Atopic Diseases and Systemic Lupus Erythematosus: An Epidemiological Study of the Risks and Correlations

Abstract
:1. Introduction
2. Material and Methods
2.1. Data Source
2.2. SLE cases and Their Controls
2.3. Atopic Diseases and Covariates

2.4. Statistical Analysis
3. Result

{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | Controls N = 6692 | Cases N = 1673 | cOR | 95% CI | |||
|---|---|---|---|---|---|---|---|
| N | % | N | % | ||||
| Sex | |||||||
| Female | 5524 | 82.5 | 1381 | 82.5 | 1.00 | (Reference) | |
| Male | 1168 | 17.5 | 292 | 17.5 | 1.00 | (0.87–1.15) | |
| Age, years | |||||||
| <20 | 964 | 14.4 | 241 | 14.4 | 1.00 | (Reference) | |
| 20–39 | 2596 | 38.8 | 649 | 38.8 | 1.00 | (0.85–1.18) | |
| 40–59 | 2108 | 31.5 | 527 | 31.5 | 1.00 | (0.84–1.19) | |
| ≥60 | 1024 | 15.3 | 256 | 15.3 | 1.00 | (0.82–1.22) | |
| Mean (SD) | 40.0 | (18.4) | 40.1 | (18.2) | |||
| Urbanization † | |||||||
| 1 | 2004 | 30.0 | 532 | 31.8 | 1.17 | (0.99–1.37) | |
| 2 | 1985 | 29.7 | 487 | 29.1 | 1.08 | (0.92–1.27) | |
| 3 | 1206 | 18.0 | 274 | 16.4 | 1.00 | (reference) | |
| 4 | 910 | 13.6 | 223 | 13.3 | 1.08 | (0.89–1.31) | |
| 5 | 587 | 8.77 | 157 | 9.38 | 1.18 | (0.95–1.47) | |
| Comorbidity † | |||||||
| Allergic rhinitis | 1274 | 19.0 | 441 | 26.4 | 1.52 | (1.34–1.73) *** | |
| Allergic conjunctivitis | 1613 | 24.1 | 548 | 32.8 | 1.53 | (1.37–1.72) *** | |
| Atopic dermatitis | 205 | 3.06 | 114 | 6.81 | 2.31 | (1.83–2.93) *** | |
| Asthma | 511 | 7.64 | 177 | 10.6 | 1.43 | (1.20–1.71) *** | |
| Atopic Diseases | All | Female | Male | |||
|---|---|---|---|---|---|---|
| OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | |
| Atopic diseases † | ||||||
| Allergic rhinitis | 1.36 | (1.19–1.55) *** | 1.39 | (1.20–1.60) *** | 1.22 | (0.88–1.68) |
| Allergic conjunctivitis | 1.43 | (1.26–1.61) *** | 1.44 | (1.27–1.64) *** | 1.32 | (0.95–1.83) |
| Atopic dermatitis | 2.13 | (1.67–2.70) *** | 2.14 | (1.66–2.76) *** | 2.00 | (1.01–3.99) * |
| Asthma | 1.18 | (0.97–1.43) | 1.21 | (0.97–1.49) | 1.04 | (0.66–1.64) |
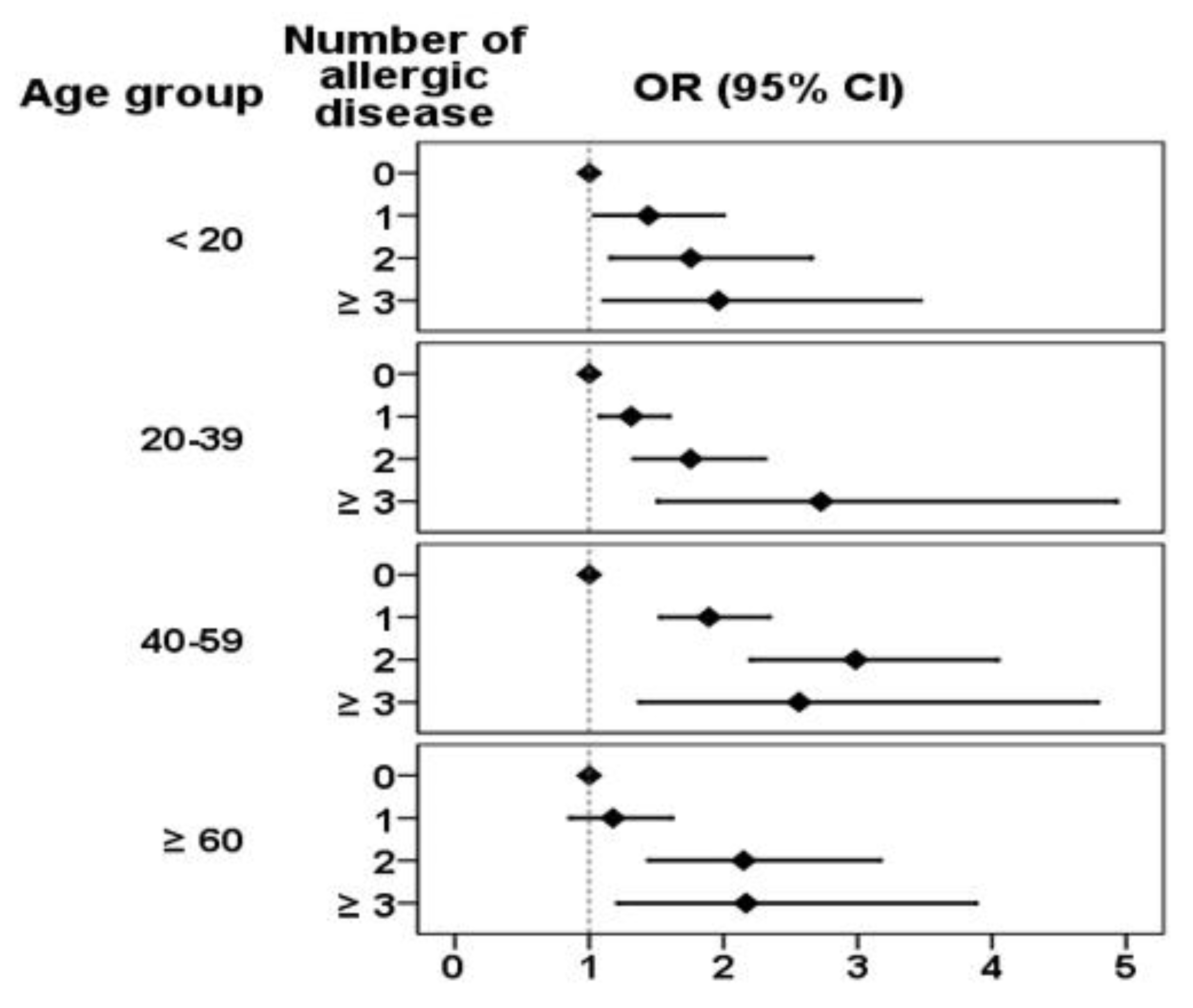
| Number of atopic diseases | ||||||
| 0 | 1.00 | (reference) | 1.00 | (reference) | 1.00 | (reference) |
| 1 | 1.46 | (1.29–1.65) *** | 1.51 | (1.32–1.73) *** | 1.24 | (0.92–1.67) |
| 2 | 2.11 | (1.79–2.49) *** | 2.24 | (1.87–2.68) *** | 1.54 | (1.04–2.37) * |
| ≥3 | 2.29 | (1.71–3.06) *** | 2.33 | (1.71–3.19) *** | 2.13 | (0.95–4.78) |
| p for trend | <0.0001 | <0.0001 | 0.007 | |||


4. Discussion
Acknowledgements
Author Contributions
Conflicts of Interest
References
- Rahman, A.; Isenberg, D.A. Systemic lupus erythematosus. N. Engl. J. Med. 2008, 358, 929–939. [Google Scholar] [CrossRef]
- Yang, C.Y.; Shih, I.H.; Yang, C.H. Neonatal lupus erythematosus infants and their mothers: A 10-year retrospective study. Dermatol. Sinica 2010, 28, 107–112. [Google Scholar] [CrossRef]
- Wozniacka, A.; Sysa-Jedrzejowska, A.; Robak, E.; Samochocki, Z.; Zak-Prelich, M. Allergic diseases, drug adverse reactions and total immunoglobulin E levels in lupus erythematosus patients. Mediat. Inflamm. 2003, 12, 95–99. [Google Scholar] [CrossRef]
- Matsui, S.; Kitaba, S.; Itoi, S.; Kijima, A.; Murota, H.; Tani, M.; Katayama, I. A case of disseminated DLE complicated by atopic dermatitis and Sjögren’s syndrome: Link between hypohidrosis and skin manifestations. Mod. Rheumatol. 2011, 21, 101–105. [Google Scholar] [CrossRef]
- Higashi, N.; Kawana, S. Atopic eczema complicated by systemic lupus erythematosus. Eur. J. Dermatol. 2005, 15, 500–502. [Google Scholar]
- Halken, S. Prevention of allergic disease in childhood: Clinical and epidemiological aspects of primary and secondary allergy prevention. Pediatr. Allergy Immunol. 2004, 15, S9–S32. [Google Scholar]
- D’Cruz, D.P.; Khamashta, M.A.; Hughes, G.R. Systemic lupus erythematosus. Lancet 2007, 369, 587–596. [Google Scholar] [CrossRef]
- Sekigawa, I.; Yoshiike, T.; Iida, N.; Hashimoto, H.; Ogawa, H. Two cases of atopic dermatitis associated with autoimmune abnormalities. Rheumatology 2003, 42, 184–185. [Google Scholar] [CrossRef]
- National Health Insurance Administration, Ministry of Health and Welfare, Taiwan. Available online: http://www.nhi.gov.tw (accessed on 5 August 2014).
- Taiwan Rheumatology Association. Available online: http://www.rheumatology.org.tw (accessed on 5 August 2014).
- Tang, T.S.; Bieber, T.; Williams, H.C. Dose “autoreactivity” play a role in atopic dermatitis? J. Allergy Clin. Immunol. 2012, 129, 1209–1215. [Google Scholar] [CrossRef]
- Goldman, J.A.; Klimek, G.A.; Ali, R. Allergy in systemic lupus erythematosus. Arthritis. Rheum. 1976, 19, 669–676. [Google Scholar] [CrossRef]
- Sequeira, J.F.; Cesia, D.; Keser, G.; Bukelica, M.; Karanagnostis, S.; Khamashta, M.A.; Hughes, G.R. Allergic disorders in systemic lupus erythematosus. Lupus 1993, 2, 187–191. [Google Scholar] [CrossRef]
- Sekigawa, I.; Yoshiike, T.; Iida, N.; Hashimoto, H.; Ogawa, H. Allergic disorders in systemic lupus erythematosus: Prevalence and family history. Lupus 2002, 11, 426–429. [Google Scholar] [CrossRef]
- Ohkouchi, K.; Mizutani, H.; Tanaka, M.; Takahashi, M.; Nakashima, K.; Shimizu, M. Anti-elongation factor-1a autoantibody in adult atopic dermatitis patients. Int. Immunol. 1999, 11, 1635–1640. [Google Scholar]
- Ochs, R.L.; Muro, Y.; Si, Y.; Ge, H.; Chan, E.K.; Tan, E.M. Autoantibodies to DFS 70 kd/transcription coactivator p75 in atopic dermatitis and other conditions. J. Allergy Clin. Immunol. 2000, 105, 1211–1220. [Google Scholar] [CrossRef]
- Van Bever, H.P.; Llanora, G. Features of childhood atopic dermatitis. Asian Pac. J. Allergy Immunol. 2011, 29, 15–24. [Google Scholar]
- Parks, C.G.; Biagini, R.E.; Cooper, G.S.; Gilkeson, G.S.; Dooley, M.A. Total serum IgE levels in systemic lupus erythematosus and associations with childhood onset allergies. Lupus 2010, 19, 1614–1622. [Google Scholar] [CrossRef]
- Schmitz, R.; Ellert, U.; Kalcklösch, M.; Dahm, S.; Thamm, M. Patterns of sensitization to inhalant and food allergens—Findings from the German health interview and examination survey for children and adolescents. Int. Arch. Allergy Immunol. 2013, 162, 263–270. [Google Scholar] [CrossRef]
- Becker, K.G.; Barnes, K.C. Underlyihng disease specificity of genetic loci in atopic dermatitis. J. Invest. Dermatol. 2001, 117, 1325–1327. [Google Scholar] [CrossRef]
- Chiu, Y.M.; Lai, C.H. Nationwide population-based epidemiologic study of systemic lupus erythematosus in Taiwan. Lupus 2010, 19, 1250–1255. [Google Scholar] [CrossRef]
- Wang, I.K.; Muo, C.H.; Chang, Y.C.; Liang, C.C.; Lin, S.Y.; Chang, C.T.; Yen, T.H.; Chuang, F.R.; Chen, P.C.; Huang, C.C.; et al. Risks, subtypes, and hospitalization costs of stroke among patients with systemic lupus erythematosus: A retrospective cohort study in Taiwan. J. Rheumatol. 2012, 39, 1611–1618. [Google Scholar] [CrossRef]
- Sekigawa, I.; Naito, T.; Hira, K.; Mitsuishi, K.; Ogasawara, H.; Hashimoto, H.; Ogawa, H. Possible mechanisms of gender bias in SLE: A new hypothesis involving a comparison of SLE with atopy. Lupus 2004, 13, 217–222. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Hsiao, Y.-P.; Tsai, J.-D.; Muo, C.-H.; Tsai, C.-H.; Sung, F.-C.; Liao, Y.-T.; Chang, Y.-J.; Yang, J.-H. Atopic Diseases and Systemic Lupus Erythematosus: An Epidemiological Study of the Risks and Correlations. Int. J. Environ. Res. Public Health 2014, 11, 8112-8122. https://doi.org/10.3390/ijerph110808112
Hsiao Y-P, Tsai J-D, Muo C-H, Tsai C-H, Sung F-C, Liao Y-T, Chang Y-J, Yang J-H. Atopic Diseases and Systemic Lupus Erythematosus: An Epidemiological Study of the Risks and Correlations. International Journal of Environmental Research and Public Health. 2014; 11(8):8112-8122. https://doi.org/10.3390/ijerph110808112
Chicago/Turabian StyleHsiao, Yu-Ping, Jeng-Dau Tsai, Chih-Hsin Muo, Chung-Hung Tsai, Fung-Chang Sung, Ya-Tang Liao, Yen-Jung Chang, and Jen-Hung Yang. 2014. "Atopic Diseases and Systemic Lupus Erythematosus: An Epidemiological Study of the Risks and Correlations" International Journal of Environmental Research and Public Health 11, no. 8: 8112-8122. https://doi.org/10.3390/ijerph110808112