Oxidative Stress of Office Workers Relevant to Tobacco Smoking and Inner Air Quality

Abstract
:1. Introduction
2. Methods
2.1. Study Subjects and Data Collection
2.2. Urine Sample Analysis
2.3. Statistical Analysis
3. Results
3.1. urinary Cotinine and 8-OHdG of All Subjects

{kind=link}
| Smoking status | Females | Males | All | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Means (SD a) | N | Means (SD a) | p-value | N | Means (SD a) | |||||||
| Cotinine (μg/g creatinine) | |||||||||||||
| Non-smoker | 270 | 2.36 (1.29) | 41 | 2.57 (1.60) | 0.346 | 311 | 2.39 (1.33) | ||||||
| Ex-smoker | 10 | 3.90 (1.37) | 23 | 4.34 (2.34) | 0.586 | 33 | 4.21 (2.08) | ||||||
| Smoker | 20 | 13.7 (6.38) | 25 | 12.3 (4.75) | 0.397 | 45 | 12.9 (5.51) | ||||||
| Total | 300 | 3.17 (3.49) | 89 | 5.76 (5.11) | <0.001 | 389 | 3.76 (4.06) | ||||||
| p-value | <0.001 | <0.001 | <0.001 | ||||||||||
| 8-OHdG (μg/g creatinine) | |||||||||||||
| Non-smoker | 270 | 5.07 (2.88) | 41 | 5.08 (2.56) | 0.963 | 311 | 5.08 (2.84) | ||||||
| Ex-smoker | 10 | 5.65 (2.85) | 23 | 6.05 (2.76) | 0.705 | 33 | 5.93 (2.75) | ||||||
| Smoker | 20 | 11.3 (3.39) | 25 | 10.6 (3.49) | 0.534 | 45 | 10.9 (3.96) | ||||||
| Total | 300 | 5.51 (3.39) | 89 | 6.88 (3.71) | 0.001 | 389 | 5.81 (3.53) | ||||||
| p-value | <0.001 | <0.001 | <0.001 | ||||||||||

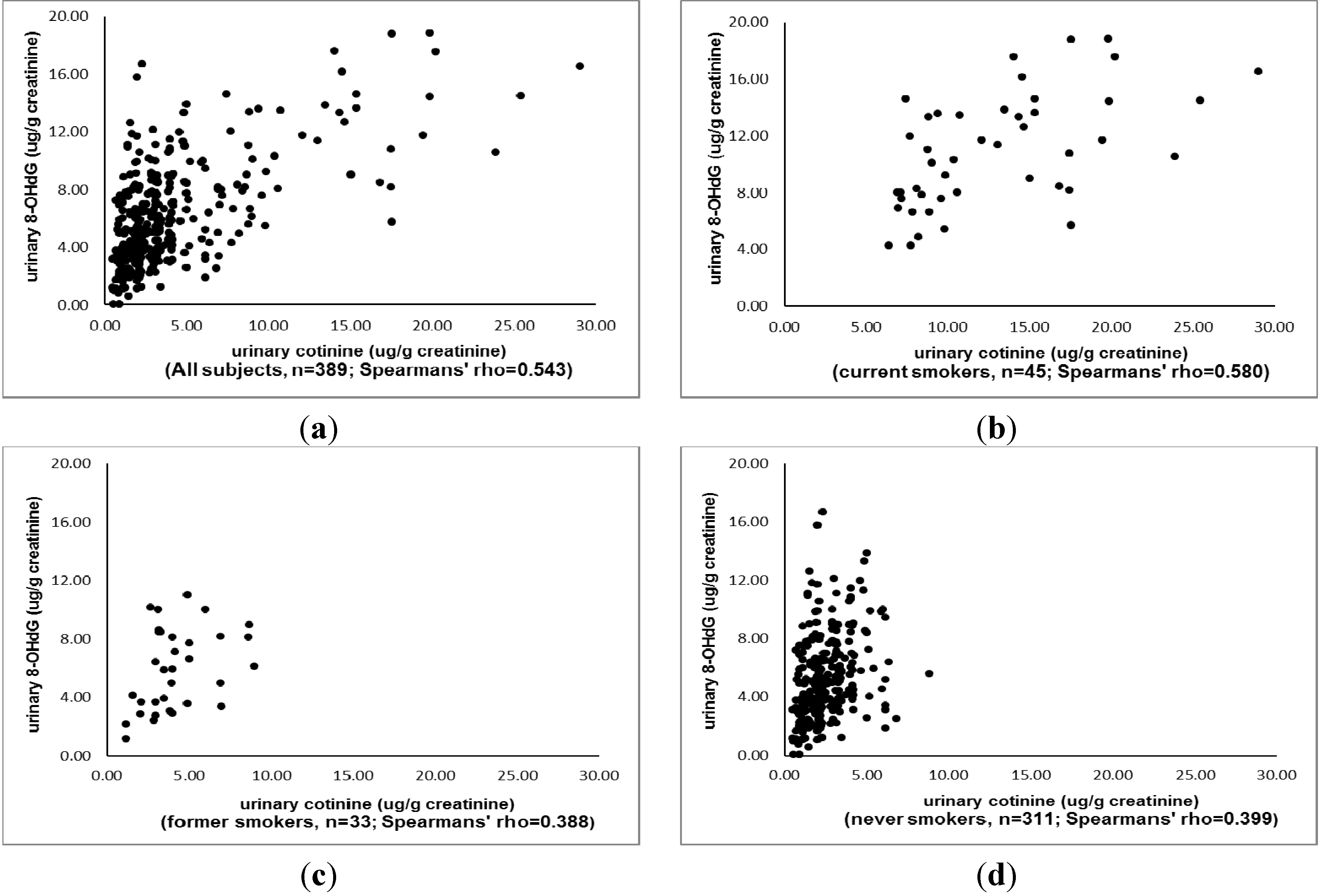
3.2. The Association between Urinary 8-Ohdg and Cotinine
| Variables (n) | Odds Ratio (95% confidence interval) |
|---|---|
| Age, years old | |
| <29 (101) | 1.0 |
| 30–39 (168) | 0.76 (0.42, 1.38) |
| 40–49 (62) | 0.85 (0.40, 1.83) |
| 50+ (58) | 1.21 (0.54, 2.68) |
| Gender | |
| Female (300) | 1.0 |
| Male (89) | 0.96 (0.47, 1.93) |
| Indoor temperature, °C | |
| ≤24 (239) | 1.0 |
| >24 (150) | 0.51 (0.24, 1.09) |
| Relative humidity, % | |
| ≤60 (322) | 1.0 |
| >60 (67) | 0.57 (0.24, 1.33) |
| CO2, ppm | |
| <600 (47) | 1.0 |
| 600–1000 (193) | 3.38 (1.24, 9.23) |
| >1000 (149) | 4.28 (1.12, 16.4) |
| VOCs, ppb | |
| ≤500 (294) | 1.0 |
| >500 (95) | 1.80 (0.82, 3.95) |
| Smoking status | |
| Never (311) | 1.0 |
| Former (33) | 0.91 (0.34, 2.43) |
| Current (45) | 5.30 (1.30, 21.5) |
| Urine cotinine level, μg/g creatinine | |
| ≤1.55 (98) | 1.0 |
| 1.56–2.32 (95) | 0.95 (0.48, 1.89) |
| 2.33–3.98 (96) | 3.30 (1.67, 6.54) |
| >3.98 (100) | 6.66 (2.80, 15.8) |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Smith, M.A.; Perry, G.; Richey, P.L.; Sayre, L.M.; Anderson, V.E.; Beal, M.F.; Kowall, N. Oxidative damage in Alzheimer’s. Nature 1996, 382, 120–121. [Google Scholar]
- Azad, N.; Rojanasakul, Y.; Vallyathan, V. Inflammation and lung cancer: Roles of reactive oxygen/nitrogen species. J. Toxicol. Environ. Health B Crit. Rev. 2008, 11, 1–15. [Google Scholar] [CrossRef]
- Eleuteri, E.; Magno, F.; Gnemmi, I.; Carbone, M.; Colombo, M.; la Rocca, G.; Anzalone, R.; Tarro Genta, F.; Zummo, G.; di Stefano, A.; et al. Role of oxidative and nitrosative stress biomarkers in chronic heart failure. Front. Biosci. 2009, 14, 2230–2237. [Google Scholar]
- Thorne, D.; Wilson, J.; Kumaravel, T.S.; Massey, E.D.; McEwan, M. Measurement of oxidative DNA damage induced by mainstream cigarette smoke in cultured NCI-H292 human pulmonary carcinoma cells. Mutat. Res. 2009, 673, 3–8. [Google Scholar] [CrossRef]
- Valavanidis, A.; Vlachogianni, T.; Fiotakis, K. Tobacco smoke: Involvement of reactive oxygen species and stable free radicals in mechanisms of oxidative damage, carcinogenesis and synergistic effects with other respirable particles. Int. J. Environ. Res. Public Health 2009, 6, 445–462. [Google Scholar] [CrossRef]
- Babizhayev, M.A.; Yegorov, Y.E. Smoking and health: Association between telomere length and factors impacting on human disease, quality of life and life span in a large population-based cohort under the effect of smoking duration. Fundam. Clin. Pharmacol. 2011, 25, 425–442. [Google Scholar] [CrossRef]
- Cataldo, J.K.; Prochaska, J.J.; Glantz, S.A. Cigarette smoking is a risk factor for Alzheimer’s Disease: An analysis controlling for tobacco industry affiliation. J. Alzheimers Dis. 2010, 19, 465–480. [Google Scholar]
- Hammadeh, M.E.; Hamad, M.F.; Montenarh, M.; Fischer-Hammadeh, C. Protamine contents and P1/P2 ratio in human spermatozoa from smokers and non-smokers. Hum. Reprod. 2010, 25, 2708–2720. [Google Scholar] [CrossRef]
- Valavanidis, A.; Vlachogianni, T.; Fiotakis, C. 8-Hydroxy-2'-deoxyguanosine (8-OHdG): A critical biomarker of oxidative stress and carcinogenesis. J. Environ. Sci. Health Part C 2009, 27, 120–139. [Google Scholar] [CrossRef]
- Erhola, M.; Toyokuni, S.; Okada, K.; Tanaka, T.; Hiai, H.; Ochi, H.; Uchida, K.; Osawa, T.; Nieminen, M.M.; Alho, H.; et al. Biomarker evidence of DNA oxidation in lung cancer patients: Association of urinary 8-hydroxy-2-deoxyguanosine excretion with radiotherapy, chemotherapy, and response to treatment. FEBS Lett. 1997, 409, 287–291. [Google Scholar] [CrossRef]
- Shen, J.; Deininger, P.; Hunt, J.D.; Zhao, H. 8-Hydroxy-2'-deoxyguanosine (8-OH-dG) as a potential survival biomarker in patients with nonsmall-cell lung cancer. Cancer 2007, 109, 574–580. [Google Scholar] [CrossRef]
- Du, Y.; Wooten, M.C.; Wooten, M.W. Oxidative damage to the promoter region of SQSTM1/p62 is common to neurodegenerative disease. Neurobiol. Dis. 2009, 35, 302–310. [Google Scholar] [CrossRef]
- Kim, J.Y.; Mukherjee, S.; Ngo, L.C.; Christiani, D.C. Urinary8-hydroxy-2'-deoxyguanosine as a biomarker of oxidative DNA damage in workers exposed to fine particulates. Environ. Health Perspect. 2004, 112, 666–671. [Google Scholar] [CrossRef]
- Toraason, M.; Butler, M.A.; Ruder, A.; Forrester, C.; Taylor, L.; Ashley, D.L.; Mathias, P.; Marlow, K.L.; Cheever, K.L.; Krieg, E.; et al. Effect of perchloroethylene, smoking, and race on oxidative DNA damage in female dry cleaners. Mutat. Res. 2003, 539, 9–18. [Google Scholar] [CrossRef]
- Nuernberg, A.M.; Boyce, P.D.; Cavallari, J.M.; Fang, S.C.; Eisen, E.A.; Christiani, D.C. Urinary 8-isoprostane and 8-OHdG concentrations in boilermakers with welding exposure. J. Occup. Environ. Med. 2008, 50, 182–189. [Google Scholar] [CrossRef]
- Ke, Y.; Cheng, J.; Zhang, Z.; Zhang, R.; Zhang, Z.; Shuai, Z.; Wu, T. Increased levels of oxidative DNA damage attributable to cooking-oil fumes exposure among cooks. Inhal. Toxicol. 2009, 21, 682–687. [Google Scholar]
- Han, Y.Y.; Donovan, M.; Sung, F.C. Increased urinary 8-hydroxy-2'-deoxyguanosine excretion in long-distance bus drivers in Taiwan. Chemosphere 2010, 79, 942–948. [Google Scholar] [CrossRef]
- Ren, C.; Fang, S.; Wright, R.O.; Suh, H.; Schwartz, J. Urinary 8-hydroxy-2'-deoxyguanosine as a biomarker of oxidative DNA damage induced by ambient pollution in the Normative Aging Study. Occup. Environ. Med. 2011, 68, 562–569. [Google Scholar] [CrossRef]
- Wang, T.C.; Song, Y.S.; Wang, H.; Zhang, J.; Yu, S.F.; Gu, Y.E.; Chen, T.; Wang, Y.; Shen, H.Q.; Jia, G. Oxidative DNA damage and global DNA hypomethylation are related to folate deficiency in chromate manufacturing workers. J. Hazard. Mater. 2012, 213–214, 440–446. [Google Scholar] [CrossRef]
- Harman, S.M.; Liang, L.; Tsitouras, P.D.; Gucclardo, F.; Heward, C.B.; Reaven, P.D.; Ping, W.; Ahmed, A.; Cutler, R.G. Urinary excretion of three nucleic acid oxidation adducts and isoprostane f2α measured by liquid chromatographymass spectrometry in smokers, ex-smokers, and nonsmokers. Free Radic. Biol. Med. 2003, 35, 1301–1309. [Google Scholar] [CrossRef]
- Asami, S.; Manabe, H.; Miyake, J.; Tsurudome, Y.; Hirano, T.; Yamaguchi, R.; Itoh, H.; Kasai, H. Cigarette smoking induces an increase in oxidative DNA damage, 8-hydroxydeoxyguanosine, in a central site of the human lung. Carcinogenesis 1997, 18, 1763–1766. [Google Scholar] [CrossRef]
- Campos, C.; Guzman, R.; Lopez-Fernandez, E.; Casado, A. Urinary biomarkers of oxidative/nitrosative stress in healthy Smokers. Inhal. Toxicol. 2011, 23, 148–156. [Google Scholar]
- Yano, T.; Shoji, F.; Baba, H.; Koga, T.; Shiraishi, T.; Orita, H.; Kohno, H. Significance of the urinary 8-OHdG level as an oxidative stress marker in lung cancer patients. Lung Cancer 2009, 63, 111–114. [Google Scholar]
- Nagano, T.; Shimizu, M.; Kiyotani, K.; Kamataki, T.; Takano, R.; Murayama, N.; Shono, F.; Yamazaki, H. Biomonitoring of urinary cotinine concentrations associated with plasma levels of nicotine metabolites after daily cigarette smoking in a male Japanese population. Int. J. Environ. Res. Public Health 2010, 7, 2953–2964. [Google Scholar] [CrossRef]
- Lu, C.Y.; Ma, Y.C.; Lin, J.M.; Chuang, C.Y.; Sung, F.C. Oxidative DNA damage estimated by urinary 8-hydroxydeoxyguanosine and indoor air pollution among non-smoking office employees. Environ. Res. 2007, 103, 331–337. [Google Scholar] [CrossRef]
- Apte, M.G.; Fisk, W.J.; Daisey, J.M. Associations between indoor CO2 concentrations and sick building syndromes in U.S. office buildings: An analysis of the 1994–1996 BASE study data. Indoor Air 2000, 10, 246–247. [Google Scholar]
- Benowitz, N.L. Cotinine as a biomarker of environmental tobacco smoke exposure. Epidemiol. Rev. 1996, 18, 188–203. [Google Scholar] [CrossRef]
- Haufroid, V.; Lison, D. Urinary cotinine as a tobacco-smoke exposure index: A minireview. Int. Arch. Occup. Environ. Health 1998, 71, 162–168. [Google Scholar] [CrossRef]
- Willers, A.; Hein, H.O.; Jansson, L. Assessment of environmental tobacco smoke exposure: Urinary cotinine concentrations in children are strongly associated with the house dust concentrations of nicotine at home. Indoor Air 2004, 14, 83–86. [Google Scholar] [CrossRef]
- Yin, B.; Whyatt, R.M.; Perera, F.P.; Randall, M.C.; Cooper, T.B.; Santella, R.M. Determination of 8-hydroxydeoxyguanosine by an immunoaffinity chromatography-monoclonal antibody-based ELISA. Free Radic. Biol. Med. 1995, 18, 1023–1032. [Google Scholar] [CrossRef]
- Nerurkar, M.K.; Sahasrabudhe, M.B. Synthesis of creatine in x-irradiated rats. Int. J. Radiat. Biol. 1960, 2, 237–246. [Google Scholar] [CrossRef]
- Morita, H.; Ikeda, H.; Haramaki, N.; Eguchi, H.; Imaizumi, T. Only two-weeksmoking cessation improves platelet aggregability and intraplatelet redox imbalance of long-term smokers. J. Am. Coll. Cardiol. 2005, 45, 589–594. [Google Scholar] [CrossRef]
- Net of Tobacco Hazards Prevention. Available online: http://tobacco.hpa.gov.tw/Show.aspx?MenuId=547 (accessed on 5 November 2013).
- Matt, G.E.; Quintana, P.J.; Zakarian, J.M.; Fortmann, A.L.; Chatfield, D.A.; Hoh, E.; Uribe, A.M.; Hovell, M.F. When smokers move out and non-smokers move in: Residential thirdhand smoke pollution and exposure. Tob. Contro 2011, 20. [Google Scholar] [CrossRef]
- Chuang, C.Y.; Lee, C.C.; Chang, Y.K.; Sung, F.C. Oxidative DNA damage estimated by urinary 8-hydroxydeoxyguanosine: Influence of taxi driving, smoking and areca chewing. Chemosphere 2003, 52, 1163–1171. [Google Scholar] [CrossRef]
- Commodore, A.A.; Zhang, J.J.; Chang, Y.; Hartinger, S.M.; Lanata, C.F.; Mäusezahl, D.; Gil, A.I.; Hall, D.B.; Aguilar-Villalobos, M.; Vena, J.E.; et al. Concentrations of urinary 8-hydroxy-2'-deoxyguanosine and 8-isoprostane in women exposed to woodsmoke in a cookstove intervention study in San Marcos, Peru. Environ. Int. 2013, 60, 112–122. [Google Scholar] [CrossRef]
- Pan, C.H.; Chan, C.C.; Wu, K.Y. Effects on Chinese restaurant workers of exposure to cooking oil fumes: A cautionary note on urinary 8-hydroxy-2'-deoxyguanosine. Cancer Epidemiol. Biomark. Prev. 2008, 17, 3351–3357. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Lu, C.-Y.; Ma, Y.-C.; Chen, P.-C.; Wu, C.-C.; Chen, Y.-C. Oxidative Stress of Office Workers Relevant to Tobacco Smoking and Inner Air Quality. Int. J. Environ. Res. Public Health 2014, 11, 5586-5597. https://doi.org/10.3390/ijerph110605586
Lu C-Y, Ma Y-C, Chen P-C, Wu C-C, Chen Y-C. Oxidative Stress of Office Workers Relevant to Tobacco Smoking and Inner Air Quality. International Journal of Environmental Research and Public Health. 2014; 11(6):5586-5597. https://doi.org/10.3390/ijerph110605586
Chicago/Turabian StyleLu, Chung-Yen, Yee-Chung Ma, Pei-Chun Chen, Chin-Ching Wu, and Yi-Chun Chen. 2014. "Oxidative Stress of Office Workers Relevant to Tobacco Smoking and Inner Air Quality" International Journal of Environmental Research and Public Health 11, no. 6: 5586-5597. https://doi.org/10.3390/ijerph110605586