Occupational Exposure to Staphylococcus aureus and Enterococcus spp. among Spray Irrigation Workers Using Reclaimed Water

Abstract
:1. Introduction
2. Experimental Section
2.1. Study Site
2.2. Subject Selection
2.3. Survey
2.4. Sample Collection
2.5. Isolation
2.6. Confirmation
2.7. Antimicrobial Susceptibility Testing
2.8. Statistical Analyses
3. Results and Discussion
3.1. Results

{kind=link}
{kind=link}
| Variable | n (%) | p-value | ||
|---|---|---|---|---|
| Spray Irrigation Workers | Office Worker Controls | |||
| Total | 19 | 24 | ||
| Age (years) | 0.41 | |||
| ≤17 | 3 (16) | 0 (0) | ||
| 18–19 | 2 (11) | 2 (8) | ||
| 20–30 | 4 (21) | 10 (42) | ||
| 31–41 | 5 (26) | 6 (25) | ||
| 42–56 | 4 (21) | 5 (21) | ||
| >56 | 1 (5) | 1 (4) | ||
| Gender | 1.00 | |||
| Male | 18 (95) | 23 (96) | ||
| Female | 1 (5) | 1 (4) | ||
| Race | 0.58 | |||
| Caucasian | 17 (90) | 23 (96) | ||
| Other | 2 (10) | 1 (4) | ||
| Education | <0.001 | |||
| Less than high school | 1 (5) | 0 (0) | ||
| High school | 12 (63) | 0 (0) | ||
| Associate | 2 (11) | 0 (0) | ||
| College | 4 (21) | 24 (100) | ||
| Yearly income ($1,000s) | 0.01 | |||
| <15 | 10 (56) | 5 (21) | ||
| 15–25 | 3 (17) | 6 (25) | ||
| 25–35 | 2 (11) | 1 (4) | ||
| 35–50 | 2 (11) | 1 (4) | ||
| >50 | 1 (6) | 11 (46) | ||
| Duration in job | 0.22 | |||
| ≤1 month | 2 (10.5) | 1 (4) | ||
| >1 month–≤6 months | 6 (31.5) | 3 (12.5) | ||
| >6 months–≤2 years | 3 (16) | 5 (21) | ||
| >2–≤5 years | 5 (26) | 5 (21) | ||
| >5–≤ 20 years | 3 (16) | 5 (21) | ||
| ≥20 years | 0 (0) | 5 (21) | ||
| Currently smoke | 0.002 | |||
| Yes | 10 (53) | 2 (8) | ||
| No | 9 (47) | 22 (92) | ||
| Smoke more than 100 cigarettes in past 6 months | <0.001 | |||
| Yes | 9 (47) | 0 (0) | ||
| No | 10 (53) | 24 (100) | ||
| Personally worked in healthcare setting | 1.00 | |||
| Yes | 3 (16) | 4 (17) | ||
| No | 16 (84) | 20 (83) | ||
| Household member worked in healthcare setting | 0.69 | |||
| Yes | 6 (32) | 9 (37.5) | ||
| No | 13 (68) | 15 (62.5) | ||
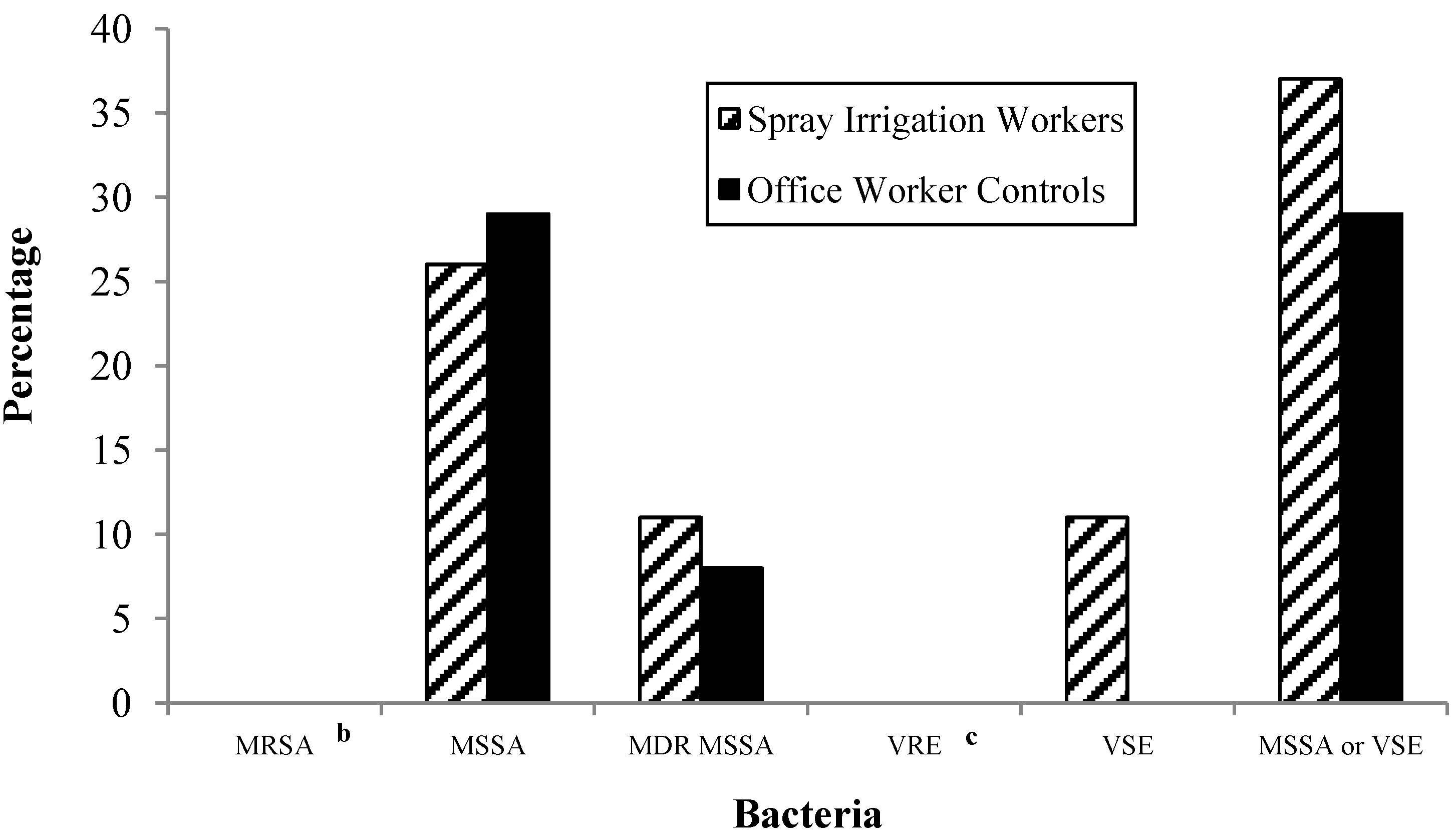
3.1.1. Presence of MRSA and MSSA

3.1.2. Presence of VRE and VSE
3.1.3. Presence of Either of the Target Bacteria in Swab Samples
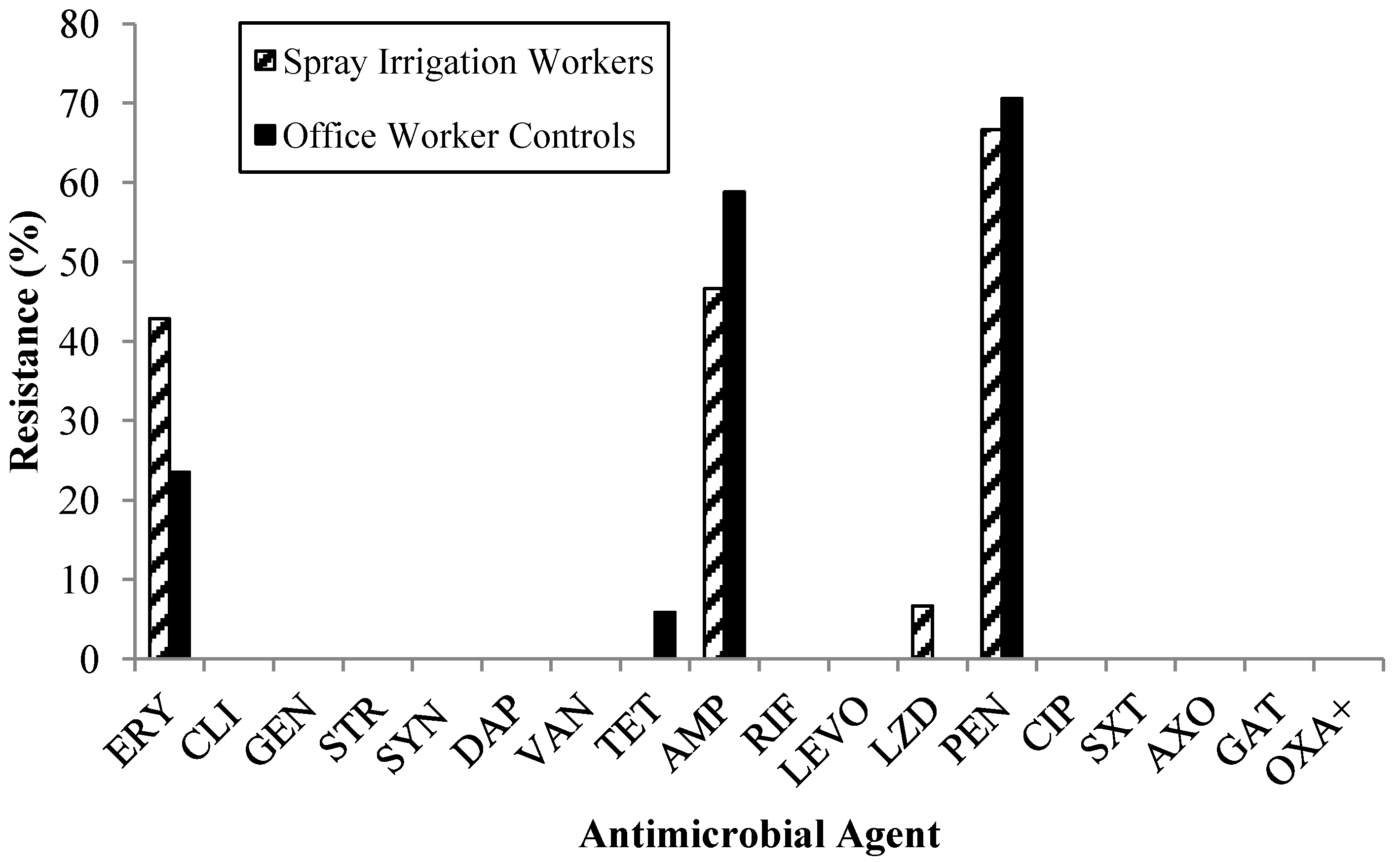
3.1.4. Antibiotic Resistance Patterns

3.1.5. Impact of Occupational Exposure on Colonization
| Unadjusted OR | 95% CI | Adjusted OR * | 95% CI | |
|---|---|---|---|---|
| MSSA | ||||
| Spray irrigation worker | 0.87 | 0.23, 3.34 | 1.40 | 0.09, 22.40 |
| Office worker control | ||||
| MDR MSSA | ||||
| Spray irrigation worker | 1.29 | 0.17, 10.15 | 7.01 | 0.13, 367.77 |
| Office worker control | — | |||
| MSSA or VSE | ||||
| Spray irrigation worker | 1.42 | 0.39, 5.11 | 2.55 | 0.15, 44.15 |
| Office worker control | — |
3.1.6. Factors Impacting MSSA and VSE Colonization among Spray Irrigation Workers
3.2. Discussion
3.2.1. MRSA and MSSA Prevalence
3.2.2. VRE and VSE Prevalence
3.2.3. Public Health Implications
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Miller, W. Water Reuse in the U.S.: Overview and Trends. In Proceedings of NWRA Annual Conference, Reno, NV, USA, 2 February 2011.
- NRC. Water Reuse: Potential for Expanding the Nation’s Water Supply through Reuse of Municipal Wastewater; National Research Council: Washington, DC, USA, 2012. [Google Scholar]
- Jjemba, P.K.; Weinrich, L.A.; Cheng, W.; Giraldo, E.; LeChevallier, M.W. Regrowth of potential opportunistic pathogens and algae in reclaimed-water distribution systems. Appl Environ. Microbiol. 2010, 76, 4169–4178. [Google Scholar] [CrossRef]
- Blumenthal, U.J.; Cifuentes, E.; Bennett, S.; Quigley, M.; Ruiz-Palacios, G. The risk of enteric infections associated with wastewater reuse: The effect of season and degree of storage of wastewater. Trans. R Soc. Trop. Med. Hyg. 2001, 95, 131–137. [Google Scholar] [CrossRef]
- Devaux, I.; Gerbaud, L.; Planchon, C.; Bontoux, J.; Glanddier, P. Infectious risk associated with wastewater reuse: An epidemiological approach applied to the case of clermont-ferrand, France. Water Sci. Technol. 2001, 43, 53–60. [Google Scholar]
- Durand, R.; Schwebach, G. Gastrointestinal effects of water reuse for public park irrigation. Amer. J. Public Health 1989, 79, 1659–1660. [Google Scholar] [CrossRef]
- Goldstein, R.E.; Micallef, S.A.; Gibbs, S.G.; Davis, J.A.; He, X.; George, A.; Kleinfelter, L.M.; Schreiber, N.A.; Mukherjee, S.; Sapkota, A.; et al. Methicillin-resistant Staphylococcus aureus (MRSA) detected at four U.S. wastewater treatment plants. Environ. Health Perspect. 2012, 120, 1551–1558. [Google Scholar] [CrossRef]
- Araujo, C.; Torres, C.; Silva, N.; Carneiro, C.; Gonclaves, A.; Radhouani, H.; Correia, S.; da Costa, M.P.; Paccheco, R.; Zarazaga, M.; et al. Vancomycin-resistant enterococci from portugese wastewater treatment plants. J. Basic Microbiol. 2010, 50, 605–609. [Google Scholar] [CrossRef]
- Börjesson, S.; Melin, S.; Matussek, A.; Lindgren, P.-E. A seasonal study of the Meca gene and Staphylococcus aureus including methicillin-resistant S. aureus in a municipal wastewater treatment plant. Water Res. 2009, 43, 925–932. [Google Scholar] [CrossRef]
- Kotzamanidis, C.; Zdragas, A.; Kourelis, A.; Moraitou, E.; Papa, A.; Yiantzi, V.; Pantelidou, C.; Yiangou, M. Characterization of vana-type Enterococcus faecium isolates from urban and hospital wastewater and pigs. J. Appl. Microbiol. 2009, 107, 997–1005. [Google Scholar] [CrossRef]
- Nagulapally, S.R.; Ahmad, A.; Henry, A.; Marchin, G.L.; Zurek, L.; Bhandari, A. Occurence of ciprofloxacin-, trimethoprim-sulfamethoxazole-, and vancomycin-resistant bacteria in a municipal wastewater treatment plant. Water Environ. Res. 2009, 81, 82–90. [Google Scholar] [CrossRef]
- Rosenberg Goldstein, R.E.; Micallef, S.A.; Gibbs, S.G.; George, A.; Claye, E.; Sapkota, A.; Joseph, S.W.; Sapkota, A.R. Detection of vancomycin-resistant enterococci (VRE) at four U.S. wastewater treatment plants that provide effluent for reuse. Sci. Total Environ. 2014, 466–467, 404–411. [Google Scholar] [CrossRef]
- Mainous, I.; Arch, G.; Diaz, V.A.; Matheson, E.M.; Gregorie, S.H.; Hueston, W.J. Trends in hospitalizations with antibiotic-resistant infections: U.S., 1997–2006. Public Health Rep. 2011, 126, 354–360. [Google Scholar]
- Bassetti, M.; Nicco, E.; Mikulska, M. Why is community-associated Mrsa spreading across the world and how will it change clinical practice? Int. J. Antimicrob. Agents 2009, 34, S15–S19. [Google Scholar] [CrossRef]
- Fracchia, L.; Pietronave, S.; Rinaldi, M.; Martinotti, G.M. Site-related airborne biological hazard and seasonal variations in two wastewater treatment plants. Water Res. 2006, 40, 1985–1994. [Google Scholar] [CrossRef]
- Murray, P.R.; Rosenthal, K.S.; Kobayashi, G.S.; Pfaller, M.A. Medical Microbiology, 4th ed.; Mosby: St. Louis, MO, USA, 2002. [Google Scholar]
- Hidron, A.I.; Edwards, J.R.; Patel, J.; Horan, T.C.; Sievert, D.M.; Pollock, D.A.; Fridkin, S.K. National Healthcare Safety Network Team. NHSN annual update: Antimicrobial-resistant pathogens associated with healthcare-associated infections: Annual summary of data reported to the national healthcare safety network at the centers for disease control and prevention, 2006–2007. Infect. Control Hosp. Epidemio 2008, 29, 996–1011. [Google Scholar] [CrossRef]
- Talebi, M.; Rahimi, F.; Katouli, M.; Mollby, R.; Pourshafie, M.R. Epidemiological link between wastewater and human vancomycin-resistant Enterococcus faecium isolates. Curr. Microbiol. 2008, 56, 468–473. [Google Scholar] [CrossRef]
- Luczkiewicz, A.; Jankowska, K.; Fudala-Ksiazek, S.; Nczuk-Neyman, O.K. Antimicrobial resistance of fecal indicators in municipal wastewater treatment plant. Water Res. 2010, 44, 5089–5097. [Google Scholar] [CrossRef]
- Korzeniewska, E.; Filipkowska, Z.; Gotkowska-Płachta, A.; Janczukowicz, W.; Dixon, B.; Czułowska, M. Determination of emitted airborne microorganisms from a Bio-Pak wastewater treatment plant. Water Res. 2009, 43, 2841–2851. [Google Scholar] [CrossRef]
- Poole, T.L.; Hume, M.E.; Campbell, L.D.; Scott, H.M.; Alali, W.Q.; Harvey, R.B. Vancomycin-resistant Enterococcus faecium strains isolated from community wastewater from a semiclosed agri-food system in Texas. Antimicrob. Agents Chemother. 2005, 49, 4382–4385. [Google Scholar] [CrossRef]
- McDonald, L.C.; Kuehnert, M.J.; Tenover, F.; Jarvis, W. Vancomycin-resistant enterococci outside the health-care setting: Prevalence, sources, and public. Emerg. Infect. Dis. 1997, 3, 311–317. [Google Scholar] [CrossRef]
- Bassetti, S.; Bischoff, W.E.; Walter, M.; Bassetti-Wyss, B.A.; Mason, L.; Reboussin, B.A.; D’Agostino, R.B.; Gwaltney, J.M.; Pfaller, M.A.; Sherertz, R.J. Dispersal of Staphylococcus aureus into the air associated with a rhinovirus infection. Infect. Control Hosp. Epidemiol. 2005, 26, 196–203. [Google Scholar]
- FDA. Bad Bug Book—Staphylococcus aureus; Center for Food Safety and Applied Nutrition: College Park, MD, USA, 2009. [Google Scholar]
- Gorwitz, R.J.; Kruszon-Moran, D.; McAllister, S.K.; McQuillan, G.; McDougal, L.K.; Fosheim, G.E.; Jensen, B.J.; Killgore, G.; Tenover, F.C.; Kuehnert, M.J. Changes in the prevalence of nasal colonization with Staphylococcus aureus in the United States, 2001–2004. J. Infect. Dis. 2008, 197, 1226–1234. [Google Scholar] [CrossRef]
- Ochei, J.; Kolhatkar, A. Medical Laboratory Science: Theory and Practice, 10th ed.; Tata McGraw-Hill: New Delhi, India., 2000. [Google Scholar]
- Kullander, J.; Forslund, O.; Dillner, J. Staphylococcus aureus and squamous cell carcinoma of the skin. Cancer Epidemiol. Biomarker. Prev. 2009, 18, 472–478. [Google Scholar] [CrossRef]
- Fang, H.; Hedin, G. Rapid screening and identification of methicillin-resistant Staphylococcus aureus from clinical samples by selective-broth and real-time PCR assay. J. Clin. Microbiol. 2003, 41, 2894–2899. [Google Scholar] [CrossRef]
- Micallef, S.A.; Goldstein, R.E.; George, A.; Ewing, L.; Tall, B.D.; Boyer, M.S.; Joseph, S.W.; Sapkota, A.R. Diversity, distribution and antibiotic resistance of Enterococcus spp. Recovered from tomatoes, leaves, water and soil on U.S. Mid-atlantic farms. Food Microbiol. 2013, 36, 465–474. [Google Scholar] [CrossRef]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2013; Volume M100-S23. [Google Scholar]
- John, J.J.; Barg, N. Staphylococcus aureus, 2nd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA., 1999; pp. 325–345. [Google Scholar]
- Crook, J. Irrigation of Parks, Playgrounds, and Schoolyards with Reclaimed Water: Extent and Safety; WateReuse Foundation: Alexandria, VA, USA, 2005. [Google Scholar]
- Stevenson, K.B.; Searle, K.; Stoddard, G.J.; Samore, M.H. Methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci in rural communities, western United States. Emerg. Infect. Dis. 2005, 11, 895–903. [Google Scholar] [CrossRef]
- Anzar, E.; Buendía, B.; García-Peñuela, E.; Escudero, E.; Alarcón, T.; López-Brea, M. Community-acquired urinary tract infection caused by vancomycin-resistant Enterococcus faecalis clinical isolate. Rev. Esp. Quimioter. 2004, 17, 263–265. [Google Scholar]
- Wendt, C.; Krause, C.; Xander, L.U.; Löffler, D.; Floss, H. Prevalence of colonization with vancomycin-resistant enterococci in various population groups in Berlin, Germany. J. Hosp. Infect. 1999, 42, 193–200. [Google Scholar] [CrossRef]
- Warren, D.K.; Nitin, A.; Hill, C.; Fraser, V.; Kollef, M. Occurrence of co-colonization or co-infection with vancomycin-resistant enterococci and methicillin-resistant Staphylococcus aureus in a medical intensive care unit. Infect. Control Hosp. Epidemiol. 2004, 25, 99–104. [Google Scholar]
- Hendrix, C.W.; Hammond, J.M.J.; Swoboda, S.M.; Merz, W.G.; Harrington, S.M.; Perl, T.M.; Dick, J.D.; Borschel, D.M.; Halczenko, P.W.; Pelz, R.K.; et al. Surveillance strategies and impact of vancomycin-resistant enterococcal colonization and infection in critically ill patients. Ann. Surg. 2001, 233, 259–265. [Google Scholar] [CrossRef]
- Camann, D.E.; Moore, B.E.; Harding, H.J.; Sorber, C.A. Microorganism levels in air near spray irrigation of municipal wastewater: The lubbock infection surveillance study. J. Water Pollut. Control 1988, 60, 1960–1970. [Google Scholar]
- Palmer, C.J.; Bonilla, G.F.; Roll, B.; Paszko-Kolva, C.; Sangermano, L.R.; Fujioka, R.S. Detection of Legionella species in reclaimed water and air with the enviroamp Legionella pcr kit and direct fluorescent antibody staining. Appl. Environ. Microbiol. 1995, 61, 407–412. [Google Scholar]
- Brissaud, F.; Blin, E.; Hemous, S.L.G. Water reuse for urban landscape irrigation: Aspersion and health related regulations. Water Sci. Technol. 2008, 57, 781–787. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Goldstein, R.E.R.; Micallef, S.A.; Gibbs, S.G.; He, X.; George, A.; Sapkota, A.; Joseph, S.W.; Sapkota, A.R. Occupational Exposure to Staphylococcus aureus and Enterococcus spp. among Spray Irrigation Workers Using Reclaimed Water. Int. J. Environ. Res. Public Health 2014, 11, 4340-4355. https://doi.org/10.3390/ijerph110404340
Goldstein RER, Micallef SA, Gibbs SG, He X, George A, Sapkota A, Joseph SW, Sapkota AR. Occupational Exposure to Staphylococcus aureus and Enterococcus spp. among Spray Irrigation Workers Using Reclaimed Water. International Journal of Environmental Research and Public Health. 2014; 11(4):4340-4355. https://doi.org/10.3390/ijerph110404340
Chicago/Turabian StyleGoldstein, Rachel E. Rosenberg, Shirley A. Micallef, Shawn G. Gibbs, Xin He, Ashish George, Amir Sapkota, Sam W. Joseph, and Amy R. Sapkota. 2014. "Occupational Exposure to Staphylococcus aureus and Enterococcus spp. among Spray Irrigation Workers Using Reclaimed Water" International Journal of Environmental Research and Public Health 11, no. 4: 4340-4355. https://doi.org/10.3390/ijerph110404340