1. Introduction
Scientists have suggested that most of the human health effects of climate change will be adverse [
1,
2]. The Intergovernmental Panel on Climate Change (IPCC) has also highlighted the many effects of temperature variations on human health, including the effects on temperature-sensitive chronic diseases [
3]. Among cardiovascular diseases, the likely direct impact is on acute myocardial infarction (AMI), a major cause of death and disability worldwide [
4,
5], because winter weather and heat waves primarily cause death by AMI [
6]. Dilaveris
et al. also reported that ambient temperature is an important predictor of AMI mortality [
7].
Several studies have shown the effect of both high and low temperatures on AMI hospital admissions [
8,
9,
10,
11,
12] and mortality [
7,
13,
14,
15]. Bhaskaran
et al., in an extensive review of prior studies, showed that both hot and cold weather had negative effects on the short-term AMI risk [
16]. Cheng and Su reported that increased physical stress caused by heat and cold was related to an increase in blood pressure and vasoconstriction, which may lead to AMI [
17]. Moreover, a study in South Korea demonstrated that the threshold temperature differed according to geographic location as well as the risk of AMI occurrence shown during both heat and cold exposure at threshold temperatures [
18].
An increased susceptibility to temperature according to demographic population factors such as gender and age has become an issue of interest in the scientific community [
19,
20,
21]. A number of studies have shown that the elderly and females were the populations most susceptible to temperature-associated AMI [
9,
10,
13,
15]. In contrast, in Copenhagen (Denmark) the strongest association between temperature and AMI hospital admissions was observed in males and younger age (19–65) groups [
8]. Further, Wichmann
et al. reported that no susceptible groups were identified based on age or sex [
22].
Most previous studies have evaluated susceptible populations according to age and gender, while data on vulnerability factors related to population density (living area) and individual socioeconomic status (SES) remain unclear or inadequate [
20,
23,
24]. Living in densely populated urban areas was an important risk factor, with many individuals vulnerable to adverse heat-related health outcomes because of the urban heat island effect [
25]. However, Hattis
et al. reported demographic characteristics such as age and ethnicity were more important factors than urbanization [
26]. Most have studies focused on mortality due to urban heat effects, with lack of evidence for cold effects.
Recently, socioeconomic factors (e.g., education and income) have also been considered as an important component of vulnerability to temperature-associated mortality [
23]. Among the elderly, those with underlying cardiovascular disease (CVD), and those who are poor, uneducated, or isolated begin to experience a rapid rise in mortality in extreme weather because of their lack of access to educational material and information resources, as well as their impaired physiological responsiveness [
27,
28]. Low SES status has been found to compound the relationship between temperature and mortality [
29,
30]. Moreover, low SES may be associated with inequality of adaptation or ability to mitigate responses to climate change [
31,
32]. A few studies have shown individual SES is independently and significantly associated with the incidence of AMI [
33,
34], while little is known about the effect of temperature on AMI hospital admissions or mortality by individual SES.
The objective of this study was to determine the associations between temperature and AMI hospital admissions by subpopulation (gender, age, living area, and SES) using the Korea National Health Insurance (KNHI) database, which covers the entire South Korean population [
35]. The seasons were divided into hot, cold, and warm weather periods to determine the differences in heat and cold effects at extreme and mild temperatures. We aimed to determine the association between threshold temperatures and relative risk (RR) for vulnerability to heat and cold on AMI hospital admissions in each weather period, according to living area (urban or rural) and individual SES among subpopulations.
2. Materials and Methods
2.1. Study Area
The study area was South Korea (latitude is 37°00′ N and longitude is 127°30′ E), located in the southern part of the Korean peninsula in Eastern Asia. South Korea has an area of 99,720 square km (38,502 square miles) and a 2413 km (1499 mile)-long coastline [
36,
37]. The population of South Korea in July 2014 was estimated at about 50 million [
38]. There are four seasons in a year in South Korea, according to Meteorological Administration climate data, with characteristics as follows [
39]: Summer (June–August) shows high temperatures and humidity under the influence of the North Pacific high pressure system; winters (December–February) are cold and dry under the influence of continental high pressure systems; spring (March–May) and autumn (September–November) are often clear and dry due to the impact of migratory anticyclones.
2.2. Health Outcome Data
We obtained daily AMI hospital admission data from the Korea National Health Insurance Corporation (KNHIC) covering the period from 1 January 2004 to 31 December 2012. The primary diagnosis code of AMI was I210–214 and 219 according to the International Classification of Diseases 10th revision (ICD-10). We excluded AMI hospital admissions that occurred within 30 days after a previous AMI hospital admission because readmissions following discharge for AMI within a month are regarded as recurrences [
40]. We divided vulnerable populations by individual SES according to enrollment in National Health Insurance (NHI) or medical assistance (Medicaid). NHI covers about 97% of the general Korean population; the other 3% in low-income brackets are covered by Medicaid [
41]. Moreover, health insurance premiums for NHI are also used as a surrogate for income in South Korea [
42]. We classified insurance premiums into three groups of low, medium, or high. Living area was divided based on population density. Cities with 500,000 or more residents were considered urban areas and counties with less than 500,000 residents were considered rural areas based on data from the Ministry of Security and Public Administration (MOSPA) in South Korea [
43].
2.3. Climatological Data and Air Pollution Data
The climatological and air pollution data for 1 January 2004 to 31 December 2012 were used to assess the health outcomes for the same period. We obtained daily meteorological data from the Korea Meteorological Administration, including mean, maximum, and minimum temperatures (°C), relative humidity (%), precipitation, and sea-level pressure. These elements were observed at 68 weather stations. The air pollution data, including particulate matter (PM10), nitrogen dioxide (NO2), sulfur dioxide (SO2), carbon monoxide (CO), and ozone (O3) were obtained from the National Institute of Environmental Research. Daily air pollution monitoring was conducted at 238 sites located based on population density and covering all regions of South Korea.
2.4. Statistical Analysis
Most studies have used threshold temperatures based on percentiles such as the interquartile range (IQR) in study periods [
8,
14,
44], but did not estimate the actual threshold temperatures that would show an increase in the risk of AMI. However, Lee
et al. reported that piecewise regression (PR) analysis performed after plotting temperature and daily hospital admissions would be a better approach for identifying the threshold temperature [
18]. We used threshold temperatures based on piecewise regression (PR) analysis to determine the inflection point of the relationship between daily adjusted hospital admissions and temperature by maximum R
2.
We explored the effects of air temperature on AMI hospital admissions in hot (June–August), cold (December–February), and warm (March–May and September–November) weather periods. The thresholds for mean and maximum temperatures were used for determining the effect of heat in summer, while the thresholds for mean and minimum temperatures were used for assessing the effect of cold in winter. The warm period, corresponding to the change of seasons between summer and winter, generally had a moderate climate; therefore, we estimated the mean thresholds for heat and cold.
We also used generalized additive models (GAMs) analysis with smoothing spline functions to describe nonlinear relationships for time-series. We considered potential confounders such as long-term trends using the calendar year and the day of the week because hospital admissions have unique day patterns, with the highest numbers occurring on Monday and the lowest numbers observed on Saturday, Sunday, and holidays. The relationships were adjusted for humidity, sea-level pressure, amount of air pollutants (PM
10, O
3, and NO
2) using the spline function, and the annual population size was considered as the offset variable in GAMs. In addition, we added the duration of a heat or cold wave into the GAMs for evaluation of the effects of extreme weather events in hot and cold weather periods. In South Korea, a heat wave is defined the heat index (HI) exceeds 41 °C using the maximum temperature and humidity, while a cold wave is defined by a daily minimum temperature of under −12 °C [
39]. The relative risk (RR) were calculated for AMI hospital admissions per 1 °C above the mean and maximum threshold temperatures for heat as well as per 1 °C below the mean and minimum threshold temperatures for cold. To compare the RR for different subgroups, we used the same threshold temperatures.
Moreover, the effects of cold have been reported to be associated with delays, therefore the remaining terms covered delays of up to 28 days with weekly groupings chosen to allow more precise estimations of the effect and because at longer lags, any temperature effects would be unlikely to vary considerably from day to day [
10]. Therefore, we analyzed risks for lags of 0, 1, 2–3, 4–7, 8–14, 15–21, and 22–28 days, respectively, in hot and cold weather. Lag was defined as the effect of the current day; lag 1 was the temperature on the prior 1 day, and lag X-Y was the average of prior X and Y days. However, in warm weather we analyzed risks for lags up to 6 days. We did not observe long-term lag effects in warm weather because of unpredictable weather during those seasons.
To confirm the general relationship between daily AMI hospital admissions and mean temperature (lag0), the smoothing spline was used with three degrees of freedom (df) for the confounding factors, such as day of the week, precipitation, humidity, sea-level pressure, air pollutants (PM10, O3, NO2), and annual population size by subgroups. We also used piecewise regression (PR) analysis to confirm the threshold temperature when the group showed distinctly higher risk curves.
We analyzed and compared the risks among several subpopulations in each period (hot, cold, or warm) by gender, age (20–74 or ≥75 years), living area (urban or rural), and individual SES. The SES was based on type of health insurance (NHI or Medicaid) and insurance premium (low, medium, or high). Data were analyzed using the statistical software SAS version 9.3 for Windows (SAS Institute Inc., Cary, NC, USA).
4. Discussion
Temperature-associated AMI studies are usually done in both hot/warm and cold weather periods in each country [
8,
44,
45]. However, we divided seasons according to hot (June to August), cold (December to February), and warm (March to May and September to November) weather periods to determine threshold temperatures, because South Korea has distinct seasons. Spring and fall have a generally moderate climate, while summer and winter have extreme weather events, such as heat and cold waves [
46]. We determined 28.5 °C to be the threshold temperature for sudden increases in AMI hospital admissions due to heat in hot weather. Our threshold for heat-related effect for AMI was similar to that found in other countries, such as for Sao Paulo in Brazil (24 °C–27 °C) [
47], and Melbourne in Australia (27 °C–30 °C) [
48], as well as for another South Korean study (27.5 °C–28.5 °C) [
18].
In cold weather periods, the thresholds were determined to be a mean temperature of −8.5 °C and a minimum temperature of −13.5 °C in this study. There have been similar mean threshold temperatures in cold regions, such as in the Czech Republic (−5.7 °C or −7.6 °C) [
49] and in Russia (−6 °C) [
50]. We also calculated the relative risk (RR) below the minimum threshold temperature, because these reflected the extreme low temperatures better than the mean temperature in cold weather, which tend to occur at irregular intervals of about 2–7 days in South Korea [
51]. In warm weather, the threshold temperature was calculated for the effects of both heat and cold because temperatures tend to increase or decrease suddenly. Few studies have reported the threshold temperatures in warm seasons, as in our study. Therefore, we compared the threshold temperatures with those for similar temperature seasons in other countries. The threshold temperature for heat was 18.5 °C, and −0.5 °C for cold in our study. England and Wales showed an estimated threshold of 20 °C for heat in the warmest months (June to August) [
12], and some studies showed a threshold for cold below 0 °C, such as −1.5 °C or −2.5 °C [
18,
52].
Our study evaluated susceptible populations by demographic characteristics, such as gender and age. Precious studies that examined the effects of temperature separately for different groups, have shown inconsistent results. Basu also reported that demographic characteristics (being female and elderly) can modify the severity of effects on temperature through various physiological and behavioral pathways [
21]. Wichmann
et al. reported that no susceptible groups were identified in Gothenburg (Sweden) based on age or gender [
22], while males and 19–65 years seemed to be more susceptible to AMI hospital admissions because males had a higher risk of developing CVD than females, and those in the age group of 19–65 years participated in more outdoor activities in Copenhagen (Denmark) [
8].
However, we determined that females had high risk of AMI hospital admission in cold periods. Females also showed significantly higher RRs above the maximum threshold temperature in hot weather. A risk for heat and cold was observed in females, which is consistent with prior confirmed outcomes [
13,
53,
54]. This could be because females have a higher risk for arrhythmia, ischemia, and high blood pressure, all of which are more affected by extreme hot and cold temperatures [
55].
Among age groups, we found that those ≥75 years showed susceptibility to heat. The effect of cold on those ≥75 years also showed a slightly higher RR than for those aged 20–74 years, but this was not statistically significant. There have been many studies reporting that the elderly were vulnerable both to heat [
12,
56] and cold [
7,
10,
13,
15]. Older people undergo physiological changes in renal function and electrolyte homeostasis in extremely hot weather [
57], and have a weaker thermoregulation system due to reduced cutaneous thermal sensitivity and diminished skin vasoconstriction with cold stress [
58].
We evaluated the association between temperature and AMI hospital admissions by population level (urban or rural area) and individual SES factors in South Korea. Our study showed that urban populations were more susceptible to AMI than rural populations in hot weather and similar risks in cold weather were found in both urban and rural areas. Urban
et al. reported more pronounced effects of heat stress on CVD during warm days in urban areas, while stronger cold effects were observed in a rural population [
49]. Hajat
et al. also showed a greater heat effect on mortality among those living in urban areas, while cold effects were greater in some rural areas [
20]. The heat effect in urban areas is probably due to the heat-island effect, whereby greater heat retention occurs in more heavily built-up areas of large cities, including in South Korea [
59]. Our study did not show a higher risk in the rural population in cold weather, probably because of reduced daily activities in the winter season.
Most studies have reported that lower SES increased the temperature-associated mortality, with SES defined by low income [
60], low education [
24,
61,
62], or living in poverty [
63]. Madrigano
et al. reported that persons living in areas with greater poverty were more susceptible to heat-related AMI occurrence [
44]. However, Wichmann
et al. reported that high SES groups seemed to be more susceptible to cold-related AMI hospital admissions in Copenhagen. This might be because high SES groups live in owned detached houses, so that cold weather behaviors such as snow shoveling could be related to increased ischemic heart disease [
8]. In this study, we focused on evaluating temperature-associated AMI hospital admissions by individual insurance type and premium based on the KNHI data, which covers the general Korean population. Therefore, this study was able to identify the effect of individual SES on increased AMI hospital admissions associated with temperature.
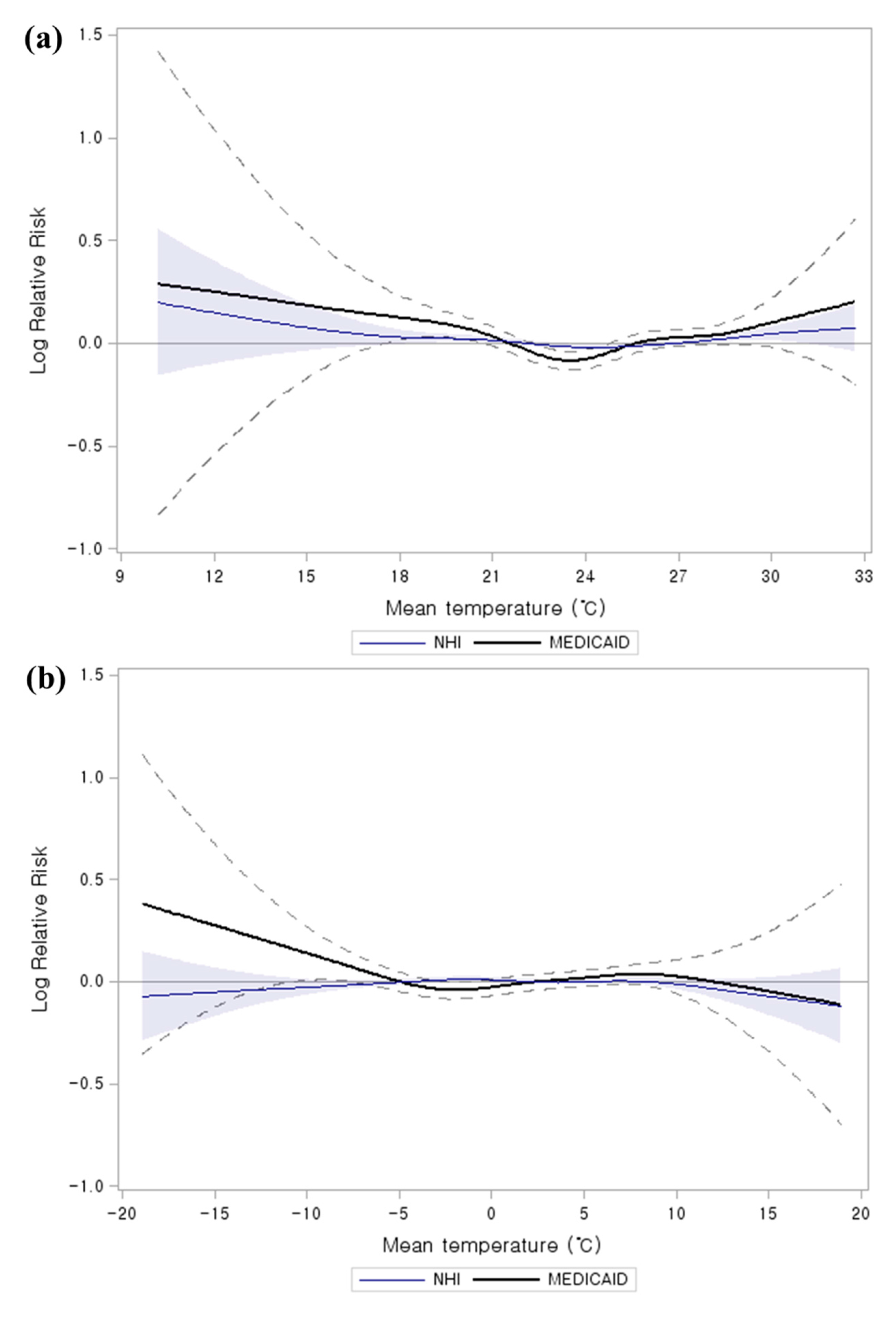
We observed that temperature-related AMI hospital admissions were more pronounced in low SES groups (Medicaid and low premium health insurance) for both heat and cold. The Medicaid population, especially the lowest SES group, had the highest significant RR among subgroups as well as confirmed distinctly higher risk curves both in hot and cold weather [
22]. Most studies showed that persons in low SES groups tend to have inadequate means (e.g., for heating/cooling systems and clothing), live in residences constructed with poor quality materials, and have poor health status [
25,
60]. The low SES population lifestyle seemed to be more vulnerable to weather, which could affect increased AMI hospital admissions.
This study has several limitations. Based on its environmental design, individual exposure levels to meteorological conditions and air pollutants were estimated by area monitoring data. Individual medical history or personal behaviors were not reflected because of lack of information. We also would not have included pre-hospitalization fatal AMIs. However, we used the data from KNHI, which is the only insurance program that universally covers the Korean population. Despite these limitations, we identified the risk of temperature-related AMI hospital admissions by gender, age, and living area, and individual-SES.



{kind=link}
