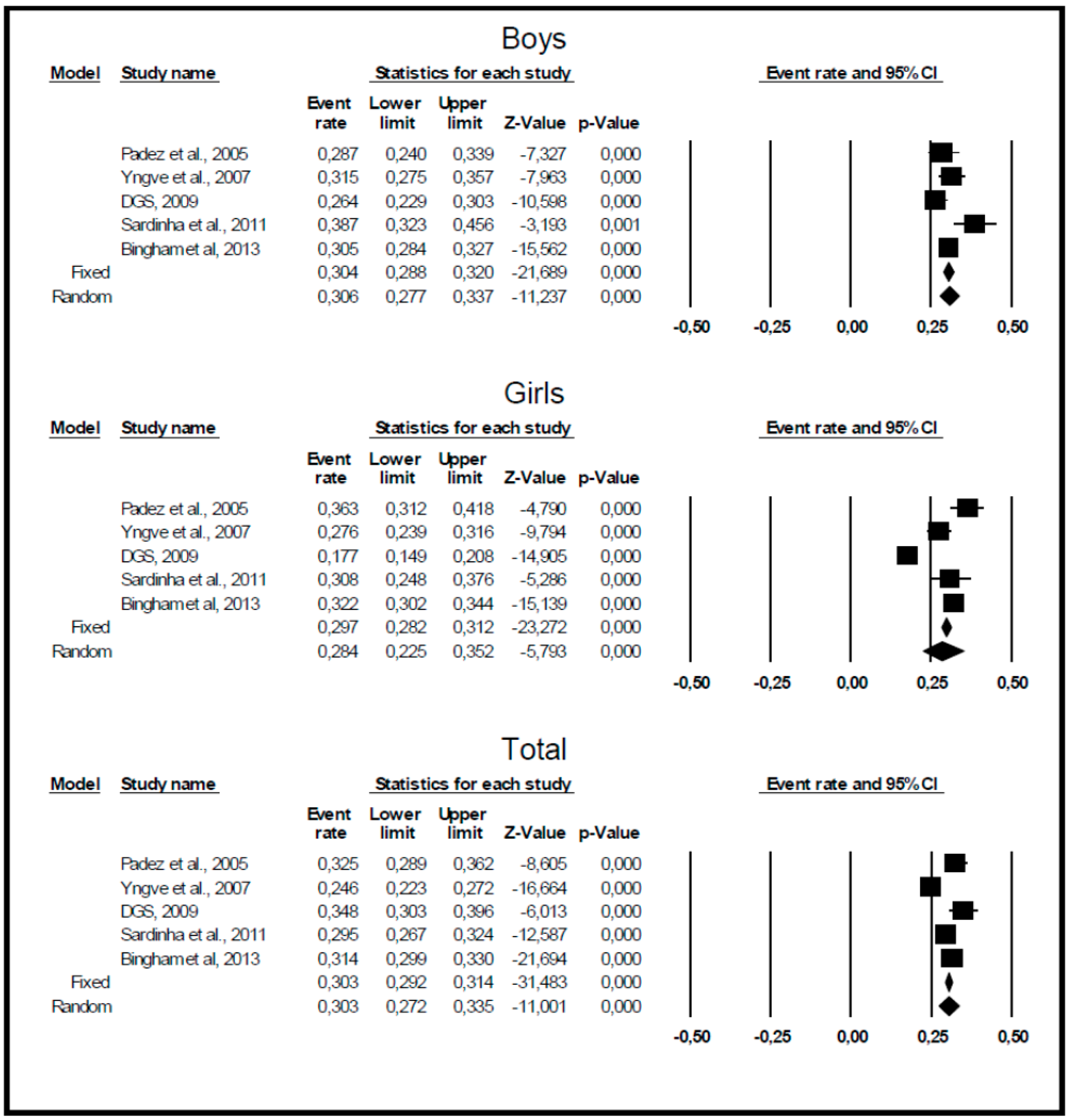
3.1. Prevalence of Overweight/Obesity among 9–11 Year-Old Portuguese Children


{kind=link}
{kind=link}
| Study | Study Year | Age Range | Sample Size | Prevalence of Overweight/Obesity | ||
|---|---|---|---|---|---|---|
| Boys | Girls | Total | ||||
| Padez et al. [38] | 2002/2003 | 9.5 years | 631 (317 boys; 314 girls) | 29% | 36% | 33% |
| Yngve et al. [36] | 2003 | 11 years | 1197 (552 boys; 645 girls) | 27% | 18% | 22% |
| DGS [16] | 2008 | 11 years | 405 (204 boys; 201 girls) | 39% | 31% | 35% |
| Sardinha [37] | 2008 | 10 years | 1001 (486 boys; 515 girls) | 32% | 28% | 19% |
| Bingham et al. [3] | 2009/2010 | 9–10 years | 3584 (1685 boys; 1899 girls) | 31% | 32% | 31% |

3.2. Biological, Behavioural and Socio-Demographic Differences between Normal-Weight and Overweight/Obese Children
| Normal-Weight (n = 417) | Overweight/Obese (n = 269) | t | p-Value | |
|---|---|---|---|---|
| Height (cm) | 141.57 ± 6.39 | 145.73 ± 6.55 | −8.403 | <0.001 |
| Weight (kg) | 34.14 ± 4.59 | 47.79 ± 7.74 | −28.584 | <0.001 |
| Biological maturity | −2.07 ± 0.85 | −1.69 ± 0.90 | −5.639 | <0.001 |
| Unhealthy diet (z-scores) | 0.005 ± 1.00 | −0.10 ± 0.91 | 1.424 | 0.155 |
| Healthy diet (z-scores) | 0.04 ± 0.98 | −0.03 ± 1.03 | 0.945 | 0.345 |
| MVPA (min) | 57.34 ± 22.48 | 55.20 ± 20.54 | 1.291 | 0.197 |
| Sedentary time (min) | 553.26 ± 61.92 | 549.68 ± 61.90 | 0.754 | 0.451 |
| Sleep time (h) | 8.26 ± 0.83 | 8.26 ± 0.90 | -0.027 | 0.979 |
| Frequencies (%) | χ2 | p-Value | ||
| SES | 0.119 | 0.730 | ||
| <€23,999 | 78.4 | 79.6 | ||
| ≥€24,000 | 21.6 | 20.4 | ||
| Mother BMI | 11.744 | 0.001 | ||
| Normal-weight | 66.3 | 52.6 | ||
| Overweight/obese | 33.7 | 47.4 | ||
| Father BMI | 4.898 | 0.027 | ||
| Normal-weight | 41.3 | 32.2 | ||
| Overweight/obese | 58.7 | 67.8 | ||
| Transport to/from school | 0.339 | 0.561 | ||
| Active | 28.8 | 26.8 | ||
| Non-active | 71.2 | 73.2 | ||
| TV bedroom | 3.564 | 0.059 | ||
| No | 33.1 | 26.4 | ||
| Yes | 66.9 | 73.6 | ||
| TV/school day | 0.743 | 0.389 | ||
| <2 h | 73.7 | 70.7 | ||
| ≥2 h | 26.3 | 29.3 | ||
3.3. Individual- and School-Level Correlates of BMI Variation
| Parameters | Model 0 | Model 1 | Model 2 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | SE | p-value | Β | SE | p-value | β | SE | p-value | |
| Intercept | 19.46 | 0.17 | <0.001 | 23.81 | 0.41 | <0.001 | 22.77 | 0.89 | <0.001 |
| Sex | 6.22 | 0.35 | <0.001 | 6.23 | 0.45 | <0.001 | |||
| Biological maturity | 3.94 | 0.20 | <0.001 | 3.96 | 0.24 | <0.001 | |||
| Mother BMI | 0.15 | 0.02 | <0.001 | 0.15 | 0.03 | <0.001 | |||
| Father BMI | 0.12 | 0.03 | <0.001 | 0.12 | 0.03 | <0.001 | |||
| TV weekdays | 0.13 | 0.26 | 0.622 | 0.16 | 0.25 | 0.540 | |||
| TV in bedroom | 0.34 | 0.25 | 0.164 | 0.32 | 0.25 | 0.205 | |||
| Unhealthy diet | −0.20 | 0.13 | 0.142 | −0.20 | 0.12 | 0.098 | |||
| Healthy diet | −0.24 | 0.10 | 0.018 | −0.27 | 0.12 | 0.020 | |||
| MVPA | −0.02 | 0.00 | <0.001 | −0.02 | 0.01 | 0.002 | |||
| Sleep time | −0.19 | 0.12 | 0.102 | −0.18 | 0.14 | 0.178 | |||
| Sports/PA clubs | 0.01 | 0.12 | 0.966 | ||||||
| Incentive for active transportation (bike) | 0.56 | 0.40 | 0.179 | ||||||
| Playground access during school hours | 0.24 | 0.67 | 0.722 | ||||||
| Access to cafeteria | 0.64 | 0.91 | 0.491 | ||||||
| Access to fast food outside school | 0.13 | 0.30 | 0.680 | ||||||
| Access to sports equipment outside school hours | 0.11 | 0.29 | 0.708 | ||||||
| Model summary | |||||||||
| Deviance statistic | 3621.93 | 2332.03 | 2323.03 | ||||||
| Number of estimated parameters | 3 | 13 | 19 | ||||||
4. Discussion
4.1. Prevalence of Overweight/Obesity in 9–11 Year-Old Portuguese Children
4.2. Biological, Behavioural and Socio-Demographic Differences between Normal-Weight and Overweight/Obese Children
4.3. Individual- and School-Level Correlates of BMI Variation
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- De Onis, M.; Blossner, M.; Borghi, E. Global prevalence and trends of overweight and obesity among preschool children. Am. J. Clin. Nutr. 2010, 92, 1257–1264. [Google Scholar] [PubMed]
- Lobstein, T.; Baur, L.; Uauy, R. Obesity in children and young people: A crisis in public health. Obes Rev. 2004, 5, 4–104. [Google Scholar] [CrossRef] [PubMed]
- Bingham, D.D.; Varela-Silva, M.I.; Ferrao, M.M.; Augusta, G.; Mourao, M.I.; Nogueira, H.; Marques, V.R.; Padez, C. Socio-demographic and behavioral risk factors associated with the high prevalence of overweight and obesity in portuguese children. Am. J. Hum. Biol 2013, 25, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Suarez, C.; Worley, A.; Grimmer-Somers, K.; Dones, V. School-based interventions on childhood obesity: A meta-analysis. Am. J. Prev. Med. 2009, 37, 418–427. [Google Scholar] [CrossRef] [PubMed]
- Lavelle, H.V.; Mackay, D.F.; Pell, J.P. Systematic review and meta-analysis of school-based interventions to reduce body mass index. J. Public Health 2012, 34, 360–369. [Google Scholar] [CrossRef]
- Harris, K.C.; Kuramoto, L.K.; Schulzer, M.; Retallack, J.E. Effect of school-based physical activity interventions on body mass index in children: A meta-analysis. CMAJ 2009, 180, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Guerra, P.H.; Nobre, M.R.; Silveira, J.A.; Taddei, J.A. The effect of school-based physical activity interventions on body mass index: A meta-analysis of randomized trials. Clinics 2013, 68, 1263–1273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fonseca, H.; Matos, M.G.; Guerra, A.; Pedro, J.G. Are overweight and obese adolescents different from their peers? Int. J. Pediatr. Obes. 2009, 4, 166–174. [Google Scholar] [CrossRef]
- Garaulet, M.; Martínez, A.; Victoria, F.; Pérez–Llamas, F.; Ortega, R.M.; Zamora, S. Differences in dietary intake and activity level between normal-weight and overweight or obese adolescents. J. Pediatr. Gastroenterol. Nutr. 2000, 30, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Prentice-Dunn, H.; Prentice-Dunn, S. Physical activity, sedentary behavior, and childhood obesity: A review of cross-sectional studies. Psychol. Health Med. 2012, 17, 255–273. [Google Scholar] [CrossRef] [PubMed]
- Belcher, B.R.; Berrigan, D.; Dodd, K.W.; Emken, B.A.; Chou, C.P.; Spruijt-Metz, D. Physical activity in us youth: Effect of race/ethnicity, age, gender, and weight status. Med. Sci. Sports Exerc. 2010, 42, 2211–2221. [Google Scholar] [CrossRef] [PubMed]
- Yannakoulia, M.; Brussee, S.E.; Drichoutis, A.C.; Kalea, A.Z.; Yiannakouris, N.; Matalas, A.L.; Klimis-Zacas, D. Food consumption patterns in mediterranean adolescents: Are there differences between overweight and normal-weight adolescents? J. Nutr. Educ. Behav. 2012, 44, 233–239. [Google Scholar] [CrossRef]
- Maier, I.B.; Ozel, Y.; Wagnerberger, S.; Bischoff, S.C.; Bergheim, I. Dietary pattern and leisure time activity of overweight and normal weight children in germany: Sex-specific differences. Nutr. J. 2013, 12. [Google Scholar] [CrossRef]
- Wang, C.; Chen, P.; Zhuang, J. A national survey of physical activity and sedentary behavior of chinese city children and youth using accelerometers. Res. Q. Exerc. Sport 2013, 84, S12–S28. [Google Scholar] [CrossRef] [PubMed]
- Padez, C.; Fernandes, T.; Mourao, I.; Moreira, P.; Rosado, V. Prevalence of overweight and obesity in 7–9-year-old portuguese children: Trends in body mass index from 1970–2002. Am. J. Hum. Biol. 2004, 16, 670–678. [Google Scholar] [CrossRef] [PubMed]
- Plataforma Contra a Obesidade. Estudo de Prevalência da Obesidade Infantil e dos Adolescentes Em Portugal Continental. 2009. Available online: http://www.plataformacontraaobesidade.dgs.pt/PresentationLayer/textos01.aspx?cttextoid=494&menuid=169&exmenuid=-1 (accessed on 27 October 2014).
- Llargues, E.; Franco, R.; Recasens, A.; Nadal, A.; Vila, M.; Perez, M.J.; Manresa, J.M.; Recasens, I.; Salvador, G.; Serra, J.; et al. Assessment of a school-based intervention in eating habits and physical activity in school children: The avall study. J. Epidemiol. Community Health 2011, 65, 896–901. [Google Scholar] [CrossRef] [PubMed]
- Story, M.; Nanney, M.S.; Schwartz, M.B. Schools and obesity prevention: Creating school environments and policies to promote healthy eating and physical activity. Milbank Q. 2009, 87, 71–100. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Comprehensive meta-analysis. A computer program for research synthesis; NJ: Englewood, 2013. [Google Scholar]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Introduction to Meta-Analysis; Wiley: Chichester, UK, 2009. [Google Scholar]
- Beretvas, S. Meta-analysis. In The Reviewer’s Guide to Quantitative Methods in the Social Sciences; Hancock, G.R., Mueller, R.O., Eds.; Routledge: New York, NY, USA, 2010; pp. 255–264. [Google Scholar]
- Katzmarzyk, P.T.; Barreira, T.V.; Broyles, S.T.; Champagne, C.M.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Johnson, W.D.; Kuriyan, R.; Kurpad, A.; et al. The international study of childhood obesity, lifestyle and the environment (ISCOLE): Design and methods. BMC Public Health 2013, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirwald, R.L.; Baxter-Jones, A.D.; Bailey, D.A.; Beunen, G.P. An assessment of maturity from anthropometric measurements. Med. Sci. Sports Exerc. 2002, 34, 689–694. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Barreira, T.V.; Schuna, J.M., Jr.; Mire, E.F.; Katzmarzyk, P.T. Fully automated waist-worn accelerometer algorithm for detecting children’s sleep-period time separate from 24-h physical activity or sedentary behaviors. Appl. Physiol. Nutr. Metab. 2014, 39, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Barreira, T.V.; Schuna, J.M., Jr.; Mire, E.F.; Katzmarzyk, P.T.; Chaput, J.-P.; Leduc, G.; Tudor-Locke, C. Identifying children’s nocturnal sleep using 24-hour waist accelerometry. Med. Sci Sports Exerc. 2014. (In press) [Google Scholar]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Tudor-Locke, C.; Barreira, T.V.; Schuna, J.M., Jr.; Mire, E.F.; Katzmarzyk, P.T. Fully automated waist-worn accelerometer algorithm for detecting children’s sleep period time separate from 24-hour physical activity or sedentary behaviors. Appl. Physiol. Nutr. Metab. 2014. (In press) [Google Scholar]
- Abramson, J.H. WINPEPI updated: Computer programs for epidemiologists, and their teaching potential. Epidemiol. Perspect. Innov. 2011. [CrossRef]
- Hedeker, D.; Gibbons, R.; Toit, M.D.; Cheng, Y. Supermix: For Mixed Effects Models; Scientific Software International, Inc.: Lincolnwood, IL, USA, 2008. [Google Scholar]
- Raudenbush, S.W.; Bryk, A.S.; Cheong, Y.F.; Congdon, R.T. Hlm 7: Hierarchical Linear and Nonlinear Modeling; Scientific Software International: Lincolnwood, IL, USA, 2011. [Google Scholar]
- Hox, J.J. Miltilevel Analysis: Techniques and Applications, 2nd ed.; Erlbaum: Mahwah, NJ, USA, 2010. [Google Scholar]
- Snijders, T.A.B.; Bosker, R. Multilevel Analysis: An Introduction to Basic and Advanced Multilevel Modeling; SAGE Publications: London, UK, 2012. [Google Scholar]
- Figueiredo, C.; Santos, D.; Chaves, R.; Souza, M.; Gomes, T.; Santos, F.; Pereira, S.; Borges, A.; Garganta, R.; Maia, J. Prevalências de sobrepeso e obesidade em adolescentes portugueses. Uma revisão da informação dos últimos 10 anos. Revista Portuguesa de Ciências do Desporto 2013, 13, 90–106. [Google Scholar]
- Antunes, A.; Moreira, P. Prevalência de excesso de peso e obesidade em crianças e adolescentes Portugueses. Acta Med. Port. 2011, 24, 279–284. [Google Scholar] [PubMed]
- Yngve, A.; De Bourdeaudhuij, I.; Wolf, A.; Grjibovski, A.; Brug, J.; Due, P.; Ehrenblad, B.; Elmadfa, I.; Franchini, B.; Klepp, K.I.; et al. Differences in prevalence of overweight and stunting in 11-year olds across Europe: The pro children study. Eur. J. Public Health 2008, 18, 126–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sardinha, L.B.; Santos, R.; Vale, S.; Silva, A.M.; Ferreira, J.P.; Raimundo, A.M.; Moreira, H.; Baptista, F.; Mota, J. Prevalence of overweight and obesity among Portuguese youth: A study in a representative sample of 10–18-year-old children and adolescents. Int. J. Pediatr. Obes. 2011, 6, e124–e128. [Google Scholar] [CrossRef] [PubMed]
- Padez, C.; Mourao, I.; Moreira, P.; Rosado, V. Prevalence and risk factors for overweight and obesity in Portuguese children. Acta Paediatr. 2005, 94, 1550–1557. [Google Scholar] [CrossRef] [PubMed]
- De Wilde, J.A.; Verkerk, P.H.; Middelkoop, B.J. Declining and stabilising trends in prevalence of overweight and obesity in Dutch, Turkish, Moroccan and South Asian children 3–16 years of age between 1999 and 2011 in the Netherlands. Arch. Dis. Child. 2014, 99, 46–51. [Google Scholar]
- Moss, A.; Klenk, J.; Simon, K.; Thaiss, H.; Reinehr, T.; Wabitsch, M. Declining prevalence rates for overweight and obesity in German children starting school. Eur. J. Pediatr. 2012, 171, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Matthiessen, J.; Velsing Groth, M.; Fagt, S.; Biltoft-Jensen, A.; Stockmarr, A.; Andersen, S.J.; Trolle, E. Prevalence and trends in overweight and obesity among children and adolescents in Denmark. Scand. J. Public Health 2008, 36, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Lioret, S.; Touvier, M.; Dubuisson, C.; Dufour, A.; Calamassi-Tran, G.; Lafay, L.; Volatier, J.L.; Maire, B. Trends in child overweight rates and energy intake in France from 1999 to 2007: Relationships with socioeconomic status. Obesity 2009, 17, 1092–1100. [Google Scholar] [CrossRef] [PubMed]
- Sundblom, E.; Petzold, M.; Rasmussen, F.; Callmer, E.; Lissner, L. Childhood overweight and obesity prevalences levelling off in Stockholm but socioeconomic differences persist. Int. J. Obes. 2008, 32, 1525–1530. [Google Scholar] [CrossRef]
- Olds, T.S.; Tomkinson, G.R.; Ferrar, K.E.; Maher, C.A. Trends in the prevalence of childhood overweight and obesity in Australia between 1985 and 2008. Int. J. Obes. 2010, 34, 57–66. [Google Scholar] [CrossRef]
- Mitchell, R.T.; McDougall, C.M.; Crum, J.E. Decreasing prevalence of obesity in primary schoolchildren. Arch. Dis. Child. 2007, 92, 153–154. [Google Scholar] [CrossRef] [PubMed]
- Tambalis, K.D.; Panagiotakos, D.B.; Kavouras, S.A.; Kallistratos, A.A.; Moraiti, I.P.; Douvis, S.J.; Toutouzas, P.K.; Sidossis, L.S. Eleven-year prevalence trends of obesity in Greek children: First evidence that prevalence of obesity is leveling off. Obesity 2010, 18, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Baptista, F.; Santos, D.A.; Silva, A.M.; Mota, J.; Santos, R.; Vale, S.; Ferreira, J.P.; Raimundo, A.M.; Moreira, H.; Sardinha, L.B. Prevalence of the Portuguese population attaining sufficient physical activity. Med. Sci. Sports Exerc. 2012, 44, 466–473. [Google Scholar] [CrossRef] [PubMed]
- Instituto do Desporto de Portugal. Estatísticas do desporto: 1996–2012. Available online: http://www.idesporto.pt/conteudo.aspx?id=103 (accessed on 5 July 2012).
- Malina, R.M.; Bouchard, C.; Bar-Or, O. Growth, Maturation and Physical Activiy; Human Kinetics: Champaign, IL, USA, 2004. [Google Scholar]
- Hu, Y.; He, L.; Wu, Y.; Ma, G.; Li, L. Familial correlation and aggregation of body mass index and blood pressure in Chinese Han population. BMC Public Health 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, R.M.; Notkola, I.L.; Shemeikka, S.; Tuomilehto, J.; Nissinen, A. Familial aggregation of body mass index: A population-based family study in Eastern Finland. Horm. Metab. Res. 2002, 34, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Storey, K.E.; Forbes, L.E.; Fraser, S.N.; Spence, J.C.; Plotnikoff, R.C.; Raine, K.D.; McCargar, L.J. Adolescent weight status and related behavioural factors: Web survey of physical activity and nutrition. J. Obes. 2012, 2012. [Google Scholar] [CrossRef] [PubMed]
- Decelis, A.; Jago, R.; Fox, K.R. Physical activity, screen time and obesity status in a nationally representative sample of Maltese youth with international comparisons. BMC Public Health 2014, 14. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Katzmarzyk, P.T.; Boyce, W.F.; King, M.A.; Pickett, W. Overweight and obesity in Canadian adolescents and their associations with dietary habits and physical activity patterns. J. Adolesc. Health 2004, 35, 360–367. [Google Scholar] [CrossRef]
- Patel, S.R.; Hu, F.B. Short sleep duration and weight gain: A systematic review. Obesity 2008, 16, 643–653. [Google Scholar] [CrossRef] [PubMed]
- Padez, C.; Mourao, I.; Moreira, P.; Rosado, V. Long sleep duration and childhood overweight/obesity and body fat. Am. J. Hum. Biol. 2009, 21, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Zheng, L.; Li, Y.; Yu, S.; Sun, G.; Yang, H.; Zhou, X.; Zhang, X.; Sun, Z.; Sun, Y. Differences in lifestyle behaviors, dietary habits, and familial factors among normal-weight, overweight, and obese Chinese children and adolescents. Int. J. Behav. Nutr. Phys. Act. 2012, 9. [Google Scholar] [CrossRef]
- Firouzi, S.; Poh, B.K.; Ismail, M.N.; Sadeghilar, A. Sleep habits, food intake, and physical activity levels in normal and overweight and obese Malaysian children. Obes. Res. Clin. Pract. 2014, 8, e70–e78. [Google Scholar] [CrossRef]
- Knutson, K.L.; Spiegel, K.; Penev, P.; Van Cauter, E. The metabolic consequences of sleep deprivation. Sleep Med. Rev. 2007, 11, 163–178. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, H.; Gama, A.; Mourao, I.; Marques, V.; Ferrao, M.; Padez, C. The associations of SES, obesity, sport activity, and perceived neighborhood environments: Is there a model of environmental injustice penalizing portuguese children? Am. J. Hum. Biol. 2013, 25, 434–436. [Google Scholar] [CrossRef]
- Zhang, Y.X.; Wang, S.R. Differences in development and the prevalence of obesity among children and adolescents in different socioeconomic status districts in Shandong, China. Ann. Hum. Biol. 2012, 39, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Meigen, C.; Keller, A.; Gausche, R.; Kromeyer-Hauschild, K.; Bluher, S.; Kiess, W.; Keller, E. Secular trends in body mass index in German children and adolescents: A cross-sectional data analysis via crescnet between 1999 and 2006. Metabolism 2008, 57, 934–939. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Wang, H.J.; Ma, J.; Lau, P.W.; Hu, P.; Zhang, B.; Wang, Z. Bmi-for-age z-score distribution shifts among Chinese children: Gender disparity. Obesity 2014, 22, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of obesity and trends in body mass index among US children and adolescents, 1999–2010. JAMA 2012, 307, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Skinner, A.C.; Skelton, J.A. Prevalence and trends in obesity and severe obesity among children in the United States, 1999–2012. JAMA Pediatr. 2014, 168, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Moreira, P. Overweight and obesity in Portuguese children and adolescents. J. Public Health 2007, 15, 155–161. [Google Scholar] [CrossRef]
- Souza, M.; Chaves, R.; Santos, D.; Fermino, R.; Garganta, R.; Seabra, A.; Maia, J. Agregação familiar na adiposidade do tronco: Um estudo em famílias nucleares portuguesas. Revista Brasileira de Educação Física e Esporte 2011, 25, 153–161. [Google Scholar]
- De Chaves, R.N.; Baxter-Jones, A.; Santos, D.; Gomes, T.N.; dos Santos, F.K.; de Souza, M.C.; Diego, V.P.; Maia, J. Clustering of body composition, blood pressure and physical activity in Portuguese families. Ann. Hum. Biol. 2014, 41, 157–165. [Google Scholar]
- Rodriguez-Ramirez, S.; Mundo-Rosas, V.; Garcia-Guerra, A.; Shamah-Levy, T. Dietary patterns are associated with overweight and obesity in Mexican school-age children. Arch. Latinoam Nutr. 2011, 61, 270–278. [Google Scholar] [PubMed]
- Maffeis, C. Aetiology of overweight and obesity in children and adolescents. Eur. J. Pediatr. 2000, 159, S35–S44. [Google Scholar] [CrossRef]
- Janssen, I.; Katzmarzyk, P.T.; Boyce, W.F.; Vereecken, C.; Mulvihill, C.; Roberts, C.; Currie, C.; Pickett, W. Comparison of overweight and obesity prevalence in school-aged youth from 34 countries and their relationships with physical activity and dietary patterns. Obes. Rev. 2005, 6, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Pallan, M.J.; Adab, P.; Sitch, A.J.; Aveyard, P. Are school physical activity characteristics associated with weight status in primary school children? A multilevel cross-sectional analysis of routine surveillance data. Arch. Dis. Child. 2014, 99, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Coelho, E.S.M.J.; Vaz Ronque, E.R.; Cyrino, E.S.; Fernandes, R.A.; Valente-Dos-Santos, J.; Machado-Rodrigues, A.; Martins, R.; Figueiredo, A.J.; Santos, R.; Malina, R.M. Nutritional status, biological maturation and cardiorespiratory fitness in Azorean youth aged 11–15 years. BMC Public Health 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.A.; Seabra, A.T.; Silva, R.G.; Katzmarzyk, P.T.; Beunen, G.P.; Maia, J.A. Prevalence of overweight, obesity and physical activity levels in children from Azores Islands. Ann. Hum. Biol. 2010, 37, 682–691. [Google Scholar] [CrossRef] [PubMed]
- Gouveia, É.; Freitas, D.; Maia, J.; Beunen, G.; Claessens, A.; Marques, A.; Thomis, M.; Almeida, S.; Lefevre, J. Prevalência de sobrepeso e obesidade em crianças e adolescentes da região autónoma da madeira, portugal. Acta Pediatr. Port. 2009, 40, 245–251. [Google Scholar]
- Steffen, L.M.; Dai, S.; Fulton, J.E.; Labarthe, D.R. Overweight in children and adolescents associated with TV viewing and parental weight: Project heartbeat! Am. J. Prev. Med. 2009, 37, S50–S55. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gomes, T.N.; Katzmarzyk, P.T.; Dos Santos, F.K.; Souza, M.; Pereira, S.; Maia, J.A.R. Overweight and Obesity in Portuguese Children: Prevalence and Correlates. Int. J. Environ. Res. Public Health 2014, 11, 11398-11417. https://doi.org/10.3390/ijerph111111398
Gomes TN, Katzmarzyk PT, Dos Santos FK, Souza M, Pereira S, Maia JAR. Overweight and Obesity in Portuguese Children: Prevalence and Correlates. International Journal of Environmental Research and Public Health. 2014; 11(11):11398-11417. https://doi.org/10.3390/ijerph111111398
Chicago/Turabian StyleGomes, Thayse Natacha, Peter T. Katzmarzyk, Fernanda K. Dos Santos, Michele Souza, Sara Pereira, and José A. R. Maia. 2014. "Overweight and Obesity in Portuguese Children: Prevalence and Correlates" International Journal of Environmental Research and Public Health 11, no. 11: 11398-11417. https://doi.org/10.3390/ijerph111111398