The Public Health Impacts of Climate Change in the former Yugoslav Republic of Macedonia


Abstract
:1. Introduction
2. Experimental Section

{kind=link}
| Objectives | Methods Used |
|---|---|
| To assess the health impacts and vulnerability to climate change | Qualitative and quantitative epidemiological methods:
|
| To develop a national health adaptation strategy | Public health approaches supported by:
|
2.1. Health Vulnerability and Impact Assessment ((h)VIA)
| Extreme Events: Heat/Cold | Extreme events: Flood/Drought | Infectious Diseases | Air Pollution/ Allergies and Pollen | |
|---|---|---|---|---|
| Assessment method | Time series analysis and Poisson regression analysis on heat-related mortality in Skopje [15,16]. Excess winter mortality, nationwide (1994–2008) [16]. Scenario based assessment (A1B and A2) [14]. Damage and adaptation costs analysis of heat-waves in Skopje [17]. | Systematic literature reviews by key words: flood, drought, health, climate change, R. Macedonia [16]. Semi-structured Interviews with national key stakeholders. Focus group and action research with stakeholders. | Salmonella human cases time series and Poisson regression analysis (1998–2008) in 5 cities of the former Yugoslav Republic of Macedonia [18]. Scenario based assessment (A1B and A2) [18]. Systematic literature review by key words: mosquito, R. Macedonia, climate change [19]. Field investigation in 6 sites for presence of dengue-mediating mosquitoes [19]. | Regression analyses [20]. Quantifying the onset of flowering, maximum and end of the length of seasons for 9 types of pollen during the vegetation period of 1996–2009 [20]. Quantifying the current and projected future burdens of temperature [20,21]. |
| Data and information sources | Meteorological data (National Hydro-meteorological Institute) Daily counts of deaths (State Statistical Office) Damage and adaptation toolkit software (WHO pilot project) Scenarios developed for the country (22) | Crisis Management Centre Protection and Rescue Directorate Ministry of Environment and Physical Planning | Meteorological data (National Hydro-meteorological Institute) Weekly counts of human Salmonella confirmed cases (National Institute for Public Health) Scenarios developed for the country (22) | Air pollution data (Ministry of Environment and Physical Planning) Meteorological data (National Hydro-meteorological Institute) Daily distribution of 9 pollens (National Institute for Occupational Medicine) |
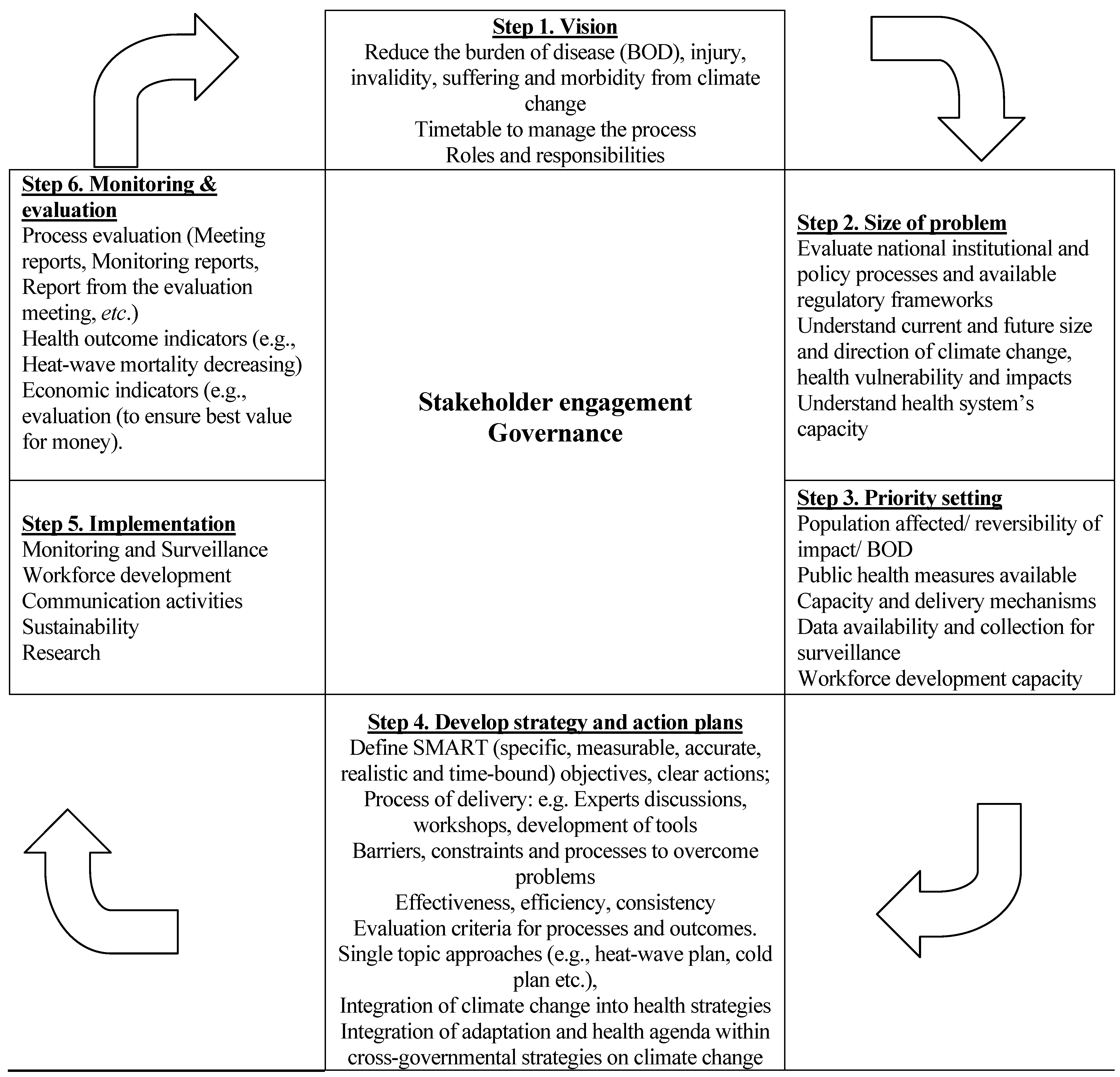
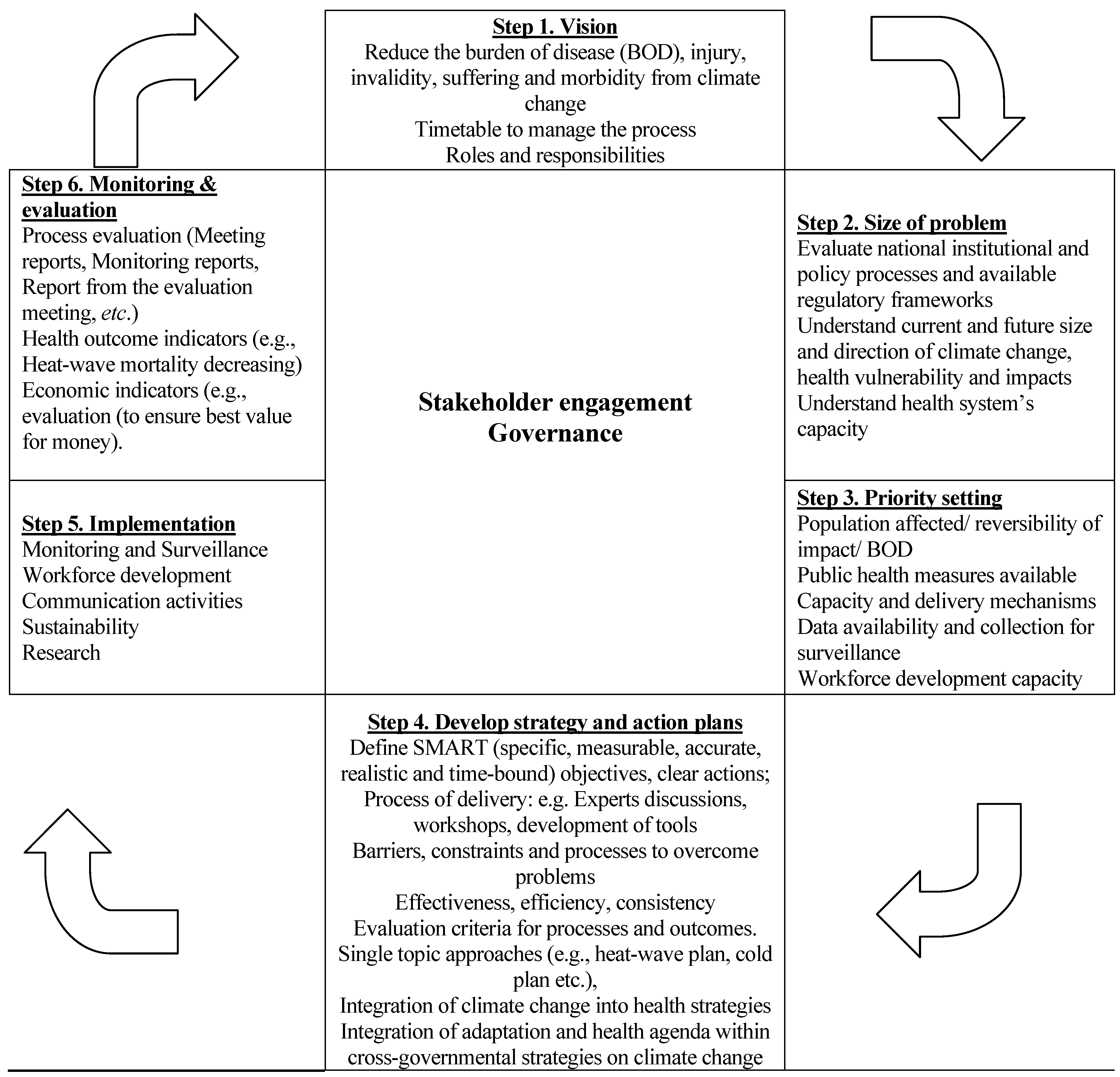
2.2. Health Adaptation Strategy Development Process
3. Results and Discussion
3.1. Results from the (h)VIA
| Climate Sensitive Diseases and Conditions | Impact: Current | Impact: Projected |
|---|---|---|
| Floods/Droughts | Catastrophic floods in past resulted in serious damage to residential areas and infrastructure as well as to the water supply and sewage systems. The weather conditions in 2007 led to one of the most extreme droughts since meteorological records began in the country [16] | Projections indicate that the combined impact of flooding events over the next century will likely affect about 4,050 households in the Skopje valley and about 1,750 households in the Pelagonia valley within the next 100 years Droughts are very likely to increase in number and severity, resulting in loss of agricultural land, with both nutritional and economic consequences [16] |
| Heat/Cold Extreme events | The climatic variables such as mean winter ambient temperature are found to be positively associated with levels of relative excess winter mortality in the country. Hot weather has a stronger impact on human mortality than cold weather. A heat-wave was defined as a period when maximum apparent temperature and minimum temperature are over the ninetieth percentile of the monthly distribution for at least two days. Under heat-wave conditions, an increase of temperature of 1 °C above the heat cut off point for Skopje (30.8 °C) leads to an increase in mortality of 4.8% [13]. Economic analysis of the costs of adaptive action was also performed. This found that the total heat-wave costs were approximately twice those of climate change-attributed costs, at approximately MKD 170million per year, or € 2.6 million [17]. | In a warmer future climate, very likely there will be more intense, more frequent and longer-lasting heat-waves in the country [29]. |
| Infectious diseases | Seasonal patterns of Salmonella infections, with a peak in the summer months after the peak of temperatures were detected. For Skopje, an increase in the weekly temperature of 1 °C above detected threshold of 17.9 °C was associated with a 2.8% increase in salmonellosis cases [18] | The projections showed that the whole Balkan Peninsula in the future is very likely to be suitable for establishment of Aedes albopictus [30]. |
| Air quality | Air pollution may compound the effects of high and low temperature morbidity on daily ambient levels of PM10 (μg/m3) and ozone (μg/m3) [23] | Increase of 10 μg/m3 of PM10 above maximum permitted values (50 μg/ m3) will likely result in increasing the daily admission of patents with cardiovascular diseases in Skopje by 12% [23]. |
| Allergies and pollen distribution | The prevalence of standard pollen allergens in Skopje shows an increase from 16.9% in 1996 to 19.8% in 2009 [20]. Allergic risk increases in 3 main periods: early spring, spring and summer, in which standard pollen allergens are the main cause of allergies during those months [20]. | The impacts of climate change, via increasing temperature in the next decades on aeroallergens, and in particular pollen, will likely include impacts on pollen production and pollen season (onset of flowering, maximum and end of the seasons) [20]. |
3.2. Climate Change Health Adaptation Strategy
- raising awareness of climate change and the effect on health;
- identifying, registering and monitoring risks connected with climate change and their influence on people’s health, and
- improving the health sector’s promotion and prevention activities.
| Climate Sensitive Diseases and Conditions | Adaptation Measures |
|---|---|
| Heat/Cold
Extreme events | National Heat Health Action Plan in place since 2010 as a pilot (evaluated December 2012) [28]. National Cold Health Action Plan endorsed in 2012 [33]. |
| Flood/DroughtExtreme events | Establish an integrated, efficient and effective approach for prevention, early warning, management to overcome the effects of climate change connected to floods and fires [32]; Other plans; Municipality action plans; Flood risk plans; Effective operational strategies to improve irrigation required. |
| Infectious diseases | Strengthening existing epidemiological surveillance, reporting, monitoring and analysis of communicable diseases that are transmitted by water, food and vectors. Education of the general public on the benefits and necessity of: -implementation of adaptation measures such as Hazard Analysis Critical Control Point (HACCP) system; -disinfection and extermination of rats and insects. Undertake preventive disinfection and pest control (extermination of rats and insects) in educational, social and health institutions [32] |
| Air quality/Allergies and pollen | Overcome the climate change health consequences connected with air pollution and cold weather during winter by establishing effective control and specific preventive measures. Continuous pollen monitoring and reporting on the type and concentration of pollen grains in the atmosphere on a daily basis [32]. |
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Disclaimer
References
- McMichael, A.J. Globalization, climate change, and human health. N. England J. Med. 2013, 368, 1335–1343. [Google Scholar] [CrossRef]
- Haines, A.; Kovats, R.S.; Campbell Lendrum, D.; Corvalan, C. Climate change and human health: Impacts, vulnerability and public health. Lancet 2006, 36, 2101–2109. [Google Scholar]
- McMichael, A.J.; Lindgren, E. Climate change: Present and future risks to health, and necessary responses. J. Intern. Med. 2011, 270, 401–413. [Google Scholar] [CrossRef]
- Campbell Lendrum, D.; Woodruff, R. Comparative risk assessment of the burden of disease from climate change. Environ. Health Persp. 2006, 114, 1935–1941. [Google Scholar]
- Managing the Risks of Extreme Events and Disasters to Advance Climate Change Adaptation. Available online: https://www.ipcc.ch/pdf/special-reports/srex/SREX_Full_Report.pdf (accessed on 1 April 2014).
- Hajat, S.; Armstrong, B.; Baccini, M.; Biggeri, A.; Bisanti, L.; Russo, A.; Paldy, A.; Menne, B.; Kosatsky, T. Impact of high temperatures on mortality: Is there an added heat wave effect? Epidemiology 2006, 17, 632–638. [Google Scholar] [CrossRef]
- Garcia-Herrera, R.; Diaz, J.; Trigo, R.M.; Luterbacher, J.; Fischer, E.M. A review of the European summer heat wave of 2003. Crit. Rev. Environ. Sci. Technol. 2010, 40, 267–306. [Google Scholar] [CrossRef]
- Schar, C.; Vidale, P.L.; Luthi, D.; Frei, C.; Haberli, C.; Liniger, M.A.; Appenzeller, C. The role of increasing temperature variability in European summer heat waves. Nature 2004, 427, 332–336. [Google Scholar] [CrossRef]
- World Health Organization (WHO) Regional Office for Europe. Improving Public Health Responses to Extreme Weather/Heat-Waves—EuroHEAT. Technical Summary; WHO Regional Office for Europe: Copenhagen, Denmark, 2009. Available online: http://www.euro.who.int/__data/assets/pdf_file/0010/95914/E92474.pdf (accessed on 26 March 2014).
- Rey, G.; Fouillet, A.; Bessemoulin, P.; Frayssinet, P.; Dufour, A.; Jougla, E.; Hemon, D. Heat exposure and socioeconomic vulnerability as synergistic factors in heat-wave-related mortality. Eur. J. Epidemiol. 2009, 24, 495–502. [Google Scholar] [CrossRef]
- World Health Organization (WHO) Regional Office for Europe. Protecting Health from Climate Change: A Seven-Country Initiative; WHO Regional Office for Europe: Copenhagen, Denmark, 2013; pp. 4–10. Available online: http://www.euro.who.int/__data/assets/pdf_file/0019/215524/PROTECTING-HEALTH-FROM-CLIMATE-CHANGE-A-seven-country-initiative.pdf?ua=1 (accessed on 16 May 2014).
- Ebi, K.; Kovats, S.; Menne, B. An approach for assessing human health vulnerability and public health interventions to adapt to climate change. Environ. Health Persp. 2006, 114, 1930–1934. [Google Scholar]
- Berry, P.; Campbell Lendrum, D.; Corvalan, C.; Guillemot, J. Protecting Health from Climate Change—Vulnerability and Adaptation Assessment; World Health Organization: Geneva, Switzerland, 2013; pp. 6–36. Available online: http://www.who.int/globalchange/publications/vulnerability-adaptation/en/ (accessed on 26 March 2014).
- Kendrovski, V.; Spasenovska, M. The Effects on Health of Climate Change in the Republic of Macedonia. Ministry of Health: Skopje, The former Yugoslav Republic of Macedonia. 2011, pp. 31–76. Available online: http://www.un.org.mk/en-publications-full/items/the-effects-on-health-of-climate-change-in-the-republic-of-macedonia.pdf (accessed on 26 March 2014).
- Kendrovski, V. The impact of ambient temperature on mortality among the urban population in Skopje, Macedonia during the period 1996–2000. BMC Public Health 2006, 6, 1–6. [Google Scholar] [CrossRef]
- Kendrovski, V.; Spasenovska, M.; Memeti, S.; Orovcanec, N.; Hristovska Kisman, M.; Mustafa, Z. Mortality as a function of weather variables: Temperature and humidity in Skopje as Climate change context. Arch. Public Health 2010, 2, 79–84. [Google Scholar]
- Hutton, G.; Sanchez, G.; Menne, B. Climate Change and Health: A Tool to Estimate Health and Adaptation Costs; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2013; pp. 33–35. Available online: http://www.euro.who.int/__data/assets/pdf_file/0018/190404/WHO_Content_Climate_change_health_DruckIII.pdf (accessed on 26 March 2014).
- Kendrovski, V.; Karadzovski, Z.; Spasenovska, M. Ambient maximum temperature as a function of Salmonella food poisoning cases in the Republic of Macedonia. North Am. J. Med. Sci. 2011, 3, 264–267. [Google Scholar]
- Stefkov, G.; Hristovski, S.; Prelik, D.; Gjorgjievska Cvetkovska, A.; Mitev, T. Study on Presence of Aedes Albopictus in the Republic of Macedonia; Ministry of Health: Skopje, Macedonia, 2011; pp. 1–20. [Google Scholar]
- Kendrovski, V.; Milkovska, S.; Bislimovska Karadzinska, J.; Minov, J.; Spasenovska, M.; Hristovska Kisman, M. The impacts of maximum temperature and climate change to current and future pollen distribution in Skopje, Republic of Macedonia. Taf. Prev. Med. Bull. 2012, 11, 35–40. [Google Scholar] [CrossRef]
- Karadzinska Bislimovska, J.; Minov, J.; Kendrovski, V.; Milkovska, S.; Stoleski, S.; Mijakoski, D. Prevalence of the respiratory allergies among adult population in the city of Skopje in relation to climatic change and change in pollen micro flora. JEP 2012, 2, 1364–1372. [Google Scholar] [CrossRef]
- Bergant, K. Climate Change Scenarios for Macedonia, Review of Methodology and Results; University of Nova Gorica: Pristava, Slovenia, 2006. Available online: http://www.seeclimateforum.org%2fupload%2fdocument%2fclimate_change_scenarios_for_macedonia.pdf (accessed on 26 March 2014).
- Kochubovski, M.; Kendrovski, V. Monitoring of the ambient air quality (PM10) in Skopje and evaluation of the health effects in 2010. JEPE 2012, 13, 789–796. [Google Scholar]
- Kovats, R.S.; Edwards, S.J.; Hajat, S.; Armstrong, B.G.; Ebi, K.L.; Menne, B. The effect of temperature on food poisoning: A time-series analysis of salmonellosis in ten European countries. Epidemiol. Infect. 2004, 132, 443–453. [Google Scholar] [CrossRef]
- Semenza, J.C.; Menne, B. Climate change and infectious diseases in Europe. Lancet Infec. Dis. 2009, 9, 365–375. [Google Scholar] [CrossRef]
- Calistri, P.; Giovannini, A.; Hubalek, Z.; Ionescu, A.; Monaco, F.; Savini, G.; Lelli, R. Epidemiology of West Nile in Europe and in the Mediterranean basin. Open Virol. J. 2010, 4, 29–37. [Google Scholar]
- Autochthonous Plasmodium Vivax Malaria in Greece. 2011. Available online: http://www.eurosurveillance.org/images/dynamic/EE/V16N42/art19993.pdf (accessed on 26 March 2014).
- Kendrovski, V.; Karadzovski, Z.; Milenkovic, Z.; Kostovska, J. Climate Change and Communicable Diseases. A Manual for Health Workers of the former Yugoslav Republic of Macedonia; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2013; pp. 4–16. Available online: http://www.euro.who.int/__data/assets/pdf_file/0019/144172/e95095.pdf?ua=1 (accessed on 16 May 2014).
- Kendrovski, V.; Spasenovska, M. Heat-Health Action Plan—To Prevent the Heat Wave Consequences on the Health of the Population in the former Yugoslav Republic of Macedonia. World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2013; pp. 9–46. Available online: http://www.euro.who.int/__data/assets/pdf_file/0020/144173/e95093.pdf (accessed on 26 March 2014).
- Rogers, D.J.; Suk, J.E.; Semenza, J.C. Using global maps to predict the risk of dengue in Europe. Acta Trop. 2014, 129, 1–14. [Google Scholar] [CrossRef]
- Bittner, I.; Matthies, F.; Dalbokova, D.; Menne, B. Are European countries prepared for the next big heat-wave? Eur. J. Public Health. 2013, 4. Available online: http://eurpub.oxfordjournals.org/content/early/2013/10/06/eurpub.ckt121.full.pdf (accessed on 26 March 2014). [CrossRef]
- Kendrovski, V.; Spasenovska, M. Climate Change—Health Adaption Strategy and Action Plan of the former Yugoslav Republic of Macedonia; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2013; pp. 4–35. Available online: http://www.euro.who.int/__data/assets/pdf_file/0018/144171/e95094.pdf (accessed on 26 March 2014).
- Kendrovski, V.; Spasenovska, M. Action Plan for Preventing the Effects of the Waves on the Population in R. Macedonia. Ministry of Health: Skopje, The former Yugoslav Republic of Macedonia, Action Plan for Preventing the Effects of the Waves on the Population in R. Macedonia; Ministry of Health: Skopje, The former Yugoslav Republic of Macedonia, 2012; pp. 3–28. Available online: http://www.studenibranovi.mk/en/downloads/AkcionenPlan_Eng.pdf (accessed on 26 March 2014).
- Frumkin, H.; Hess, J.; Luber, G.; Malilay, J.; McGeehin, M. Climate change: The public health response. Am. J. Public Health. 2008, 98, 435–445. [Google Scholar] [CrossRef]
- Hess, J.; McDowell, J.; Luber, G. Integrating climate change adaptation into public health practice: Using adaptive management to increase adaptive capacity and build resilience. Environ. Health Persp. 2012, 120, 171–179. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Kendrovski, V.; Spasenovska, M.; Menne, B. The Public Health Impacts of Climate Change in the former Yugoslav Republic of Macedonia. Int. J. Environ. Res. Public Health 2014, 11, 5975-5988. https://doi.org/10.3390/ijerph110605975
Kendrovski V, Spasenovska M, Menne B. The Public Health Impacts of Climate Change in the former Yugoslav Republic of Macedonia. International Journal of Environmental Research and Public Health. 2014; 11(6):5975-5988. https://doi.org/10.3390/ijerph110605975
Chicago/Turabian StyleKendrovski, Vladimir, Margarita Spasenovska, and Bettina Menne. 2014. "The Public Health Impacts of Climate Change in the former Yugoslav Republic of Macedonia" International Journal of Environmental Research and Public Health 11, no. 6: 5975-5988. https://doi.org/10.3390/ijerph110605975