
Secular Trends in Growth and Nutritional Outcomes of Children under Five Years Old in Xiamen, China


Abstract
:1. Introduction
2. Subjects and Methods
2.1. Subjects and Sampling
2.2. Anthropometry
2.3. Diagnostic Criteria
2.4. Statistical Analyses
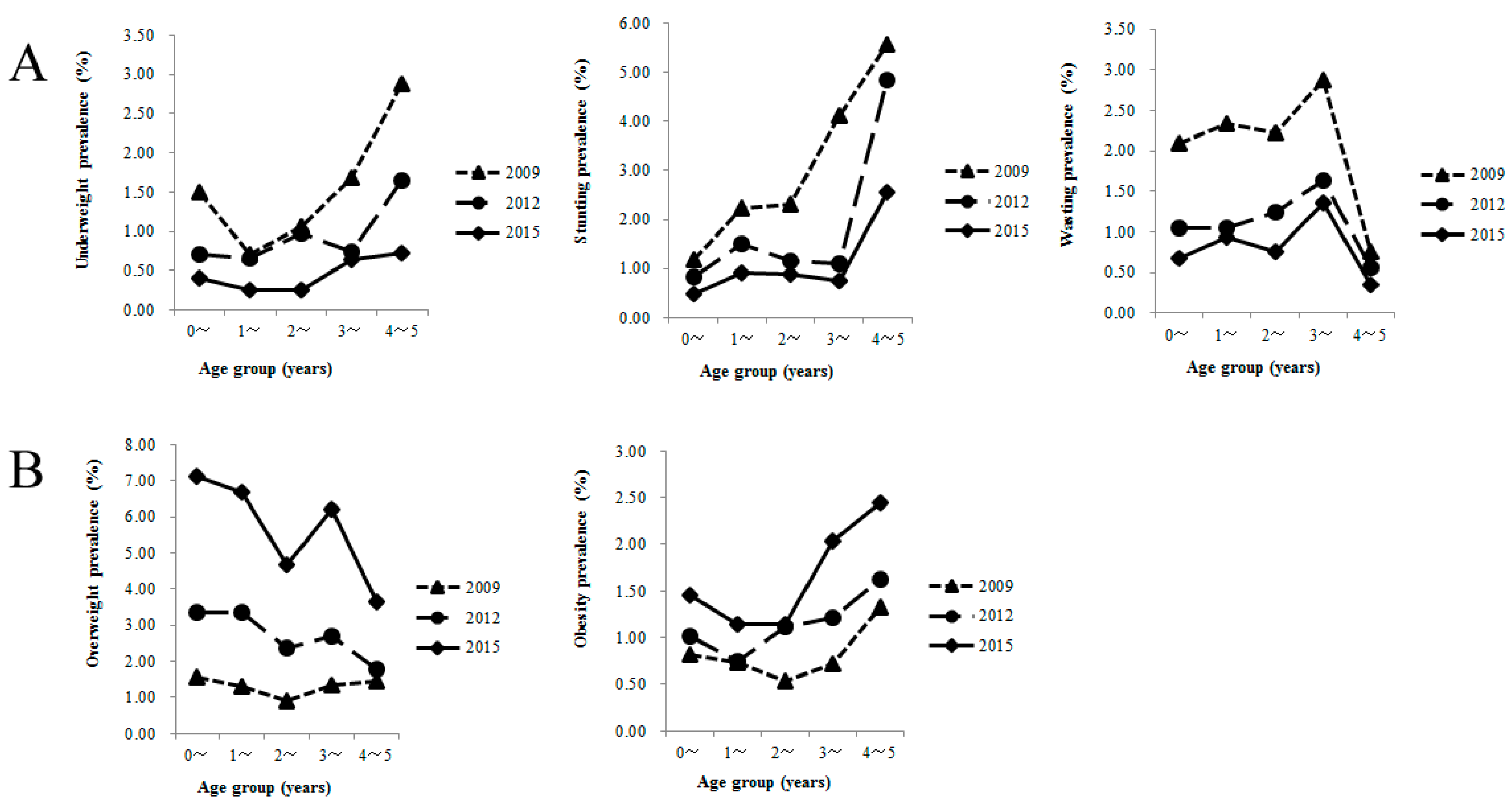
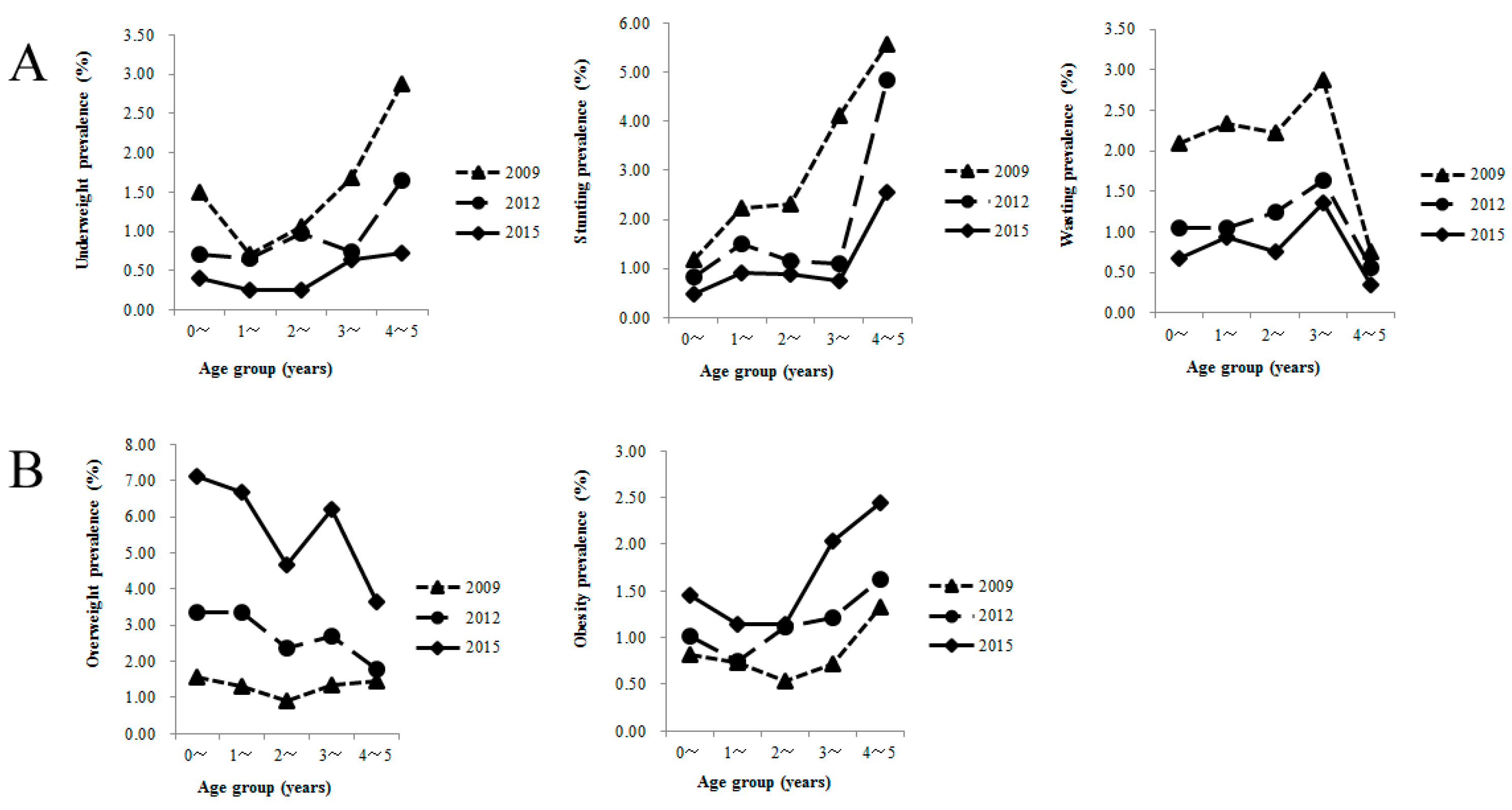
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- De onis, M.; Blossner, M.; Borghi, E.; Morris, R.; Frongillo, E.A. Methodology for estimating regional and global trends of child malnutrition. Int. J. Epidemiol. 2004, 33, 1260–1270. [Google Scholar] [CrossRef] [PubMed]
- Betran, A.P.; Ye, J.; Moller, A.B.; Zhang, J.; Gulmezoglu, A.M.; Torloni, M.R. The Increasing trend in caesarean section rates: Global, regional and national estimates: 1990–2014. PLoS ONE 2016, 11, e0148343. [Google Scholar] [CrossRef] [PubMed]
- Archenti, A.; Pasqualinotto, L. Childhood obesity: The epidemic of the third millenium. Acta. Biomed. 2008, 79, 151–155. [Google Scholar] [PubMed]
- Wang, Y.; Lobstein, T. Worldwide trends in childhood overweight and obesity. Int. J. Pediatr. Obes. 2006, 1, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Zhai, F.Y.; He, Y.N.; Ma, G.S.; Li, Y.P.; Wang, Z.H.; Hu, Y.S.; Zhao, L.Y.; Cui, Z.H.; Li, Y.; Yang, X.G. Study on the current status and trend of food consumption among Chinese population. Zhonghua Liu Xing Bing Xue Za Zhi 2005, 26, 485–488. (In Chinese) [Google Scholar] [PubMed]
- Lohman, T.; Roche, A.; Martorell, E. (Eds.) Anthropometric Standardization Reference Manual; Human Kinetics: Champaign, IL, USA, 2011.
- WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age: Methods and Development; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- WHO. World Health Organization Training Course on Child Growth Assessment; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Das, M.K.; Bhattacharyya, N.; Bhattacharyya, A.K. WHO child growth standards. Eur. J. Pediatr. 2010, 169, 253–255. [Google Scholar] [CrossRef] [PubMed]
- Ji, C.Y.; Hu, P.J.; He, Z.H. Secular growth trends in the Chinese urban youth and its implications on public health. Beijing Da Xue Xue Bao 2007, 39, 126–131. (In Chinese) [Google Scholar] [PubMed]
- Must, A.; Jacques, P.F.; Dallal, G.E.; Bajema, C.J.; Dietz, W.H. Long-term morbidity and mortality of overweight adolescents. A follow-up of the Harvard Growth Study of 1922 to 1935. N. Engl. J. Med. 1992, 327, 1350–1355. [Google Scholar] [CrossRef] [PubMed]
- Di Pietro, L.; Mossberg, H.O.; Stunkard, A.J. A 40-year history of overweight children in Stockholm: Life-time overweight, morbidity, and mortality. Int. J. Obes. Relat. Metab. Disord. 1994, 18, 585–590. [Google Scholar]
- Popkin, B.M. Will China’s nutrition transition overwhelm its health care system and slow economic growth? Health Aff. (Millwood) 2008, 27, 1064–1076. [Google Scholar] [CrossRef] [PubMed]
- Zhai, F.; Fu, D.; Du, S.; Ge, K.; Chen, C.; Popkin, B.M. What is China doing in policy-making to push back the negative aspects of the nutrition transition? Public. Health Nutr. 2002, 5, 269–273. [Google Scholar] [CrossRef] [PubMed]
- The Chinese Ministry of Health. Chinese Children Aged 0–6 Years Nutrition Development Report; The Chinese Ministry of Health: Beijing, China, 2012.
- The Central People’s Government of the People’s Republic of China. National Program of Action for Child Development in China (2011–2020); The Central People’s Government of the People’s Republic of China: Beijing, China, 2011.
- Yu, D.M.; Zhao, L.Y.; Yang, Z.Y.; Chang, S.Y.; Yu, W.T.; Fang, H.Y.; Wang, X.; Yu, D.; Guo, Q.Y.; Xu, X.L.; et al. Comparison of undernutrition prevalence of children under 5 Years in China between 2002 and 2013. Biomed. Environ. Sci. 2016, 29, 165–176. [Google Scholar] [PubMed]
- Nazri, C.; Yamazaki, C.; Kameo, S.; Herawati, D.M.; Sekarwana, N.; Raksanagara, A.; Koyama, H. Factors influencing mother’s participation in Posyandu for improving nutritional status of children under-five in Aceh Utara district, Aceh province, Indonesia. BMC Public Health 2016, 16, 69. [Google Scholar] [CrossRef] [PubMed]
- Kien, V.D.; Lee, H.Y.; Nam, Y.S.; Oh, J.; Giang, K.B.; Van Minh, H. Trends in socioeconomic inequalities in child malnutrition in Vietnam: Findings from the Multiple Indicator Cluster Surveys, 2000–2011. Glob. Health Action 2016, 9, 29263. [Google Scholar] [CrossRef] [PubMed]
- Lissner, L.; Sohlstrom, A.; Sundblom, E.; Sjoberg, A. Trends in overweight and obesity in Swedish schoolchildren 1999–2005: Has the epidemic reached a plateau? Obes. Rev. 2010, 11, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Olds, T.S.; Tomkinson, G.R.; Ferrar, K.E.; Maher, C.A. Trends in the prevalence of childhood overweight and obesity in Australia between 1985 and 2008. Int. J. Obes. (Lond.) 2010, 34, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Romon, M.; Lommez, A.; Tafflet, M.; Basdevant, A.; Oppert, J.M.; Bresson, J.L.; Ducimetiere, P.; Charles, M.A.; Borys, J.M. Downward trends in the prevalence of childhood overweight in the setting of 12-year school- and community-based programmes. Public Health Nutr. 2009, 12, 1735–1742. [Google Scholar] [CrossRef] [PubMed]
- Tambalis, K.D.; Panagiotakos, D.B.; Kavouras, S.A.; Kallistratos, A.A.; Moraiti, I.P.; Douvis, S.J.; Toutouzas, P.K.; Sidossis, L.S. Eleven-year prevalence trends of obesity in Greek children: First evidence that prevalence of obesity is leveling off. Obesity (Silver Spring) 2010, 18, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Carriere, C.; Langevin, C.; Deti, E.K.; Barberger-Gateau, P.; Maurice, S.; Thibault, H. Stabilization of overweight prevalence and improvement of dietary habits in French children between 2004 and 2008. Public Health Nutr. 2015, 18, 1883–1889. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Curtin, L.R.; McDowell, M.A.; Tabak, C.J.; Flegal, K.M. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA 2006, 295, 1549–1555. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Alvarez, A.; Serra-Majem, L.; Ribas-Barba, L.; Castell, C.; Foz, M.; Uauy, R.; Plasencia, A.; Salleras, L. Obesity and overweight trends in Catalonia, Spain (1992–2003): Gender and socio-economic determinants. Public Health Nutr. 2007, 10, 1368–1378. [Google Scholar] [CrossRef] [PubMed]
- Kowal, M.; Woronkowicz, A.; Kryst, Ł.; Sobiecki, J.; Pilecki, M.W. Sex differences in prevalence of overweight and obesity, and in extent of overweight index, in children and adolescents (3–18 years) from Krakow, Poland in 1983, 2000 and 2010. Public Health Nutr. 2016, 19, 1035–1046. [Google Scholar] [CrossRef] [PubMed]
- Lazzeri, G.; Panatto, D.; Pammolli, A.; Azzolini, E.; Simi, R.; Meoni, V.; Giacchi, M.V.; Amicizia, D.; Gasparini, R. Trends in overweight and obesity prevalence in Tuscan schoolchildren (2002–2012). Public Health Nutr. 2015, 18, 3078–3085. [Google Scholar] [CrossRef] [PubMed]
- Khader, Y.; Irshaidat, O.; Khasawneh, M.; Amarin, Z.; Alomari, M.; Batieha, A. Overweight and obesity among school children in Jordan: Prevalence and associated factors. Matern. Child Health J. 2009, 13, 424–431. [Google Scholar] [CrossRef] [PubMed]
- Antal, M.; Peter, S.; Biro, L.; Nagy, K.; Regoly-Merei, A.; Arato, G.; Szabo, C.; Martos, E. Prevalence of underweight, overweight and obesity on the basis of body mass index and body fat percentage in Hungarian schoolchildren: Representative survey in metropolitan elementary schools. Ann. Nutr. Metab. 2009, 54, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Dibley, M.J.; Sibbritt, D.; Yan, H. An assessment of adolescent overweight and obesity in Xi’an City, China. Int. J. Pediatr. Obes. 2006, 1, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Zeng, X.; Zhuang, Q.; Zheng, Y.; Chen, S. Intervention of childhood and adolescents obesity in Shantou city. Obes. Res. Clin. Pract. 2015, 9, 357–364. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Age | 2009 | 2012 | 2015 | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| B | G | Total | B | G | Total | B | G | Total | ||
| 0~ | 2514 | 2105 | 4619 | 2672 | 2293 | 4965 | 2549 | 2076 | 4625 | 14,209 |
| 1~ | 2456 | 1936 | 4392 | 2751 | 2247 | 4998 | 2550 | 2224 | 4774 | 14,164 |
| 2~ | 2598 | 2035 | 4633 | 2643 | 2310 | 4953 | 2600 | 2150 | 4750 | 14,336 |
| 3~ | 2482 | 1974 | 4456 | 2720 | 2260 | 4980 | 2834 | 2054 | 4888 | 14,324 |
| 4–5 | 2524 | 1952 | 4476 | 2800 | 2120 | 4920 | 2720 | 2080 | 4800 | 14,196 |
| Total | 12,574 | 10,002 | 22,576 | 13,586 | 11,230 | 24,816 | 13,253 | 10,584 | 23,837 | 71,229 |
| Variable | 2009 | 2012 | 2015 | F | p-Value |
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | |||
| Boys | |||||
| Height | 69.2 ± 11.3 | 73.7 ± 13.4 | 77.2 ± 13.5 | 1772.19 | <0.001 1,2,3 |
| Weight | 8.3 ± 2.8 | 9.3 ± 3.3 | 9.9 ± 3.3 | 1323.78 | <0.001 1,2,3 |
| BMI | 16.3 ± 1.6 | 16.6 ± 1.7 | 16.8 ± 1.6 | 399.30 | <0.001 1,2,3 |
| Girls | |||||
| Height | 67.9 ± 11.3 | 72.1 ± 13.5 | 74.7 ± 13.6 | 1717.36 | <0.001 1,2,3 |
| Weight | 7.7 ± 2.7 | 8.6 ± 3.2 | 9.1 ± 3.2 | 1298.63 | <0.001 1,2,3 |
| BMI | 15.9 ± 1.5 | 16.1 ± 1.6 | 16.2 ± 1.6 | 515.96 | <0.001 1,2,3 |
| Variable | Height (Mean ± SD) | Weight (Mean ± SD) | BMI (Mean ± SD) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2009 | 2012 | 2015 | Pairwise Comparisons | 2009 | 2012 | 2015 | Pairwise Comparisons | 2009 | 2012 | 2015 | Pairwise Comparisons | |
| Boys | (only when F has a p < 0.05) | |||||||||||
| 0~ | 56.3 ± 2.3 | 56.4 ± 2.2 | 56.5 ± 2.2 | 09 = 12 09 < 15 12 = 15 | 4.9 ± 0.6 | 4.9 ± 0.7 | 5.0 ± 0.6 | 09 = 12 09 < 15 12 < 15 | 15.5 ± 1.3 | 15.5 ± 1.3 | 15.6 ± 1.3 | 09 = 12 09 < 15 12 < 15 |
| 2~ | 63.1 ± 3.6 | 63.1 ± 3.6 | 63.5 ± 3.5 | 09 = 12 09 < 15 12 < 15 | 6.9 ± 1.1 | 6.9 ± 1.1 | 7.1 ± 1.1 | 09 = 12 09 < 15 12 < 15 | 17.1 ± 1.7 | 17.2 ± 1.6 | 17.4 ± 1.6 | 09 < 12 09 < 15 12 < 15 |
| 6~ | 71.0 ± 3.5 | 71.1 ± 3.5 | 71.4 ± 3.5 | 09 = 12 09 < 15 12 < 15 | 8.7 ± 1.2 | 8.8 ± 1.2 | 9.0 ± 1.1 | 09 < 12 09 < 15 12 < 15 | 17.2 ± 1.5 | 17.4 ± 1.6 | 17.6 ± 1.5 | 09 < 12 09 < 15 12 < 15 |
| 12~ | 80.4 ± 4.7 | 83.0 ± 6.2 | 84.7 ± 6.8 | 09 < 12 09 < 15 12 < 15 | 10.9 ± 1.5 | 11.4 ± 1.8 | 11.5 ± 1.9 | 09 < 12 09 < 15 12 < 15 | 16.0 ± 1.3 | 16.5 ± 1.3 | 16.8 ± 1.4 | 09 < 12 09 < 15 12 < 15 |
| 24~ | 90.8 ± 3.9 | 90.9 ± 4.1 | 91.4 ± 4.3 | 09 = 12 09 < 15 12 < 15 | 12.9 ± 1.7 | 13.1 ± 1.7 | 13.2 ± 1.7 | 09 = 12 09 < 15 12 < 15 | 15.6 ± 1.2 | 15.7 ± 1.3 | 16.0 ± 1.3 | 09 < 12 09 < 15 12 < 15 |
| 36~ | 97.9 ± 4.2 | 98.1 ± 3.4 | 98.3 ± 4.3 | — | 14.8 ± 2.0 | 14.9 ± 1.6 | 15.0 ± 2.1 | — | 15.4 ± 1.3 | 15.4 ± 1.3 | 15.4 ± 1.4 | — |
| 48~60 | 103.7 ± 4.3 | 105.1 ± 4.5 | 105.1 ± 4.4 | — | 16.4 ± 2.8 | 16.7 ± 2.2 | 16.8 ± 2.4 | — | 15.1 ± 1.3 | 15.1 ± 1.4 | 15.2 ± 1.1 | — |
| Girls | ||||||||||||
| 0~ | 55.1 ± 2.2 | 55.9 ± 2.4 | 56.2 ± 2.1 | 09 < 12 09 < 15 12 < 15 | 4.6 ± 0.6 | 4.8 ± 0.7 | 4.9 ± 0.6 | 09 < 12 09 < 15 12 < 15 | 14.9 ± 1.2 | 15.3 ± 1.4 | 15.5 ± 1.3 | 09 < 12 09 < 15 12 < 15 |
| 2~ | 59.4 ± 3.5 | 61.4 ± 3.4 | 61.6 ± 3.4 | 09 < 12 09 < 15 12 < 15 | 5.8 ± 1.0 | 6.2 ± 1.0 | 6.3 ± 1.0 | 09 < 12 09 < 15 12 < 15 | 16.2 ± 1.6 | 16.4 ± 1.6 | 16.6 ± 1.6 | 09 < 12 09 < 15 12 < 15 |
| 6~ | 69.2 ± 3.4 | 70.6 ± 3.9 | 70.7 ± 3.2 | 09 < 12 09 < 15 12 < 15 | 8.0 ± 1.1 | 8.4 ± 1.3 | 8.9 ± 1.1 | 09 < 12 09 < 15 12 < 15 | 16.7 ± 1.5 | 16.9 ± 1.5 | 17.7 ± 1.6 | 09 < 12 09 < 15 12 < 15 |
| 12~ | 78.7 ± 4.5 | 81.8 ± 6.2 | 82.9 ± 6.9 | 09 < 12 09 < 15 12 < 15 | 10.1 ± 1.3 | 10.7 ± 1.7 | 10.9 ± 1.9 | 09 < 12 09 < 15 12 < 15 | 15.7 ± 1.3 | 16.0 ± 1.3 | 16.3 ± 1.3 | 09 < 12 09 < 15 12 < 15 |
| 24~ | 89.4 ± 3.7 | 89.6 ± 4.1 | 90.2 ± 4.4 | 09 = 12 09 < 15 12 < 15 | 12.4 ± 1.6 | 12.5 ± 1.5 | 12.6 ± 1.7 | 09 = 12 09 < 15 12 = 15 | 15.3 ± 1.2 | 15.4 ± 1.2 | 15.6 ± 1.3 | 09 = 12 09 < 15 12 < 15 |
| 36~ | 96.1 ± 4.3 | 96.8 ± 4.2 | 96.8 ± 4.4 | — | 14.2 ± 1.9 | 14.3 ± 1.9 | 14.3 ± 1.9 | — | 15.1 ± 1.2 | 15.2 ± 1.3 | 15.4 ± 1.1 | — |
| 48~60 | 104.1 ± 5.1 | 104.3 ± 4.8 | 104.5 ± 4.3 | — | 15.3 ± 2.6 | 16.3 ± 2.7 | 16.5 ± 2.3 | — | 14.1 ± 1.4 | 14.9 ± 1.6 | 15.0 ± 1.4 | — |
| Variable | 2009 | 2012 | 2015 | |||||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | Trend | p-Value | |
| Boys | ||||||||
| Underweight | 157 | 1.25 | 109 | 0.80 | 48 | 0.36 | Decreasing | <0.001 |
| Stunted | 357 | 2.84 | 197 | 1.45 | 107 | 0.81 | Decreasing | <0.001 |
| Wasted | 204 | 1.62 | 171 | 1.26 | 127 | 0.96 | Decreasing | <0.001 |
| Overweight | 185 | 1.47 | 440 | 3.24 | 857 | 6.47 | Increasing | <0.001 |
| Obese | 113 | 0.90 | 136 | 1.00 | 197 | 1.49 | Increasing | <0.001 |
| Girls | ||||||||
| Underweight | 120 | 1.20 | 107 | 0.95 | 46 | 0.43 | Decreasing | <0.001 |
| Stunted | 267 | 2.67 | 130 | 1.16 | 72 | 0.68 | Decreasing | <0.001 |
| Wasted | 144 | 1.44 | 107 | 0.95 | 59 | 0.56 | Decreasing | <0.001 |
| Overweight | 99 | 0.99 | 314 | 2.80 | 646 | 6.10 | Increasing | <0.001 |
| Obese | 83 | 0.83 | 92 | 0.82 | 135 | 1.28 | Increasing | <0.001 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.; Chen, W.; Zeng, G.; Li, G. Secular Trends in Growth and Nutritional Outcomes of Children under Five Years Old in Xiamen, China. Int. J. Environ. Res. Public Health 2016, 13, 1104. https://doi.org/10.3390/ijerph13111104
Chen J, Chen W, Zeng G, Li G. Secular Trends in Growth and Nutritional Outcomes of Children under Five Years Old in Xiamen, China. International Journal of Environmental Research and Public Health. 2016; 13(11):1104. https://doi.org/10.3390/ijerph13111104
Chicago/Turabian StyleChen, Jing, Wei Chen, Guozhang Zeng, and Guimei Li. 2016. "Secular Trends in Growth and Nutritional Outcomes of Children under Five Years Old in Xiamen, China" International Journal of Environmental Research and Public Health 13, no. 11: 1104. https://doi.org/10.3390/ijerph13111104