Trends of Non-Accidental, Cardiovascular, Stroke and Lung Cancer Mortality in Arkansas Are Associated with Ambient PM2.5 Reductions

Abstract
:1. Introduction
2. Methods
2.1. Health Impacts Assessment

2.2. PM2.5 Mass Concentrations

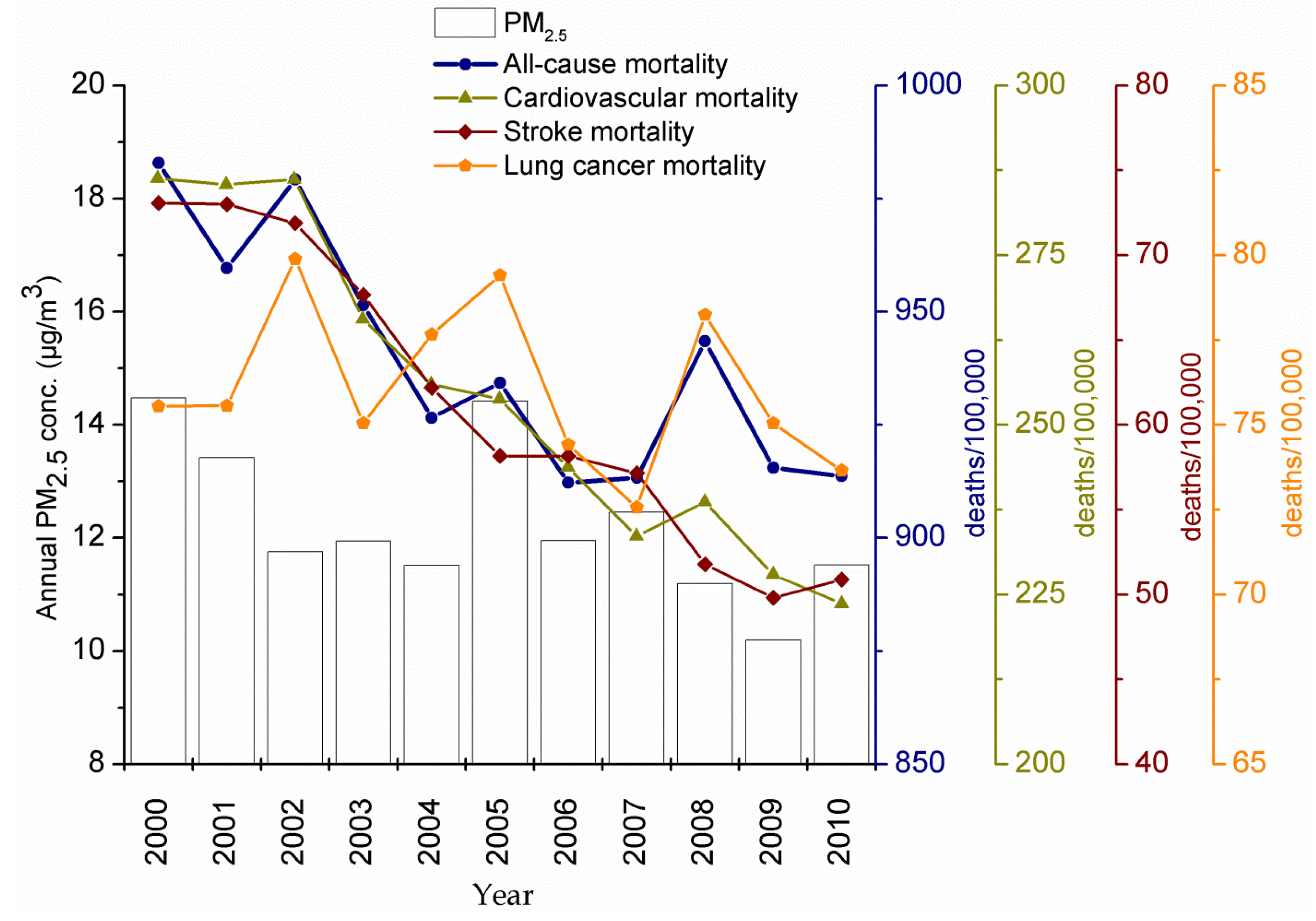
3. Results
3.1. PM2.5 Annual and Spatial Trends

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Site | Annual Trend (μg/m3/year) | ΔC | %ΔC/Ref | COD | ||
|---|---|---|---|---|---|---|
| Median | SD | Median | SD | |||
| ar1 | −0.3 ± 0.5 | −0.9 | 3.5 | −8.1 | 74.5 | 0.19 ± 0.02 |
| ar1 | −0.5 ± 0.6 | −1.0 | 4.8 | −8.2 | 122.8 | 0.19 ± 0.03 |
| ar3 | −0.4 ± 0.5 | −0.5 | 4.4 | −4.4 | 83.5 | 0.18 ± 0.01 |
| ar4 | −0.3 ± 0.5 | −0.7 | 3.1 | −6.2 | 103.5 | 0.19 ± 0.03 |
| ar5 | −0.2 ± 0.5 | −1.0 | 3.4 | −9.3 | 31.7 | 0.20 ± 0.04 |
| ar6 | −0.2 ± 1.0 | −1.1 | 4.5 | −10.3 | 120.3 | 0.22 ± 0.05 |
| ar7 | −0.3 ± 0.6 | −1.1 | 4.5 | −9.1 | 87.8 | 0.20 ± 0.04 |
| ar8 | −0.1 ± 0.3 | −1.5 | 4.4 | −13.4 | 109.9 | 0.21 ± 0.06 |
| ar9 | −0.2 ± 0.4 | −0.7 | 4.0 | −5.9 | 36.3 | 0.18 ± 0.01 |
| ar10 | −0.3 ± 0.4 | - | - | - | - | - |
| ar11 | −0.3 ± 0.5 | 0.3 | 3.0 | 2.5 | 88.7 | 0.16 ± 0.01 |
| ar12 | −0.3 ± 0.5 | 0.1 | 2.7 | 1.3 | 58.3 | 0.16 ± 0.01 |
| ar13 | −0.1 ± 0.5 | −0.7 | 4.4 | −6.9 | 127.5 | 0.19 ± 0.03 |
| ar14 | −0.3 ± 0.5 | −0.6 | 4.6 | −5.7 | 134.0 | 0.18 ± 0.04 |
| ar15 | −0.2 ± 0.3 | −1.4 | 4.7 | −13.9 | 39.3 | 0.21 ± 0.05 |
| ar16 | −0.3 ± 0.5 | −0.7 | 3.8 | −6.1 | 108.3 | 0.20 ± 0.04 |
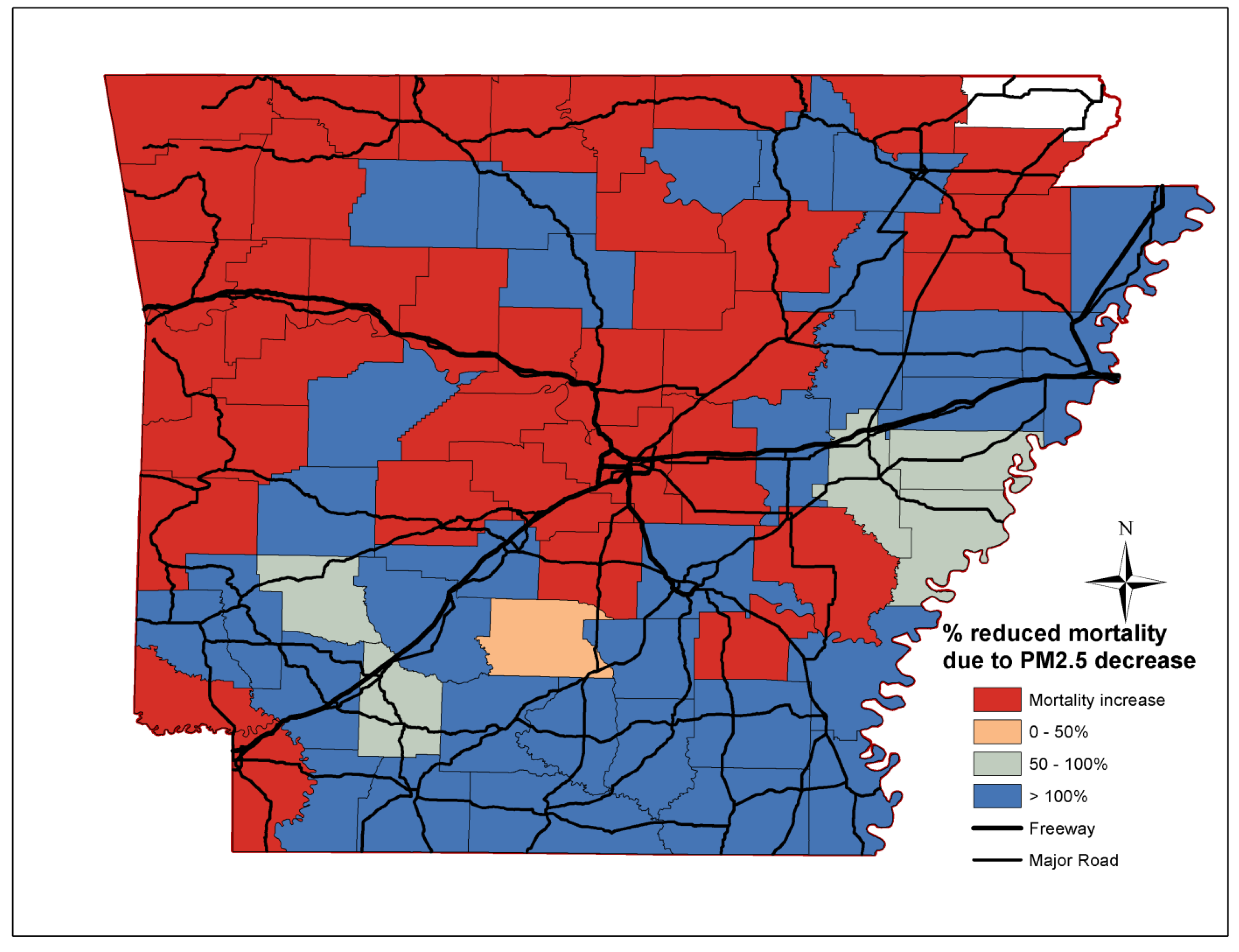
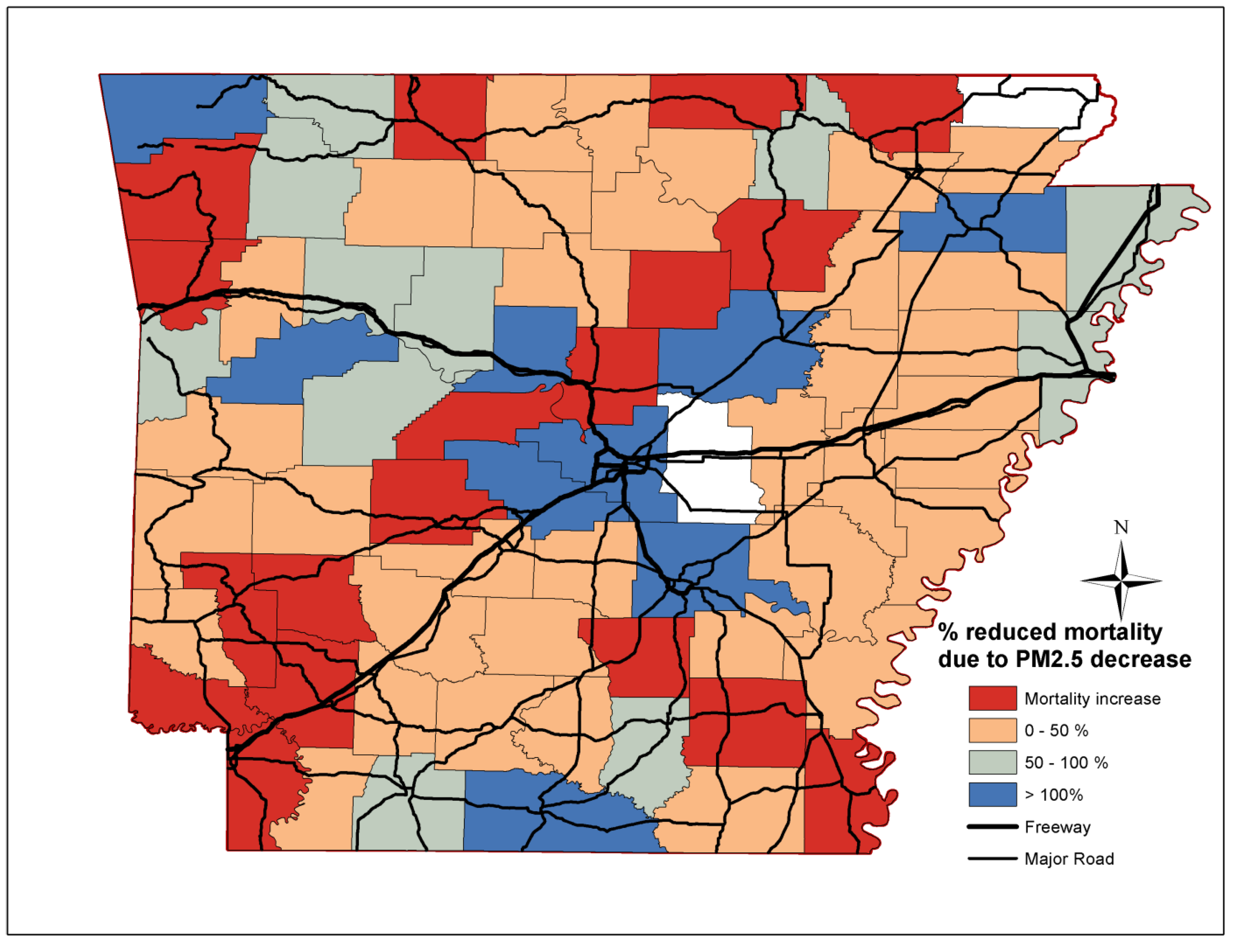
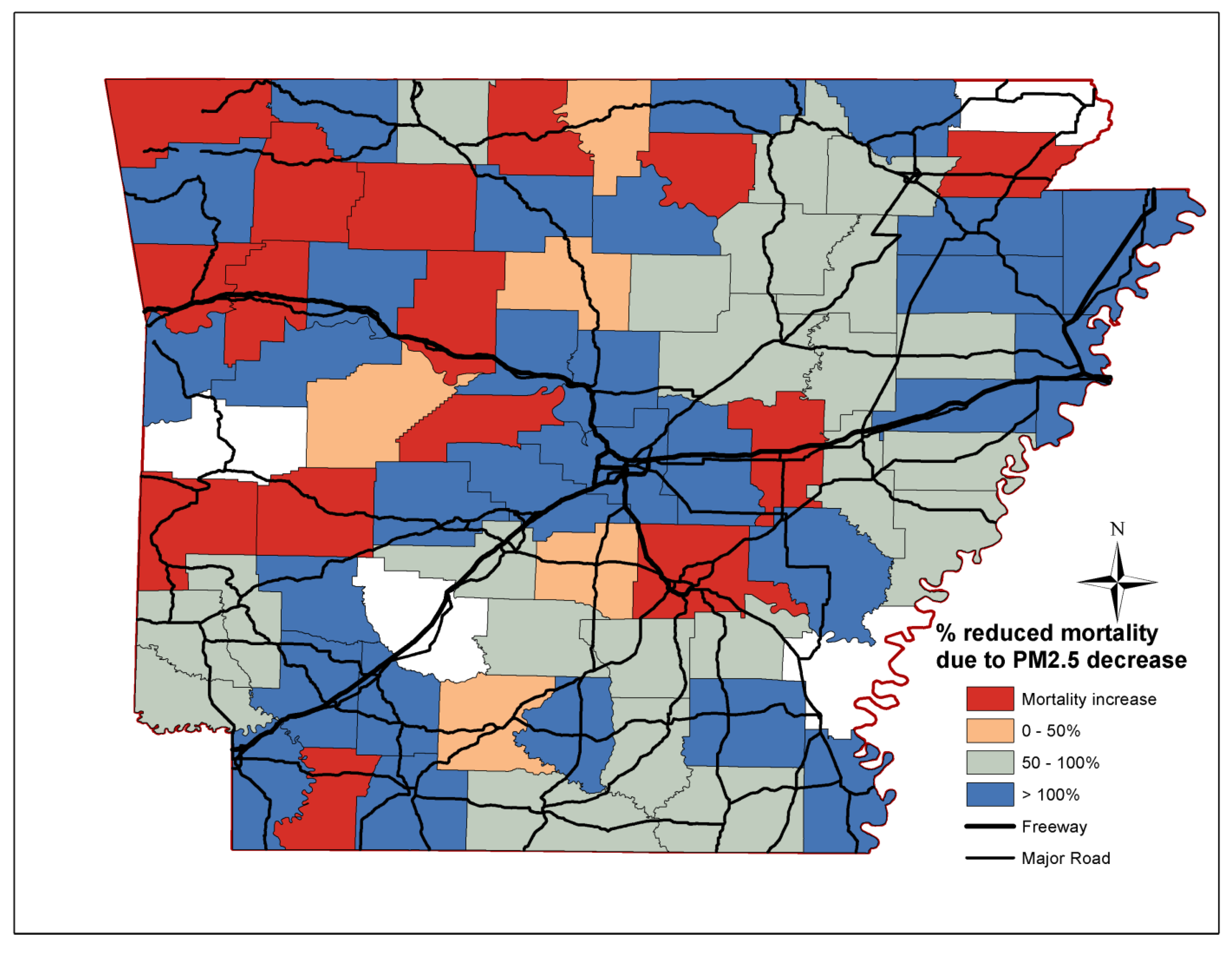
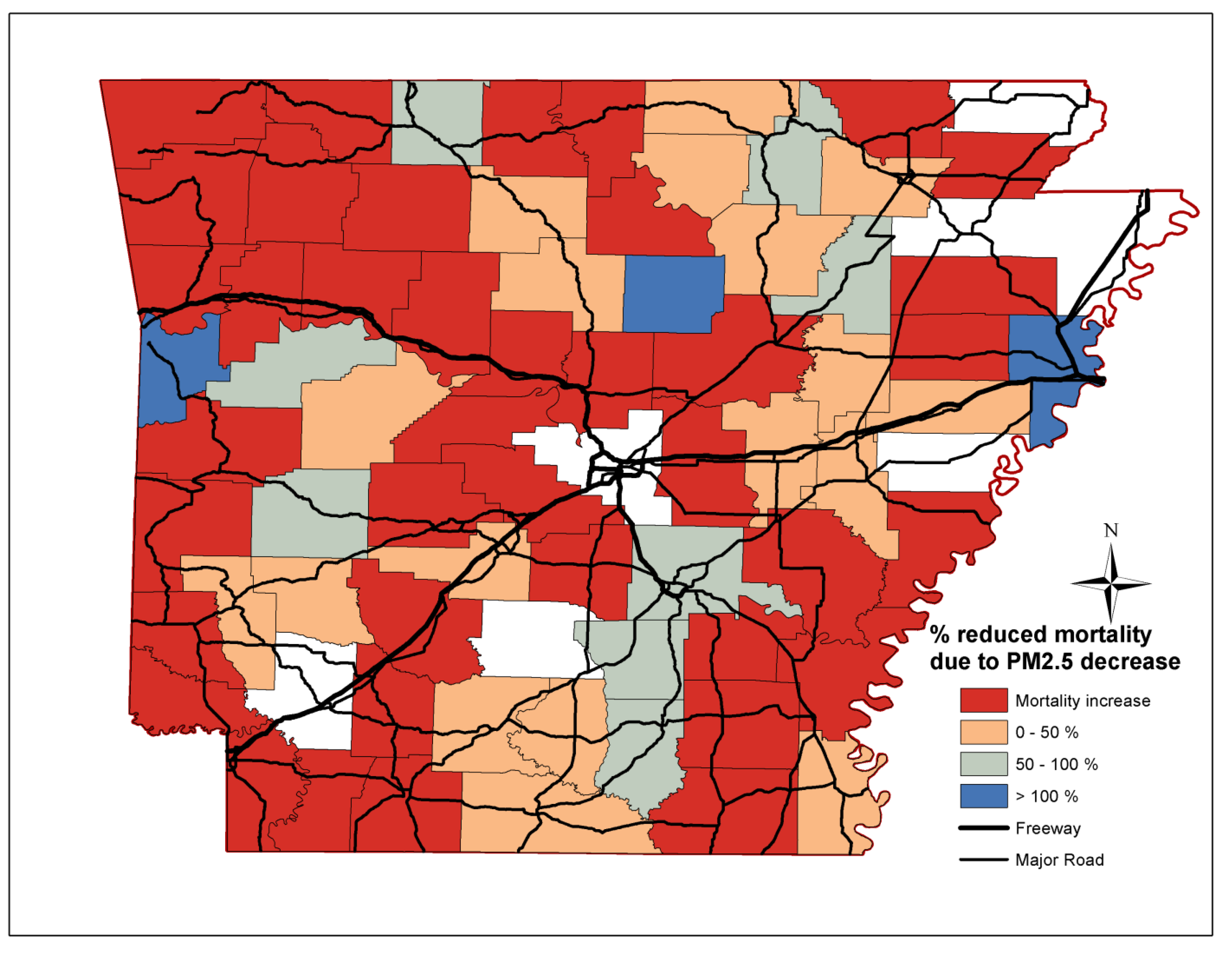
3.2. Mortality Reductions





4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Mujib, M.; Zhang, Y.; Feller, M.A.; Ahmed, A. Evidence of a “Heart Failure Belt” in the southeastern United States. Amer. J. Cardiol. 2011, 107, 935–937. [Google Scholar] [CrossRef]
- Howard, G. Why do we have a stroke belt in the southeastern United States? A review of unlikely and uninvestigated potential causes. Amer. J. Med. Sci. 1999, 317, 160–167. [Google Scholar] [CrossRef]
- Maulden, J.; Philips, M.M. 2012 Arkansas Heart Disease and Stroke Report—A Snapshot of Cardiovascular Diseases IN Arkansas; Arkansas Minority Health Commission: Little Rock, AR, USA, 2012. [Google Scholar]
- Balamurugan, A.; Mehta, P.; Bates, J.; Mehta, J.L. Change in mortality from coronary heart disease and stroke in Arkansas (1979 to 2007). Amer. J. Cardiol. 2011, 107, 156–160. [Google Scholar] [CrossRef]
- McClure, L.A.; Murphy, H.L.; Roseman, J.; Howard, G.; Malarcher, A. Regional and racial differences in smoking and exposure to secondhand smoke: The reasons for geographic and racial differences in stroke (REGARDS) study. In Prev. Chronic Dis.; 2011; 8. Available online: http://www.cdc.gov/pcd/issues/2011/sep/pdf/10_0190.pdf (accessed on 5 June 2014). [Google Scholar]
- Peel, J.; Tolbert, P.; Klein, M.; Metzger, K.; Flanders, W.; Todd, K.; Mulholland, J.; Ryan, P.; Frumkin, H. Ambient air pollution and respiratory emergency department visits. Epidemiology 2005, 16, 164–174. [Google Scholar] [CrossRef]
- Zanobetti, A.; Schwartz, J. The effect of particulate air pollution on emergency admissions for myocardial infarction: A multicity case-crossover analysis. Environ. Health Perspect. 2005, 113, 978–982. [Google Scholar] [CrossRef]
- Dominici, F.; Peng, R.; Bell, M.; Pham, L.; McDermott, A.; Zeger, S.; Samet, J. Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. JAMA 2006, 295, 1127–1134. [Google Scholar] [CrossRef]
- Ostro, B.; Broadwin, R.; Green, S.; Feng, W.; Lipsett, M. Fine particulate air pollution and mortality in nine California counties: Results from CALFINE. Environ. Health Perspect. 2006, 114, 29–33. [Google Scholar]
- Crouse, D.L.; Peters, P.A.; van Donkelaar, A.; Goldberg, M.S.; Villeneuve, P.J.; Brion, O.; Khan, S.; Atari, D.O.; Jerrett, M.; Pope, C.A.; et al. Risk of non accidental and cardiovascular mortality in relation to long-term exposure to low concentrations of fine particulate matter: A Canadian national-level cohort study. Environ. Health Perspect. 2012, 120, 708–714. [Google Scholar] [CrossRef]
- Turner, M.C.; Krewski, D.; Pope, C.A., III; Chen, Y.; Gapstur, S.M.; Thun, M.J. Long-term ambient fine particulate matter air pollution and lung cancer in a large cohort of never-smokers. Amer. J. Respir. Crit. Care Med. 2011, 184, 1374–1381. [Google Scholar] [CrossRef]
- Zhou, J.; Ito, K.; Lall, R.; Lippmann, M.; Thurston, G. Time-series analysis of mortality effects of fine particulate matter components in Detroit and Seattle. Environ. Health Perspect. 2011, 119, 461–466. [Google Scholar]
- Wellenius, G.A.; Burger, M.R.; Coull, B.A.; Schwartz, J.; Suh, H.H.; Koutrakis, P.; Schlaug, G.; Gold, D.R.; Mittleman, M.A. Ambient air pollution and the risk of acute ischemic stroke. Arch. Intern. Med. 2012, 172, 229–234. [Google Scholar] [CrossRef]
- Chalbot, M.-C.; McElroy, B.; Kavouras, I.G. Sources, trends and regional impacts of fine particulate matter in southern Mississippi Valley: Significance of emissions from sources in the Gulf of Mexico coast. Atmos. Chem. Phys. 2013, 13, 3721–3732. [Google Scholar] [CrossRef]
- Bell, M.L.; Dominici, F.; Ebisu, K.; Zeger, S.L.; Samet, J.M. Spatial and temporal variation in PM2.5 chemical composition in the United States for health effects studies. Environ. Health Perspect. 2007, 115, 989–995. [Google Scholar] [CrossRef]
- Krall, J.R.; Anderson, G.B.; Dominici, F.; Bell, M.L.; Peng, R.D. Short-term exposure to particulate matter constituents and mortality in a national study of U.S. urban communities. Environ. Health Perspect. 2013, 121, 1148–1153. [Google Scholar]
- Spak, S.N.; Holloway, T. Seasonality of speciated aerosol transport over the great lakes region. J. Geophys. Res.-Atmos. 2009, 114. [Google Scholar] [CrossRef]
- Ballester, F.; Medina, S.; Goodman, P.; Boldo, E.; le Tertre, A.; Neuberger, M.; Larrieu, S.; Kuenzli, N.; Cambra, K.; Katsouyanni, K.; et al. Health impact assessment on the benefits of reducing PM2.5 using mortality data from 28 European cities. Epidemiology 2006, 17, S248–S248. [Google Scholar]
- Boldo, E.; Medina, S.; LeTertre, A.; Hurley, F.; Muecke, H.-G.; Ballester, F.; Aguilera, I. Apheis: Health impact assessment of long-term exposure to PM2.5 in 23 European cities. Eur. J. Epidemiol. 2006, 21, 449–458. [Google Scholar] [CrossRef]
- Sheffield, P.E.; Knowlton, K.; Carr, J.L.; Kinney, P.L. Modeling of regional climate change effects on ground-level ozone and childhood asthma. Amer. J. Prev. Med. 2011, 41, 251–257. [Google Scholar] [CrossRef]
- World Health Organization. Evaluation and Use of Epidemilogical Evidence for Environmental Health Risk Assessment; WHO Regional Office for Europe: Copenhagen, Denmark, 2000; p. 39. [Google Scholar]
- World Health Organization. Quantification of Health Effect of Exposure to Air Pollution; WHO Regional Office for Europe: Copenhagen, Denmark, 2001; p. 34. [Google Scholar]
- Pope, C.A.I.; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 2002, 287, 1132–1141. [Google Scholar] [CrossRef]
- Krewski, D.; Burnett, R.; Jerrett, M.; Pope, C.; Rainham, D.; Calle, E.; Thurston, G.; Thun, M. Mortality and long-term exposure to ambient air pollution: Ongoing analyses based on the American cancer society cohort. J. Toxicol. Environ. Health Pt. A 2005, 68, 1093–1109. [Google Scholar] [CrossRef]
- Krewski, D.; Jerrett, M.; Burnett, R.T.; Ma, R.; Hughes, E.; Shi, Y.; Turner, M.C.; Pope, C.A., III; Thurston, G.; Calle, E.E.; et al. Extended Follow-up and Spatial Analysis of the American Cancer Society Study Linking Particulate Air Pollution and Mortality; Health Effects Institute: Boston, MA, USA, 2009. Available online: http://pubs.healtheffects.org/getfile.php?u=478 (accessed on 21 April 2014).
- Franklin, M.; Zeka, A.; Schwartz, J. Association between PM2.5 and all-cause and specific-cause mortality in 27 USA communities. J. Expo. Sci. Environ. Epidemiol. 2007, 17, 279–287. [Google Scholar] [CrossRef]
- Jaffe, D.; Ray, J. Increase in surface ozone at rural sites in the western USA. Atmos. Environ. 2007, 41, 5452–5463. [Google Scholar] [CrossRef]
- Pinto, J.; Lefohn, A.; Shadwick, D. Spatial variability of PM2.5 in urban areas in the United States. J. Air Waste Manage. Assoc. 2004, 54, 440–449. [Google Scholar] [CrossRef]
- Lianou, M.; Chalbot, M.; Kotronarou, A.; Kavouras, I.G.; Karakatsani, A.; Katsouyanni, K.; Puustinnen, A.; Hameri, K.; Vallius, M.; Pekkanen, J.; et al. Dependence of home outdoor particulate mass and number concentrations on residential and traffic features in urban areas. J. Air Waste Manage. Assoc. 2007, 57, 1507–1517. [Google Scholar]
- Gulliver, J.; de Hoogh, K.; Fecht, D.; Vienneau, D.; Briggs, D. Comparative assessment of gIS-based methods and metrics for estimating long-term exposures to air pollution. Atmos. Environ. 2011, 45, 7072–7080. [Google Scholar] [CrossRef]
- Liao, D.; Peuquet, D.J.; Duan, Y.; Whitsel, E.A.; Dou, J.; Smith, R.L.; Lin, H.; Chen, J.; Heiss, G. GIS approaches for the estimation of residential-level ambient PM concentrations. Environ. Health Perspect. 2006, 114, 1374–1380. [Google Scholar] [CrossRef]
- Pearce, J.L.; Rathbun, S.L.; Aguilar-Villalobos, M.; Naeher, L.P. Characterizing the spatiotemporal variability of PM2.5 in Cusco, Peru using Kriging with external drift. Atmos. Environ. 2009, 43, 2060–2069. [Google Scholar] [CrossRef]
- Reeve, G.R.; Balamurugan, A.; Simon, W.; Faulker, L.; Zohoori, N. The Burden of Heart Disease & Stroke in Arkansas; Arkansas Department of Health: Little Rock, AR, USA, 2012; pp. 1–94. [Google Scholar]
- Kavouras, I.G.; DuBois, D.W.; Etyemezian, V.; Nikolich, G. Spatiotemporal variability of ground-level ozone and influence of smoke in treasure valley, Idaho. Atmos. Res. 2013, 124, 44–52. [Google Scholar] [CrossRef]
- Kumar, N.; Chu, A.D.; Foster, A.D.; Peters, T.; Willis, R. Satellite remote sensing for developing time and space resolved estimates of ambient particulate in Cleveland, OH, USA. Aerosol Sci. Tech. 2011, 45, 1090–1108. [Google Scholar] [CrossRef]
- Lee, S.; Serre, M.L.; van Donkelaar, A.; Martin, R.V.; Burnett, R.T.; Jerrett, M. Comparison of geostatistical interpolation and remote sensing techniques for estimating long-term exposure to ambient PM2.5 concentrations across the continental United States. Environ. Health Perspect. 2012, 120, 1727–1732. [Google Scholar]
- Lackland, D.T.; Roccella, E.J.; Deutch, A.F.; Fornage, M.; George, M.G.; Howard, G.; Kissela, B.M.; Kittner, S.J.; Lichtman, J.H.; Lisabeth, L.D.; et al. Factors influencing the decline in stroke mortality: A statement from the American heart association/American stroke association. Stroke 2014, 1. [Google Scholar] [CrossRef]
- Franklin, M.; Koutrakis, P.; Schwartz, J. The role of particle composition on the association between PM2.5 and mortality. Epidemiology 2008, 19, 680–689. [Google Scholar] [CrossRef]
- Bell, M.L.; Ebisu, K. Environmental inequality in exposures to airborne particulate matter components in the United States. Environ. Health Perspect. 2012, 120, 1699–1704. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Chalbot, M.-C.G.; Jones, T.A.; Kavouras, I.G. Trends of Non-Accidental, Cardiovascular, Stroke and Lung Cancer Mortality in Arkansas Are Associated with Ambient PM2.5 Reductions. Int. J. Environ. Res. Public Health 2014, 11, 7442-7455. https://doi.org/10.3390/ijerph110707442
Chalbot M-CG, Jones TA, Kavouras IG. Trends of Non-Accidental, Cardiovascular, Stroke and Lung Cancer Mortality in Arkansas Are Associated with Ambient PM2.5 Reductions. International Journal of Environmental Research and Public Health. 2014; 11(7):7442-7455. https://doi.org/10.3390/ijerph110707442
Chicago/Turabian StyleChalbot, Marie-Cecile G., Tamara A. Jones, and Ilias G. Kavouras. 2014. "Trends of Non-Accidental, Cardiovascular, Stroke and Lung Cancer Mortality in Arkansas Are Associated with Ambient PM2.5 Reductions" International Journal of Environmental Research and Public Health 11, no. 7: 7442-7455. https://doi.org/10.3390/ijerph110707442