1. Introduction
Demographic structures change as society changes. Developed countries worldwide are experiencing aging problems. Statistics by the Ministry of Interior, Executive Yuan of the R.O.C. (Republic of China, Taiwan) revealed that the senior citizen population was 7% of the total population in Taiwan in 1993. Taiwan has become an aging society, as defined by the World Health Organization. This percentage reached 10.9% at the end of 2011, and the aging index increased from 42.3% to 72.2%. The population aged 65 or older is estimated to exceed 20% by 2026. Taiwan would then become a super-aged society. In addition, the senior citizen population is estimated to be 36.97% of the total population by 2051; in other words, one senior citizen aged 65 or older for every three citizens.
With the phenomenon of the aging of the population, some crucial issues with seeking medical services have been emerged, including emergency medical care, life care when physical and mental functions are lost, chronic diseases, and so on. These care issues have revealed the increasing demands of long-term care and senior health management. Telhealth is considered one possible solution to answer these demands by providing cost-effective care through the use of information technology and biomedical technology.
Under the promotion of the National Information Infrastructure (NII), Executive Yuan, R.O.C. (Taiwan), Taiwan’s government has accumulated experience in implementing Telemedicine/Telecare/Telehealth Policy for more than 10 years with focus in supporting people living in offshore islands and mountain areas. Since 1995 the Department of Health, Executive Yuan, R.O.C. (Taiwan) has been promoting Telemedicine Pilot Program to remedy the problem of inadequate medical resources in rural area. The applications of Telemedicine can be categorized into three areas—Teleconsultation, Telediagnosis and Teleeducation. Since 2007 the Department of Health has commissioned Information and Communications Laboratories, Industrial Technology Research Institute to develop Telecare Pilot Program. It is aimed at developing Community-based, Home-based, Institution-based Telecare service models and their application systems with user-friendly human/machine interface through introduction and application of the information and communication technology, thus further establishing Telecare Information Integration Platform. In 2008 Telecare Quality and Service Improvement Program was launched. An integrated and continual network of Telemedicine was developed based upon two original telemedicine models consisting of Home/Community-based and Institution-based models. Meanwhile Ministry of Economic Affairs began to launch two famous telehealth projects. The M-care project, which was one of Mobile Taiwan Applications promotion projects (M-Taiwan), was one of the initial telehealth projects in 2006. The purpose of this project was to deliver health care into remote country to improve residents’ health. In 2007 the U-Care project was launched. The scope of this project was to integrate various industries to create a valuable and innovative business model of telehealth care service. Owing to the advantages of telecommunication technology and medical care, the Taiwanese government in 2008 included telecare and telehealth as a development project in the emerging service industry [
1].
The R.O.C. government is promoting relevant health care plans to resolve the weakening care-giving capability of families from the increase of nuclear family, which is made up of the parents and their children, and to manage increasing demands for long-term health care services in an aging society. Information technology (IT) has gradually been integrated into health care services. For residents in rural areas, resources in the community may be effectively combined with medical care and localized through community-based telecare services, helping people self-monitor their physiological conditions and develop healthy behaviors.
Telemedicine has been defined as the electronically transmitted rapid exchange of medical information between sites of clinical practice for the purposes of relief and/or education. Telemedicine includes diagnosis, treatment, monitoring, and education of patients by using systems that allow ready access to expert advice and patient information no matter where the patient or relevant information is located [
2]. That is, telemedicine emphasize the use of information and communication technologies (ICT) to provide clinical services to patients in remote areas, for instance, video conferencing with specialists, remote medical diagnoses, and the digital transmission of medical imaging data. Telecare refers to technology that allows patients to stay safe and independent in their own homes. It is characterized by remote, automatic, and passive monitoring of personal health and safety, and home environment [
3]. These devices include fall detection systems, lifestyle monitoring devices and home videophones. Telehealth refers to the remote exchange of data between a patient (usually at home) and healthcare professionals (at a monitoring center) to assist in the management of an existing long-term condition [
3]. The service scope of telehealth is more broadly than telemedicine and telecare. The service scope of telehealth is more broadly than telemedicine and telecare. It also includes administration and training in addition to clinical services [
4]. Some telehealth programs’ goals now have extended beyond chronic care to include acute care management, health promotion, and disease prevention [
5]. Telehealth allows for such things as remote doctor-patient consultations (telemedicine), remote monitoring of vital signs (e.g., blood pressure), and health education services. The use of telehealth that can facilitate the assessment of symptoms reported by patients themselves, may enhance effective symptom management in medical care and provide a means to overcome identified barriers to home care, improving the patients’ experience of care [
6]. The purpose of target systems of this currently study is not only to provide the rural residents with remote clinical services, but also self-management of health and disease prevention. To avoid confusion, this study will use the term telehealth throughout the whole article.
The Technology Acceptance Model (TAM) has been found more favorable in many studies [
7]. Many studies of TAM have confirmed its robustness and reliability to predict and explain IS acceptance behavior [
8]. Some studies have also utilized TAM to investigate patients’ adoption of healthcare information systems and found that TAM provides an appropriate theoretical basis [
1,
9,
10,
11]. Despite the widespread use of TAM in practice, little attention is paid to extending TAM to better understand the adoption of telehealth systems. Davis [
12] also proposed that additional factors should be added to the TAM based on the study context. Specially, the goal of telehealth is to extend medical services provided by remote hospitals and to provide early diagnosis and early treatment through patients’ self-management of health. Telehealth is not only an innovative information system, but also health care delivery systems. Therefore, there is a need for research to expand TAM to include important variables and examine the relationships among those variables and eventual telehealth acceptance behavior.
Social capital refers to the features of social structure, such as networks, norms, and social trust, which facilitate coordination and cooperation for mutual benefits [
13]. Social capital has been proven to be critical for maintaining population health [
14]. In addition, the self-efficacy concept of the social cognitive theory (SCT) of Bandura [
15] has been used to understand the behavior and performance of people in various activities. From an empirical standpoint of computer/information technology context, self-efficacy has been found to be an important determinant of the perceptions of users about such technologies [
16]. Rahimpour
et al. [
10] also suggested system self-efficacy should be critical important in the acceptance of telehealth.
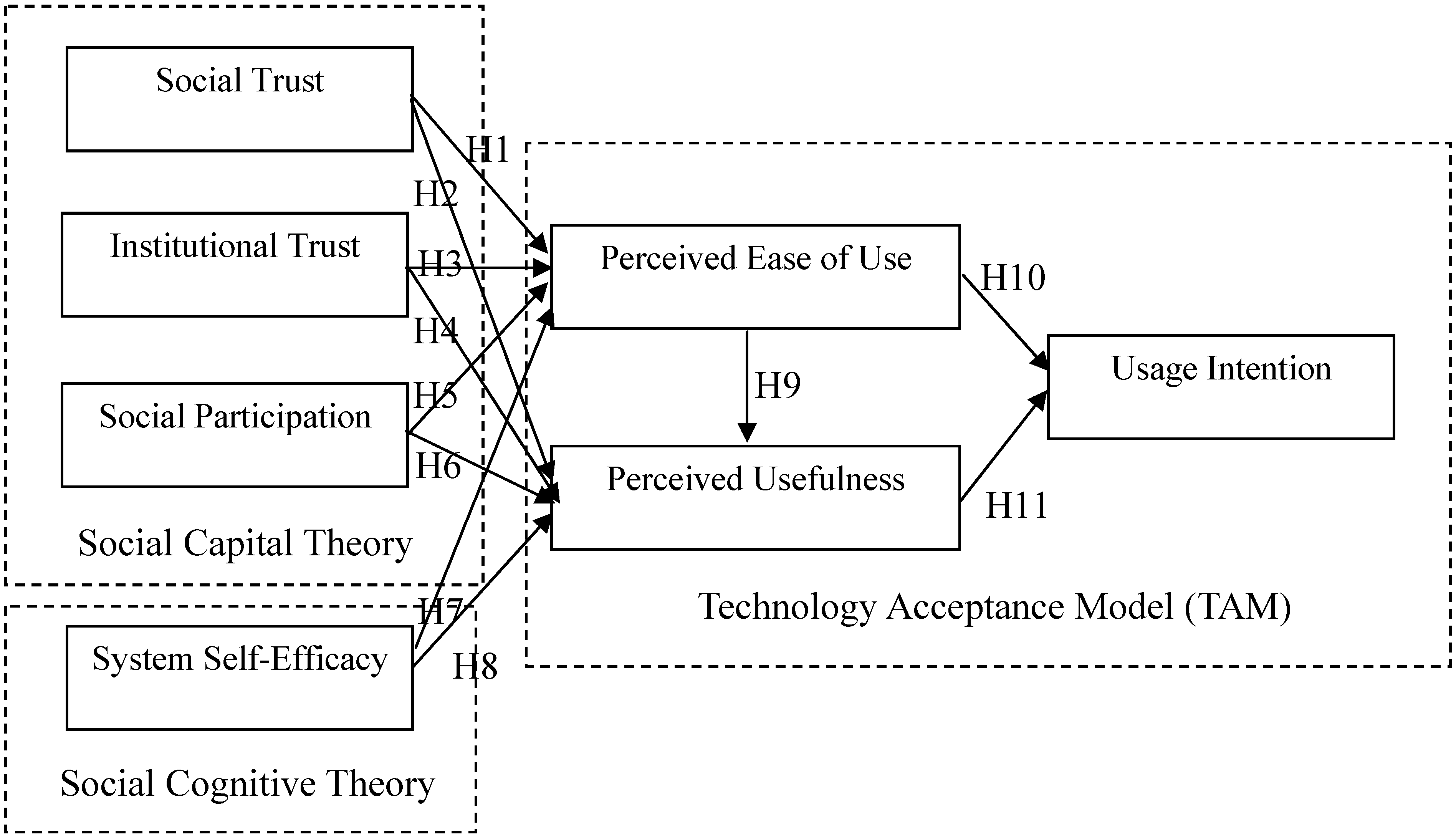
Accordingly, the objective of this study is to integrate the theoretical perspectives of the TAM, social capital theory, and social cognitive theory to theoretically develop and empirically examine the behavioral model of residents in a rural community in using telehealth and to understand the relationships among those crucial factors that affect their behavioral intention of telehealth. Furthermore, the structural equation modeling (SEM) was used to examine the psychometric properties of questionnaires and validate the proposed model and hypotheses. The insights of these findings can be used for the further implementation of telehealth systems and may contribute to the future academic studies in this field.
3. Research Method
3.1. Survey Method and Pretest
We used a self-report questionnaire to examine the proposed research model empirically. A self-report method refers to an approach in which observation data are provided by participants instead of raters or coders. The method is commonly used in behavioral and management science research. The items of measurement used in the questionnaire were developed based on previous studies. Responses to the various variables related to the perceptions of the individual subjects were measured with 5-point Likert-type scales, ranging from 1 (strongly disagree) to 5 (strongly agree).
Figure 1.
The Proposed Research Model.
Figure 1.
The Proposed Research Model.
Following the public explanation session, the residents were arranged to visit the community center and participated in the survey. Before the interview, the researcher, research assistants, and well-trained interviewers introduced the investigation and invited them to participate in the study. The survey subjects of the questionnaire were those residents who were the end users of a telehealth system from Nantou County, Taiwan. All of these end users had used the telehealth system for at least one month. The participants were interviewed in person. The survey questions were read to participants by interviewers in Chinese and they verbalized their answers or wrote down directly on the survey response scale. The interviews lasted for 20 to 30 min.
The telehealth system was developed and installed by a community hospital in Jhushang township, namely Chu Shang Show Chwan Hospital. The overall telehealth system is shown in
Figure 2. It shows that the computer screen with health information system (software) and the peripherals used for physiological recording (hardware).
Figure 2.
The telehealth system.
Figure 2.
The telehealth system.
The hardware includes weight scale, blood pressure cuff, blood glucose meter, and pulse oximeter. The equipment measures vital signs tailored to residents’ clinical needs, such as weight, blood pressure, blood glucose, heart rate, and oxygen saturation.
Before the study, we conducted a pretest to refine and finalize the survey instruments. A pretest was conducted on 20 selected residents of Nantou County, Taiwan. The respondents were provided with verbal and written feedback on individual items after completing the questionnaire. The scale items were modified according to the feedback of these respondents.
3.2. Measurement
The measurement items of the questionnaire in the study were generated from in-depth interviews with senior physicians, nurses, residents who have ever used the telehealth system, and adjusted from the original constructs’ instruments developed by previous studies. The demographic variables include five questions: gender, age, marital status, educational level, and elderly main carer.
Perceived ease of use describes the extent to which a person believes that using the telehealth system will be free of effort. Perceived ease of use was measured with two items which adapted from Davis [
52], Davis, Bagozzi, and Warshaw [
22], and Venkatesh [
49]. A total score ranging from 2 to 10 was obtained by adding the two items. Higher score on the scale were indicative of higher perceived ease of use. The instrument has a high internal consistency (Cronbach’s α = 0.96).
Perceived usefulness is defined as the extent to which a person believes that using the telehealth system will enhance her/his health. Perceived usefulness was measured with three items which adapted from Davis [
52], Davis, Bagozzi, and Warshaw [
22], and Venkatesh [
49]. A total score ranging from 3 to 15 was obtained by adding the three items. Higher score on the scale were indicative of higher perceived usefulness. The instrument has a high internal consistency (Cronbach’s α = 0.99).
Usage intention is the strength of one’s intention to use the telehealth systems. Usage intention was measured with two items which adapted from Davis [
52], Davis, Bagozzi, and Warshaw [
22], and Venkatesh [
49]. A total score ranging from 2 to 10 is obtained by adding the two items. Higher score on the scale are indicative of higher usage intention. The instrument has a high internal consistency (Cronbach’s α = 0.99).
System self-efficacy refers to a belief of one’s capability to use the telehealth systems. System self-efficacy was measured with three items which adapted from Compeau and Higgins [
48], Venkatesh [
49], and Rahimpour
et al. [
10]. A total score ranging from 3 to 15 was obtained by adding the three items. Higher score on the scale were indicative of higher system self-efficacy. The instrument has a high internal consistency (Cronbach’s α = 0.99).
Social trust refers to the expectation that health-care providers will act competently, fairly, openly, and considerately. Social trust was measured with three items which adapted from Mohseni and Lindstrom [
38]. A total score ranging from 3 to 15 was obtained by adding the three items. Higher score on the scale were indicative of higher social trust. The instrument has a high internal consistency (Cronbach’s α = 0.99).
Institutional trust refers to an individual’s trust in the hospital. Institutional trust was measured with three items which adapted from Mohseni and Lindstrom [
38]. A total score ranging from 3 to 15 was obtained by adding the three items. Higher score on the scale were indicative of higher institutional trust. The instrument has a high internal consistency (Cronbach’s α = 0.96).
Social participation describes how actively a person has taken part in social free-time activities. Social participation was measured with three items which adapted from Nummela
et al. [
37]. A total score ranging from 3 to 15 was obtained by adding the three items. Higher score on the scale were indicative of higher social participation. The instrument has a high internal consistency (Cronbach’s α = 0.80).
3.3. Statistical Method
For examining the proposed model empirically, structural equation modeling (SEM) was used to validate the model and hypotheses. SEM is a statistical methodology that involves a confirmatory approach to analyzing a structural theory bearing on a particular phenomenon. Typically, this theory represents “causal” processes that generate observations of multiple variables [
53]. The data analysis proceeded according to the two-step approach recommended by Anderson and Gerbing [
54]. First, the assessment of the measurement model consisting of 10 latent factors included reliability, discriminant validity, and convergent validity of the scales. Second, the structural model was validated individually by considering the series of path relationships linking the 10 constructs.
5. Discussion
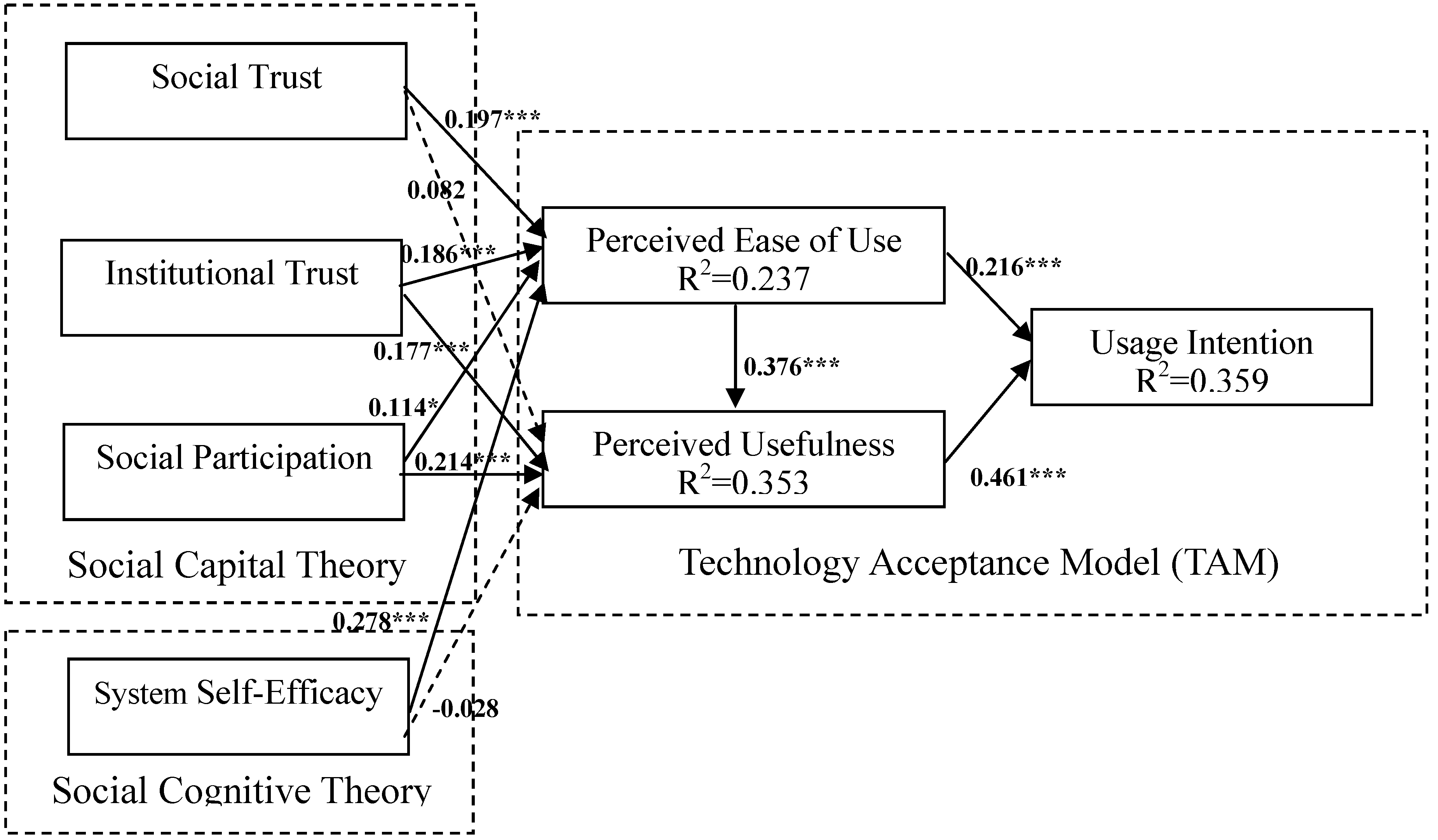
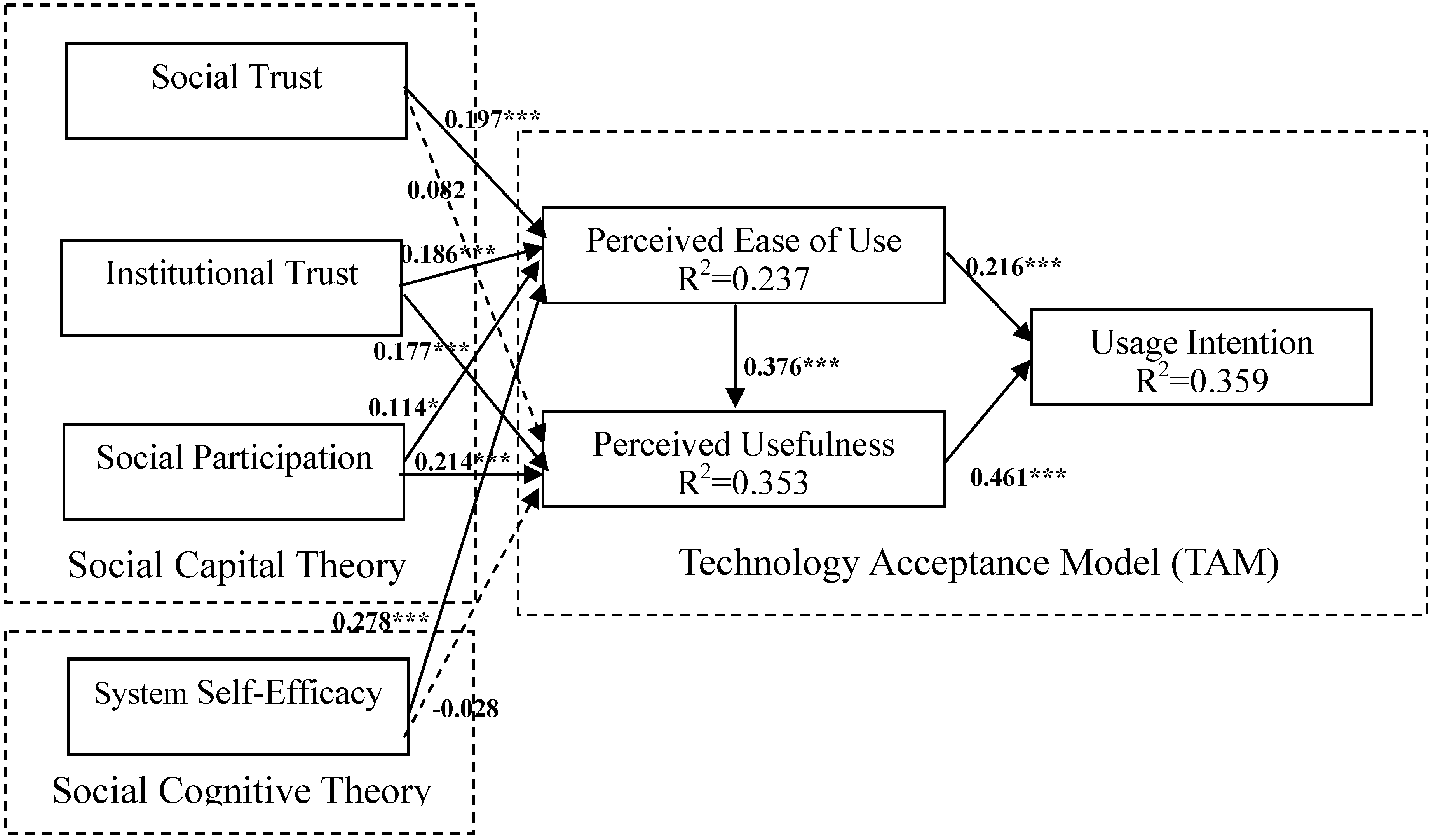
This study investigated the determinants of behavioral intention toward the telehealth acceptance of elderly rural residents in Taiwan by integrating social capital, system self-efficacy, and the TAM. The results strongly support the proposed behavioral model and provide comprehensive understanding of the relationships among social capital (social trust, institutional trust, and social participation), system self-efficacy, technological factors (perceived ease of use and perceived usefulness), and behavioral intention to use this system. Based on the results of SEM, the hypotheses validate the fit of empirical data and the proposed model. The results show that nearly all of the relationships proposed in the model are supported. In addition, the model demonstrated excellent fit and is thus valuable for evaluating and predicting the behavioral intention toward adopting telehealth.
However, social trust affected perceived usefulness nonsignificantly. This unexpected finding can be attributed to the interpersonal trusting climate that may not directly affect the perception of usefulness of people. The effect of social trust on perceived usefulness may be mediated by social participation. Nahapiet and Ghoshal [
32] argued that the relationships of users can strongly influence their willingness to share information in interactive environments, such as social networks or social participation. For example, through “weak ties” and “friends and friends,” network members can acquire privileged access to relevant health information and knowledge, which improves residents’ perception of usefulness toward telehealth systems. Similarly, system self-efficacy affected perceived usefulness nonsignificantly. Consistent with the results provided in Hasan [
8], the effect of system self-efficacy on perceived usefulness was negative (
β = −0.028). One possible explanation is that people exhibiting high system self-efficacy beliefs may be able to identify the limitations of telehealth systems that may not be immediately obvious to those exhibiting low efficacy beliefs [
60].
The results of this study indicate that the elderly rural residents generally reported positive perceptions toward ease of use, usefulness, and intention to use the telehealth system. Moreover, perceived usefulness was the most significantly direct antecedent of behavioral intention. This result is consistent with that presented in Liu, Tsai, and Jang [
9], who focused on the acceptance of patients toward a web-based personal health record system. Therefore, the empirical finding of the current study indicates that the elderly rural residents valued the benefits derived from the telehealth system. In addition, Davis, Bagozzi, and Warshaw [
22] also found that users would adopt a new IT system if they perceived the system to be useful, even if they disliked it. In other words, how to provide elderly rural residents with independence, security, confidence, quality of life, and the ability to remain in their own homes is considerably crucial in developing telehealth systems [
3]. In addition, further investment is necessary to manage the infrastructure to support and sustain the use of such technologies to ensure their safety, security, and reliability [
6].
The findings of this study also imply that social capital factors play a key role in perceived ease of use and perceived usefulness. Accordingly, some practices can increase social trust by encouraging interpersonal interactions of residents through, for example, religious communities, sports or dancing clubs, formal or informal meetings, and activities that facilitate the flow of affection within a community. In addition, to improve institutional trust, cultivating equality and a partnership in the doctor-patient relationship is crucial. Health service providers expressing their willingness to refer to and respect patients’ feelings, opinions, and self-knowledge is critical. Social participation encourages the attachment of people in public (
i.e., community identity). Kwak, Shah, and Holbert [
61] demonstrated that various forms of social associations may strongly contribute to the community participation of people. Developing social associations is essential, because people with stronger psychological ties to their communities are more active in telehealth usage.
In addition, the findings of this study suggest that system self-efficacy significantly affect ease of use perception. The training courses aimed at improving the system self-efficacy of end users could cause increased user acceptance [
16]. In introductory telehealth presentations or training programs, no requirement to possess any knowledge on the telehealth system must be emphasized [
10]. Thus, successfully deploying this innovation requires more than merely installing the equipment. The role of specialists and community nurses is vital, because the telehealth system is used to enhance health services for rural residents [
3]. Local service professionals and remote call centers should provide real-time support cooperatively to users when they encounter any obstacles during operating processes. These proactive design interventions may maximize the acceptance of rural residents to use the technology and promote its effective diffusion [
10].
In this study, behavioral intention was used as dependent variable instead of actual usage behavior. Future studies that incorporate actual telehealth usage into the research model would enable a more comprehensive examination of the integrative model in explaining or predicting telehealth acceptance by residents.
6. Conclusions
This study integrated two sociopsychological theories, social capital theory and social cognitive theory, with a widely used IS technology acceptance model (i.e., the TAM) to provide a comprehensive behavioral model for understanding elderly rural residents’ intention toward using telehealth systems. The framework was extended from the original TAM by considering the relationships among social capital factors (social trust, institutional trust, and social participation), technological factors (perceived ease of use and perceived usefulness), social cognitive factors (system self-efficacy), and behavioral intention to use the system. The proposed model has been proven to be valuable for evaluating and predicting the behavioral intention of telehealth system because it provides an integrative perspective that prompts researchers and practitioners to pay attention to the interdependence of these aspects. The integrative psychosocial-technological viewpoint implies that hospital managers should consider these key factors simultaneously.
Recently, small sample sizes (typically less than 100) have limited the generalizability of most previous telemedicine/telecare/telehealth studies, causing barriers to knowledge development in the telemedicine/telecare/telehealth area [
62]. The large sample size of the current empirical study (365 respondents) can overcome methodological concerns of generalizability and provide valuable insights into the innovative technology development.
The delivery of health care is being transformed by advances in e-health and by an empowered, computer-literate public. However, interactive IS developed for both patients and physicians remain at the early stages of development [
9]. This study could be a useful foundation for exploring the implementation of telehealth systems in Taiwan. Future research could continue to explore other factors that influence decisions for adopting telehealth systems. We believe that the proposed integrated model will provide valuable and informative contributions to practitioners and scholars.



{kind=link}
{kind=link}
{kind=link}