
Lung Cancer Mortality Trends in China from 1988 to 2013: New Challenges and Opportunities for the Government

Abstract
:1. Introduction
2. Materials and Methods
3. Results
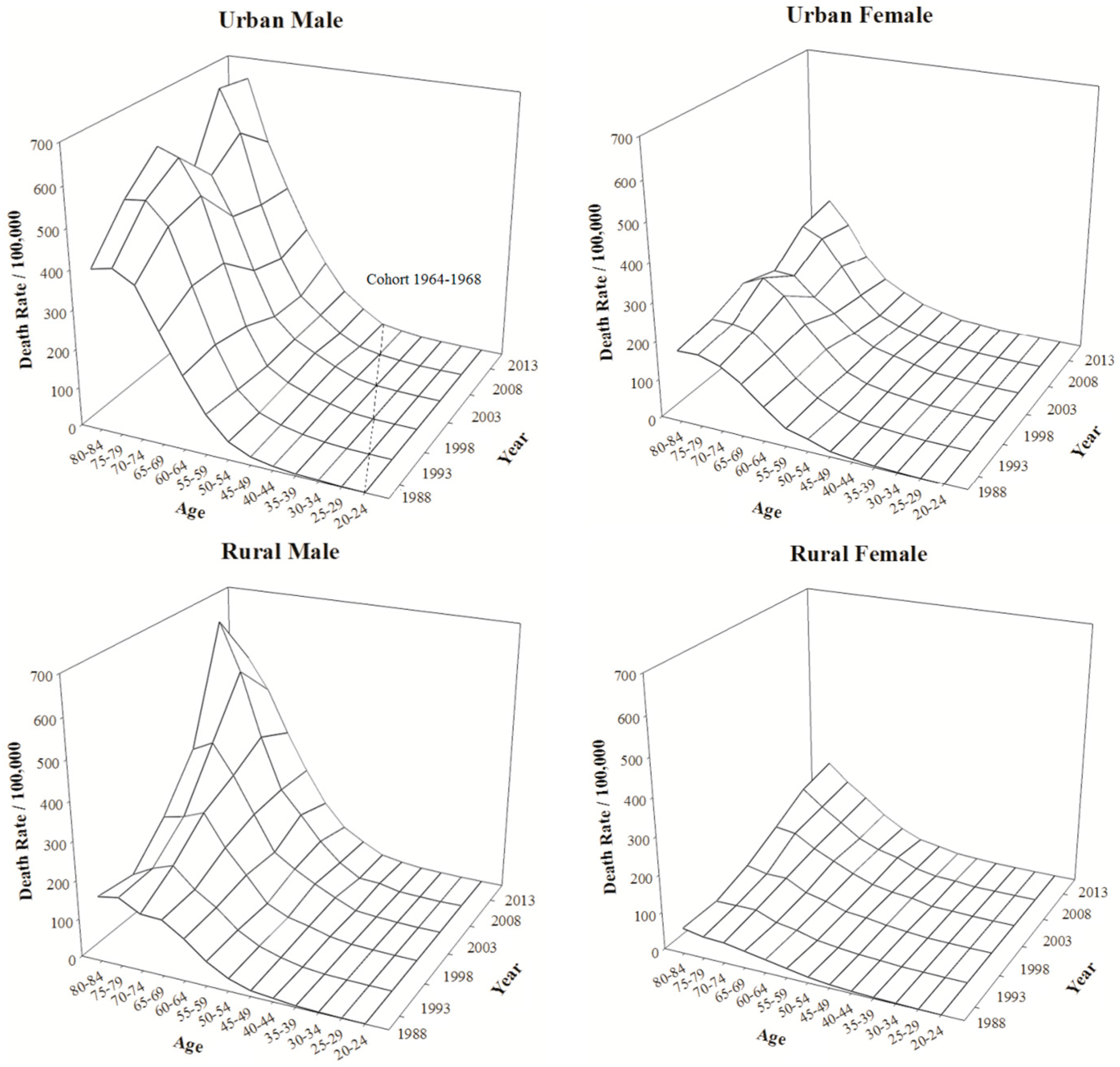
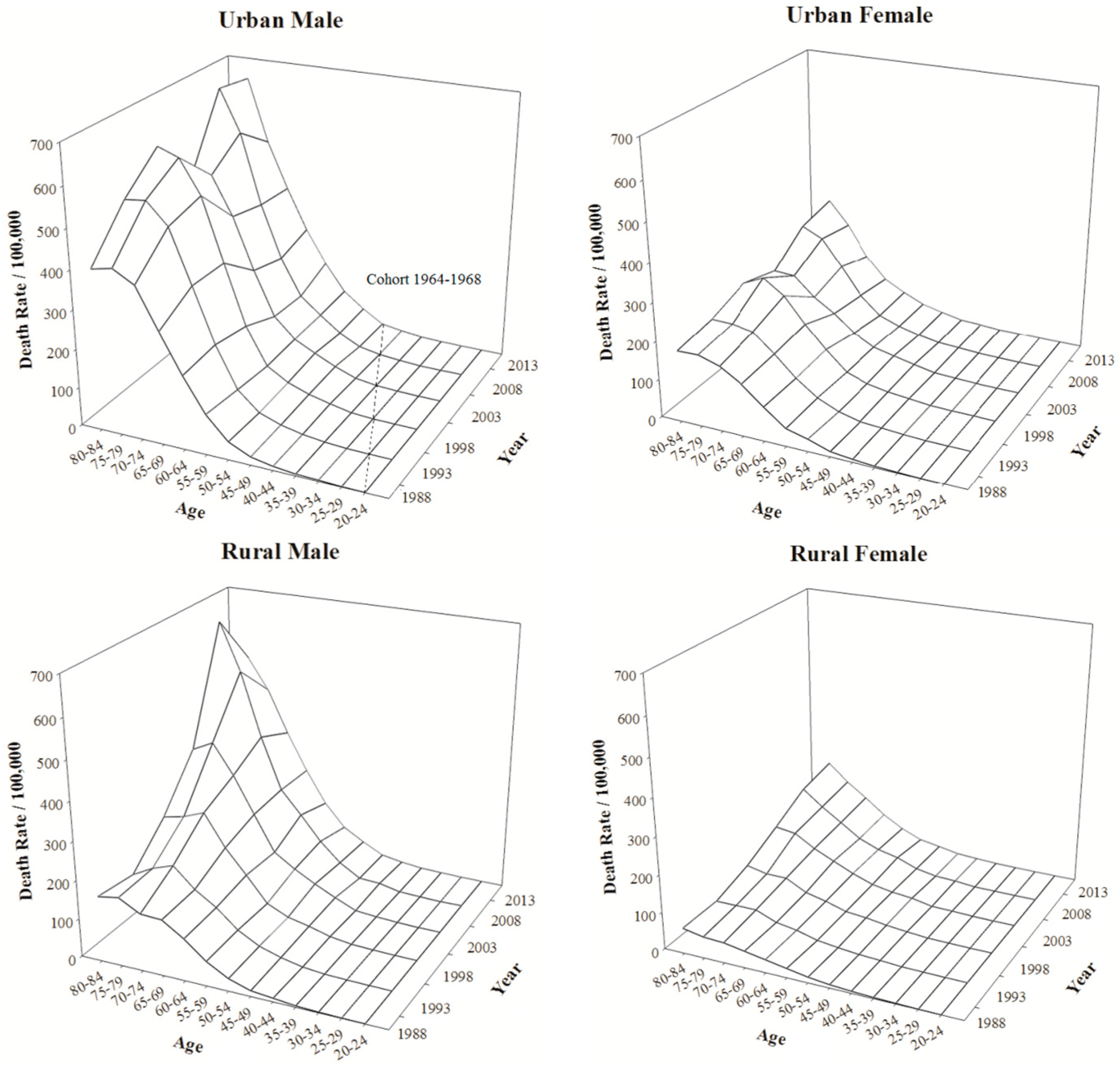
3.1. Descriptive Analysis of Age-Specific Mortality Rates of Lung Cancer
3.2. Model Comparison
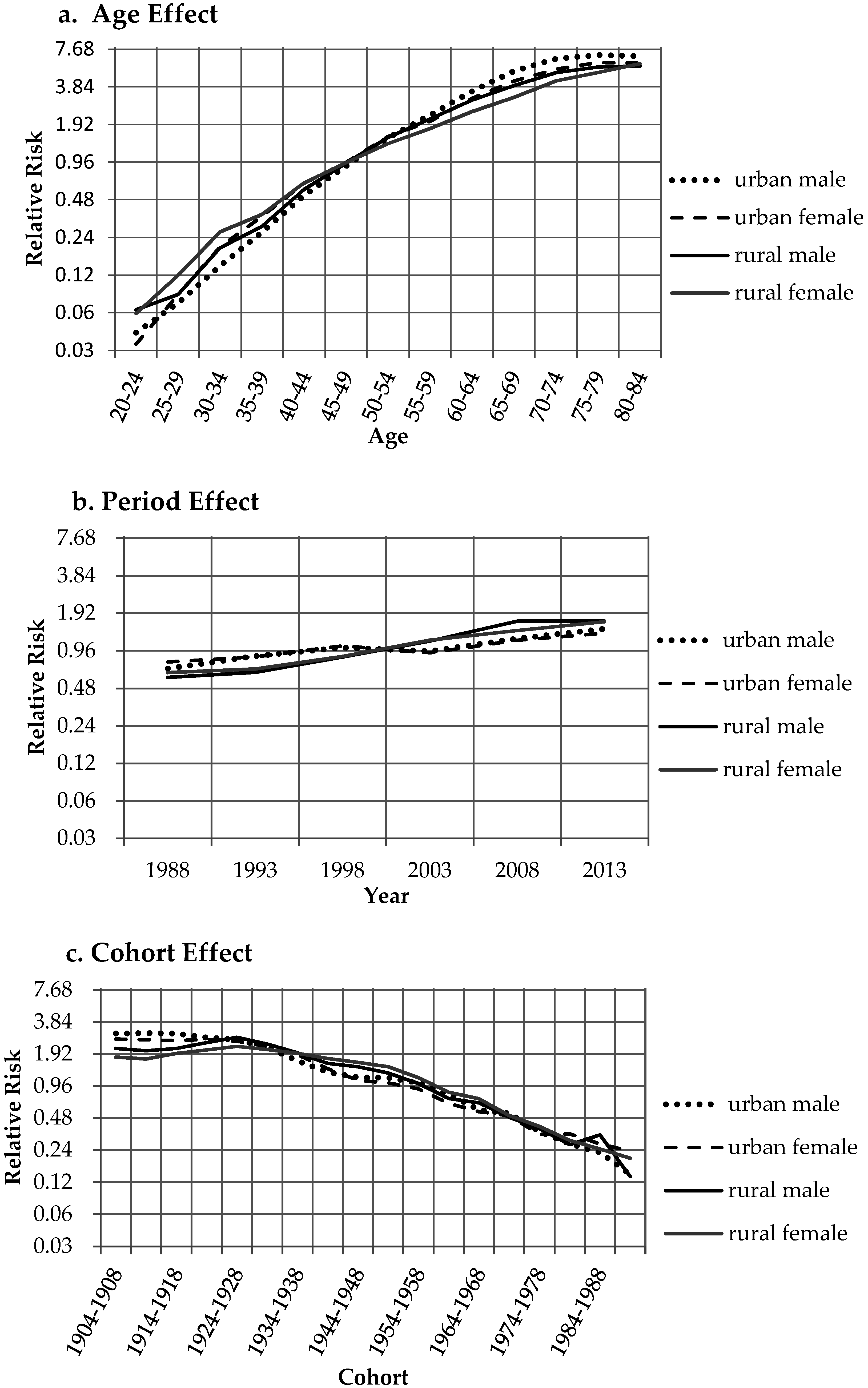
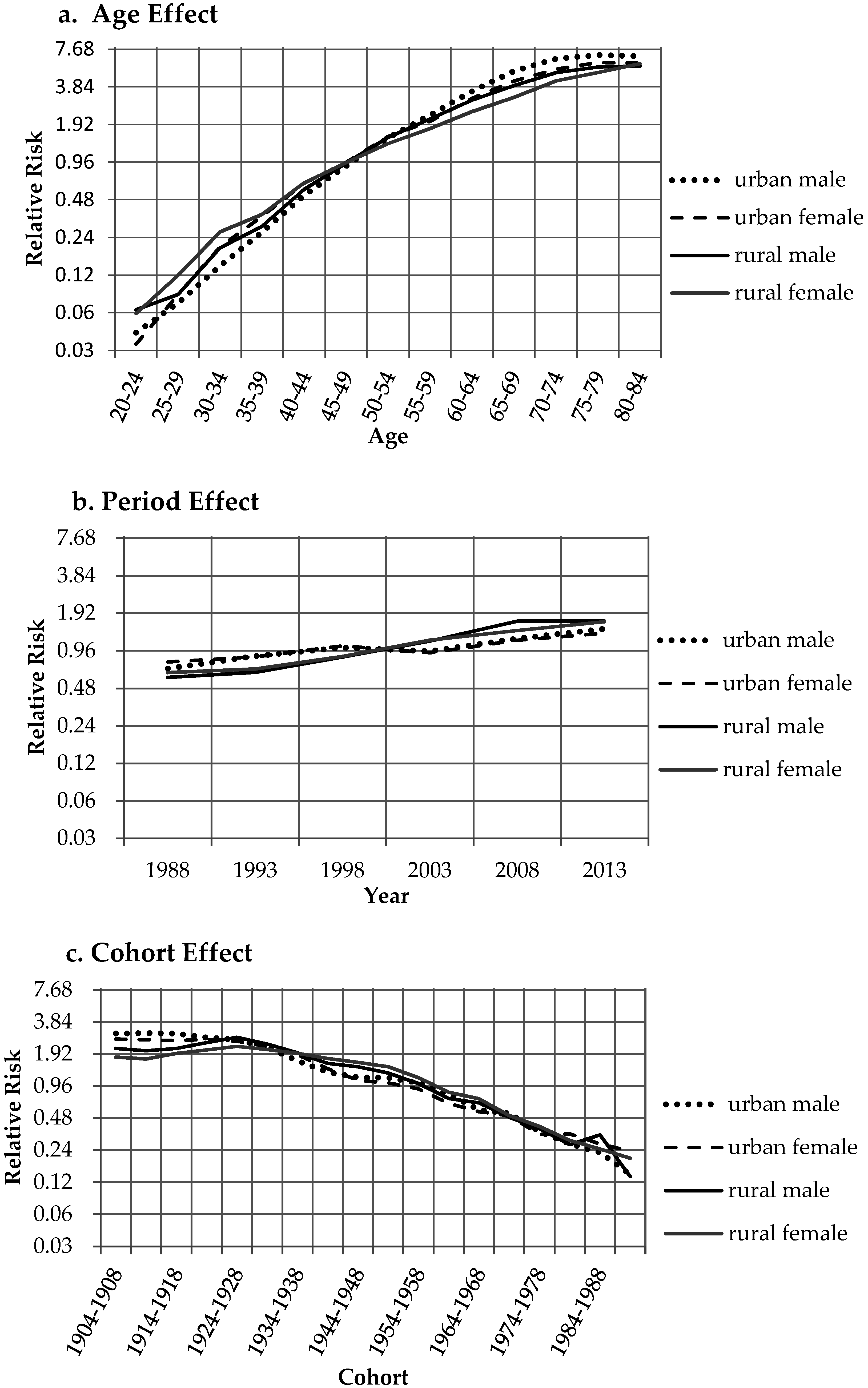
3.3. Age-Period-Cohort Analysis
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix

{kind=link}
{kind=link}
| Sex | Year | |||
|---|---|---|---|---|
| 1984 | 1996 | 2002 | 2010 | |
| Male | 62.0 | 63.0 | 57.4 | 52.9 |
| Female | 7.0 | 3.8 | 2.6 | 2.4 |
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.J.; Bi, Y.; Li, S.; Zhang, Q.; Zhao, G.; Guo, Y.; Song, Q. Reduced risk of lung cancer with metformin therapy in diabetic patients: A systematic review and meta-analysis. Am. J. Epidemiol. 2014, 180, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.J.; Li, S. The prognostic value of metformin for cancer patients with concurrent diabetes: A systematic review and meta-analysis. Diabetes Obes. Metab. 2014, 16, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Fitzmaurice, C.; Dicker, D.; Pain, A.; Hamavid, H.; Moradi-Lakeh, M.; MacIntyre, M.F.; Allen, C.; Hansen, G.; Woodbrook, R.; Wolfe, C.; et al. The global burden of cancer 2013. JAMA Oncol. 2015, 1, 505–527. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zhang, S.; Zou, X. Estimation and projection of lung cancer incidence and mortality in China. Chin. J. Lung Cancer 2010, 13, 488–493. [Google Scholar]
- Fang, J.; Dong, H.; Wu, K.; Du, P.; Xu, Z.; Lin, K. Characteristics and prediction of lung cancer mortality in China from 1991 to 2013. Asian Pac. J. Cancer Prev. 2015, 16, 5829–5834. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zheng, R.; Zeng, H. Bayesian age-period-cohort prediction of lung cancer incidence in China. Thorac. Cancer 2011, 2, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Lin, X.; Zhang, L.; Li, Y.; Xie, S.; Yang, M.; Guo, J.; Lin, E.; Liu, Q.; Hong, M.; et al. Secular trend analysis of lung cancer incidence in Sihui city, China between 1987 and 2011. Chin. J. Cancer 2015, 34, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Mason, K.O.; Mason, W.M.; Winsborough, H.H.; Poole, W.K. Some methodological issues in cohort analysis of archival data. Am. Sociol. Rev. 1973, 38, 242–258. [Google Scholar] [CrossRef]
- Yang, Y. Trends in U.S. adult chronic disease mortality, 1960–1999: Age, period, and cohort variations. Demography 2008, 45, 387–416. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Statistics Annual 1993; WHO: Geneva, Switzerland, 1994. [Google Scholar]
- Rao, K.; Chen, Y.; Chen, X.; Al, E. Selection of a national area sample for acquisition of national health information in China. Chin. Health Stat. 1992, 9, 1–6. [Google Scholar]
- Yang, L.; Parkin, D.M.; Li, L.D.; Chen, Y.D. A comparison of the sources of cancer mortality in China. Cancer Cause Control 2004, 15, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Fu, W. Ridge estimator in singular design with application to age-period-cohort analysis of disease rates. Commun. Stat. Theory Methods 2000, 29, 263–278. [Google Scholar] [CrossRef]
- Yang, Y.; Schulhofer-Wohl, S.; Fu, W.; Land, K.C. The intrinsic estimator for age-period-cohort analysis: What it is and how to use it. Am. J. Sociol. 2008, 113, 1697–1736. [Google Scholar] [CrossRef]
- Yang, Y.; Fu, W.; Land, K.C. A methodological comparison of age-period-cohort models: The intrinsic estimator and conventional generalized linear models. Am. J. Sociol. 2004, 34, 75–110. [Google Scholar] [CrossRef]
- O’Brien, R.M. The age-period-cohort conundrum as two fundamental problems. Qual. Quant. 2011, 45, 1429–1444. [Google Scholar] [CrossRef]
- Pelzer, B.; Te, G.M.; Eisinga, R.; Schmidt-Catran, A.W. The non-uniqueness property of the intrinsic estimator in APC models. Demography 2015, 52, 315–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, F. Cohort patterns in mortality trends among the elderly in seven European countries, 1950–1999. Int. J. Epidemiol. 2005, 34, 1149–1159. [Google Scholar] [CrossRef] [PubMed]
- Reither, E.N.; Hauser, R.M.; Yang, Y. Do birth cohorts matter? Age-period-cohort analyses of the obesity epidemic in the United States. Soc. Sci. Med. 2009, 69, 1439–1448. [Google Scholar] [CrossRef] [PubMed]
- Straif, K.; Cohen, A.; Samet, J. Air Pollution and Cancer; IARC Scientific Publication No. 161; IARC Press: Lyon, France, 2013; pp. 1–169. [Google Scholar]
- Guo, Y.; Zeng, H.; Zheng, R.; Li, S.; Barnett, A.G.; Zhang, S.; Zou, X.; Huxley, R.R.; Chen, W.; Williams, G. Lung cancer incidence and ambient air pollution in China: A spatial age-period cohort study 1990–2009. Lancet 2015. [Google Scholar] [CrossRef]
- Peng, J.; Chen, S.; Lü, H.; Liu, Y.; Wu, J. Spatiotemporal patterns of remotely sensed PM2.5 concentration in China from 1999 to 2011. Remote Sens. Environ. 2016, 174, 109–121. [Google Scholar] [CrossRef]
- Zhang, Y.; Cao, F. Fine particulate matter (PM2.5) in China at a city level. Sci. Rep. 2015. [Google Scholar] [CrossRef] [PubMed]
- Bidoli, E.; Pappagallo, M.; Birri, S.; Frova, L.; Zanier, L.; Serraino, D. Residential proximity to major roadways and lung cancer mortality. Italy, 1990–2010: An observational study. Int. J. Environ. Res. Public Health 2016, 13, 191. [Google Scholar] [CrossRef] [PubMed]
- Bittoni, M.A.; Wexler, R.; Spees, C.K.; Clinton, S.K.; Taylor, C.A. Lack of private health insurance is associated with higher mortality from cancer and other chronic diseases, poor diet quality, and inflammatory biomarkers in the United States. Prev. Med. 2015, 81, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, A.R.; Kroon, L.; Chen, L.; Li, C.I.; Jones, B. Insurance status and risk of cancer mortality among adolescents and young adults. Cancer Am. Cancer Soc. 2015, 121, 1279–1286. [Google Scholar] [CrossRef] [PubMed]
- Niu, X.; Roche, L.M.; Pawlish, K.S.; Henry, K.A. Cancer survival disparities by health insurance status. Cancer Med. 2013, 2, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zheng, R.; Zeng, H.; Zhang, S.; He, J. Annual report on status of cancer in China, 2011. Chin. J. Cancer Res. 2015, 27, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Allemani, C.; Weir, H.K.; Carreira, H.; Harewood, R.; Spika, D.; Wang, X.; Bannon, F.; Ahn, J.V.; Johnson, C.J.; Bonaventure, A.; et al. Global surveillance of cancer survival 1995–2009: Analysis of individual data for 25,676,887 patients from 279 population-based registries in 67 countries (CONCORD-2). Lancet 2015, 385, 977–1010. [Google Scholar] [CrossRef]
- Eilstein, D.; Eshai, K. Lung and breast cancer mortality among women in France: Future trends. Cancer Epidemiol. 2012, 36, 341–348. [Google Scholar] [CrossRef] [PubMed]
- John, U.; Hanke, M. Age- and sex-specific trends in lung cancer mortality over 62 years in a nation with a low effort in cancer prevention. Int. J. Environ. Res. Public Health 2016, 13, 362. [Google Scholar] [CrossRef] [PubMed]
- Cayuela, A.; Rodríguez-Domínguez, S.; López-Campos, J.L.; Vigil, E. Age-period-cohort analysis of lung cancer mortality rates in Andalusia, 1975–2004. Lung Cancer 2007, 57, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Mukhtar, H. Dietary agents for prevention and treatment of lung cancer. Cancer Lett. 2015, 359, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Wang, Y.; Wu, Y.; Yang, J.; Wan, X. The road to effective tobacco control in China. Lancet 2015, 385, 1019–1028. [Google Scholar] [CrossRef]
- Zhu, C.; Young-soo, S.; Beaglehole, R. Tobacco control in China: Small steps towards a giant leap. Lancet 2012, 379, 779–780. [Google Scholar] [CrossRef]
- Chinese Center for Disease Control and Prevention. Global Adult Tobacco Survey (GATS) China Country Report; Chinese Center for Disease Control and Prevention: Beijing, China, 2011. [Google Scholar]
- Zhang, Z.J. One author replies. Am. J. Epidemiol. 2014, 180, 1217–1218. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.J.; Zheng, Z.J.; Kan, H.; Song, Y.; Cui, W.; Zhao, G.; Kip, K.E. Reduced risk of colorectal cancer with metformin therapy in patients with type 2 diabetes-a meta-analysis. Diabetes Care 2011, 34, 2323–2328. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.J.; Zheng, Z.J.; Shi, R.; Su, Q.; Jiang, Q.; Kip, K.E. Metformin for Liver Cancer Prevention in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. J. Clin. Endocrinol. Metab. 2012, 97, 2347–2353. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.J. One author replies. Am. J. Epidemiol. 2014, 180, 1131–1132. [Google Scholar] [CrossRef] [PubMed]
- Chung, R.Y.; Schooling, C.M.; Cowling, B.J.; Leung, G.M. How does socioeconomic development affect risk of mortality? An age-period-cohort analysis from a recently transitioned population in China. Am. J. Epidemiol. 2010, 171, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Liaw, Y.; Huang, Y.; Lien, G. Patterns of lung cancer mortality in 23 countries: Application of the age-period-cohort model. BMC Public Health 2005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jemal, A.; Chu, K.C.; Tarone, R.E. Recent trends in lung cancer mortality in the United States. J. Natl. Cancer Inst. 2001, 93, 277–283. [Google Scholar] [CrossRef] [PubMed]
| df | AP | AC | PC | APC-C | APC-IE |
|---|---|---|---|---|---|
| 60 | 48 | 55 | 44 | 44 | |
| Urban Male | |||||
| Deviation | 160.89 | 80.60 | 478.47 | 27.40 | 27.40 |
| AIC | 614.30 | 558.01 | 941.88 | 512.80 | 6.57 |
| BIC | 656.72 | 628.71 | 996.08 | 592.93 | −164.30 |
| Urban Female | |||||
| Deviation | 108.51 | 49.36 | 157.33 | 24.35 | 24.35 |
| AIC | 510.80 | 475.65 | 569.62 | 458.64 | 5.88 |
| BIC | 553.22 | 546.35 | 623.82 | 538.77 | −167.34 |
| Rural Male | |||||
| Deviation | 240.49 | 108.15 | 226.33 | 39.96 | 39.96 |
| AIC | 679.67 | 571.33 | 675.50 | 511.14 | 6.55 |
| BIC | 722.09 | 642.03 | 729.71 | 591.27 | −151.74 |
| Rural Female | |||||
| Deviation | 58.07 | 14.91 | 31.61 | 9.11 | 9.11 |
| AIC | 435.50 | 416.34 | 419.04 | 418.53 | 5.37 |
| BIC | 477.92 | 487.04 | 473.24 | 498.66 | −182.59 |
| Factor | Urban Male RR (95% CI) | Urban Female RR (95% CI) | Rural Male RR (95% CI) | Rural Female RR (95% CI) |
|---|---|---|---|---|
| Age | ||||
| 20–24 | 0.04 (0.02–0.11) | 0.03 (0.01–0.13) | 0.06 (0.02–0.17) | 0.06 (0.03–0.12) |
| 25–29 | 0.07 (0.04–0.13) | 0.08 (0.04–0.18) | 0.08 (0.04–0.18) | 0.12 (0.08–0.19) |
| 30–34 | 0.14 (0.09–0.22) | 0.20 (0.12–0.34) | 0.20 (0.12–0.32) | 0.27 (0.20–0.36) |
| 35–39 | 0.27 (0.19–0.37) | 0.35 (0.24–0.53) | 0.29 (0.20–0.44) | 0.37 (0.29–0.47) |
| 40–44 | 0.52 (0.41–0.67) | 0.65 (0.47–0.90) | 0.58 (0.43–0.78) | 0.65 (0.54–0.80) |
| 45–49 | 0.90 (0.74–1.09) | 0.96 (0.74–1.24) | 0.94 (0.74–1.20) | 0.95 (0.81–1.12) |
| 50–54 | 1.50 (1.29–1.76) | 1.54 (1.25–1.89) | 1.51 (1.25–1.83) | 1.35 (1.19–1.54) |
| 55–59 | 2.29 (2.02–2.59) | 2.04 (1.73–2.41) | 2.13 (1.83–2.48) | 1.78 (1.60–1.98) |
| 60–64 | 3.54 (3.20–3.92) | 3.11 (2.72–3.56) | 3.01 (2.67–3.39) | 2.44 (2.24–2.66) |
| 65–69 | 5.15 (4.68–5.67) | 4.28 (3.78–4.84) | 3.93 (3.55–4.36) | 3.17 (2.93–3.43) |
| 70–74 | 6.45 (5.78–7.19) | 5.32 (4.64–6.09) | 4.98 (4.47–5.56) | 4.28 (3.94–4.65) |
| 75–79 | 6.92 (6.04–7.92) | 6.01 (5.10–7.09) | 5.53 (4.83–6.32) | 4.99 (4.52–5.51) |
| 80–84 | 6.76 (5.71–8.00) | 5.95 (4.85–7.30) | 5.62 (4.75–6.65) | 5.87 (5.20–6.63) |
| Period | ||||
| 1988 | 0.69 (0.62–0.77) | 0.78 (0.68–0.89) | 0.58 (0.51–0.67) | 0.64 (0.58–0.70) |
| 1993 | 0.87 (0.81–0.93) | 0.86 (0.78–0.94) | 0.64 (0.59–0.70) | 0.68 (0.64–0.73) |
| 1998 | 1.02 (0.98–1.05) | 1.05 (1.00–1.10) | 0.85 (0.81–0.90) | 0.86 (0.83–0.90) |
| 2003 | 0.95 (0.91–0.99) | 0.92 (0.87–0.98) | 1.14 (1.09–1.20) | 1.17 (1.12–1.21) |
| 2008 | 1.20 (1.12–1.29) | 1.16 (1.06–1.27) | 1.65 (1.53–1.79) | 1.39 (1.32–1.47) |
| 2013 | 1.44 (1.29–1.60) | 1.33 (1.16–1.52) | 1.65 (1.46–1.86) | 1.64 (1.51–1.77) |
| Cohort | ||||
| 1904–1908 | 3.00 (2.33–3.85) | 2.65 (1.94–3.62) | 2.16 (1.61–2.90) | 1.79 (1.47–2.18) |
| 1909–1913 | 3.02 (2.43–3.75) | 2.62 (2.01–3.43) | 2.06 (1.61–2.64) | 1.72 (1.46–2.03) |
| 1914–1918 | 2.99 (2.46–3.62) | 2.56 (2.02–3.24) | 2.16 (1.74–2.68) | 1.94 (1.69–2.24) |
| 1919–1923 | 2.74 (2.30–3.27) | 2.64 (2.13–3.28) | 2.45 (2.03–2.97) | 2.09 (1.85–2.37) |
| 1924–1928 | 2.62 (2.21–3.11) | 2.53 (2.06–3.11) | 2.75 (2.30–3.30) | 2.26 (2.02–2.54) |
| 1929–1933 | 2.22 (1.87–2.64) | 2.26 (1.84–2.79) | 2.38 (1.98–2.85) | 2.11 (1.88–2.37) |
| 1934–1938 | 1.66 (1.38–2.00) | 1.90 (1.51–2.38) | 1.97 (1.62–2.41) | 1.95 (1.72–2.22) |
| 1939–1943 | 1.30 (1.05–1.60) | 1.40 (1.09–1.81) | 1.57 (1.25–1.96) | 1.74 (1.51–2.02) |
| 1944–1948 | 1.16 (0.91–1.47) | 1.09 (0.81–1.46) | 1.46 (1.13–1.88) | 1.60 (1.35–1.90) |
| 1949–1953 | 1.15 (0.88–1.51) | 1.03 (0.74–1.44) | 1.27 (0.95–1.70) | 1.46 (1.20–1.77) |
| 1954–1958 | 1.03 (0.76–1.40) | 0.90 (0.62–1.33) | 1.01 (0.72–1.42) | 1.15 (0.92–1.44) |
| 1959–1963 | 0.81 (0.57–1.14) | 0.66 (0.43–1.02) | 0.73 (0.50–1.08) | 0.84 (0.65–1.08) |
| 1964–1968 | 0.57 (0.38–0.86) | 0.55 (0.33–0.91) | 0.67 (0.43–1.03) | 0.73 (0.55–0.97) |
| 1969–1973 | 0.53 (0.33–0.85) | 0.51 (0.28–0.91) | 0.49 (0.29–0.83) | 0.51 (0.36–0.72) |
| 1974–1978 | 0.36 (0.19–0.68) | 0.34 (0.15–0.74) | 0.38 (0.19–0.75) | 0.40 (0.26–0.63) |
| 1979–1983 | 0.27 (0.11–0.68) | 0.34 (0.12–0.95) | 0.27 (0.10–0.70) | 0.30 (0.16–0.54) |
| 1984–1988 | 0.23 (0.06–0.90) | 0.27 (0.05–1.48) | 0.33 (0.10–1.15) | 0.25 (0.09–0.64) |
| 1989–1993 | 0.14 (0.01–3.06) | 0.24 (0.01–9.94) | 0.14 (0.01–3.17) | 0.20 (0.03–1.51) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, L.; Yu, C.; Liu, Y.; Wang, J.; Li, C.; Wang, Q.; Wang, P.; Wu, S.; Zhang, Z.-J. Lung Cancer Mortality Trends in China from 1988 to 2013: New Challenges and Opportunities for the Government. Int. J. Environ. Res. Public Health 2016, 13, 1052. https://doi.org/10.3390/ijerph13111052
Wang L, Yu C, Liu Y, Wang J, Li C, Wang Q, Wang P, Wu S, Zhang Z-J. Lung Cancer Mortality Trends in China from 1988 to 2013: New Challenges and Opportunities for the Government. International Journal of Environmental Research and Public Health. 2016; 13(11):1052. https://doi.org/10.3390/ijerph13111052
Chicago/Turabian StyleWang, Lijun, Chuanhua Yu, Yu Liu, Jun Wang, Chunhui Li, Quan Wang, Peigang Wang, Shaotang Wu, and Zhi-Jiang Zhang. 2016. "Lung Cancer Mortality Trends in China from 1988 to 2013: New Challenges and Opportunities for the Government" International Journal of Environmental Research and Public Health 13, no. 11: 1052. https://doi.org/10.3390/ijerph13111052