Protecting Health from Climate Change in the WHO European Region


 ,
,
Abstract
:1. Introduction
- integrate health issues in all climate change mitigation and adaptation measures, policies and strategies at all levels and in all sectors;
- strengthen health, social welfare and environmental systems and services to improve their response to the impacts of climate change in a timely manner, for example to extreme weather events and heat waves. In particular, we will protect the supply of water and the provision of sanitation and safe food through adequate preventive, preparedness and adaptive measures;
- develop and strengthen early warning surveillance and preparedness systems for extreme weather events and disease outbreaks, for example vector-borne diseases, at the animal-human-ecosystem interface, where appropriate;
- develop and implement educational and public awareness programmes on climate change and health, to encourage healthy, energy-efficient behaviours in all settings and provide information on opportunities for mitigation and adaptation interventions, with a particular focus on vulnerable groups and sub regions;
- collaborate to increase the health sector’s contribution to reducing greenhouse gas emissions and strengthen its leadership on energy- and resource-efficient management and stimulate other sectors, such as the food sector, to do the same;
- encourage research and development, for example with tools for forecasting climate impacts on health, identifying health vulnerability and developing appropriate mitigation and adaptation measures [2].
- assess the current status of Member States regarding activities to mitigate or adapt to climate change;
- identify gaps in the implementation of the Parma commitments;
- provide feedback to European Member States on their action towards protecting health from climate change;
- share experiences and information on best practices in developing and implementing effective adaptation and mitigation measures;
- identify priorities on climate change and health for the next ministerial conference on environment and health.
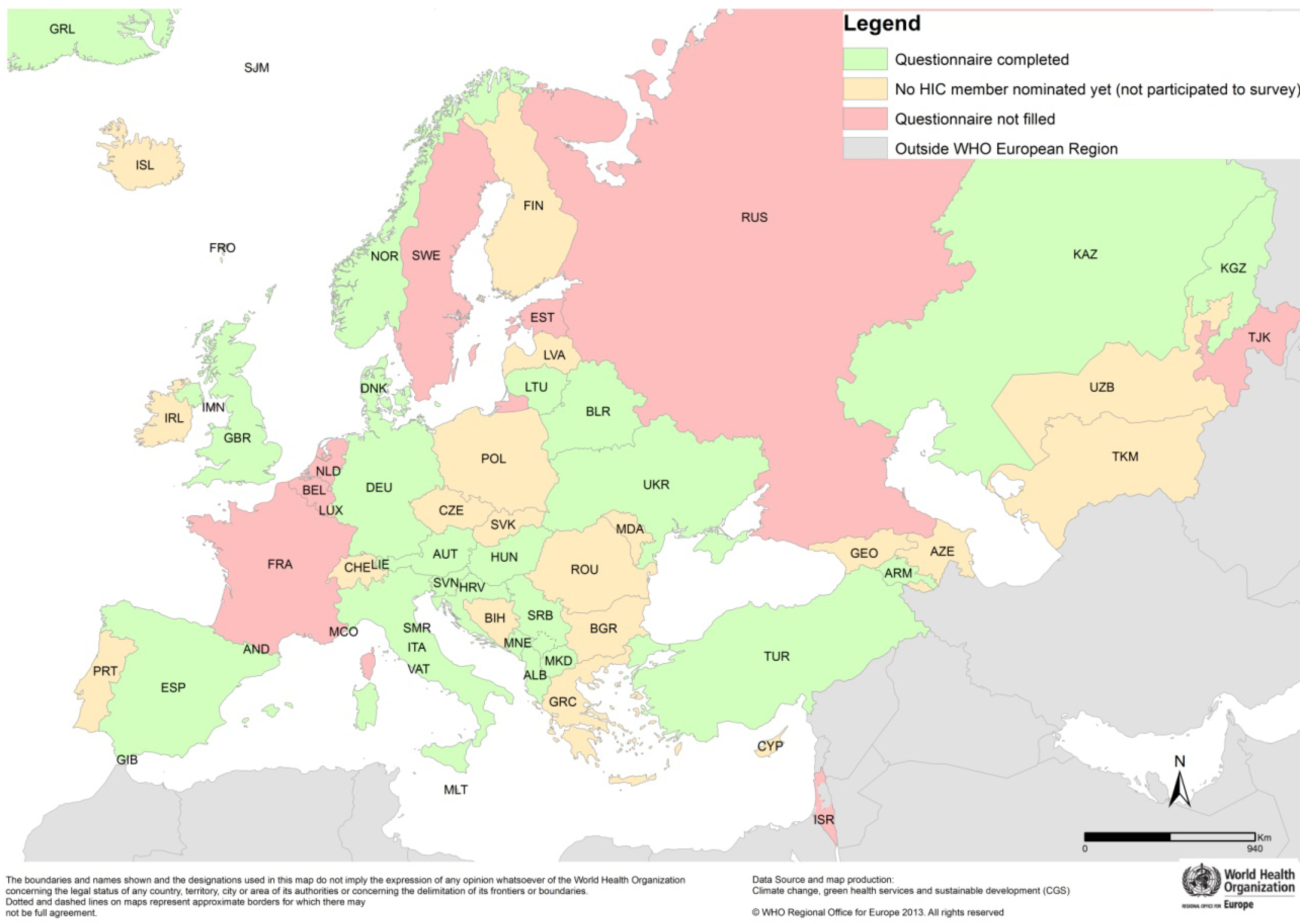
2. Methods: The Questionnaire Survey
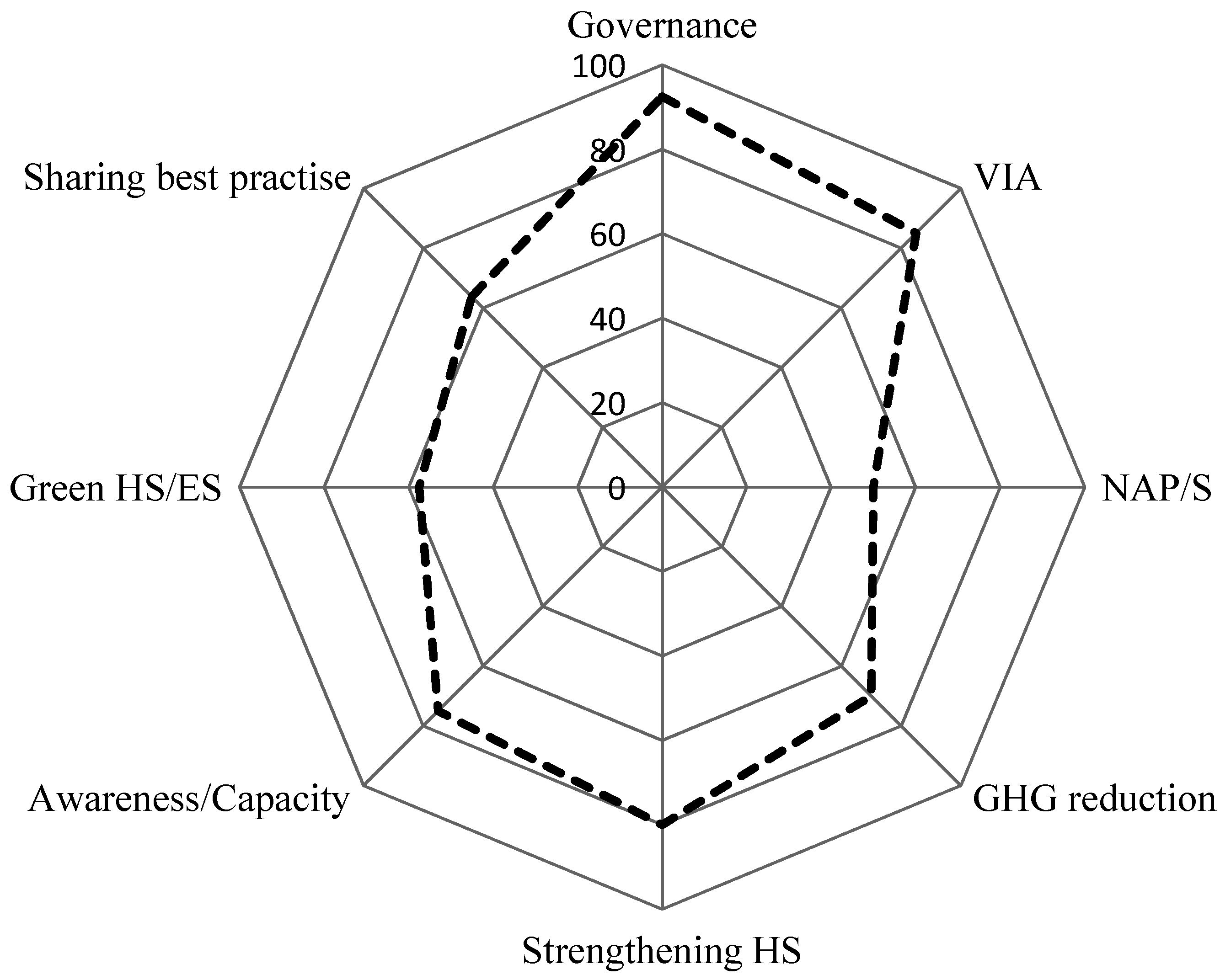
- governance
- vulnerability, impact and adaptation (health) assessments
- adaptation strategies and action plans
- climate change mitigation
- strengthen health systems
- raise awareness and build capacity
- green health services
- sharing best practices.
- (1)
- For the quantitative analysis, positive responses to each sub question were scored as one point and considered as progress towards implementing the Parma Commitment. Both negative responses and lack of responses were scored as zero. Whereas the negative responses can be directly correlated with a relative lack of progress towards policy commitments in different areas, the same cannot be said about lack of response for a question. Reasons for not answering individual items can be manifold, and should not necessarily be interpreted as a negative response. Average positive response score by area and presentation of top-scoring countries by items;
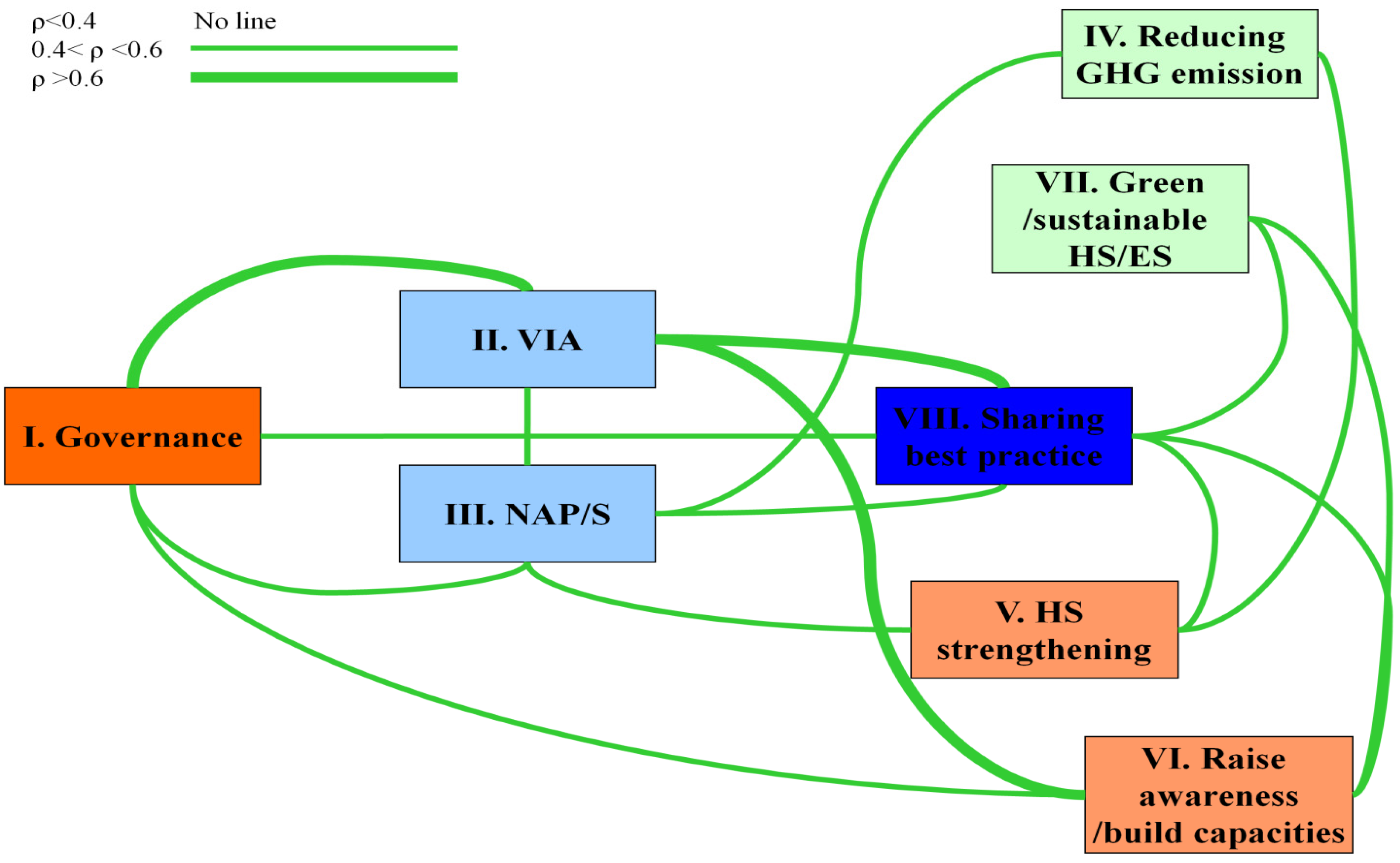
- (2)
- Spearman correlation coefficient was used to detect associations between different sections of the questionnaire.
3. Results

3.1. General Evaluation


{kind=link}
{kind=link}
{kind=link}
| Measures Taken by Member States to Strengthen Health Systems | Number of Countries Replying “Yes” or Giving Examples |
|---|---|
| Strengthened infectious disease surveillance | 19 |
| Strengthened of environmental health services (water, sanitation, vaccination) | 15 |
| Strengthened health security and implementation of International Health Regulations | 15 |
| Strengthened early-warning and disaster response | 15 |
| Mainstreamed climate change into public health policy | 11 |
| Strengthened primary health care service | 13 |
| Ensuring that planning for climate change was included in public health policy | 14 |
| Developed integrated climate, environment and health surveillance | 7 |
| Built climate-resilient infrastructure | 6 |
3.2. Regional Variation
| Country | Governance | VIA | NAP | HS | GHG Redu | GHS | Awareness | Best Practice |
|---|---|---|---|---|---|---|---|---|
| Albania | x | x | x | |||||
| Armenia | x | x | x | x | ||||
| Austria | x | x | x | x | ||||
| Belarus | x | x | x | x | x | |||
| Croatia | x | x | x | x | x | x | ||
| Denmark | x | |||||||
| Germany | x | x | x | x | x | x | ||
| Hungary | x | x | x | x | ||||
| Italy | x | x | ||||||
| Kazakhstan | x | |||||||
| Kyrgyzstan | x | x | ||||||
| Lithuania | x | x | x | |||||
| Montenegro | ||||||||
| Norway | x | x | ||||||
| San Marino | ||||||||
| Serbia | ||||||||
| Slovenia | x | x | ||||||
| Spain | x | x | x | x | x | x | x | |
| The former Yugoslav Republic of Macedonia | x | x | x | x | x | x | ||
| Turkey | x | |||||||
| Ukraine | x | x | x | |||||
| United Kingdom | x | x | x | |||||
| Total | 16 | 17 | 4 | 7 | 4 | 5 | 6 | 6 |
- establishing mechanisms for the exchange of information on climate change between agencies;
- allocating resources for implementation at different levels of government (national, regional and local);
- establishing regulatory or legislative instruments to facilitate implementation; and
- involving a wide variety of stakeholders from the inception phase of strategies and plans.
- cross-sectoral vulnerability and adaptation evaluations as part of their communications to the UNFCCC;
- economic evaluations of sectoral impacts and adaptation;
- studies evaluating climate effects on vulnerable populations;
- supporting subnational authorities in conducting VIA activities; and
- taking into account emerging threats in their VIA activities.
- The plans have not only general strategies to adapt to climate change, but also health-specific adaptation plans that are approved by the government.
- A capacity building component is included.
- Mitigation in the health sector is considered.
- Inclusion of stakeholders is promoted through participatory processes.
- incentives for health care facilities engaging in sustainability activities (e.g. energy efficiency, resource use minimization, etc.);
- linking economic, social and environmental sustainability in their long-term strategies for health systems; and
- indicator-based evaluations of sustainability in health systems.
- making information of good practice available publicly on the internet;
- referring information to regional repositories or clearinghouses (e.g., EU); and
- including good practices in comprehensive communications regarding climate change.
3.3. Interrelationship between responses

4. Discussion
- Governance mechanisms for climate policy seem well-established, at least in countries with HIC representatives.
- Financial and human resources for climate change health adaptation are mainstreamed into ongoing activities and respective resource planning.
- Although VIA works seems to be an area of relatively strong performance, there are gaps in knowledge and in translating scientific evidence into action.
- The level of governmental approval and uptake of national health adaptation plans is still low.
- Most countries are engaged in mitigation activities of GHG related to buildings, infrastructure and transportation. However, the health co-benefits of these activities were less evaluated.
- Countries reported several activities on health systems strengthening. However, important areas remain lacking, for instance integrated climate, environment and health surveillance, or building climate-resilient health infrastructures.
5. Conclusions
Acknowledgments
Author contributions
Conflicts of interest
References
- Resolution WHA61.19: Climate Change and Health. In Sixty-first World Health Assembly; World Health Organization: Geneva, Swizerlands, 2008; pp. 1–3.
- WHO Regional Office for Europe. Parma Declaration on Environment and Health. In Proceedings of Fifth Ministerial Conference on Environment and Health, “Protecting Children’s Health in a Changing Environment”, Parma, Italy, 10–12 March 2010; pp. 1–10.
- Protecting Health in an Environment Challenged by Climate Change: European Regional Framework for Action; WHO Regional Office for Europe: Copenhagen, Denmark, 2010; pp. 1–9.
- CEHAPIS Work Package 5 Policy Monitoring and Assessment; Dalbokova, D.; Kryzanowski, M.; Egorov, A.; Gapp, C. (Eds.) WHO Regional Office for Europe: Copenhagen, Denmark, 2011.
- European Union Countries. How the EU Works. Available online: http://europa.eu/about-eu/countries/index_en.htm (accessed on 27 March 2014).
- List of OECD Member Countries—Ratification of the Convention on the OECD. Available online: http://www.oecd.org/about/membersandpartners/list-oecd-member-countries.htm (accessed on 27 March 2014).
- List of Member States by Region and Mortality Stream. In World Health Report; World Health Organization: Geneva, Swizerlands, 2003; pp. 182–184.
- United Nations Statistics Division. Composition of Macro Geographical (Continental) Regions, Geographical Subregions, and Selected Economic and other Groupings. Available online: https://unstats.un.org/unsd/methods/m49/m49regin.htm (accessed on 27 March 2014).
- Human Development Index and Its Components. In Human Development Report 2011: A Better Future for All; UNDP: New York, NY, USA, 2011; pp. 137–130.
Appendix
| Question Number | Topic/Question | Points | Remark |
|---|---|---|---|
| 1 | Governance | 4 | |
| 2 | Vulnerability, impact and adaptation assessment | 2 | |
| 3 | National and subnational adaptation strategies | 4 | |
| 4 | Climate change mitigation | 6 | |
| 5 | Strengthen health systems | 7 | |
| 6 | Raise awareness—build capacity | 10 | |
| 7 | Green health services | 4 | |
| 8 | Sharing best practices | 8 | |
| total | 45 | ||
| Question Number | Sub Question | Points | Remark |
| 1.1 | Who is in charge of climate change in your country? | 1 | for answer |
| 1.2 | Who is in charge of the health aspects of climate change? | 1 | for answer |
| 1.3 | Has a multisectoral committee been established to deal with climate change? | 1 | for yes |
| 1.4 | Have you identified human and economic resources | 1 | for yes |
| subtotal | 4 | ||
| 2.1 | Have you carried out a national assessment of climate change impact, vulnerability and adaptation in your country? | 1 | for yes |
| 2.2 | Have you done a national (or regional) health impact, vulnerability and adaptation assessment of climate change in your country? | 1 | for yes |
| subtotal | 2 | ||
| 3.1 a | Have you developed a national adaptation strategy to climate change in your country? | 1 | for yes |
| 3.1 b | Has it been approved by your government | 1 | for yes |
| 3.2 a | Have you developed a national climate change health adaptation strategy or health action plan? | 1 | for yes |
| 3.2 b | Has it been approved by your government | 1 | for yes |
| subtotal | 4 | ||
| 4.1 | Do you promote energy efficient buildings? | 1 | for yes |
| 4.2 | Do you promote access to safe transport or public transport modes? | 1 | for yes |
| 4.3 | Do you promote carbon neutral agriculture practices? | 1 | for yes |
| 4.4 | Have you assessed the health benefits of the above measures? | 1 | for yes |
| 4.5 | Have mitigation measures in other sectors in your country been taken? | 1 | for yes |
| 4.6 | If mitigation measures in other sectors have been taken, have any health effects of those mitigation measures been assessed? | 1 | for yes |
| subtotal | 6 | ||
| 5.1 | Have you strengthened public health and health services to cope with climate change? semi-qual.: 10 sub categories | 1 | for yes |
| 5.2 | Have you enhanced disease surveillance and early warning of climate sensitive diseases? semi-qual.: sub categories | 1 | for yes |
| 5.3 | Have you developed early warning systems for extreme weather events and have you developed appropriate health sector response plans in the areas below? semi qual.: 12 sub categories | 1 | for yes |
| 5.4 | Have you strengthened health sector engagement in emergency planning for extreme weather events and have you developed cross-sector plans? semi qual.: 12 sub categories | 1 | for yes |
| 5.5 | Have you improved monitoring of climate sensitive environmental determinants of health | 1 | for yes |
| 5.6 | Have you developed a cross-sector approach on climate change adaptation? | 1 | for yes |
| 5.7 | Do you intend to address health benefits/damages (e.g., by conducting health impact assessment) | 1 | for yes |
| subtotal | 7 | ||
| 6.1 | Is climate change perceived as important in political developments in your country? | 1 | for yes |
| 6.2 | Are health effects of climate change of high relevance in political processes? | 1 | for yes |
| 6.3 a | Is the level of support for policies targeting climate change and related effects on health high in public and private sector of the society? Public sector | 1 | for public |
| 6.3 b | Is the level of support for policies targeting climate change and related effects on health high in public and private sector of the society? Private sector | 1 | for private |
| 6.4 | Do you have enough information at your disposal on climate change and its impact on health with regard to your country? | 1 | completed answer |
| Question Number | Special Question | Points | Remark |
| 6.5 | Have you built capacity and developed a workforce on climate change and health-related aspects | 1 | for yes |
| 6.6 | Have you raised public awareness about climate change and health and mitigation and adaptation measures? | 1 | for yes |
| 6.7 | Have you developed communication messages for extreme weather events to be released with an early warning for such an event? | 1 | for yes |
| 6.8 | Have you developed communication plans for key messages on climate change and health for other sectors and the general public? | 1 | for yes |
| 6.9 | What are the main messages on protecting health from climate change you would like to communicate? | 1 | for example |
| subtotal | 10 | ||
| 7.1 | Greening health services | 1 | for example |
| 7.2 a | Can you list a few examples of measures that have been taken | 1 | for legislation |
| 7.2 b | Have local measures in any health care facilities been taken, like training and organizing the workforce? | 1 | for measures |
| 7.2 c | Have local measures in any health care facilities been taken, like training and organizing the workforce? | 1 | for evaluation |
| subtotal | 4 | ||
| 8.1 | Can you share information on best practice with regard to: 6 choices | 1 | for yes |
| 8.2 | Have you developed projects or aspects related to innovation and research? | 1 | for yes |
| 8.3 | Evaluation of health damage and adaption costs: Have you estimated the costs of climate change and/or the health damage costs | 1 | for yes |
| 8.4 | Do you measure and evaluate trends in climate change, environment and health indicators | 1 | for yes |
| 8.5 | What do you measure? And to whom do you report? | 1 | for any measurements |
| 8.6 | Are you aware of pilot projects in your country on climate change and health? semi qual.: examples of pilot projects | 1 | for example |
| 8.7 | Which of the results would you promote to share with other European Member States? | 1 | for any results |
| 8.8 | Do you make your information available on the EU adaptation clearinghouse? | 1 | |
| subtotal | 8 | ||
| total | 45 |
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Wolf, T.; Martinez, G.S.; Cheong, H.-K.; Williams, E.; Menne, B. Protecting Health from Climate Change in the WHO European Region. Int. J. Environ. Res. Public Health 2014, 11, 6265-6280. https://doi.org/10.3390/ijerph110606265
Wolf T, Martinez GS, Cheong H-K, Williams E, Menne B. Protecting Health from Climate Change in the WHO European Region. International Journal of Environmental Research and Public Health. 2014; 11(6):6265-6280. https://doi.org/10.3390/ijerph110606265
Chicago/Turabian StyleWolf, Tanja, Gerardo Sanchez Martinez, Hae-Kwan Cheong, Eloise Williams, and Bettina Menne. 2014. "Protecting Health from Climate Change in the WHO European Region" International Journal of Environmental Research and Public Health 11, no. 6: 6265-6280. https://doi.org/10.3390/ijerph110606265