Creating an Interest in Research and Development as a Means of Reducing the Gap between Theory and Practice in Primary Care: An Interventional Study Based on Strategic Communication

Abstract
:1. Introduction
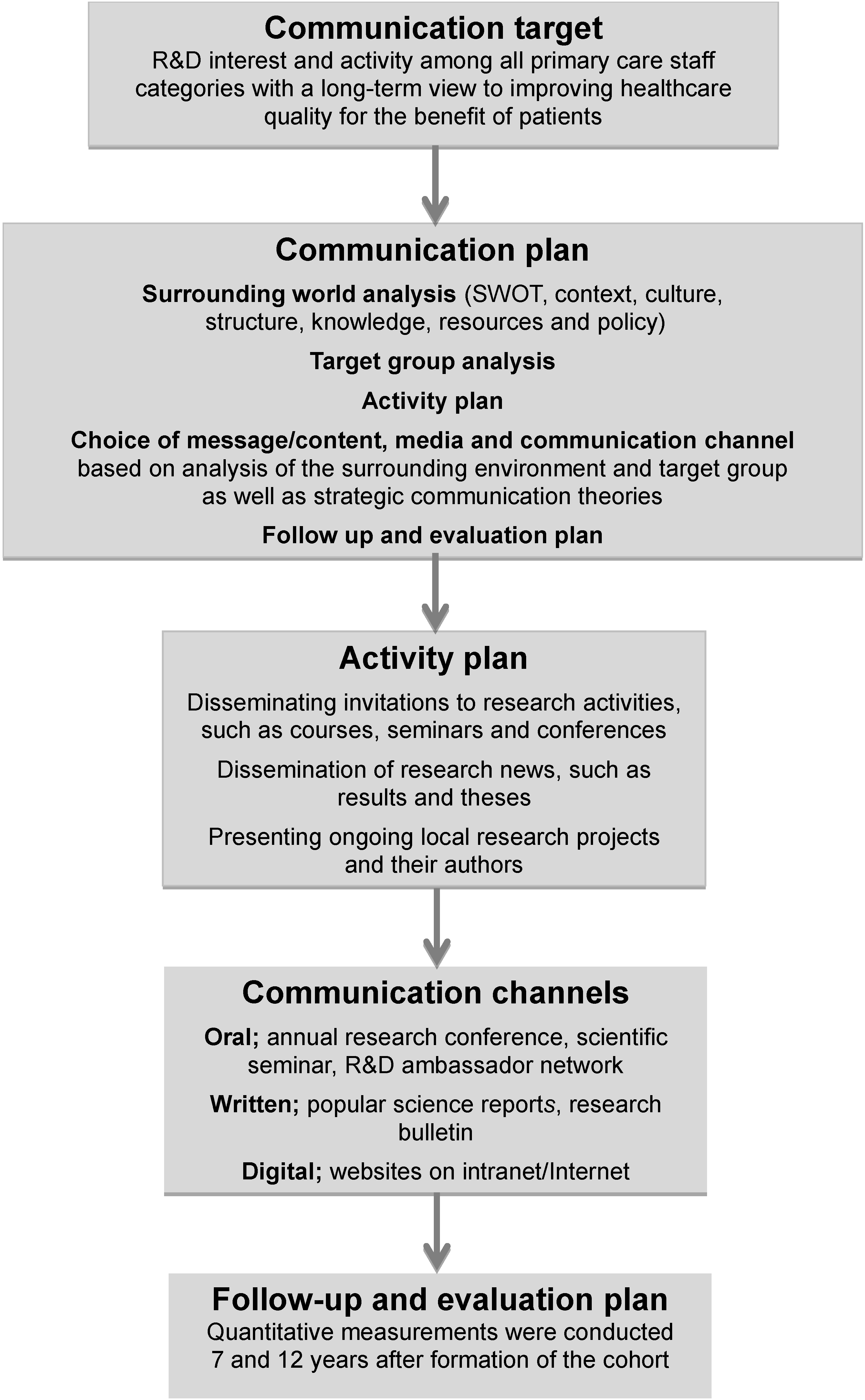
Strategic Communication Process
- Can strategic communication contribute to creating interest in R&D among PCSMs over time?
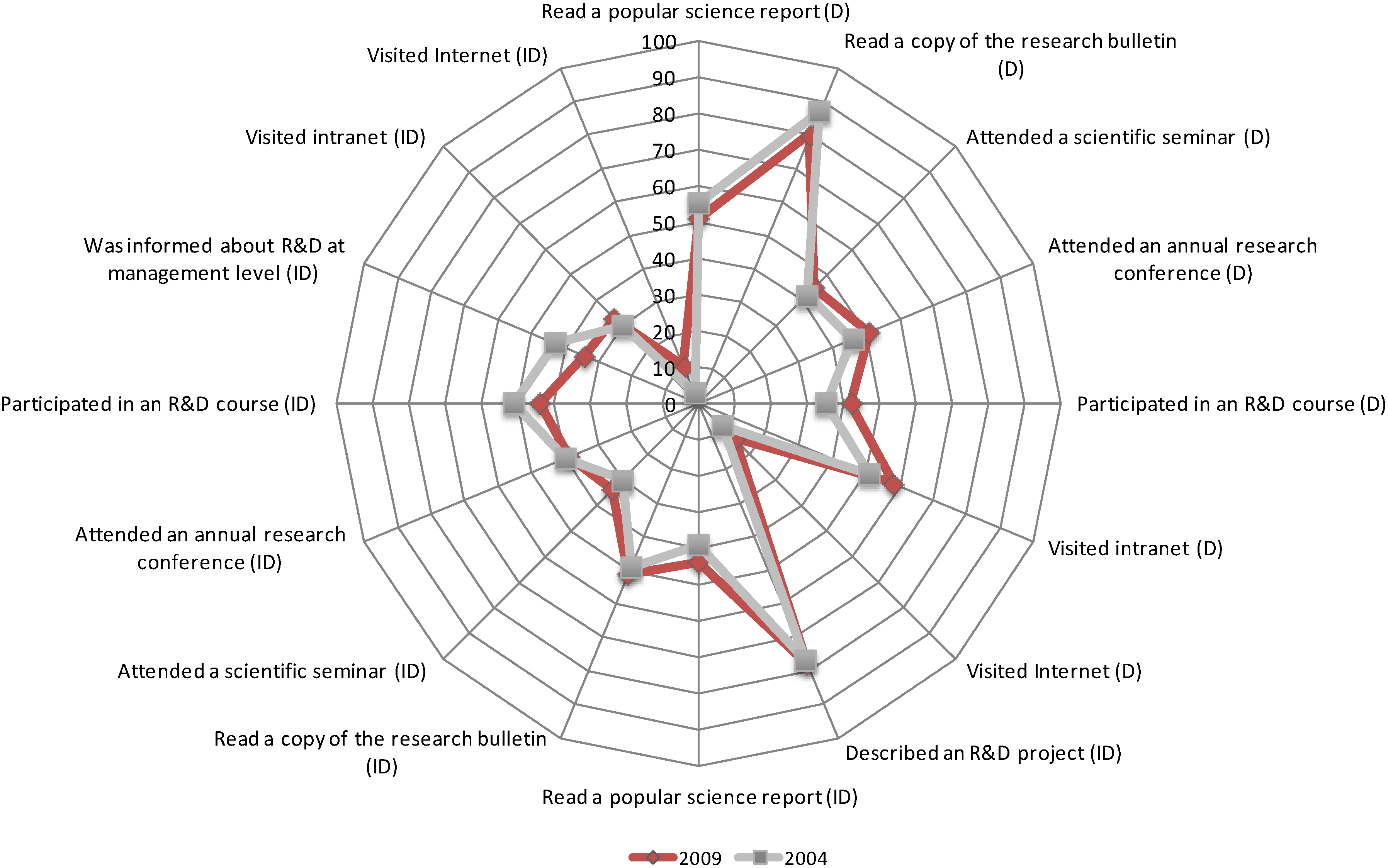
- What is the role of the direct and indirect communication channels in this context?
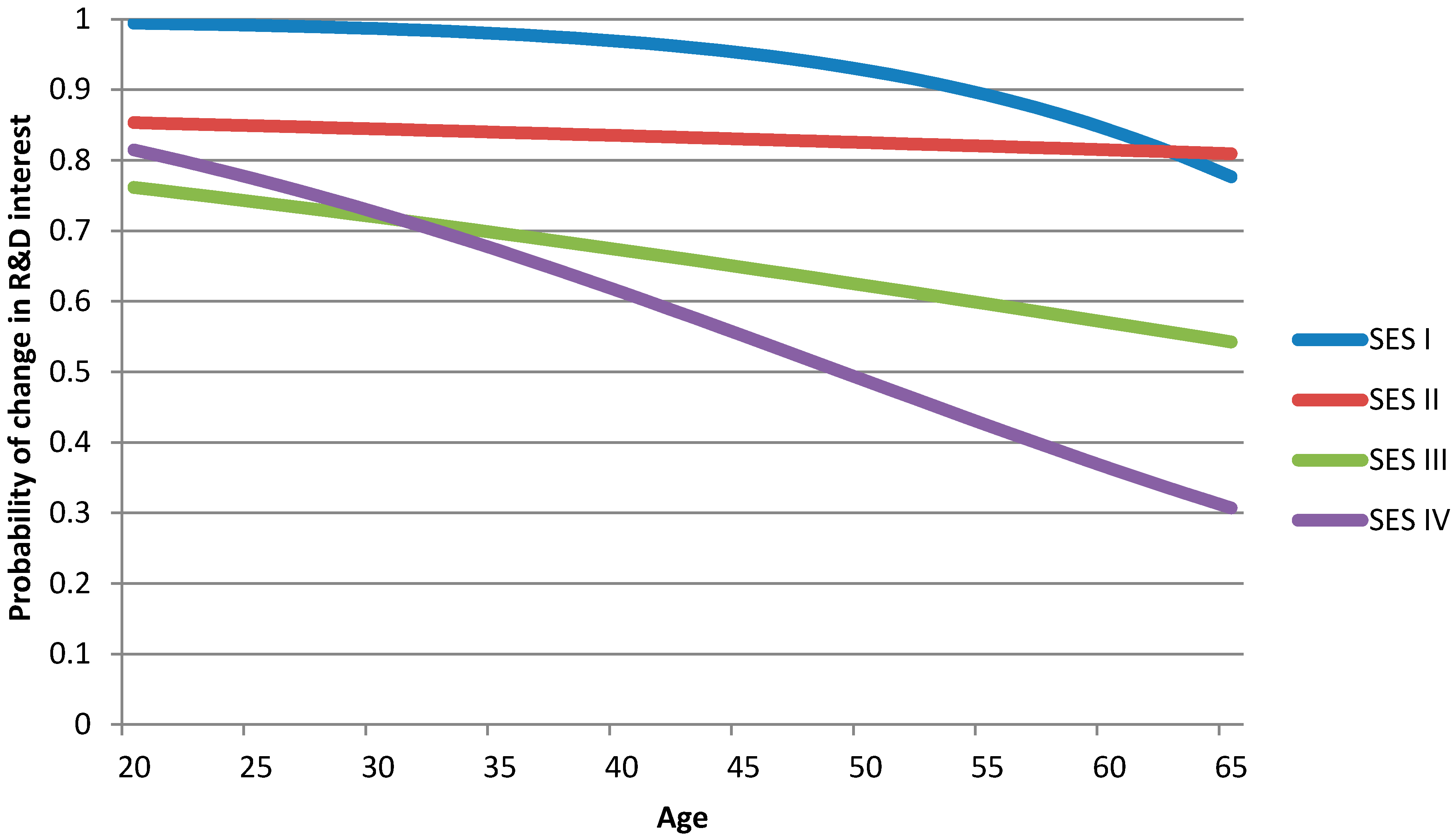
- What is the role of the background variables in the development process?
2. Methods
2.1. Design and Setting
2.2. Strategic Communication Intervention

2.3. Follow Up of the Intervention
2.4. Participants and Data Collection
2.5. Instrument and Statistical Methods
3. Results

{kind=link}
{kind=link}
{kind=link}
| Study Variables | First Measurement | Second Measurement | ||||||
|---|---|---|---|---|---|---|---|---|
| Year 2004 | Year 2009 | |||||||
| n | % | Mean (SD) | Median (IQR) | n | % | Mean (SD) | Median (IQR) | |
| Sex | 846 | 100.0 | 762 | 100.0 | ||||
| Men | 95 | 11.2 | 73 | 9.6 | ||||
| Women | 751 | 88.8 | 688 | 90.4 | ||||
| Age | 846 | 100.0 | 49.5 | 50.0 | 757 | 100.0 | 49.6 | 51.0 |
| (8.8) | (44–56) | (10.1) | (51–58) | |||||
| SES | 820 | 100.0 | 730 | 100.0 | ||||
| I | 71 | 8.7 | 50 | 6.8 | ||||
| Assistant nurse | 71 | 8.7 | 50 | 6.8 | ||||
| II | 205 | 25.0 | 185 | 25.3 | ||||
| Dental nurse (assistant) | 104 | 12.7 | 103 | 14.1 | ||||
| Medical secretary | 51 | 6.2 | 52 | 7.1 | ||||
| Administrative staff | 50 | 6.1 | 30 | 4.1 | ||||
| III | 376 | 45.8 | 340 | 44.6 | ||||
| Nurse | 51 | 6.2 | 47 | 6.4 | ||||
| District nurse | 159 | 19.4 | 129 | 17.6 | ||||
| Midwife | 36 | 4.4 | 40 | 5.4 | ||||
| Dental hygienist | 38 | 4.6 | 32 | 4.6 | ||||
| Physiotherapist | 56 | 6.8 | 55 | 7.5 | ||||
| Occupational Therapist | 36 | 4.4 | 35 | 4.7 | ||||
| IV | 168 | 20.5 | 155 | 20.3 | ||||
| Physician | 77 | 9.4 | 65 | 8.9 | ||||
| Dentist | 63 | 7.7 | 58 | 7.9 | ||||
| Psychologist | 28 | 3.4 | 32 | 4.4 | ||||
| The Different Communication Ways | Gained R&D Interest 2004 | Gained R&D Interest 2009 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | chi-2 | p | n | % | chi-2 | p | ||
| Through one’s own initiative (direct) | |||||||||
| Read a popular science report | 198 | 54.5 | 1.64 | 0.201 | 184 | 51.5 | 0.09 | 0.768 | |
| Read a copy of the research bulletin | 270 | 87.0 | 148.15 | <0.001 | 252 | 80.2 | 91.68 | <0.001 | |
| Attended a scientific seminar | 190 | 42.1 | 4.74 | 0.030 | 182 | 44.5 | 2.20 | 0.138 | |
| Attended an annual research conference | 211 | 46.4 | 1.07 | 0.302 | 205 | 51.2 | 0.12 | 0.727 | |
| Participated in an R&D course | 195 | 34.9 | 17.85 | <0.001 | 200 | 42.0 | 5.12 | 0.024 | |
| Visited intranet | 211 | 51.2 | 0.12 | 0.731 | 206 | 57.8 | 4.97 | 0.026 | |
| Visited Internet | 153 | 8.5 | 105.42 | <0.001 | 156 | 13.5 | 83.31 | <0.001 | |
| Heard about somebody who had (indirect) | |||||||||
| Described an R&D project | 246 | 76.8 | 70.83 | <0.001 | 228 | 78.1 | 71.86 | <0.001 | |
| Read a popular science report | 163 | 38.7 | 8.40 | 0.004 | 164 | 43.9 | 2.44 | 0.118 | |
| Read a copy of the research bulletin | 172 | 48.8 | 0.09 | 0.760 | 182 | 50.5 | 0.02 | 0.882 | |
| Attended a scientific seminar | 154 | 29.9 | 24.96 | <0.001 | 147 | 34.0 | 15.03 | <0.001 | |
| Attended an annual research conference | 166 | 39.8 | 6.96 | 0.008 | 159 | 39.0 | 7.70 | 0.006 | |
| Participated in an R&D course | 174 | 50.6 | 0.02 | 0.879 | 161 | 43.5 | 2.74 | 0.098 | |
| Been informed about R&D at management level | 162 | 43.2 | 2.99 | 0.084 | 152 | 34.2 | 15.16 | <0.001 | |
| Visited intranet | 163 | 30.1 | 25.92 | <0.001 | 154 | 32.5 | 18.94 | <0.001 | |
| Visited Internet | 141 | 2.8 | 125.45 | <0.001 | 142 | 11.3 | 85.21 | <0.001 | |

| Dependent Variable: R&D Interest | Independent Variable: Age | |||||
|---|---|---|---|---|---|---|
| 1= Interest | ||||||
| 0= No Interest | ||||||
| N | Beta-coefficient | p-value | OR | 95% CI | ||
| SES I | 121 | −0.09 | 0.257 | 0.917 | 0.789–1.065 | |
| SES II | 382 | −0.01 | 0.792 | 0.993 | 0.942–1.047 | |
| SES III | 716 | −0.02 | 0.047 | 0.979 | 0.958–0.988 | |
| SES IV | 323 | −0.05 | <0.0001 | 0.950 | 0.924–0.976 | |

4. Discussion
4.1. Long-Term Interest in R&D
4.2. The Role of the Communication Channels
4.3. Colleagues and Manager Create Interest
4.4. The influence of Networks
4.5. Interest in R&D Is Greatest among Younger Staff Members
4.6. General Discussion
4.7. Limitations
5. Conclusions
Acknowledgments
Conflicts of Interest
References
- Dopson, S.; FitzGerald, L.; Ferlie, E.; Gabbay, J.; Locock, L. No magic targets! Changing clinical practice to become more evidence based. Health Care Manage. Rev. 2002, 27, 35–47. [Google Scholar] [CrossRef] [PubMed]
- De Maeseneer, J.M.; van Driel, M.L.; Green, L.A.; van Weel, C. The need for research in primary care. Lancet 2003, 362, 1314–1319. [Google Scholar]
- Sanson-Fisher, R.W. Diffusion of innovation theory for clinical change. Med. J. Australia 2004, 180, 55–56. [Google Scholar]
- Helfrich, C.D.; Blevins, D.; Smith, J.L.; Kelly, P.A.; Hogan, T.P.; Hagedorn, H.; Dubbert, P.M.; Sales, A.E. Predicting implementation from organizational readiness for change: A study protocol. Implement. Sci. 2011, 6. [Google Scholar] [CrossRef]
- Stewart, M.; Reid, G.; Brown, J.B.; Burge, F.; Dicenso, A.; Watt, S.; McWilliam, C.; Beaulieu, M.D.; Meredith, L. Development and implementation of training for interdisciplinary research in primary health care. Acad. Med. 2010, 85, 974–979. [Google Scholar] [CrossRef] [PubMed]
- Schuster, M.A.; McGlynn, E.A.; Brook, R.H. How good is the quality of health care in the United States? Milbank Quart. 1998, 76, 517–563. [Google Scholar]
- Grol, R. Successes and failures in the implementation of evidence-based guidelines for clinical practice. Med. Care 2001, 39, 46–54. [Google Scholar]
- McGlynn, E.A.; Asch, S.M.; Adams, J.; Keesey, J.; Hicks, J.; DeCristofaro, A.; Kerr, E.A. The quality of health care delivered to adults in the united states. N. Engl. J. Med. 2003, 348, 2635–2645. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Emmons, K.M. How can we increase translation of research into practice? Types of evidence needed. Annu. Rev. Public Health 2007, 28, 413–433. [Google Scholar] [CrossRef] [PubMed]
- Mortenius, H.; Baigi, A.; Palm, L.; Fridlund, B.; Björkelund, C.; Hedberg, B. Impact of the organisational culture on primary care staff members’ intention to engage in research and development. J. Health Organ. Manage. 2014, in press. [Google Scholar]
- Gensichen, J.; Huchzermeier, C.; Aldenhoff, J.B.; Gerlach, F.M.; Hinze-Selch, D. Signals for the initiation of structured diagnostic procedures for depression in primary health care. A practice-relevant evaluation of international guidelines. Z Arztl Fortbild Qualitat. 2005, 99, 57–63. (In German) [Google Scholar]
- Godin, G.; Belanger-Gravel, A.; Eccles, M.; Grimshaw, J. Healthcare professionals’ intentions and behaviours: A systematic review of studies based on social cognitive theories. Implement. Sci. 2008, 3. [Google Scholar] [CrossRef]
- Foy, R.; Eccles, M.; Grimshaw, J. Why does primary care need more implementation research? Fam Pract. 2001, 18, 353–355. [Google Scholar]
- Albert, E.; Mickan, S. Closing the gap and widening the scope: New directions for research capacity building in primary health care. Aust. Fam. Physician 2003, 32, 1038–1040. [Google Scholar] [PubMed]
- Cooke, J. A framework to evaluate research capacity building in health care. BMC Fam. Pract. 2005, 6. [Google Scholar] [CrossRef]
- Malterud, K. Reflexivity and metapositions: Strategies for appraisal of clinical evidence. J. Eval. Clin. Pract. 2002, 8, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Funk, S.G.; Champagne, M.T.; Wiese, R.A.; Tornquist, E.M. Barriers to using research findings in practice: The clinician’s perspective. Appl. Nurs. Res. 1991, 4, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Whitford, D.; Walker, C.; Jelley, D.; Clarke, C.; Watson, B. Developing R&D capacity in a primary care trust: Use of the r&d culture index. Prim. Health Care Res. Dev. 2005, 6, 110–116. [Google Scholar] [CrossRef]
- Jowett, S.; Macleod, J.; Wilson, S.; Hobbs, F. Research in primary care: Extent of involvement and perceived determinants among practitioners from one english region. Brit. J. Gen. Pract. 2000, 50, 387–389. [Google Scholar]
- Dahlin, B.; Kuuse, J. Från Provinsialläkare till Primärvård—En Historisk Exposé (From District Medical Officer to Primary Care—A Historical Survey); Göteborgstryckeriet: Lerum, Sweden, 2010. (In Swedish) [Google Scholar]
- The Law of the Healtcare System in Sweden; Regeringskansliet (Government office of Sweden): Stockholm, Sweden, 1996. (In Swedish)
- Profetto-McGrath, J.; Hesketh, K.L.; Lang, S.; Estabrooks, C.A. A study of critical thinking and research utilization among nurses. West. J. Nurs. Res. 2003, 25, 322–337. [Google Scholar]
- Caldwell, E.; Whitehead, M.; Fleming, J.; Moes, L. Evidence-based practice in everyday clinical practice: Strategies for change in a tertiary occupational therapy department. Aust. Occup. Ther. J. 2008, 55, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Hemmelgarn, A.; Glisson, C.; James, L. Organizational culture and climate: Implications for services and interventions research. Clin. Psychol. Sci. Pract. 2006, 13, 73–89. [Google Scholar] [CrossRef]
- Glisson, C.; Williams, N.J.; Green, P.; Hemmelgarn, A.; Hoagwood, K. The organizational social context of mental health medicaid waiver programs with family support services: Implications for research and practice. Adm. Policy Ment. Health 2014, 41, 32–42. [Google Scholar] [CrossRef] [PubMed]
- Vinnova (Verkets Innovationssystem Swedish Govermental Agancy for Innovation Systems). Forskning—Till Vilken Nytta? (Research—What’s the Use?); Samhällsförlaget: Stockholm, Sweden, 2012. (In Swedish) [Google Scholar]
- Mortenius, H.; Marklund, B.; Palm, L.; Fridlund, B.; Baigi, A. The utilization of knowledge of and interest in research and development among primary care staff by means of strategic communication: A staff cohort study. J. Eval. Clin. Pract. 2012, 4, 768–775. [Google Scholar] [CrossRef]
- Hallahan, K.; Holtzhausen, D.; van Ruler, B.; Vercic, D.; Sriramesh, K. Defining strategic communication. Int J. Strat. Comm. 2007, 1, 3–35. [Google Scholar] [CrossRef]
- Rogers, E.M. Diffusion of Innovations, 5th ed.; Free Press: New York, NY, USA, 2003. [Google Scholar]
- Kitson, A.L.; Rycroft-Malone, J.; Harvey, G.; McCormack, B.; Seers, K.; Titchen, A. Evaluating the successful implementation of evidence into practice using the PARIHS framework: Theoretical and practical challenges. Implement. Sci. 2008, 3. [Google Scholar] [CrossRef]
- Windahl, S.; Olson, J.T.; Signitzer, B. Using Communication Theory: An Introduction to Planned Communication, 2nd ed.; Sage: London, UK, 2008. [Google Scholar]
- Bandura, A. Self-Efficacy: The Exercise of Control; Freeman: New York, NY, USA, 1997. [Google Scholar]
- Rogers, E.M. Lessons for guidelines from the diffusion of innovations. Jt. Comm. J. Qual. Improv. 1995, 21, 324–328. [Google Scholar] [PubMed]
- Mortenius, H.; Marklund, B.; Palm, L.; Björkelund, C.; Baigi, A. The implementation of innovative attitudes and behaviour in primary health care by means of strategic communication: A seven-year follow-up. J. Eval. Clin. Pract. 2011, 3, 659–665. [Google Scholar]
- Rydell, R.J.; McConnell, A.R. Understanding implicit and explicit attitude change: A systems of reasoning analysis. J. Pers. Soc. Psychol. 2006, 91, 995–1008. [Google Scholar] [CrossRef] [PubMed]
- Population Statistics 2009; Statistiska Centralbyrån (SCB): Stockholm, Sweden, 2009.
- Landstingsstatistik (The Provencial Statistics); Landstinget Halland: Halmstad, Sweden, 2009. (In Swedish)
- Glenngård, A.; Hjalte, F.; Svensson; Anell, A.; Bankauskaite, V. Health Systems in Transition; Regional Office for Europe on Behalf of the European Observatory on Health Systems and Policies, WHO: Copenhagen, Denmark, 2005. [Google Scholar]
- Ovhed, I.; van Royen, P.; Hakansson, A. What is the future of primary care research? Probably fairly bright, if we may believe the historical development. Scand. J. Prim. Health Care 2005, 23, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Ahlenius, D. FoU, Forskning och Utveckling (R&D, Research and Development); Landstinget Halland (County Council of Halland): Halmstad, Sweden, 1995. (In Swedish) [Google Scholar]
- McGuire, W.J. Personality and attitude change: An information-processing theory. In Psychological Foundations of Attitudes; Academic Press: New York, NY, USA, 1968. [Google Scholar]
- Palm, L. Kommunikationsplanering. En Handbok på Vetenskaplig Grund (Communication Planning. A Handbook on Evidence-Based Practice); Stundentlitteratur: Lund, Sweden, 2006. (In Swedish) [Google Scholar]
- Macfarlane, F.; Shaw, S.; Greenhalgh, T.; Carter, Y.H. General practices as emergent research organizations: A qualitative study into organizational development. Fam. Pract. 2005, 22, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Stetler, C.B.; Legro, M.W.; Rycroft-Malone, J.; Bowman, C.; Curran, G.; Guihan, M.; Hagedorn, H.; Pineros, S.; Wallace, C.M. Role of “external facilitation” in implementation of research findings: A qualitative evaluation of facilitation experiences in the veterans health administration. Implement. Sci. 2006, 1. [Google Scholar] [CrossRef]
- Fenton, E.; Harvey, J.; Griffiths, F.; Wild, A.; Sturt, J. Reflections from organization science on the development of primary health care research networks. Fam. Pract. 2001, 18, 540–544. [Google Scholar] [CrossRef] [PubMed]
- The World Medical Association. Ethical Principles for Medical Research Involving Human Subjects; World Medical Association Declaration of Helsinki: Washington, DC, USA, 2005. [Google Scholar]
- Statistiska Centralbyrån. Socioekonomisk Indelning (SEI) Swedish Socio-Economic Classification; SCB: Stockholm, Sweden, 1982. [Google Scholar]
- IBM SPSS Statistics for Windows; Version 21.0; IBM Corp.: Armonk, NY, USA, 2012.
- Fleiss, J.L.; Levin, B.; Paik, M.C. Statistical Methods for Rates and Proportions, 3rd ed.; Wiley: Hoboken, NJ, USA, 2003. [Google Scholar]
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regression; Wiley: New York, NY, USA, 1989. [Google Scholar]
- Thompson, D.S.; Estabrooks, C.A.; Scott-Findlay, S.; Moore, K.; Wallin, L. Interventions aimed at increasing research use in nursing: A systematic review. Implement. Sci. 2007, 2. [Google Scholar] [CrossRef]
- Squires, J.; Estabrooks, C.A.; Gustavsson, P.; Wallin, L. Individual determinants of research utilization by nurses: A systematic review update. Implement. Sci 2011, 6. [Google Scholar] [CrossRef]
- Estabrooks, C.A.; Scott, S.; Squires, J.E.; Stevens, B.; O’Brien-Pallas, L.; Watt-Watson, J.; Profetto-McGrath, J.; McGilton, K.; Golden-Biddle, K.; Lander, J.; et al. Patterns of research utilization on patient care units. Implement. Sci. 2008, 3. [Google Scholar] [CrossRef]
- Barnett, L.; Holden, D.; Donoghue, M.; Passey, M.; Birden, H. What’s needed to increase research capacity in rural primary health care? Aust. J. Prim. Health 2005, 11, 45–53. [Google Scholar] [CrossRef]
- Meltzer, D.; Chung, J.; Khalili, P.; Marlow, E.; Arora, V.; Schumock, G.; Burt, R. Exploring the use of social network methods in designing healthcare quality improvement teams. Soc. Sci. Med. 2010, 71, 1119–1130. [Google Scholar] [CrossRef] [PubMed]
- Xyrichis, A.; Lowton, K. What fosters or prevents interprofessional teamworking in primary and community care? A literature review. Int. J. Nurs. Stud. 2008, 45, 140–153. [Google Scholar] [CrossRef] [PubMed]
- Kvarnström, S. Collaboration in Health and Social Care: Service User Participation and Teamwork in Interprofessional Clinical Microsystems. PhD Thesis, Jönköping University, Jönköping, Sweden, 25 May 2011. [Google Scholar]
- Werkö, L. Physicians do not longer rule the health care-roost. Good cooperation between the team and the teamleader is more and more important. Läkartidningen 2003, 100, 2373–2377. [Google Scholar]
- Carlfjord, S. The Challenge of Changing Practice. PhD Thesis, Linköping University, Linköping, Sweden, 1 February 2012. [Google Scholar]
- Holden, L.; Pager, S.; Golenko, X.; Ware, R.S.; Weare, R. Evaluating a team-based approach to research capacity building using a matched-pairs study design. BMC Fam. Pract. 2012, 13. [Google Scholar] [CrossRef]
- Finch, E.; Cornwell, P.; Ward, E.C.; McPhail, S.M. Factors influencing research engagement: Research interest, confidence and experience in an Australian speech-language pathology workforce. BMC Health Serv. Res. 2013, 13. [Google Scholar] [CrossRef] [Green Version]
- Drucker, P.F. The discipline of innovation. Harv. Bus. Rev. 1998, 76, 149–157. [Google Scholar] [PubMed]
- Grimshaw, J.M.; Eccles, M.P.; Lavis, J.N.; Hill, S.J.; Squires, J.E. Knowledge translation of research findings. Implement. Sci. 2012, 7. [Google Scholar] [CrossRef]
- Naik, P.; Raman, K. Understanding the impact of synergy in multimedia communications. J. Market. Res. 2003, 40, 375–388. [Google Scholar] [CrossRef]
- Perry, R.N. Role modeling excellence in clinical nursing practice. Nurse Educ. Pract. 2009, 9, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Shaw, S.; Macfarlane, F.; Greaves, C.; Carter, Y.H. Developing research management and governance capacity in primary care organizations: Transferable learning from a qualitative evaluation of UK pilot sites. Fam. Pract. 2004, 21, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Pickstone, C.; Nancarrow, S.; Cooke, J.; Vernon, W.; Mountain, G.; Boyce, R.A.; Campbell, J. Building research capacity in the allied health professions. Evid. Policy: J. Res. Debate Pract. 2008. [Google Scholar] [CrossRef]
- Frontera, W.R.; Fuhrer, M.J.; Jette, A.M.; Chan, L.; Cooper, R.A.; Duncan, P.W.; Kemp, J.D.; Ottenbacher, K.J.; Peckham, P.H.; Roth, E.J.; et al. Rehabilitation medicine summit: Building research capacity. J. Head Trauma Rehabil. 2006, 21, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Russell, J.; Greenhalgh, T.; Boynton, P.; Rigby, M. Soft networks for bridging the gap between research and practice: Illuminative evaluation of chain. BMJ 2004, 328. [Google Scholar] [CrossRef]
- Berwick, D.M. Disseminating innovations in health care. JAMA 2003, 289, 1969–1975. [Google Scholar] [CrossRef] [PubMed]
- Zwar, N.A.; Weller, D.P.; McCloughan, L.; Traynor, V.J. Supporting research in primary care: Are practice-based research networks the missing link? Med. J. Aust. 2006, 185, 110–113. [Google Scholar]
- Allen, J.; Andrew D., James; Phil, G. Formal versus informal knowledge networks in R&D: A case study using social network analysis. R D Manage. 2007, 37, 179–196. [Google Scholar]
- Jippes, E.; Achterkamp, M.C.; Brand, P.L.; Kiewiet, D.J.; Pols, J.; van Engelen, J.M. Disseminating educational innovations in health care practice: Training versus social networks. Soc. Sci. Med. 2010, 70, 1509–1517. [Google Scholar] [CrossRef] [PubMed]
- Gunn, J.; Morris, K.; Chondros, P. Recruiting general practitioners for practice-based, population health activities—A randomised trial of two approaches. Aust. N. Z. J. Public Health 2002, 26, 276–277. [Google Scholar] [CrossRef] [PubMed]
- Thomas, P. General medical practitioners need to be aware of the theories on which our work depend. Ann. Fam. Med. 2006, 4, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Wallis, K.C.; Poulton, J.L. Internalization: The Origins and Construction of Internal Reality; Open University: Buckingham, Philadelphia, PA, USA, 2001. [Google Scholar]
- Holt, D.T.; Armenakis, A.A.; Feild, H.S.; Harris, S.G. Readiness for organizational change: The systematic development of a scale. J. Appl. Behav. Sci. 2007, 43, 232–255. [Google Scholar] [CrossRef]
- Wallin, L.; Gustavsson, P.; Ehrenberg, A.; Rudman, A. A modest start, but a steady rise in research use: A longitudinal study of nurses during the first five years in professional life. Implement. Sci. 2012, 7. [Google Scholar] [CrossRef]
- Jette, D.U.; Bacon, K.; Batty, C.; Carlson, M.; Ferland, A.; Hemingway, R.D.; Hill, J.C.; Ogilvie, L.; Volk, D. Evidence-based practice: Beliefs, attitudes, knowledge, and behaviors of physical therapists. Phys. Ther. 2003, 83, 786–805. [Google Scholar] [PubMed]
- Forsman, H.; Gustavsson, P.; Ehrenberg, A.; Rudman, A.; Wallin, L. Research use in clinical practice—Extent and patterns among nurses one and three years postgraduation. J. Adv. Nurs. 2009, 65, 1195–1206. [Google Scholar] [CrossRef] [PubMed]
- Iles, R.; Davidson, M. Evidence based practice: A survey of physiotherapists’ current practice. Physiother. Res. Int. 2006, 11, 93–103. [Google Scholar] [CrossRef] [PubMed]
- McCluskey, A. Occupational therapists report a low level of knowledge, skill and involvement in evidence-based practice. Aust. Occup. Ther. J. 2003, 50, 3–12. [Google Scholar] [CrossRef]
- Ilott, L.; Bury, T. Research capacity: A challenge for the therapy professions. Physiotherapy 2002, 88, 194–200. [Google Scholar] [CrossRef]
- Pettigrew, A.; Woodman, R.; Cameron, K. Studying organizational changes and development: Challenges for future research. Acad. Manage. J. 2001, 44, 697–713. [Google Scholar] [CrossRef]
- Rickard, C.M.; Williams, G.; Ray-Barruel, G.; Armit, L.; Perry, C.J.; Luke, H.; Duffy, P.; Wallis, M. Towards improved organisational support for nurses working in research roles in the clinical setting: A mixed method investigation. Collegian 2011, 18, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Burstrom, B. Market-oriented, demand-driven health care reforms and equity in health and health care utilization in sweden. Int. J. Health Serv. 2009, 39, 271–285. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, L.; Dopson, S. Professional Boundaries and the Diffusion of Innovation; Oxford University Press: Oxford, UK, 2005. [Google Scholar]
- Smith, P.; Hampson, L.; Scott, J.; Bower, K. Introducing innovation in a management development programme for a UK primary care organisation. J. Health Organ. Manage. 2011, 25, 261–280. [Google Scholar]
- Schein, E.H. Organizational Culture and Leadership, 2nd ed.; Jossey-Bass: San Francisco, CA, USA, 2004. [Google Scholar]
- Sanchez, P.M. Organizational Culture, 2nd ed.; Jossey-Bass: San Francisco, CA, USA, 2011. [Google Scholar]
- Vårdval (Genomförandet av Vårdval i Primärvården); Socialstyrelsen (National Board of Health and Welfare): Stockholm, Sweden, 2010. (In Swedish)
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Morténius, H. Creating an Interest in Research and Development as a Means of Reducing the Gap between Theory and Practice in Primary Care: An Interventional Study Based on Strategic Communication. Int. J. Environ. Res. Public Health 2014, 11, 8689-8708. https://doi.org/10.3390/ijerph110908689
Morténius H. Creating an Interest in Research and Development as a Means of Reducing the Gap between Theory and Practice in Primary Care: An Interventional Study Based on Strategic Communication. International Journal of Environmental Research and Public Health. 2014; 11(9):8689-8708. https://doi.org/10.3390/ijerph110908689
Chicago/Turabian StyleMorténius, Helena. 2014. "Creating an Interest in Research and Development as a Means of Reducing the Gap between Theory and Practice in Primary Care: An Interventional Study Based on Strategic Communication" International Journal of Environmental Research and Public Health 11, no. 9: 8689-8708. https://doi.org/10.3390/ijerph110908689