A Survey Aimed at General Citizens of the US and Japan about Their Attitudes toward Electronic Medical Data Handling

Abstract
:1. Introduction
- (1)
- What kinds of doctors, public organizations, private companies, people allow to access their medical data?
- (2)
- Is a scheme allowing healthcare providers or private companies to access people’s anonymous medical data for the purpose of healthcare cost savings accepted?
- (3)
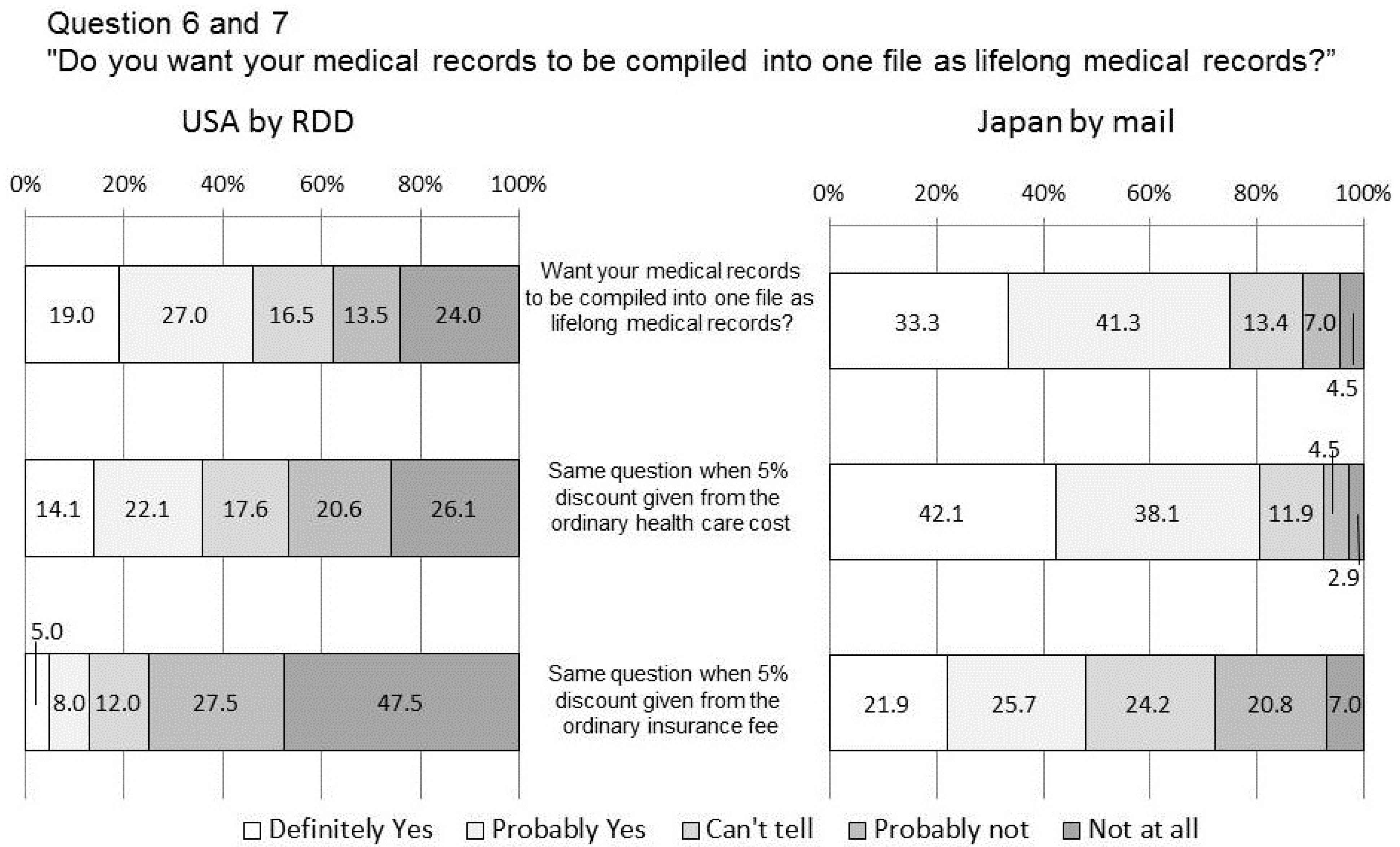
- Do people prefer to compile their medical records into one life-long record?
- (4)
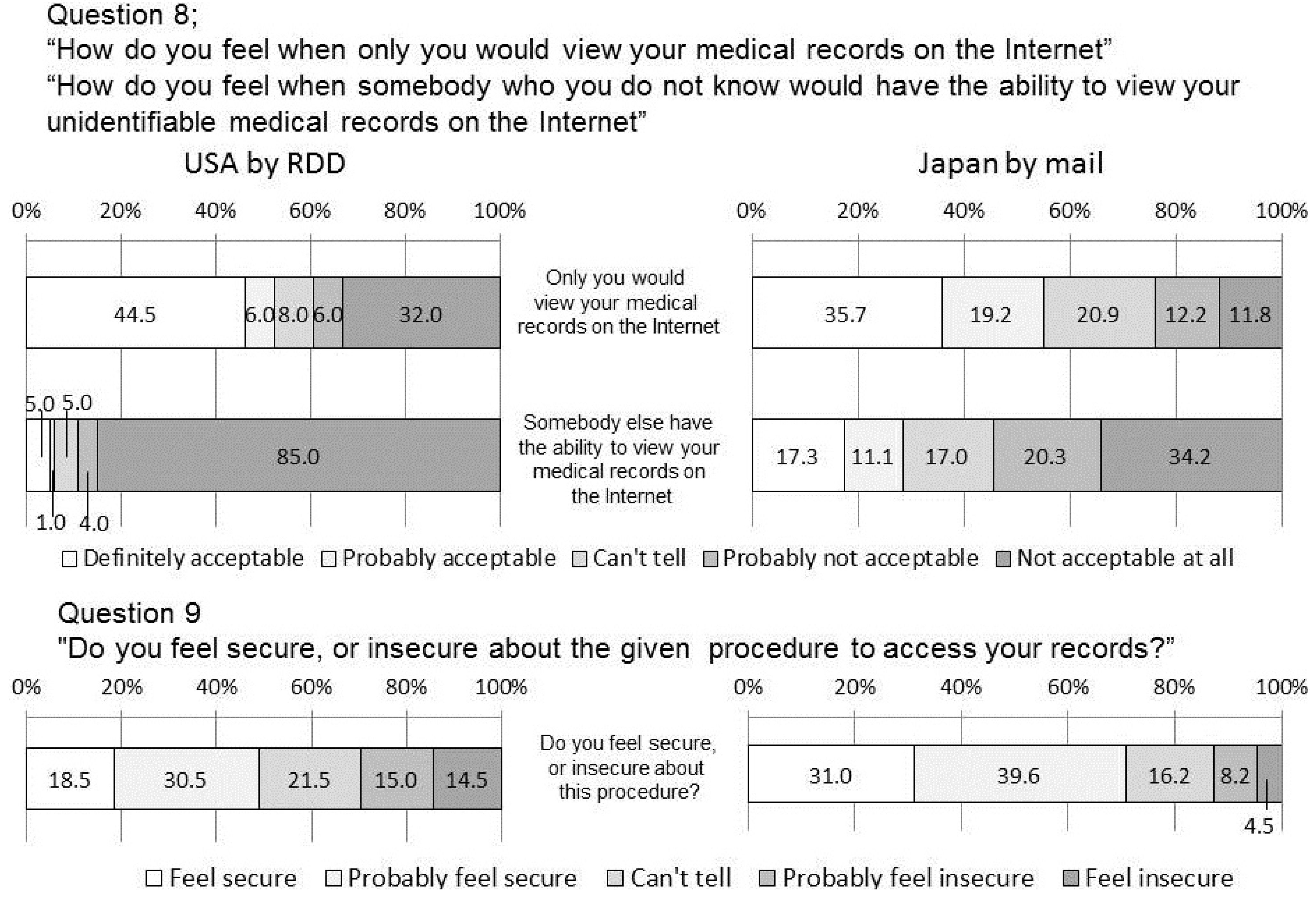
- Is access to their medical data via the internet considered acceptable and safe?
- (5)
- Do the results differ between these two countries, considering the differences in their healthcare policy?
2. Methods
2.1. Survey in the US
2.2. Survey in Japan
2.3. Statistical Analysis
2.4. Explained Definition of “Identified” and “Unidentified”
2.5. Questionnaires
3. Results
3.1. Responder Attributes

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Categories | Attributes | US | Japan |
|---|---|---|---|
| Sex | Male | 42.5% | 76.1% |
| Female | 57.5% | 23.9% | |
| Age | 19–29 | 8.0% | 2.9% |
| 30–39 | 12.0% | 5.7% | |
| 40–49 | 11.5% | 15.7% | |
| 50–59 | 27.0% | 33.1% | |
| 60–69 | 22.5% | 42.5% | |
| 70+ | 17.5% | ||
| No response | 1.5% | n/a | |
| Current physical condition | Healthy | 60.0% | 30.0% |
| Rather healthy | 25.5% | 49.2% | |
| Not very healthy | 9.0% | 16.8% | |
| Not healthy | 5.5% | 4.0% |
3.2. Questionnaire Results
| Percentage | Single choice answers |
|---|---|
| 21.0% | Being able to receive treatment of the same quality at any physician’s office or hospital |
| 18.0% | Avoiding duplicated tests and prescriptions |
| 9.0% | Healthcare cost savings |
| 5.0% | Receiving an adequate explanation for your disease |
| 4.0% | Promotion of collaborative community healthcare |
| 4.0% | Provision of a lifelong medical record system |
| 4.0% | Contribution to future medical progress |
| 1.5% | Access to health care at a nearby hospital |
| 1.0% | Establishment of a team-based healthcare environment in various medical facilities |
| 32.5% | Other |
4. Discussion
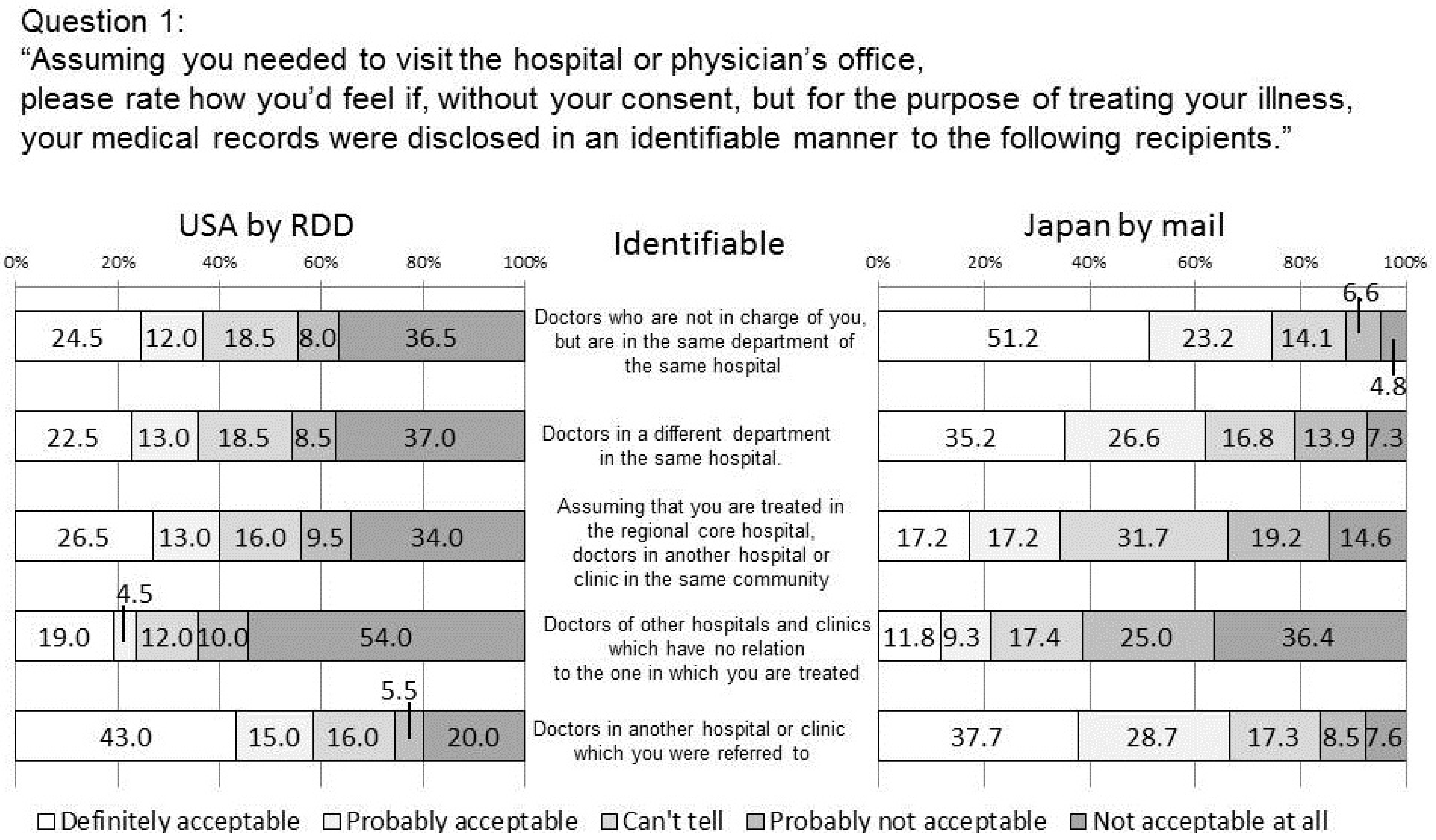
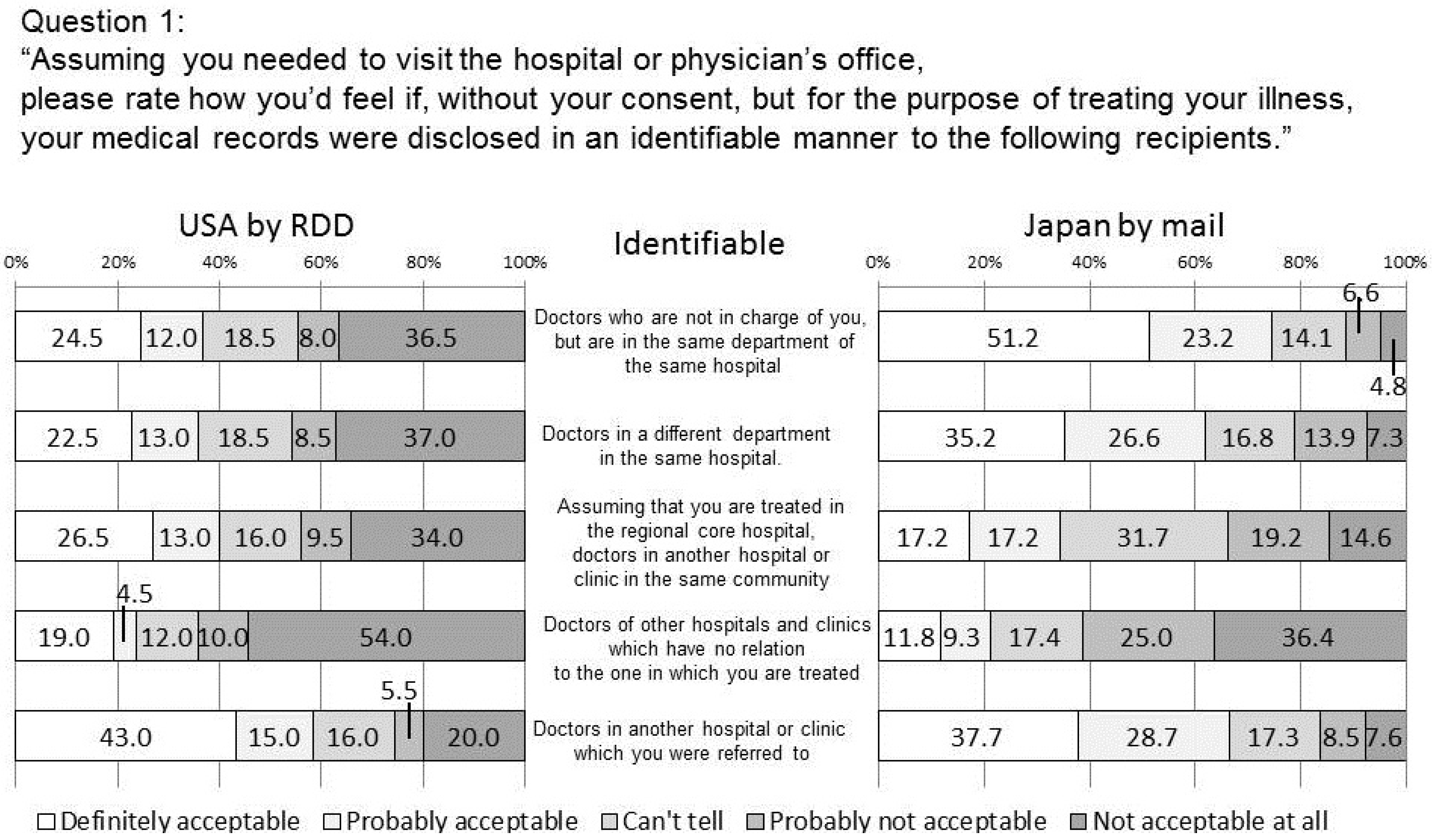
4.1. Q1 about the Handling of Medical Records
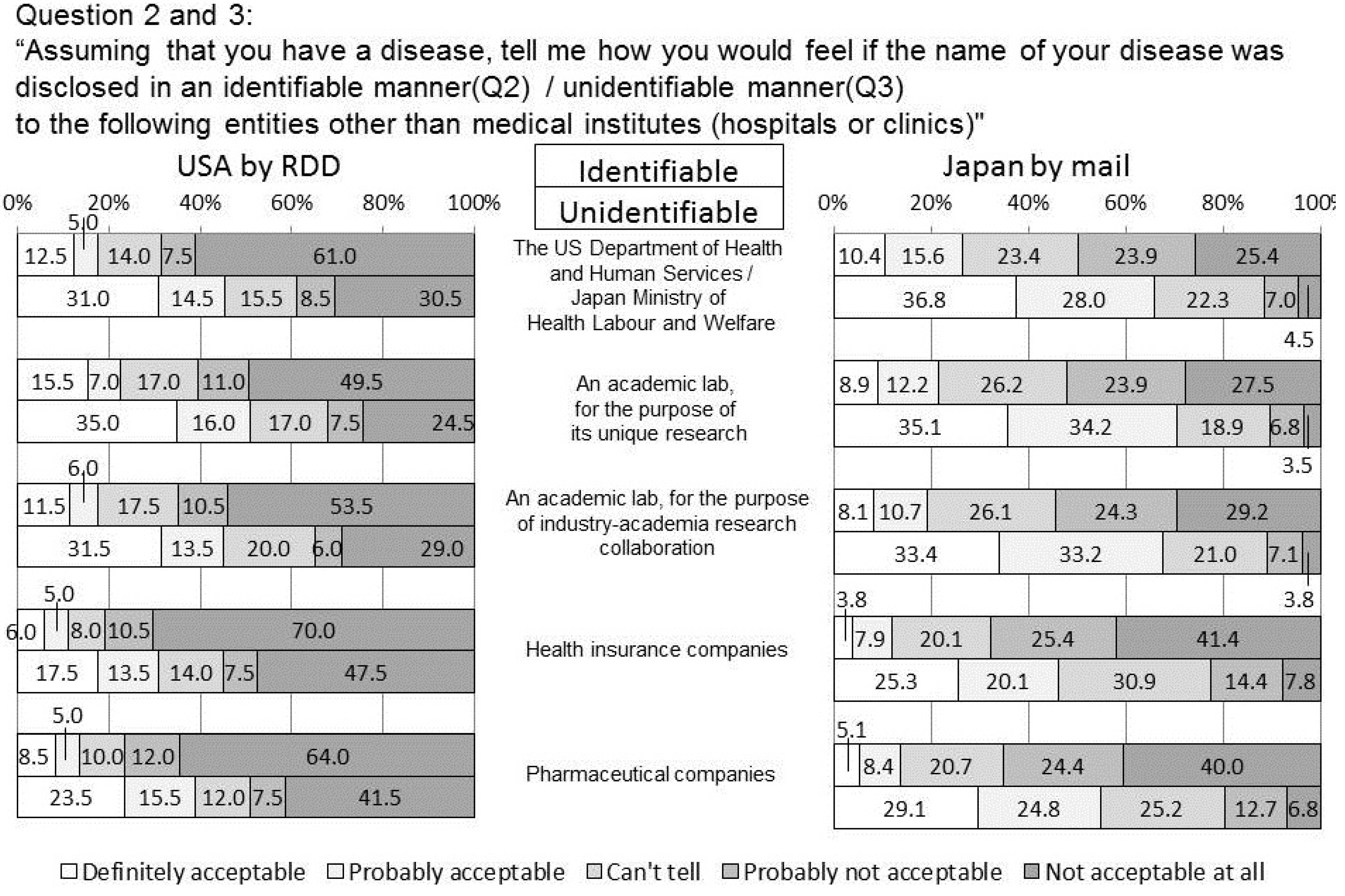
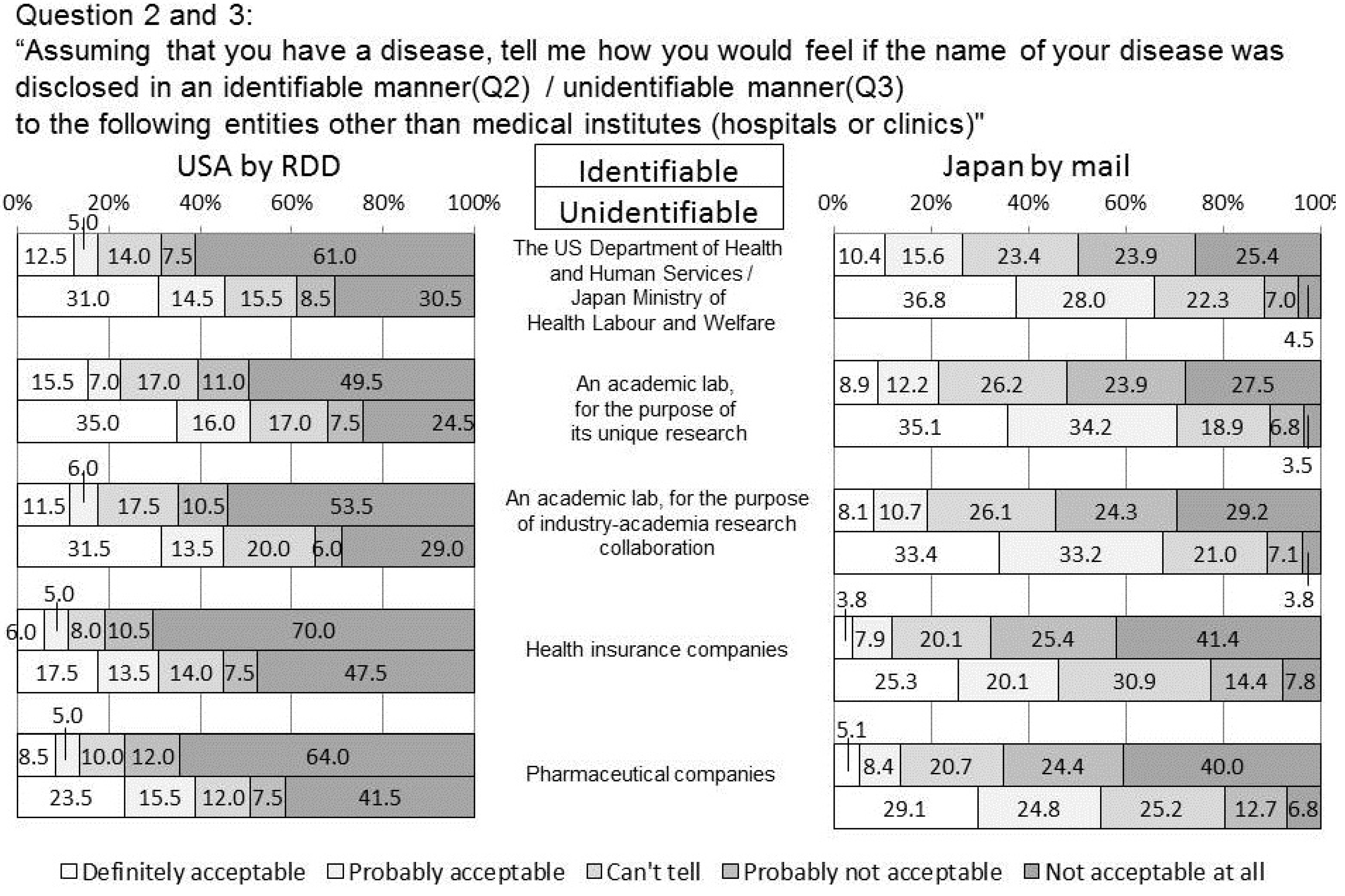
4.2. Q2 and 3 Disclosure of the Name of the Disease
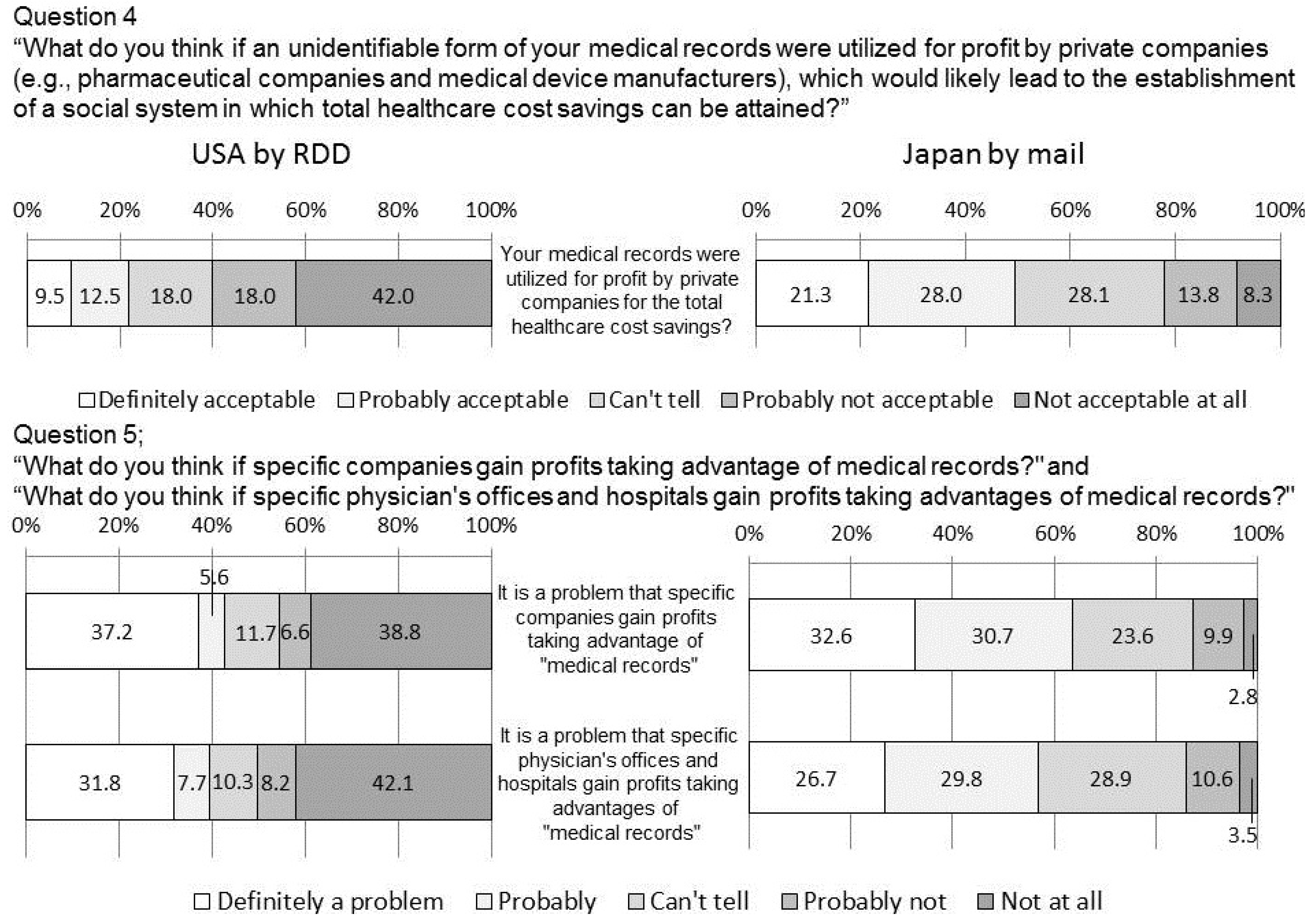
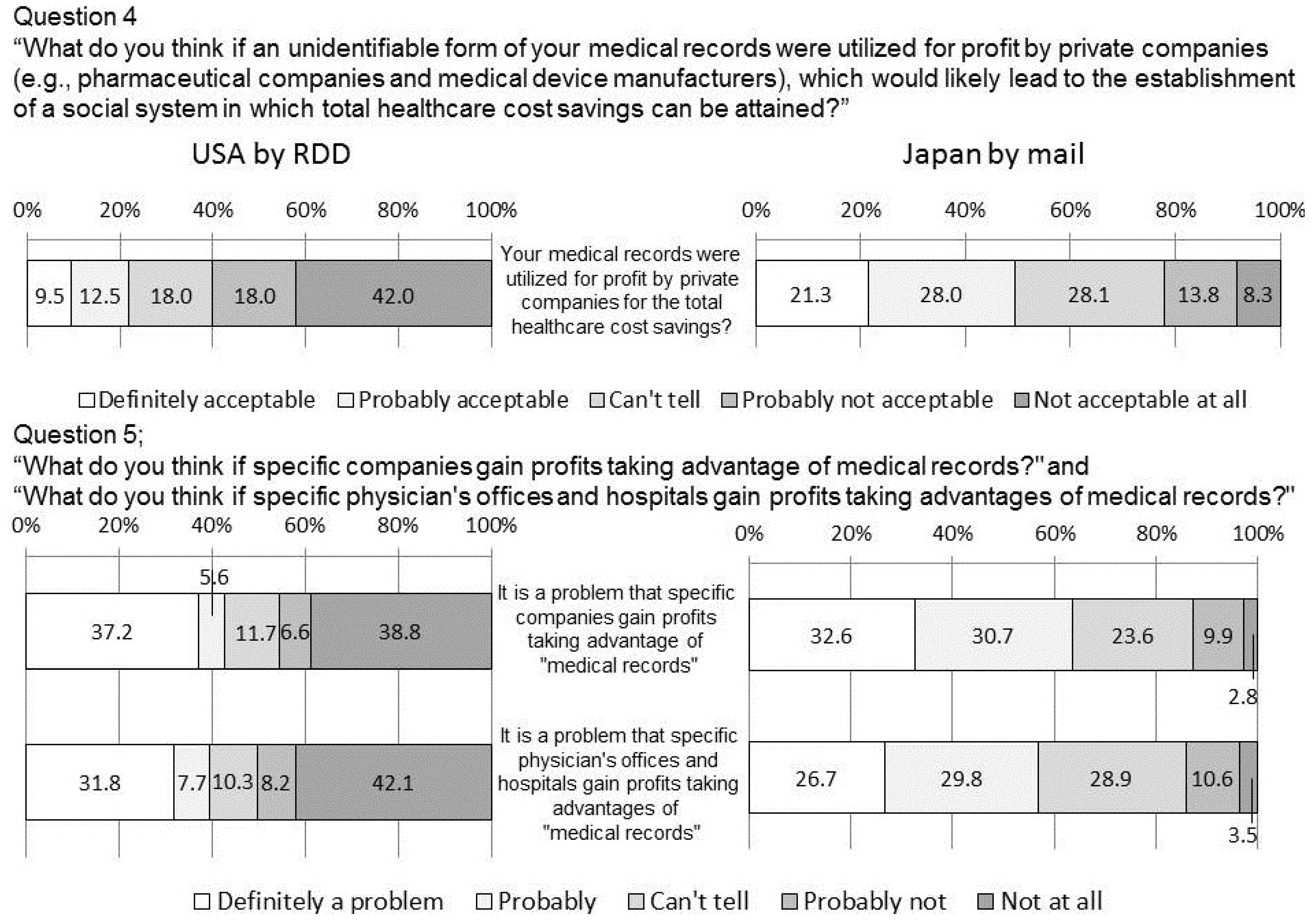
4.3. Q4 and 5 Secondary Usage of Information
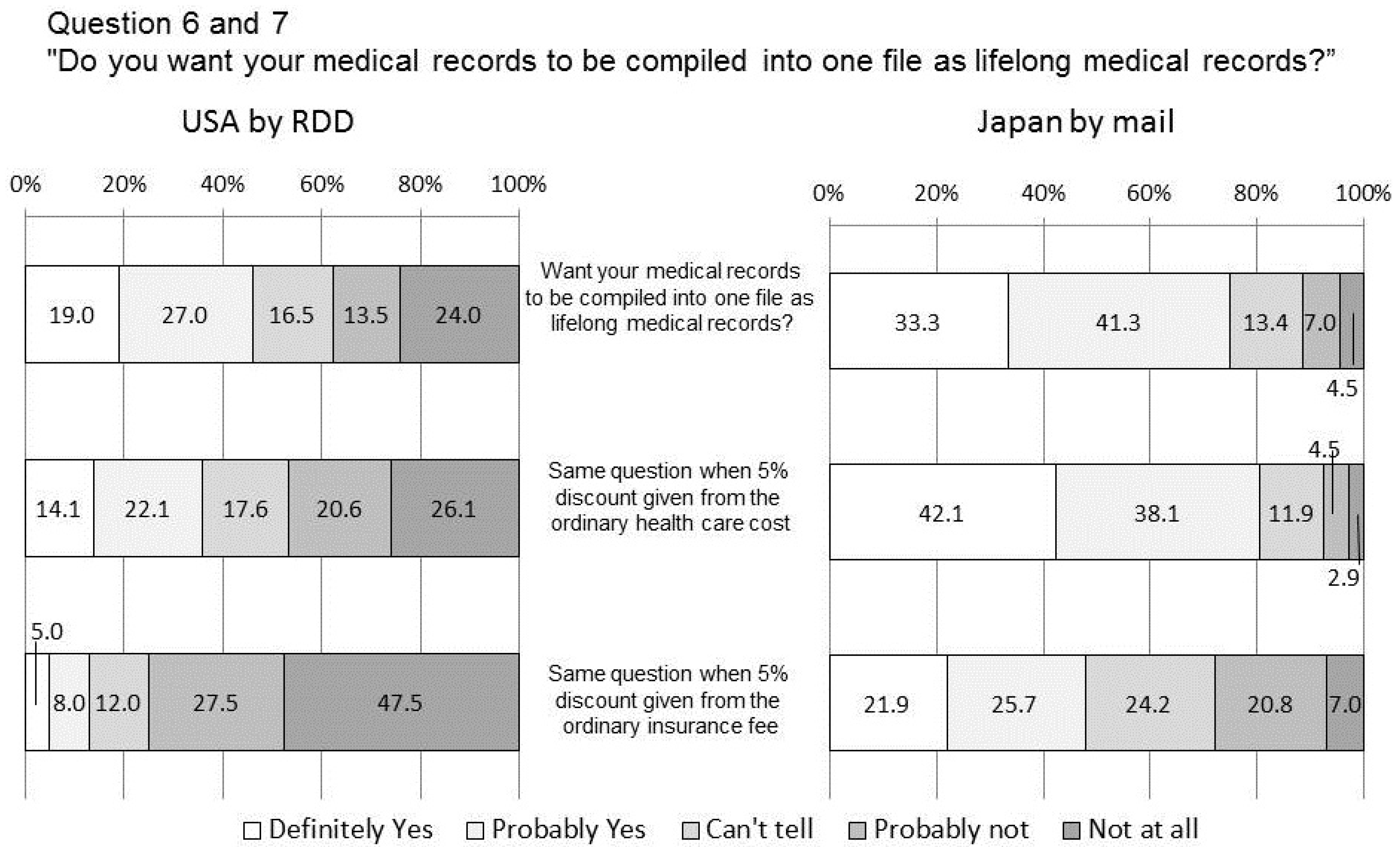
4.4. Q6 and 7 Lifelong Medical Records
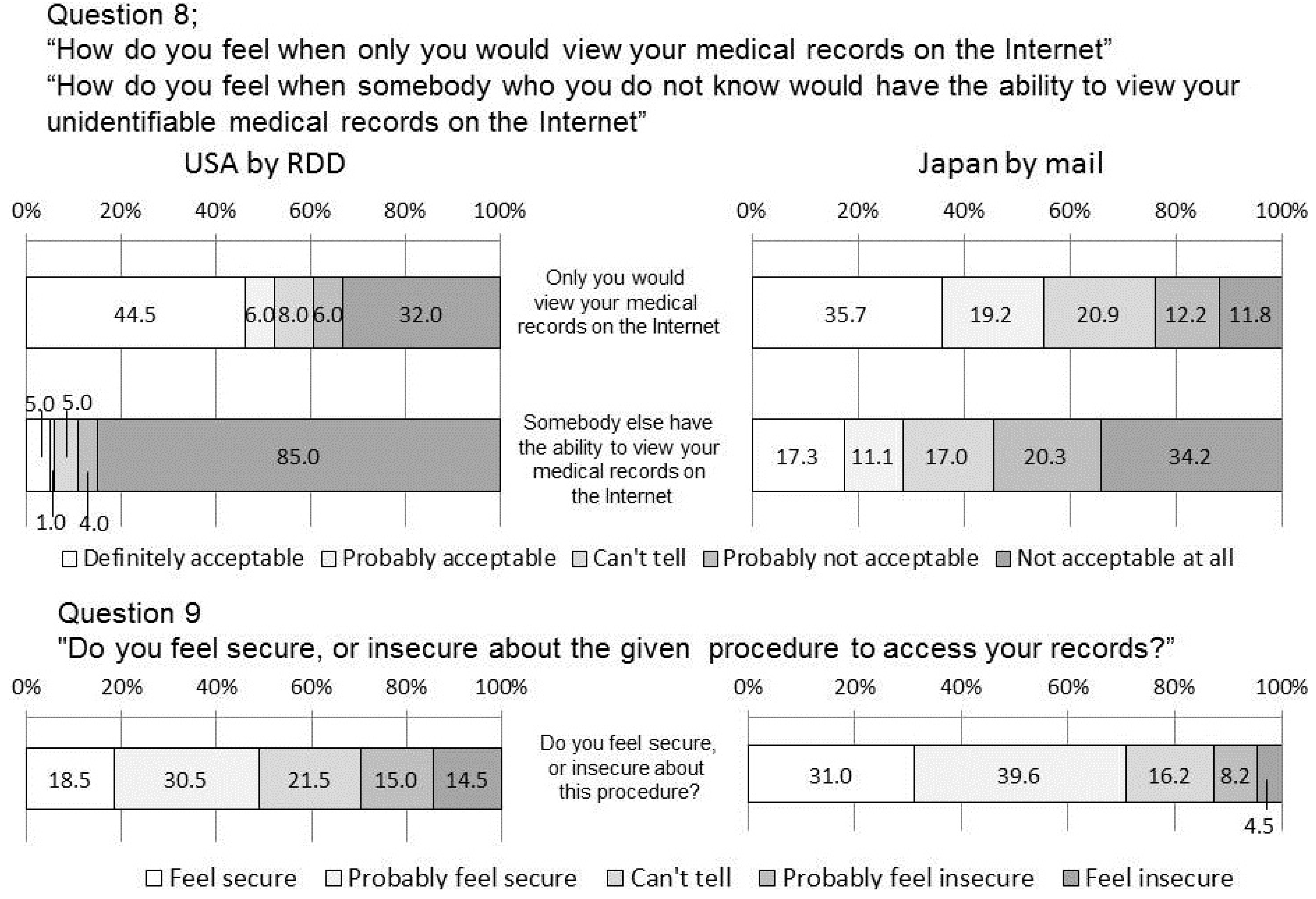
4.5. Q8 and 9 Access to Medical Records on the Internet
4.6. Q10 Expectation for Healthcare IT Innovation
4.7. Limitations of This Survey
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- McDonald, C.J.; Overhage, J.M.; Barnes, M.; Schadow, G.; Blevins, L.; Dexter, P.R.; Mamlin, B.; the INPC Management. The Indiana network for patient care: A working local health information infrastructure. Health Aff. 2005, 24, 1214–1220. [Google Scholar] [CrossRef]
- Miller, R.H.; Miller, B.S. The Santa Barbara county care data exchange: What happened? Health Aff. 2007, 26, W568–W580. [Google Scholar] [CrossRef]
- Giokas, D. Canada’s Interoperable EHR. Infoway chooses the more challenging path, the greater benefits. J. Ahima. 2008, 79, 56–57. [Google Scholar]
- Becker, M.Y. Information governance in NHS’s NPfIT: A case for policy specification. Int. J. Med. Inform. 2007, 76, 432–437. [Google Scholar] [CrossRef]
- Jian, W.-S.; Hsu, C.-Y.; Hao, T.-H.; Wen, H.-C.; Hsu, M.-H.; Lee, Y.-L.; Li, Y.-C.; Chang, P. Building a portable data and information interoperability infrastructure-framework for a standard Taiwan electronic medical record template. Comput. Methods Programs Biomed. 2007, 88, 102–111. [Google Scholar] [CrossRef]
- Jensen, P.B.; Jensen, L.J.; Branak, S. Mining electronic health records: Towards better research applications and clinical care. Nature Rev. Genet. 2012, 13, 395–405. [Google Scholar] [CrossRef]
- Machan, C.; Ammenwerth, E.; Schabetsberger, T. Evaluation of the electronic transmission of medical findings from hospitals to practitioners by triangulation. Method Inform. Med. 2006, 45, 225–233. [Google Scholar]
- Anderson, J.G. Social, ethical and legal barriers to E-health. Int. J. Med. Inform. 2007, 76, 480–483. [Google Scholar] [CrossRef]
- Simon, S.R.; Soran, C.S.; Kaushal, R.; Jenter, C.A.; Volk, L.A.; Burdick, E.; Cleary, P.D.; Orav, E.J.; Poon, E.G.; Bates, D.W. Physicians’ use of key functions in electronic health records from 2005 to 2007: A statewide survey. J. Am. Med. Inform. Assn. 2009, 16, 465–470. [Google Scholar] [CrossRef]
- Wright, A.; Soran, C.; Jenter, C.A.; Volk, L.A.; Bates, D.W.; Simon, S.R. Physician attitudes toward health information exchange: Results of a statewide survey. J. Am. Med. Inform. Assn. 2010, 17, 66–70. [Google Scholar] [CrossRef]
- Gadd, C.S.; Ho, Y.-X.; Cala, C.M.; Blakemore, D.; Chen, Q.; Frisse, M.E.; Johnson, K.B. User perspectives on the usability of a regional health information exchange. J. Am. Med. Inform. Assn. 2011, 18, 711–716. [Google Scholar] [CrossRef]
- Rylance, G. Privacy, dignity, and confidentiality: Interview study with structured questionnaire. Brit. Med. J. 1999, 318. [Google Scholar] [CrossRef]
- Whiddett, R.; Hunter, I.; Engelbrecht, J.; Handy, J. Patients’ attitudes towards sharing their health information. Int. J. Med. Inform. 2006, 75, 530–541. [Google Scholar] [CrossRef]
- Dey, A.; Reid, B.; Godding, R.; Campbell, A. Perceptions and behaviour of access of the internet: A study of women attending a breast screening service in Sydney. Int. J. Med. Inform. 2008, 77, 24–32. [Google Scholar] [CrossRef]
- Nazi, K.M. Veterans’ voices: Use of the American customer satisfaction index (ACSI) survey to identify my healthevet personal health record users’ characteristics, needs, and preferences. J. Am. Med. Inform. Assn. 2010, 17, 203–211. [Google Scholar] [CrossRef]
- Nambisan, P. Information seeking and social support in online health communities: Impact on patients’ perceived empathy. J. Am. Med. Inform. Assn. 2011, 18, 298–304. [Google Scholar] [CrossRef]
- Wen, L.M.; Rissel, C.; Baur, L.A.; Lee, E.; Simpson, J.M. Who is not likely to access the internet for health information? Findings from first-time mothers in southwest Sydney, Australia. Int. J. Med. Inform. 2011, 80, 406–411. [Google Scholar] [CrossRef]
- Lim, S.; Xue, L.S.; Yen, C.C.; Chang, L.; Chan, H.C.; Tai, B.C.; Duh, H.B.L.; Choolani, M. A study on Singaporean women’s acceptance of using mobile phones to seek health. Int. J. Med. Inform. 2011, 80, e189–e202. [Google Scholar] [CrossRef]
- Willison, D.J.; Schwartz, L.; Abelson, J.; Charles, C.; Swinton, M.; Northrup, D.; Thabane, L. Alternatives to project-specific consent for access to personal information for health research: What is the opinion of the Canadian public? J. Am. Med. Inform. Assn. 2007, 14, 706–712. [Google Scholar] [CrossRef]
- Hoerbst, A.; Kohl, C.D.; Knaup, P.; Ammenwerth, E. Attitudes and behaviors related to the introduction of electronic health records among Austrian and German citizens. Int. J. Med. Inform. 2010, 79, 81–89. [Google Scholar] [CrossRef]
- Perera, G.; Holbrook, A.; Thabane, L.; Foster, G.; Willison, D.J. Views on health information sharing and privacy from primary care practices using electronic medical records. 2011, 80, 94–101. [Google Scholar]
- Sweeney, L. K-anonymity: A model for protecting privacy. Int. J. Unc. Fuzz. Knowl. Based Syst. 2002, 10, 557–570. [Google Scholar] [CrossRef]
- Sweeney, L. Achieving k-anonymity privacy protection using generalization and suppression. Int. J. Unc. Fuzz. Knowl. Based Syst. 2002, 10, 571–588. [Google Scholar] [CrossRef]
- Malin, B.; Sweeney, L. How (not) to protect genomic data privacy in a distributed network: Using trail re-identification to evaluate and design anonymity protection systems. J. Biomed. Inform. 2004, 37, 179–192. [Google Scholar] [CrossRef]
- Uzuner, O.; Luo, Y.; Szolovits, P. Evaluating the state-of-the-art in automatic de-identification. J. Am. Med. Inform. Assn. 2007, 14, 550–563. [Google Scholar] [CrossRef]
- Halpern, S.D.; Asch, D.A.; Shaked, A.; Stock, P.G.; Blumberg, E. Standard definitions: Final dispositions of case codes and outcome rates for surveys. Am. J. Trans. 2005, 5, 1319–1325. [Google Scholar] [CrossRef]
- Lovis, C.; Spahni, S.; Cassoni, N.; Geissbuhler, A. Comprehensive management of the access to the electronic patient record: Towards trans-institutional networks. Int. J. Med. Inform. 2007, 76, 466–470. [Google Scholar] [CrossRef]
- Nakashima, N.; Kobayashi, K.; Inoguchi, T.; Daisuke, N.; Naomi, T.; Hiromi, N.; Akihiko, H.; Hidehisa, S.; Ryoichi, T.; Hajime, N. A Japanese model of disease management. Stud. Health Technol. Inform. 2007, 129, 1174–1178. [Google Scholar]
- Link, M.W.; Battaglia, M.P.; Frankel, M.R.; Osborn, L.; Mokdad, A.H. A comparison of address-based sampling (ABS) vs. random-digit dialing (RDD) for general population surveys. Public Opin. Q. 2008, 72, 6–27. [Google Scholar] [CrossRef]
- 2012 Commonwealth Fund International Survey of Primary Care Doctors. Available online: http://www.commonwealthfund.org/Surveys/2012/Nov/2012-International-Survey.aspx (accessed on 20 March 2014).
- Japan Association of Healthcare Information System Industry. Order Entry and Electronic Medical Record Installation Survey 2012 version. Available online: http://www.jahis.jp/members/data_list/data0204/ (accessed on 26 March 2014).
Appendix
Questionnaires
- Being able to receive treatment of the same quality at any physician’s office or hospital
- Avoiding duplicated tests and prescriptions01
- Healthcare cost savings
- Receiving an adequate explanation for your disease
- Promotion of collaborative community healthcare
- Provision of a lifelong medical record system
- Contribution to future medical progress
- Access to health care at a nearby hospital
- Establishment of team-based healthcare environment in various medical facilities
- Other
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Kimura, M.; Nakaya, J.; Watanabe, H.; Shimizu, T.; Nakayasu, K. A Survey Aimed at General Citizens of the US and Japan about Their Attitudes toward Electronic Medical Data Handling. Int. J. Environ. Res. Public Health 2014, 11, 4572-4588. https://doi.org/10.3390/ijerph110504572
Kimura M, Nakaya J, Watanabe H, Shimizu T, Nakayasu K. A Survey Aimed at General Citizens of the US and Japan about Their Attitudes toward Electronic Medical Data Handling. International Journal of Environmental Research and Public Health. 2014; 11(5):4572-4588. https://doi.org/10.3390/ijerph110504572
Chicago/Turabian StyleKimura, Michio, Jun Nakaya, Hiroshi Watanabe, Toshiro Shimizu, and Kazuyuki Nakayasu. 2014. "A Survey Aimed at General Citizens of the US and Japan about Their Attitudes toward Electronic Medical Data Handling" International Journal of Environmental Research and Public Health 11, no. 5: 4572-4588. https://doi.org/10.3390/ijerph110504572