A Novel Socioeconomic Measure Using Individual Housing Data in Cardiovascular Outcome Research

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Setting
2.2. Study Design
2.3. Study Subjects
2.4. Socioeconomic Indicators and HOUSES Index
2.5. Other Variables
2.6. All-Cause Mortality after MI
2.7. Statistical Analysis
3. Results
3.1. Subject Characteristics
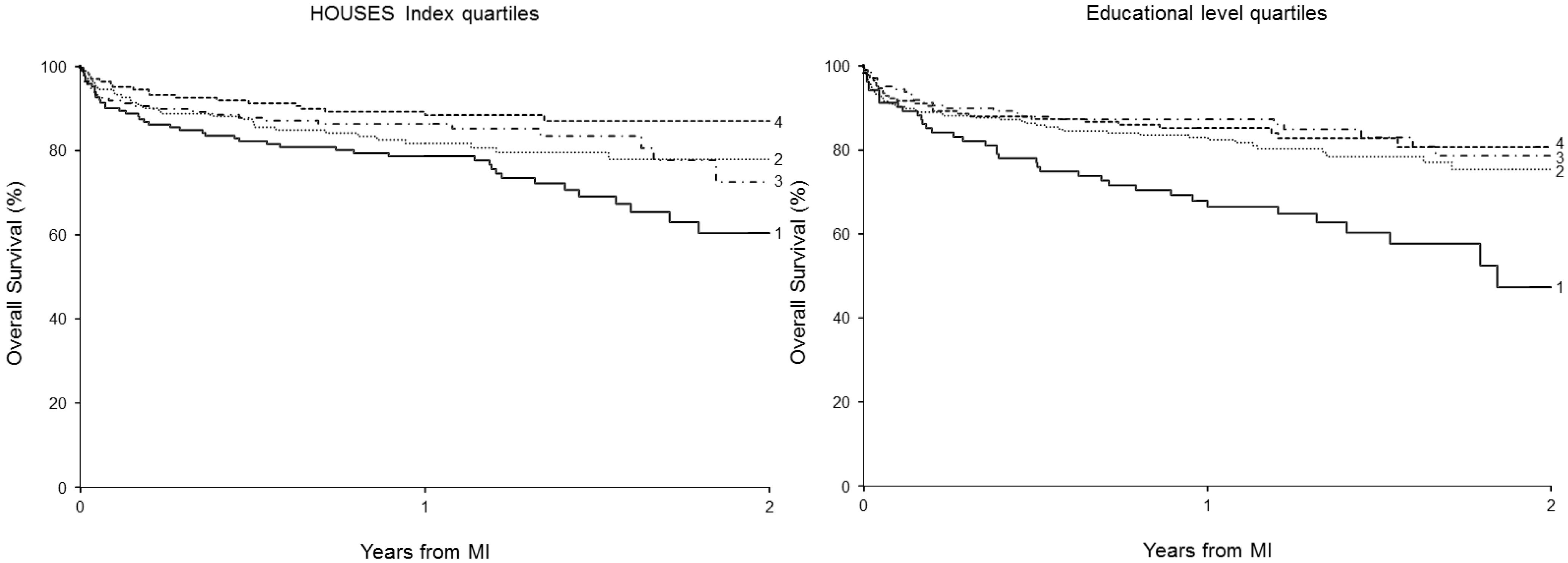
3.2. The Association between HOUSES Index and Education Level with Mortality Post-MI


{kind=link}
| SES Group | Individual Education Level | HOUSES Index | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 (Lowest) (n = 100) | 2 (n = 234) | 3 (n = 158) | 4 (Highest) (n = 167) | p | 1 (Lowest) (n = 159) | 2 (n = 159) | 3 (n = 159) | 4 (Highest) (n = 160) | p | |
| Median | 8 | 12 | 14 | 16 | −4.3213 | −0.7935 | 0.9718 | 3.3681 | ||
| Demographics, n (%) | ||||||||||
| Age (years) | 78 ± 13 | 68 ± 14 | 66 ± 15 | 66 ± 15 | <0.001 | 71 ± 16 | 70 ± 14 | 66 ± 14 | 63 ± 14 | <0.001 |
| Female | 51 (51) | 114 (49) | 72 (46) | 55 (33) | 0.001 | 90 (57) | 65 (41) | 52 (33) | 57 (36) | <0.001 |
| Caucasians | 92 (92) | 226 (97) | 154 (97) | 161 (96) | 0.145 | 146 (92) | 156 (98) | 152 (96) | 154 (96) | 0.146 |
| Risk factors, n (%) | ||||||||||
| Prior MI | 8 (8) | 13 (6) | 9 (6) | 3 (2) | 0.028 | 17 (11) | 6 (4) | 4 (3) | 5 (3) | 0.002 |
| Hypertension | 79 (79) | 168 (72) | 119 (75) | 108 (65) | 0.028 | 121 (76) | 117 (74) | 107 (67) | 105 (66) | 0.019 |
| Diabetes | 36 (36) | 58 (25) | 42 (27) | 24 (14) | <0.001 | 46 (29) | 38 (24) | 37 (23) | 33 (21) | 0.092 |
| Hyperlipidemia | 56 (56) | 147 (63) | 105 (66) | 93 (56) | 0.783 | 97 (61) | 92 (58) | 100 (63) | 99 (62) | 0.659 |
| Current smoker | 15 (15) | 63 (27) | 32 (20) | 15 (9) | 0.008 | 39 (25) | 30 (19) | 36 (23) | 24 (15) | 0.081 |
| BMI | 27.9 ± 6.1 | 28.7 ± 6.4 | 28.7 ± 6.4 | 28.6 ± 5.7 | 0.379 | 29.0 ± 6.1 | 29.0 ± 6.5 | 28.1 ± 6.2 | 29.3 ± 6.2 | 0.684 |
| MI characteristics and comorbidity, n (%) | ||||||||||
| Killip class (n = 639) | ||||||||||
| >1 | 40 (42) | 53 (23) | 33 (21) | 39 (24) | 0.011 | 54 (35) | 52 (33) | 30 (19) | 27 (18) | <0.001 |
| Anterior MI | 48 (48) | 94 (40) | 52 (33) | 66 (40) | 0.147 | 67 (42) | 72 (45) | 61 (38) | 49 (31) | 0.016 |
| ST elevation | 17 (17) | 44 (19) | 29 (18) | 42 (25) | 0.097 | 32 (20) | 29 (18) | 36 (23) | 34 (21) | 0.587 |
| Ejection fraction | 0.070 | 0.015 | ||||||||
| >50 | 45 (57) | 135 (70) | 86 (68) | 100 (72) | 75 (60) | 94 (69) | 86 (67) | 100 (76) | ||
| 35–49 | 20 (26) | 40 (21) | 29 (23) | 27 (20) | 33 (27) | 33 (24) | 24 (19) | 23 (18) | ||
| <35 | 13 (17) | 17 (9) | 11 (9) | 11 (8) | 16 (13) | 10 (7) | 18 (14) | 8 (6) | ||
| Comorbidity index | <0.001 | <0.001 | ||||||||
| 0 | 13 (13) | 68 (29) | 46 (29) | 79 (47) | 31 (20) | 51 (32) | 61 (38) | 68 (43) | ||
| 1–2 | 37 (37) | 70 (30) | 69 (44) | 45 (27) | 57 (36) | 56 (35) | 51 (32) | 44 (28) | ||
| >3 | 50 (50) | 96 (41) | 43 (27) | 43 (26) | 71 (45) | 52 (33) | 47 (30) | 48 (30) | ||
| Treatment | ||||||||||
| PTCA | 37 (37) | 109 (47) | 79 (50) | 86 (52) | 0.027 | 67 (42) | 71 (45) | 86 (54) | 82 (51) | 0.038 |
| CABG | 8 (8) | 16 (7) | 16 (10) | 10 (6) | 0.803 | 3 (2) | 18 (11) | 13 (8) | 15 (9) | 0.041 |
| Statins | 62 (62) | 161 (69) | 111 (70) | 116 (69) | 0.277 | 102 (64) | 110 (69) | 122 (77) | 111 (69) | 0.154 |
| β-blockers | 87 (87) | 208 (89) | 150 (95) | 151 (90) | 0.176 | 145 (91) | 147 (92) | 140 (88) | 143 (89) | 0.348 |
| Aspirin | 90 (90) | 216 (92) | 149 (94) | 155 (93) | 0.373 | 149 (94) | 147 (92) | 148 (93) | 149 (93) | 0.900 |
| HOUSES | 1 Year | 2 Year | Education | 1 Year | 2 Year | ||||
|---|---|---|---|---|---|---|---|---|---|
| Survival Rate (%) | 95% CI | Survival Rate (%) | 95% CI | Survival Rate (%) | 95% CI | Survival Rate (%) | 95% CI | ||
| 4 (highest SES) | 89 | 84–94 | 87 | 81–93 | 4 (highest SES) | 85 | 80–91 | 81 | 74–88 |
| 3 | 86 | 81–92 | 72 | 60–87 | 3 | 87 | 82–93 | 79 | 70–88 |
| 2 | 82 | 76–88 | 78 | 71–85 | 2 | 83 | 78–88 | 75 | 68–83 |
| 1 (lowest SES) | 78 | 72–85 | 60 | 50–72 | 1 (lowest SES) | 68 | 59–78 | 47 | 33–67 |
3.3. Identification of Factors that Account for the Association between SES Measures and Post-MI Mortality
| Regression Models | HOUSES Index (Quartiles) | Education Level (4 Categories) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| (Hazard Ratio, 95%CI, p-Value) b | (Hazard Ratio, 95%CI, p-Value) b | |||||||||
| 4 (ref.) (highest SES) | 3 | 2 | 1 (lowest SES) | p a | 4 (ref) (highest SES) | 3 | 2 | 1 (lowest SES) | P a | |
| Model 1 (unadjusted model) | 1 | 1.52 | 1.76 | 2.47 | <0.001 | 1 | 1.01 | 1.27 | 2.53 | <0.001 |
| (0.85–2.73) | (1.01–3.06) | (1.46–4.19) | (0.59–1.72) | (0.79–2.03) | (1.55–4.14) | |||||
| Model 2 | 1 | 1.37 | 1.27 | 1.86 | 0.036 | 1 | 0.95 | 1.16 | 1.84 | 0.015 |
| (0.75–2.52) | (0.71–2.26) | (1.07–3.24) | (0.55–1.67) | (0.70–1.90) | (1.11–3.05) | |||||
| Model 3 (full model) | 1 | 1.29 | 1.19 | 1.45 | 0.24 | 1 | 0.82 | 0.83 | 0.93 | 0.84 |
| (0.68–2.43) | (0.65–2.16) | (0.82–2.58) | (0.46–1.44) | (0.51–1.37) | (0.55–1.57) | |||||
4. Discussion
| Unadjusted HRs and 95%CI | HOUSES Index (Quartiles) | Education Level (Quartiles) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 4 (ref) | 3 | 2 | 1 | p a | 4 (ref) | 3 | 2 | 1 | p a | |
| 1 | 1.52 | 1.76 | 2.47 | <0.001 | 1 | 1.01 | 1.27 | 2.53 | <0.001 | |
| (0.85, 2.73) | (1.01, 3.06) | (1.46, 4.19) | (0.59, 1.72) | (0.79, 2.03) | (1.55, 4.14) | |||||
| Adjusted HRs for HOUSES Index and Educational Level Controlled for each Variable Listed Below | ||||||||||
| Model adjusted for: | ||||||||||
| Age | 1 | 1.34 | 1.25 | 1.59 | 0.116 | 1 | 0.99 | 1.19 | 1.48 | 0.089 |
| (0.75, 2.40) | (0.72, 2.19) | (0.93, 2.72) | (0.58, 1.69) | (0.75, 1.91) | (0.90, 2.45) | |||||
| Comorbidity b | 1 | 1.46 | 1.63 | 1.74 | 0.028 | 1 | 0.75 | 0.83 | 1.33 | 0.186 |
| (0.82, 2.63) | (0.93, 2.83) | (1.03, 2.94) | (0.44, 1.29) | (0.51, 1.33) | (0.81, 2.18) | |||||
| Female | 1 | 1.52 | 1.73 | 2.31 | 0.002 | 1 | 0.96 | 1.20 | 2.39 | <0.001 |
| (0.85, 2.73) | (1.00, 3.01) | (1.35, 3.94) | (0.56, 1.64) | (0.75, 1.92) | (1.46, 3.92) | |||||
| White race | 1 | 1.52 | 1.73 | 2.52 | <0.001 | 1 | 0.99 | 1.27 | 2.58 | <0.001 |
| (0.85, 2.73) | (0.99, 3.00) | (1.49, 4.26) | (0.58, 1.70) | (0.79, 2.02) | (1.58, 4.21) | |||||
| Hypertension | 1 | 1.50 | 1.68 | 2.27 | 0.002 | 1 | 0.94 | 1.21 | 2.34 | <0.001 |
| (0.84, 2.69) | (0.97, 2.92) | (1.34, 3.86) | (0.55, 1.62) | (0.75, 1.93) | (1.43, 3.84) | |||||
| Diabetes | 1 | 1.50 | 1.75 | 2.35 | 0.001 | 1 | 0.94 | 1.20 | 2.27 | 0.001 |
| (0.84, 2.70) | (1.01, 3.04) | (1.39, 3.99) | (0.55, 1.61) | (0.75, 1.92) | (1.37, 3.75) | |||||
| Hyperlipidemia | 1 | 1.57 | 1.76 | 2.55 | <0.001 | 1 | 1.07 | 1.34 | 2.54 | <0.001 |
| (0.88, 2.82) | (1.01, 3.05) | (1.51, 4.33) | (0.62, 1.83) | (0.84, 2.15) | (1.56, 4.15) | |||||
| Current smoker | 1 | 1.55 | 1.76 | 2.56 | <0.001 | 1 | 1.06 | 1.38 | 2.59 | <0.001 |
| (0.87, 2.78) | (1.01, 3.06) | (1.51, 4.34) | (0.62, 1.82) | (0.86, 2.22) | (1.58, 4.23) | |||||
| BMI | 1 | 1.36 | 1.61 | 2.38 | <0.001 | 1 | 1.03 | 1.32 | 2.44 | <0.001 |
| (0.76, 2.43) | (0.93, 2.81) | (1.40, 4.03) | (0.60, 1.76) | (0.82, 2.10) | (1.49, 3.98) | |||||
| Killip class > 1 | 1 | 1.37 | 1.41 | 2.14 | 0.005 | 1 | 0.96 | 1.19 | 2.23 | 0.003 |
| (0.76, 2.48) | (0.80, 2.49) | (1.26, 3.66) | (0.56, 1.66) | (0.74, 1.91) | (1.35, 3.69) | |||||
| Anterior MI | 1 | 1.49 | 1.69 | 2.40 | <0.001 | 1 | 1.02 | 1.25 | 2.44 | <0.001 |
| (0.83, 2.67) | (0.97, 2.95) | (1.42, 4.08) | (0.59, 1.75) | (0.78, 2.00) | (1.49, 3.99) | |||||
| Ejection fraction | 1 | 1.42 | 1.71 | 2.21 | 0.001 | 1 | 1.02 | 1.28 | 2.41 | <0.001 |
| (0.79, 2.54) | (0.98, 2.97) | (1.36, 3.93) | (0.60, 1.75) | (0.80, 2.05) | (1.48, 3.95) | |||||
| Aspirin | 1 | 1.50 | 1.75 | 2.46 | <0.001 | 1 | 1.02 | 1.24 | 2.38 | <0.001 |
| (0.84, 2.69) | (1.01, 3.04) | (1.45, 4.16) | (0.59, 1.74) | (0.78, 1.99) | (1.46, 3.89) | |||||
| β-blockers | 1 | 1.52 | 1.80 | 2.53 | <0.001 | 1 | 1.03 | 1.27 | 2.49 | <0.001 |
| (0.85, 2.72) | (1.04, 3.13) | (1.49, 4.29) | (0.60, 1.76) | (0.79, 2.03) | (1.52, 4.07) | |||||
| Statins | 1 | 1.68 | 1.78 | 2.39 | 0.001 | 1 | 1.01 | 1.29 | 2.33 | <0.001 |
| (0.94, 3.02) | (1.02, 3.09) | (1.41, 4.05) | (0.59, 1.73) | (0.81, 2.07) | (1.42, 3.81) | |||||
| PTCA | 1 | 1.62 | 1.66 | 2.25 | 0.003 | 1 | 0.94 | 1.17 | 2.04 | 0.004 |
| (0.90, 2.90) | (0.95, 2.88) | (1.33, 3.81) | (0.55, 1.61) | (0.73, 1.88) | (1.25, 3.35) | |||||
| CABG | 1 | 1.51 | 1.81 | 2.35 | 0.001 | 1 | 1.04 | 1.28 | 2.62 | <0.001 |
| (0.84, 2.72) | (1.04, 3.14) | (1.39, 3.98) | (0.60, 1.78) | (0.80, 2.04) | (1.60, 4.29) | |||||
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Murphy, S.L.; Xu, J.; Kochanek, K.D. National Vital Statistics Reports. Deaths: Preliminary Data for 2010; Centers for Disease Control and Prevention: Hyattsville, MD, USA, 2012.
- Yeh, R.W.; Sidney, S.; Chandra, M.; Sorel, M.; Selby, S.V.; Go, A.S. Population trends in the incidence and outcomes of acute myocardial infarction. N. Engl. J. Med. 2010, 362, 2155–2165. [Google Scholar]
- Rosamond, W.D.; Chambless, L.E.; Heiss, G.; Mosley, T.H.; Coresh, J.; Whitsel, E.; Wagenknecht, L.; Ni, H.; Folsom, A.R. Twenty-two-year trends in incidence of myocardial infarction, coronary heart disease mortality, and case fatality in 4 US communities, 1987–2008. Circulation 2012, 125, 1848–1857. [Google Scholar]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart disease and stroke statistics—2013 Update: A report from the American heart association. Circulation 2013, 127, e6–e245. [Google Scholar]
- Lynch, J.W.; Kaplan, G.A.; Cohen, R.D.; Kauhanen, J.; Wilson, T.W.; Smith, N.L.; Salonen, J.T. Childhood and adult socioeconomic status as predictors of mortality in Finland. Lancet 1994, 343, 524–527. [Google Scholar]
- Kaplan, G.A.; Keil, J.E. Socioeconomic factors and cardiovascular disease: A review of the literature. Circulation 1993, 88, 1973–1998. [Google Scholar]
- Kaplan, G.A.; Salonen, J.T. Socioeconomic conditions in childhood and ischaemic heart disease during middle age. BMJ 1990, 301, 1121–1123. [Google Scholar]
- Kim, E.M.; Hwang, S.Y.; Kim, A.L. Knowledge of stroke and heart attack symptoms and risk factors among rural elderly people: A questionnaire survey. Korean Circ. J. 2011, 41, 259–264. [Google Scholar]
- Beebe-Dimmer, J.; Lynch, J.W.; Turrell, G.; Lustgarten, S.; Raghunathan, T.; Kaplan, G.A. Childhood and adult socioeconomic conditions and 31-year mortality risk in women. Am. J. Epidemiol. 2004, 159, 481–490. [Google Scholar]
- Salomaa, V.; Miettinen, H.; Niemelä, M.; Ketonen, M.; Mähönen, M.; Immonen-Räihä, P.; Lehto, S.; Vuorenmaa, T.; Koskinen, S.; Palomäki, P.; et al. Relation of socioeconomic position to the case fatality, prognosis and treatment of myocardial infarction events; The FINMONICA MI Register Study. J. Epidemiol. Community Health 2001, 55, 475–482. [Google Scholar]
- Mehta, R.H.; O’Shea, J.C.; Stebbins, A.L.; Granger, C.B.; Armstrong, P.W.; White, H.D.; Topol, E.J.; Califf, R.M.; Ohman, E.M. Association of mortality with years of education in patients with ST-segment elevation myocardial infarction treated with fibrinolysis. J. Am. Coll. Cardiol. 2011, 57, 138–146. [Google Scholar]
- Ancona, C.; Arcà, M.; Saitto, C.; Agabiti, N.; Fusco, D.; Tancioni, V.; Perucci, C.A. Differences in access to coronary care unit among patients with acute myocardial infarction in Rome: Old, ill, and poor people hold the burden of inefficiency. BMC Health Serv. Res. 2004, 4. [Google Scholar] [CrossRef]
- Blais, C.; Hamel, D.; Rinfret, S. Impact of socioeconomic deprivation and area of residence on access to coronary revascularization and mortality after a first acute myocardial infarction in Quebec. Can. J. Cardiol. 2012, 28, 169–177. [Google Scholar]
- Tonne, C.; Schwartz, J.; Mittleman, M.; Melly, S.; Suh, H.; Goldberg, R. Long-term survival after acute myocardial infarction is lower in more deprived neighborhoods. Circulation 2005, 111, 3063–3070. [Google Scholar]
- Alter, D.A.; Chong, A.; Austin, P.C.; Mustard, C.; Iron, K.; Williams, J.I.; Morgan, C.D.; Tu, J.V.; Irvine, V.; Naylor, D.; et al. Socioeconomic status and mortality after acute myocardial infarction. Ann. Intern. Med. 2006, 144, 82–93. [Google Scholar]
- Pardo-Crespo, M.R.; Narla, N.P.; Williams, A.R.; Beebe, T.J.; Sloan, J.; Yawn, B.P.; Wheeler, P.H.; Juhn, Y.J. Comparison of individual-level versus versus area-level socioeconomic measures in assessing health outcomes of children in Olmsted County, Minnesota. J. Epidemiol. Community Health 2013, 67, 305–310. [Google Scholar]
- Liberatos, P.; Link, B.G.; Kelsey, J.L. The measurement of social class in epidemiology. Epidemiol. Rev. 1988, 10, 87–121. [Google Scholar]
- Karaca-Mandic, P.; Jena, A.B.; Joyce, G.F.; Goldman, D.P. Out-of-pocket medication costs and use of medications and health care services among children with asthma. JAMA 2012, 307, 1284–1291. [Google Scholar]
- Juhn, Y.J.; Beebe, T.J.; Finnie, D.M.; Sloan, J.; Wheeler, P.H.; Yawn, B.; Williams, A.R. Development and initial testing of a new socioeconomic status measure based on housing data. J. Urban Health 2011, 88, 933–944. [Google Scholar]
- Johnson, M.D.; Urm, S.H.; Jung, J.A.; Yun, H.D.; Munitz, G.E.; Tsigrelis, C.; Baddour, L.M.; Juhn, Y.J. Housing data-based socioeconomic index and risk of invasive pneumococcal disease: An exploratory study. Epidemiol. Infect. 2013, 141, 880–887. [Google Scholar]
- Harris, M.N.; Lundien, M.C.; Finnie, D.M.; Williams, A.R.; Beebe, T.J.; Sloan, J.A.; Yawn, B.Y.; Juhn, Y.J. Application of a novel socioeconomic measure using individual housng data in asthma research. Prim. Care Respir. J. 2014. [Google Scholar] [CrossRef]
- Butterfield, M.C.; Williams, A.R.; Beebe, T.; Finnie, D.; Liu, H.; Liesinger, J.; Sloan, J.; Wheeler, P.H.; Yawn, B.; Juhn, Y.J. A two-county comparison of the HOUSES index on predicting self-rated health. J. Epidemiol. Community Health 2011, 65, 254–259. [Google Scholar]
- Diez Roux, A.V. Conceptual approaches to the study of health disparities. Annu. Rev. Pub. Health 2011, 13, 1–18. [Google Scholar]
- Kurland, L.T.; Molgaard, C.A. The patient record in epidemiology. Sci. Am. 1981, 245, 54–63. [Google Scholar]
- Melton, L.J., 3rd. History of the Rochester Epidemiology Project. Mayo Clin. Proc. 1996, 71, 266–274. [Google Scholar]
- St. Sauver, J.L.; Grossardt, B.R.; Leibson, C.L.; Yawn, B.P.; Melton, L.J., 3rd; Rocca, W.A. Generalizability of epidemiological findings and public health decisions: An illustration from the Rochester Epidemiology Project. Mayo Clin. Proc. 2012, 87, 151–160. [Google Scholar]
- Rocca, W.A.; Yawn, B.P.; St Sauver, J.L.; Grossardt, B.R.; Melton, L.J., 3rd. History of the Rochester Epidemiology Project: Half a century of medical records linkage in a US population. Mayo Clin. Proc. 2012, 87, 1202–1213. [Google Scholar]
- Gerber, Y.; Weston, S.A.; Killian, J.M.; Therneau, T.M.; Jacobsen, S.J.; Roger, V.L. Neighborhood income and individual education: Effect on survival after myocardial infarction. Mayo Clin. Proc. 2008, 83, 663–669. [Google Scholar]
- Roger, V.L.; Killian, J.M.; Weston, S.A.; Jaffe, A.S.; Kors, J.; Santrach, P.J.; Tunstall-Pedoe, H.; Jacobsen, S.J. Redefinition of myocardial infarction: Prospective evaluation in the community. Circulation 2006, 114, 790–797. [Google Scholar]
- Hersh, A.L.; Jackson, M.A.; Hicks, L.A.; the Committee on Infectious Diseases. Principles of judicious antibiotic prescribing for upper respiratory tract infections in pediatrics. Pediatrics 2013, 132, 1146–1154. [Google Scholar]
- Williams, D.R. Missed opportunities in monitoring socioeconomic status. Pub. Health Rep. 1997, 112, 492–494. [Google Scholar]
- Smith, S. The essential qualities of a home. J. Environ. Psychol. 1994, 14, 31–46. [Google Scholar]
- Smith, S.J. Healthy status and the housing system. Soc. Sci. Med. 1990, 31, 753–762. [Google Scholar]
- Dunn, J.R. Housing and inequalities in health: A study of socioeconomic dimensions of housing and self reported health from a survey of Vancouver residents. J. Epidemiol. Community Health 2002, 56, 671–681. [Google Scholar]
- Dunn, J.R.; Hayes, M.V.; Hulchanski, J.D.; Hwang, S.W.; Potvin, L. Housing as a socio-economic determinant of health: Findings of a national needs, gaps and opportunities assessment. Can. J. Pub. Health 2006, 97 (Suppl. 3), S11–S15. [Google Scholar]
- Macintyre, S.; Ellaway, A.; Der, G.; Ford, G.; Hunt, K. Do housing tenure and car access predict health because they are simply markers of income or self esteem? A Scottish study. J. Epidemiol. Community Health 1998, 52, 657–664. [Google Scholar]
- Howden-Chapman, P.L.; Chandola, T.; Stafford, M.; Marmot, M. The effect of housing on the mental health of older people: The impact of lifetime housing history in Whitehall II. BMC Pub. Health 2011, 11. [Google Scholar] [CrossRef]
- Laaksonen, M.; Martikainen, P.; Nihtilä, E.; Rahkonen, O.; Lahelma, E. Home ownership and mortality: A register-based follow-up study of 300,000 Finns. J. Epidemiol. Community Health 2008, 62, 293–297. [Google Scholar]
- Smith, G.D.; Egger, M. Socioeconomic differences in mortality in Britain and the United States. Am. J. Pub. Health 1992, 82, 1079–1081. [Google Scholar]
- Yun, H.D.; Knoebel, E.; Fenta, Y.; Gabriel, S.E.; Leibson, C.L.; Loftus, E.V., Jr.; Roger, V.; Yawn, B.P.; Li, B.; Juhn, Y.J. Asthma and proinflammatory conditions: A population-based retrospective matched cohort study. Mayo Clin. Proc. 2012, 87, 953–960. [Google Scholar]
- Iribarren, C.; Tolstykh, I.V.; Miller, M.K.; Sobel, E.; Eisner, M.D. Adult asthma and risk of coronary heart disease, cerebrovascular disease, and heart failure: A prospective study of 2 matched cohorts. Am. J. Epidemiol. 2012, 176, 1014–1024. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bang, D.W.; Manemann, S.M.; Gerber, Y.; Roger, V.L.; Lohse, C.M.; Rand-Weaver, J.; Krusemark, E.; Yawn, B.P.; Juhn, Y.J. A Novel Socioeconomic Measure Using Individual Housing Data in Cardiovascular Outcome Research. Int. J. Environ. Res. Public Health 2014, 11, 11597-11615. https://doi.org/10.3390/ijerph111111597
Bang DW, Manemann SM, Gerber Y, Roger VL, Lohse CM, Rand-Weaver J, Krusemark E, Yawn BP, Juhn YJ. A Novel Socioeconomic Measure Using Individual Housing Data in Cardiovascular Outcome Research. International Journal of Environmental Research and Public Health. 2014; 11(11):11597-11615. https://doi.org/10.3390/ijerph111111597
Chicago/Turabian StyleBang, Duk Won, Sheila M. Manemann, Yariv Gerber, Veronique L. Roger, Christine M. Lohse, Jennifer Rand-Weaver, Elizabeth Krusemark, Barbara P. Yawn, and Young J. Juhn. 2014. "A Novel Socioeconomic Measure Using Individual Housing Data in Cardiovascular Outcome Research" International Journal of Environmental Research and Public Health 11, no. 11: 11597-11615. https://doi.org/10.3390/ijerph111111597