
A Robot-Based Tool for Physical and Cognitive Rehabilitation of Elderly People Using Biofeedback



Abstract
:1. Introduction and Background
- General objective: Design and implementation of a Lego-based robot for both cognitive and physical maintenance and rehabilitation of elderly people, taking into account biological parameters regarding arm movements and heart rate values.
- Specific technological objectives:
- (1)
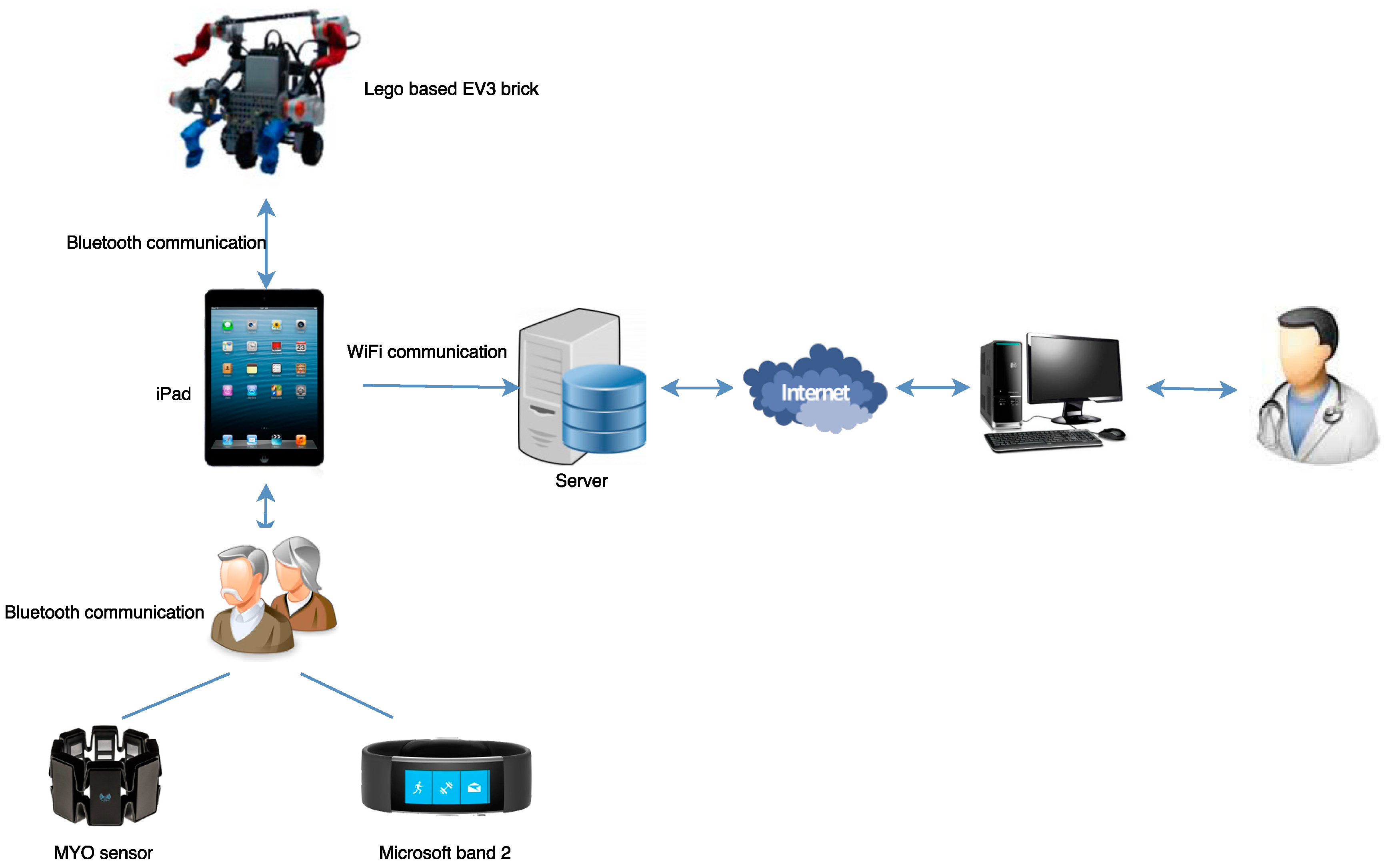
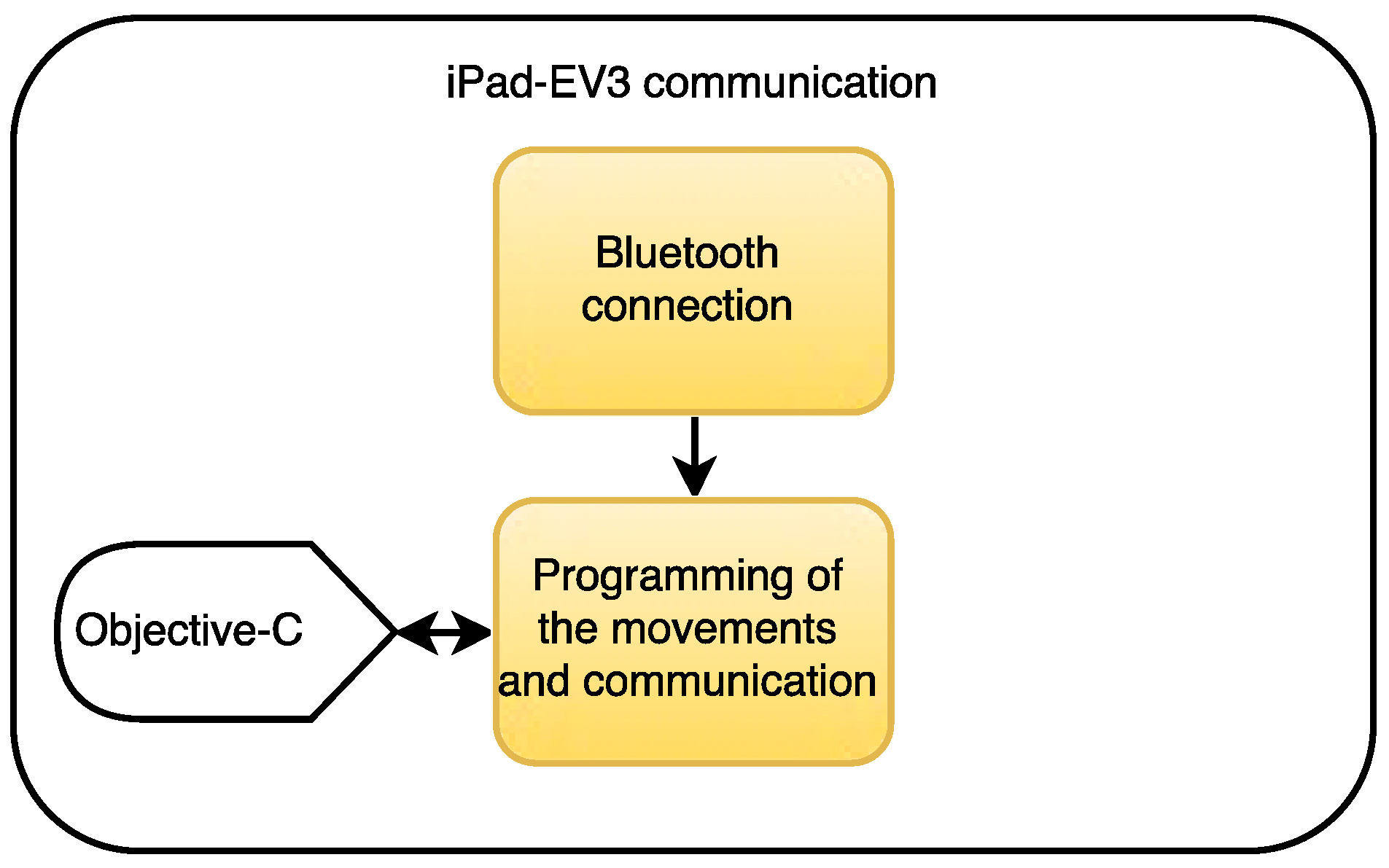
- Design and implementation of the communication between the Lego-based robot EV3 and an iPad mini.
- (2)
- Design and implementation of the serious game.
- (3)
- Data acquisition from biological sensors.
- (4)
- Validation of the system with real patients.
2. Methods
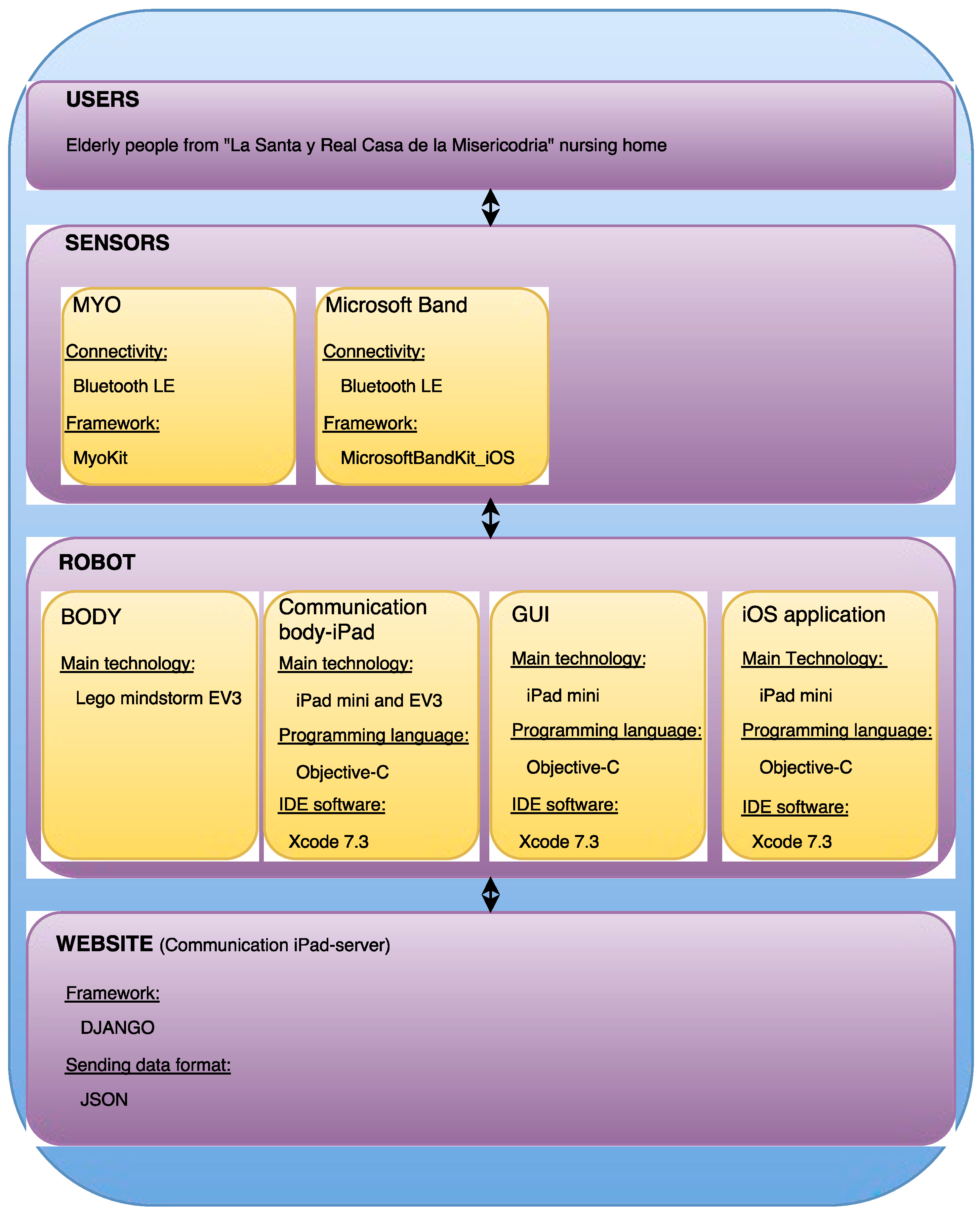
2.1. Design of the Platform
- (1)
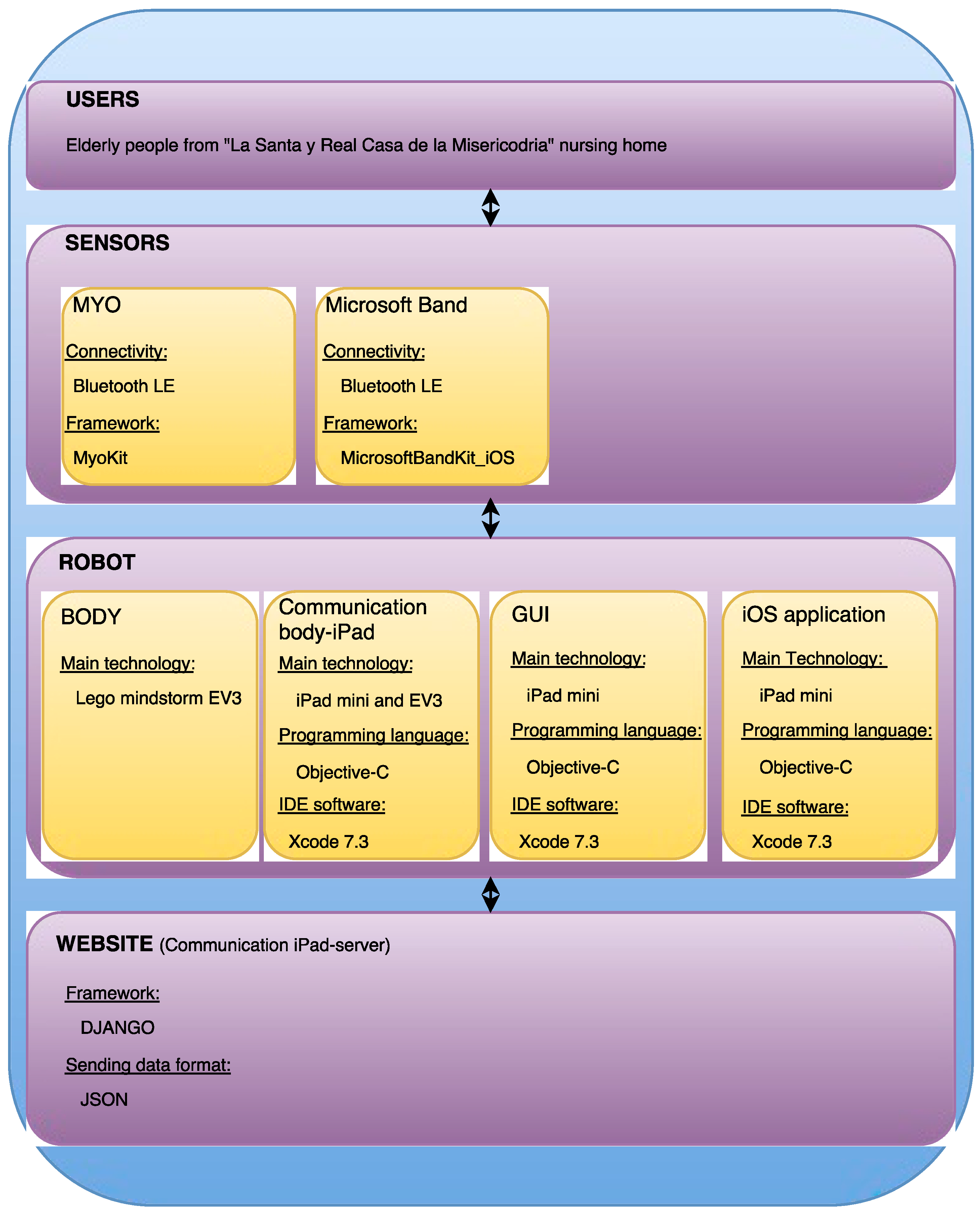
- The design of the Graphical User Interface (GUI) of the iOS application, as well as the serious game that the users from La Santa y Real Casa de la Misericordia have to play.
- (2)
- The design of the biofeedback, consisting in the following two sub-stages:
- (2.1)
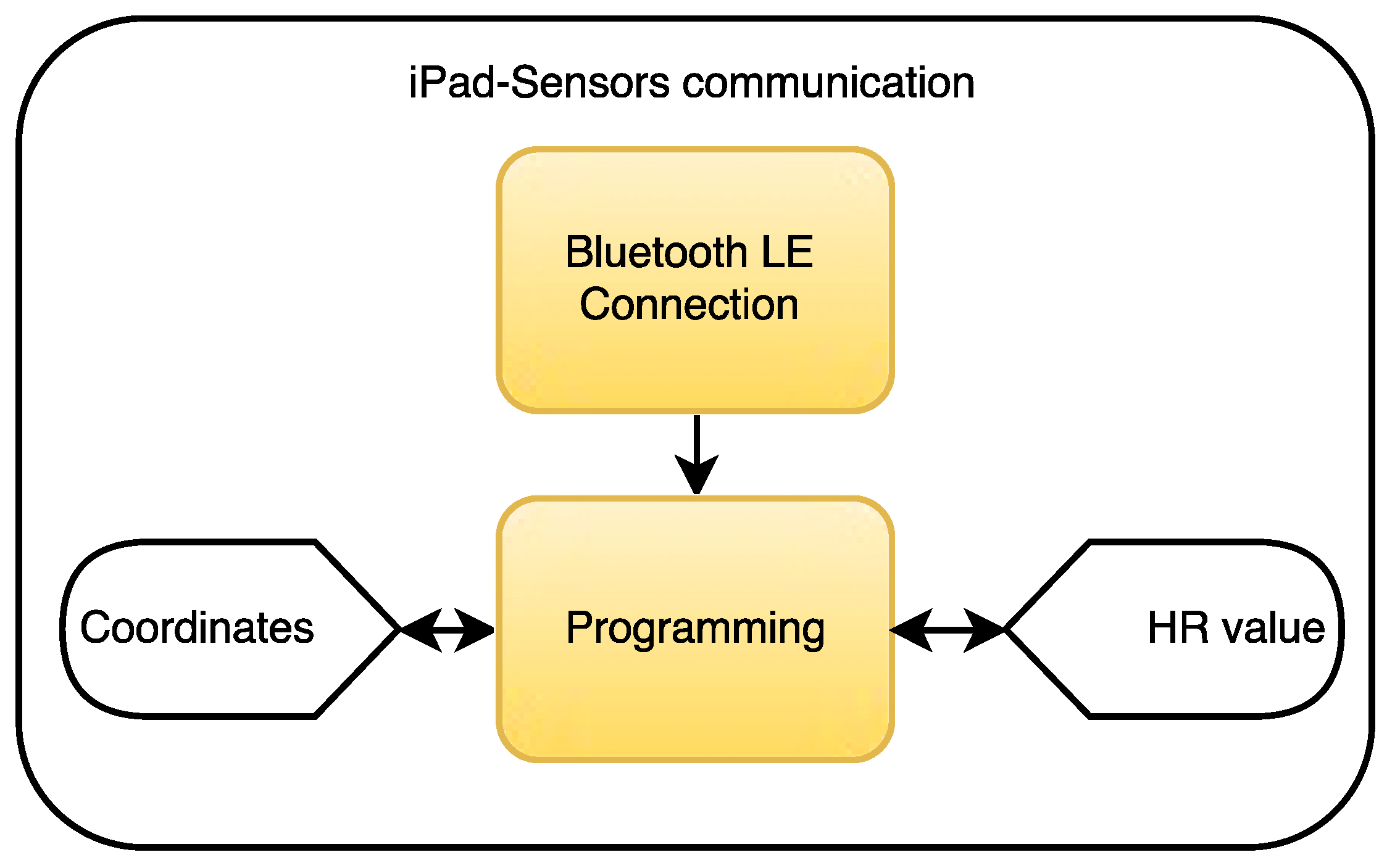
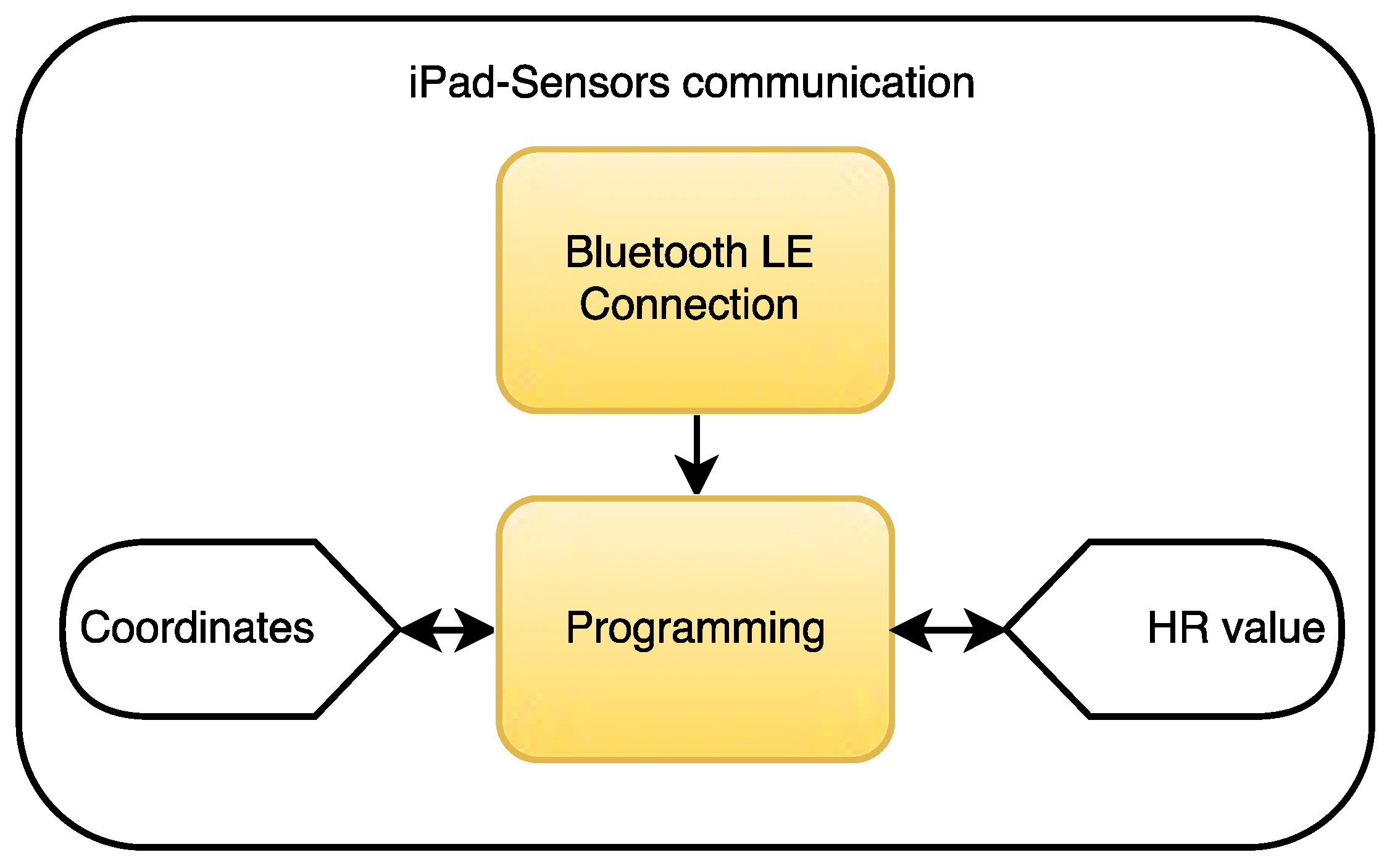
- The design of the wireless communication between the iPad mini and the biological sensors.
- (2.2)
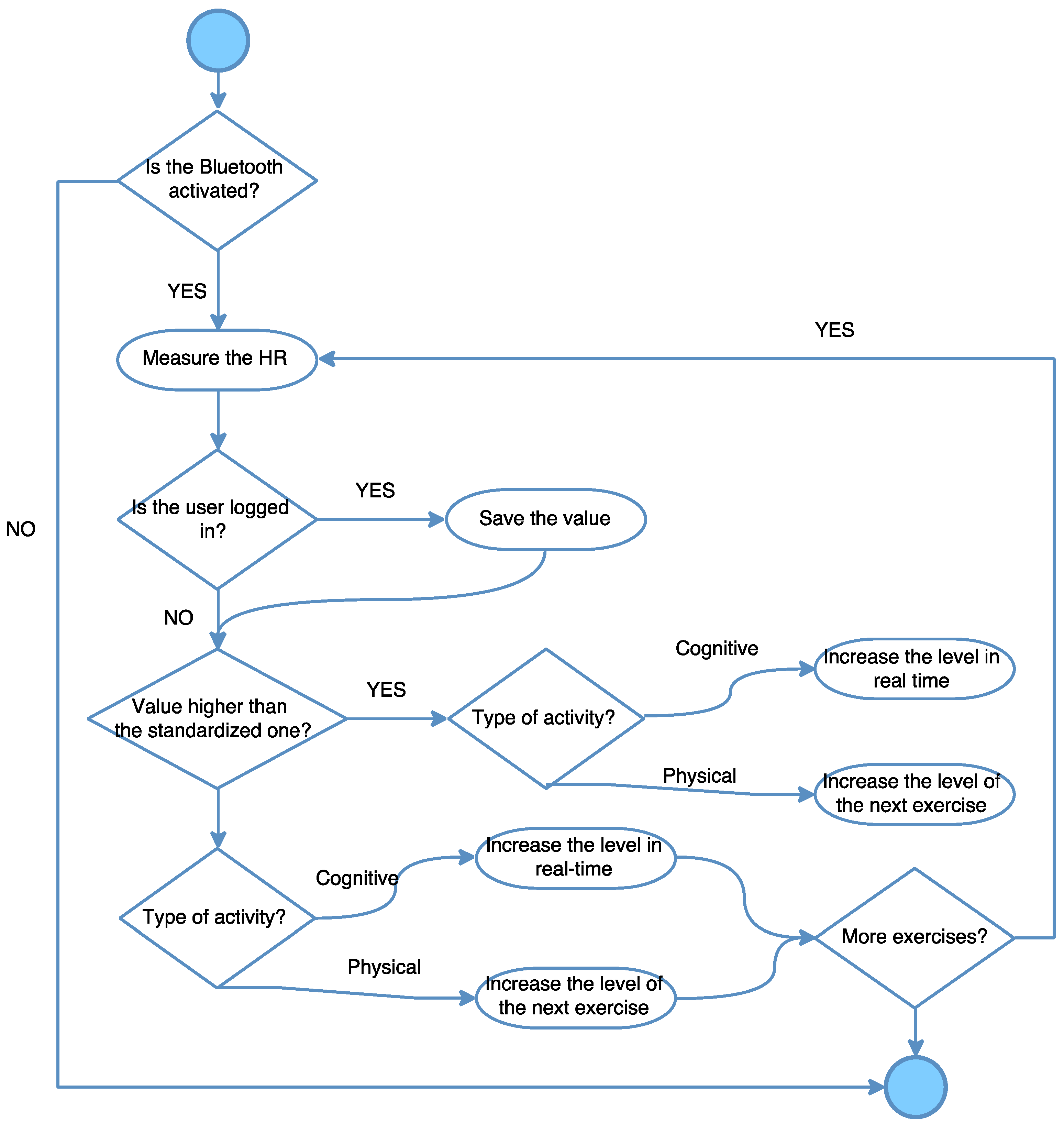
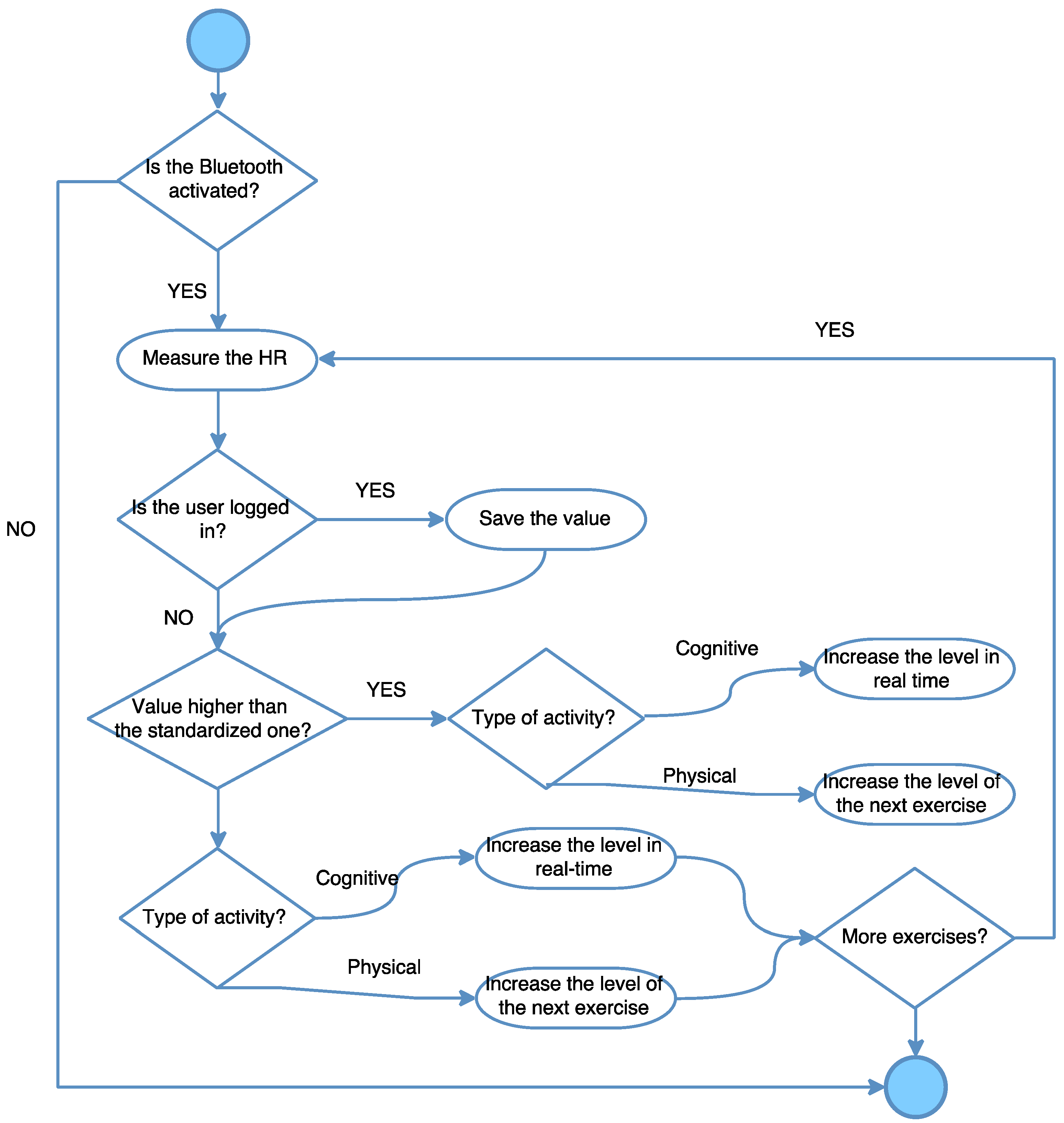
- The design of the biofeedback system itself to track how activities change depending on the values received.
- (3)
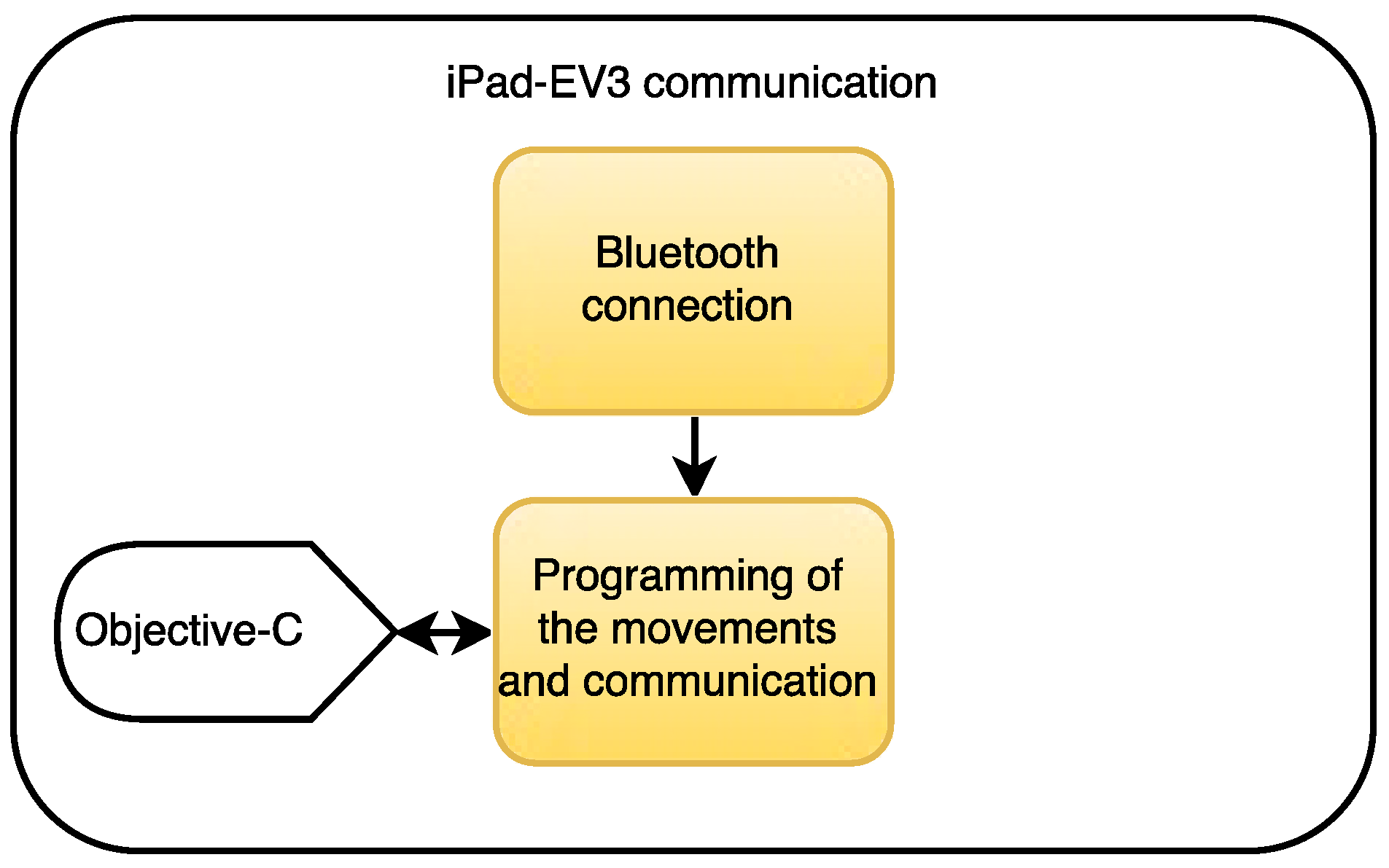
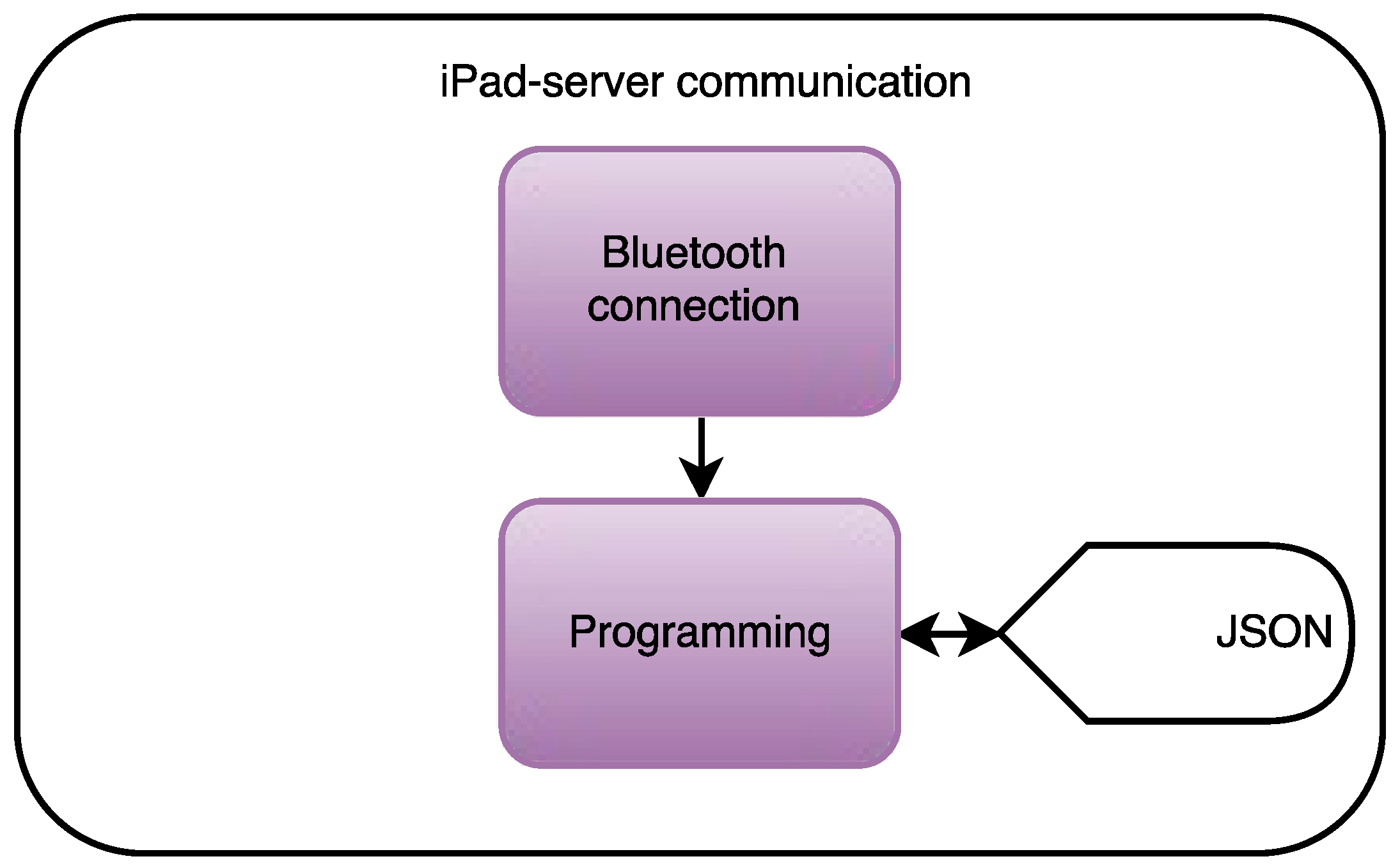
- Communication between the Lego EV3 brick and the program which will be run on the iPad.
- (4)
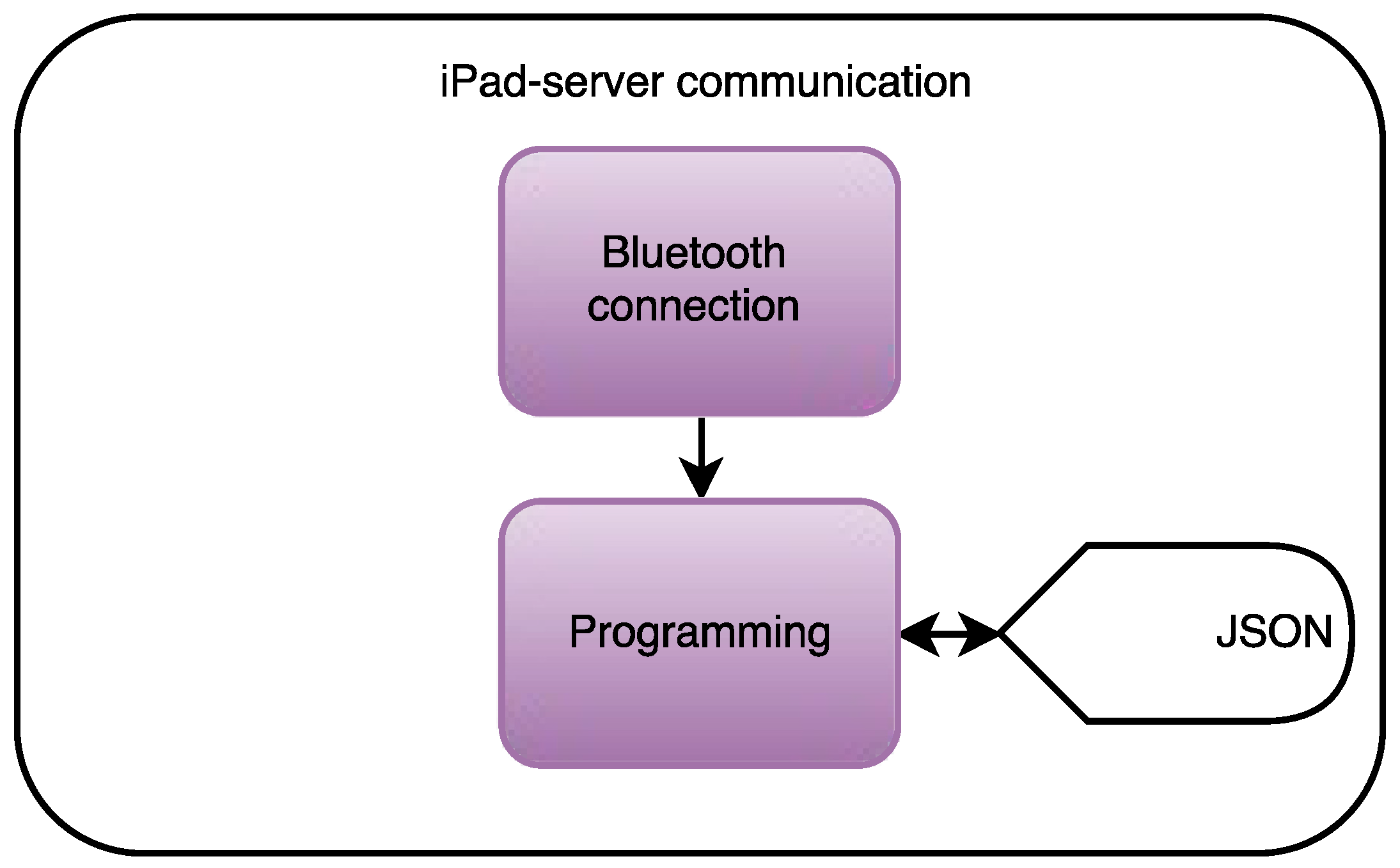
- Communication between the iPad and the server and the website accessible to the nursing home staff.
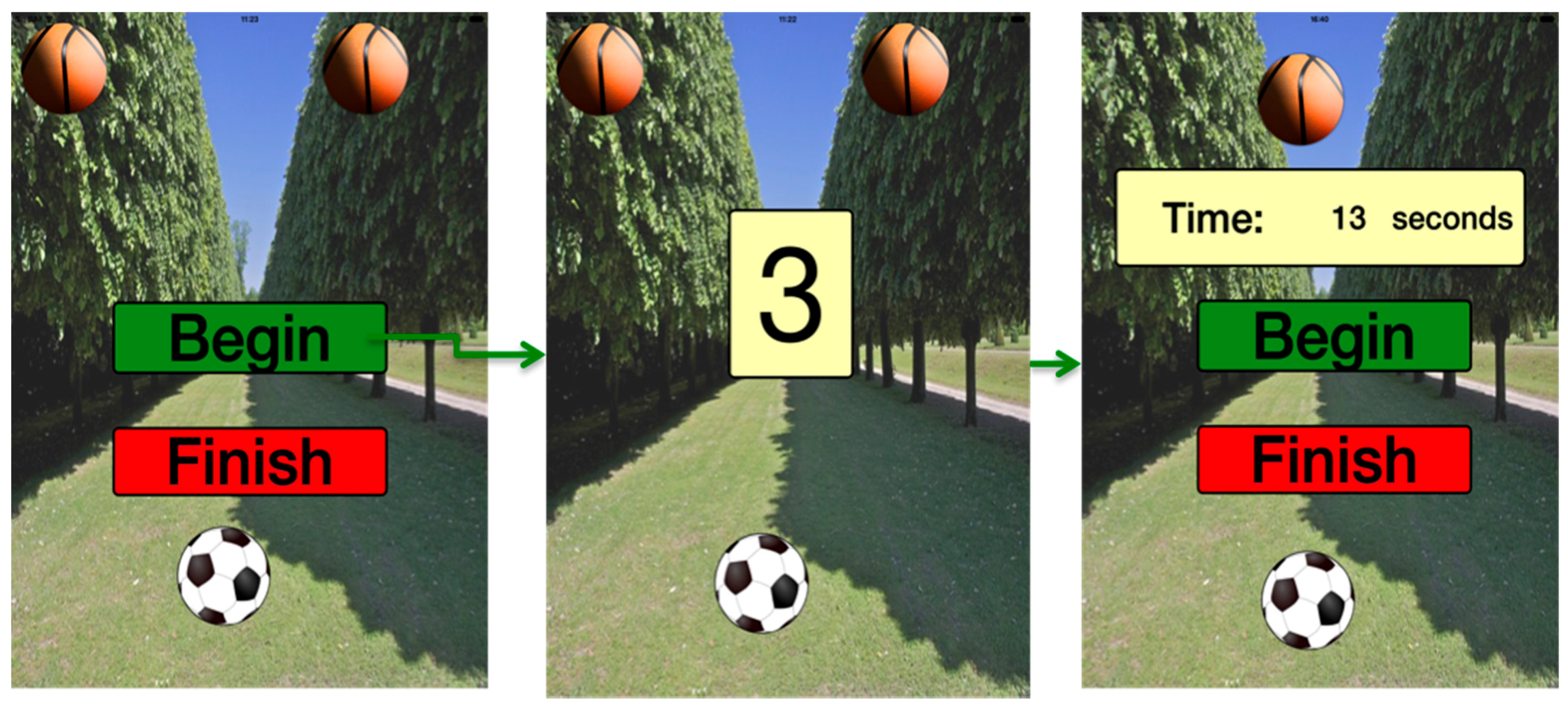
2.1.1. Stage 1: Graphical User Interface and Game Run on the iOS Application
2.1.2. Stage 2: Biofeedback
2.1.3. Stage 3: Data Acquisition of the Biological Sensors
2.1.4. Stage 2.2: Design of the Biofeedback System
2.1.5. Stage 3: Communication with the EV3 and Programming of the Activities
2.1.6. Stage 4: Data Cloud Computing
2.2. Materials
2.2.1. Hardware
2.2.2. Software
2.2.3. Participants
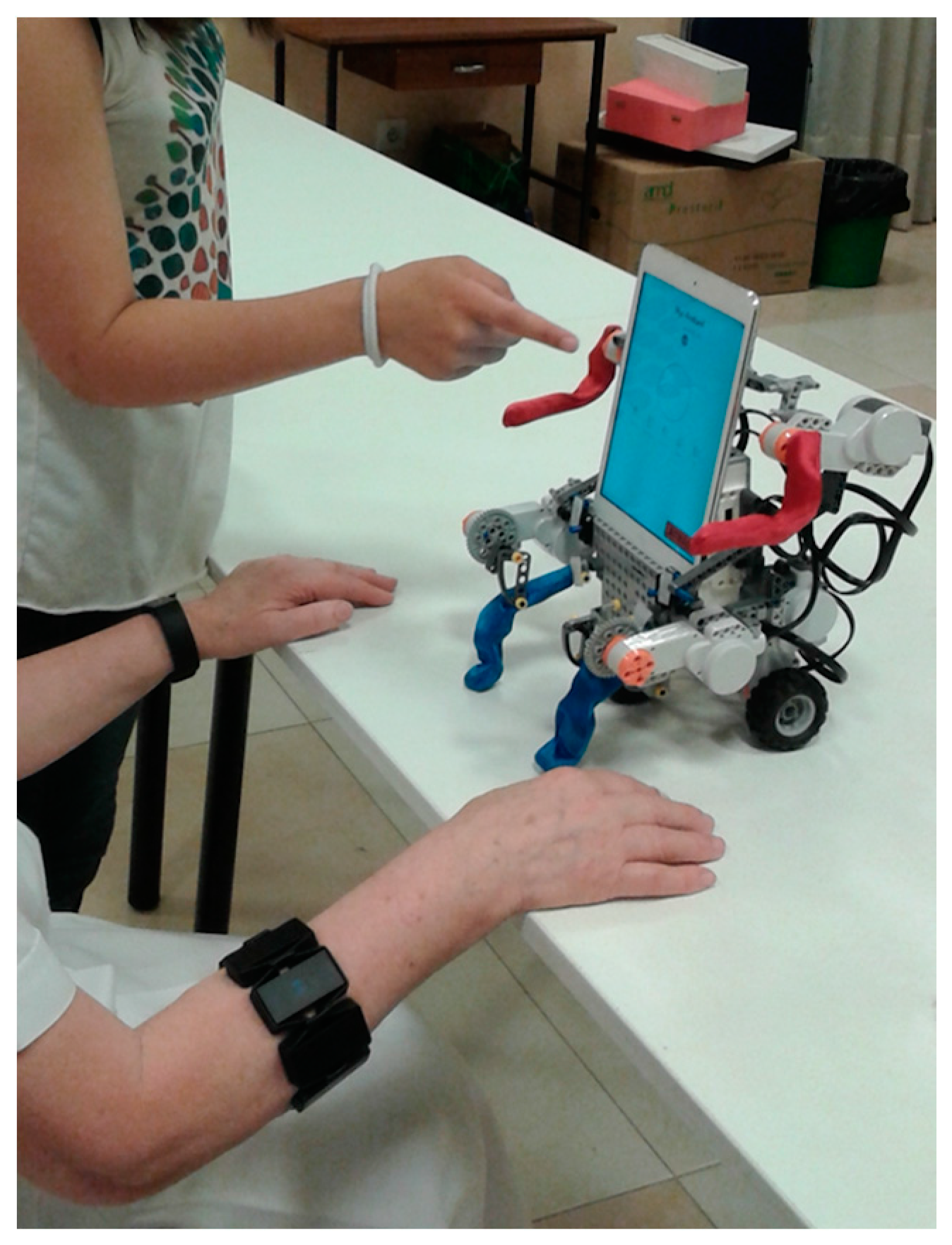
2.3. Implementation
2.4. Experimental Protocol
- In summary, the methodology applied to test the system can be described as follows:
- Location: the Santa y Real Casa de la Misericordia nursing home in Bilbao, Spain.
- Duration of the session: 25 min.
- Frequency: Once every 3 months.
- Exercise types: Cognitive and physical activities.
- Questionnaires:
- (1)
- WHOQOL-BREF
- (2)
- ICT Questionnaire
- (3)
- SUS
3. Results and Discussion
- WHOQOL DOM 1: physical health
- WHOQOL DOM 2: psychological domain
- WHOQOL DOM 3: social relationships
- WHOQOL DOM 4: environment
- The users from the Santa y Real Casa de la Misericordia nursing home were not familiar with ICTs. Hence, it has been noted that the scores obtained on the cognitive exercises improved after their initial contact with the system.
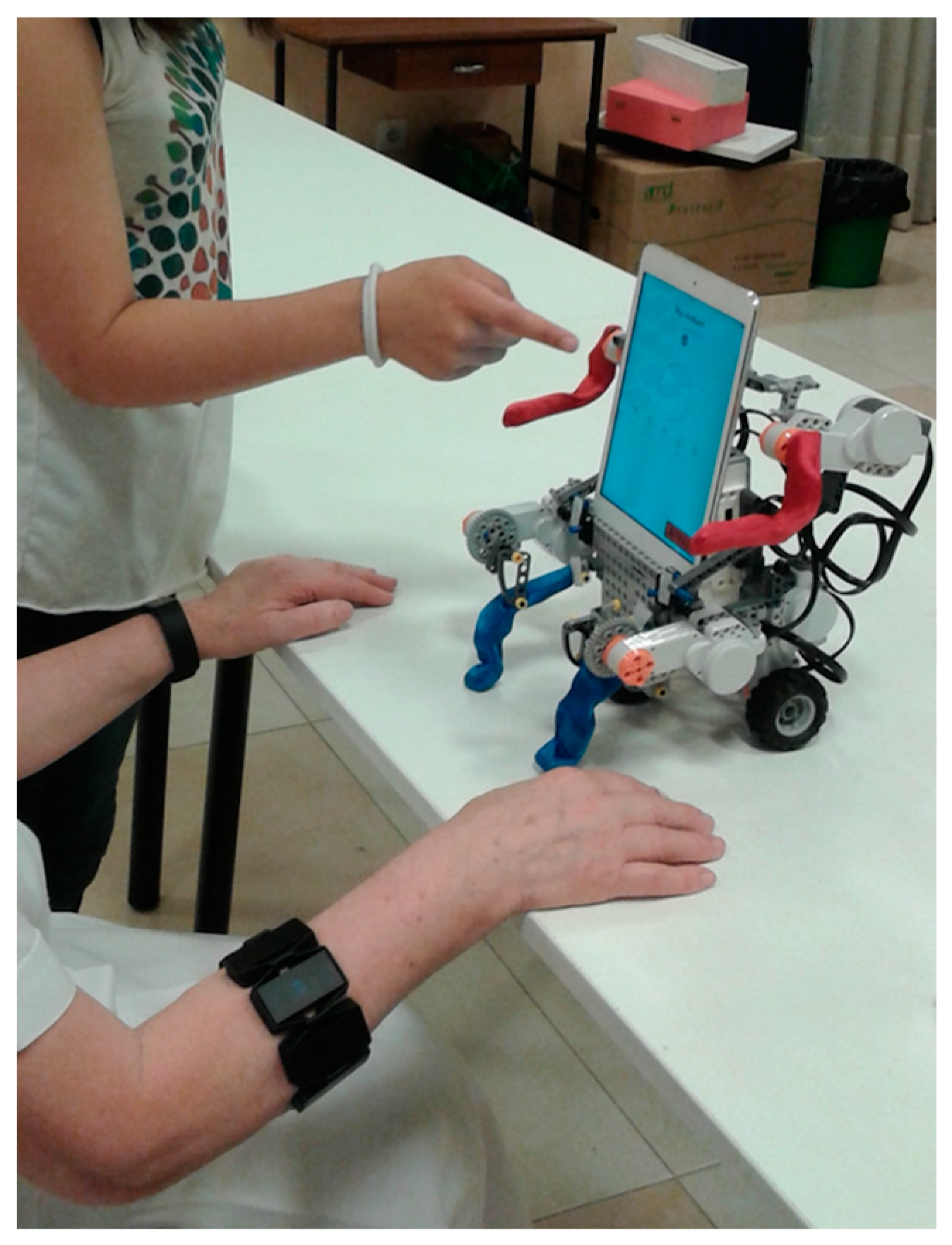
- Three of the seven users preferred playing without the MYO sensor. In fact, they preferred playing the game by controlling the ball with their finger. This was due to the fact that they were not accustomed either to using this kind of sensors or to controlling games with hand movements. In fact, elderly people consider putting external devices on their body to be too artificial. Therefore, the ideal system should provide the biofeedback in a totally unobtrusive mode.
4. Conclusions
4.1. Strengths
4.2. Limitations and Perspectives
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World-Birth Rate-Historical Data Graphs per Year. Available online: http://data.worldbank.org/indicator/SP.DYN.CBRT.IN (accessed on 2 June 2014).
- Aparicio García-Molina, V.A.; Carbonell-Baeza, A.; Delgado Fernández, M. Beneficios de la actividad física en personas mayores. Rev. Int. Med. Cienc. Act. Fís. Deport. 2010, 40, 4–20. [Google Scholar]
- Cantoral-Ceballos, J.; Nurgiyatna, N.; Wright, P.; Vaughan, J.; Brown-Wilson, C.; Scully, P.J.; Ozanya, K.B. Intelligent Carpet System, Based on Photonic Guided-Path Tomography, for Gait and Balance Monitoring in Home Environments. Sens. J. IEEE 2015, 15, 279–289. [Google Scholar] [CrossRef]
- Feil-Seifer, D.; Mataric, M.J. Defining socially assistive robotics. In Proceedings of the 9th International Conference on Rehabilitation Robotics, Chicago, IL, USA, 28 June–1 July 2005; pp. 465–468.
- Firedman, B.; Kahn, J.P.H.; Hagman, J. Hardware companions? What online AIBO discussion forums reveal about the human-robotic relationship. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Fort Lauderdale, FL, USA, 10–15 April 2003; pp. 273–280.
- Chang, W.L.; Šabanovic, S.; Huber, L. Use of seal-like robot PARO in sensory group therapy for older adults with dementia. In Proceedings of the 8th ACM/IEEE International Conference on Human-Robot Interaction, Tokyo, Japan, 3–6 March 2013; pp. 101–102.
- Short, E.; Swift-Spong, K.; Greczek, J.; Ramachandran, A.; Litoiu, A.; Grigore, E.C.; Feil-Seifer, D.; Shuster, S.; Lee, J.J.; Huang, S.; et al. How to train your DragonBot: Socially assistive robots for teaching children about nutrition through play. In Proceedings of the 23rd IEEE International Symposium on Robot and Human Interactive Communication, Edinburgh, UK, 25–29 August 2014; pp. 924–929.
- Stiehl, W.D.; Lee, J.K.; Breazeal, C.; Nalin, M.; Morandi, A.; Sanna, A. The huggable. In Proceedings of the 8th International Conference on Interaction Design and Children—IDC ’09, Como, Italy, 3–5 June 2009; p. 317.
- Gonzalez-Pacheco, V.; Ramey, A.; Alonso-Martin, F.; Castro-Gonzalez, A.; Salichs, M.A. Maggie: A Social Robot as a Gaming Platform. Int. J. Soc. Robot 2011, 3, 371–381. [Google Scholar] [CrossRef]
- Fasola, J.; Mataric, M.J. Robot exercise instructor: A socially assistive robot system to monitor and encourage physical exercise for the elderly. In Proceedings of the 19th International Symposium in Robot and Human Interactive Communication, Viareggio, Italy, 13–15 September 2010; pp. 416–421.
- Fasola, J.; Mataric, M.J. Using Socially Assistive human-robot interaction to monitvate physical exercise for older adults. Proc. IEEE 2012, 100, 2512–2526. [Google Scholar] [CrossRef]
- Fasola, J.; Mataric, M.J. Robot motivator: Increasing user enjoyment and performance on a physical/cognitive task. In Proceedings of the 2010 IEEE 9th International Conference on Development and Learning (ICDL), Ann Arbor, MI, USA, 18–21 August 2010; pp. 274–279.
- Vandermaesen, M.; Robert, K.; Luyten, K.; Coninx, K. ReHoblet—A home-based rehabilitation game on the tablet. In Proceedings of the 2014 IEEE 16th International Conference on e-Health Networking, Applications and Services (Healthcom), Nata, Brazil, 15–18 October 2014; pp. 411–416.
- Curtis, J.; Ruijs, L.; de Vries, M.; Winters, R.; Martens, J.B. Rehabilitation of handwriting skills in stroke patients using interactive games. In Proceedings of the 27th International Conference Extended Abstracts on Human Factors in Computing Systems—CHI EA ’09, Boston, MA, USA, 22–27 April 2009; p. 3931.
- Arshad, U.M.; Levine, J. Tablet PC Based Web Applications in the Rehabilitation of Stroke Patients; University of Strathclyd: Glasgow, UK, 2014. [Google Scholar]
- Papangelis, A.; Mouchakis, G.; Texas, A.B.; Kosmopoulos, D.; Karkaletsis, V.; Makedon, F. A game system for remote rehabilitation of cerebral palsy patients. In Proceedings of the 5th International Conference on PErvasive Technologies Related to Assistive Environments—PETRA ’12, Crete, Greece, 6–8 June 2012; p. 1.
- Barco, A.; Albo-Canals, J.; Ng, M.K.; Garriga, C.; Callejón, L.; Turón, M.; Gómez, C.; López-Sala, A. A Robotic Therapy for Children with TBI. In Proceedings of the 8th ACM/IEEE International Conference on Human-Robot Interaction, Tokyo, Japan, 3–6 March 2013; pp. 75–76.
- Pérez, P.J.; Garcia-Zapirain, B.; Mendez-Zorrilla, A. Caregiver and social assistant robot for rehabilitation and coaching for the elderly. Technol. Health Care 2015, 23, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Basmajian, J.V. Biofeedback in rehabilitation: A review of principles and practices. Arch. Phys. Med. Rehabil. 1981, 62, 469–475. [Google Scholar] [PubMed]
- Montoya, R.; Dupui, P.; Pagès, B.; Bessou, P. Step-length biofeedback device for walk rehabilitation. Med. Biol. Eng. Comput. 1994, 32, 416–420. [Google Scholar] [CrossRef] [PubMed]
- Lünenburger, L.; Colombo, G.; Riener, R. Biofeedback for robotic gait rehabilitation. J. Neuroeng. Rehabil. 2007, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Winters, J.M. UniTherapy: A Computer-Assisted Motivating Neurorehabilitation Platform for Teleassessment and Remote Therapy. In Proceedings of the 9th International Conference on Rehabilitation Robotics, Chicago, IL, USA, 28 June–1 July 2005; pp. 349–352.
- Chin, J.P.; Diehl, V.A.; Norman, K.L. Development of an instrument measuring user satisfaction of the human-computer interface. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Washington, DC, USA, 15–19 June 1988; pp. 213–218.
- World Health Organization, Division of Mental Health. WHOQOL-BREF: Introduction, Administration, Scoring and Generic Version of the Assessment: Field Trial Version, December 1996; World Health Organization: Geneva, Switzerland, 1996. [Google Scholar]
- Brooke, J. SUS—A quick and dirty usability scale. Usability Eval. Ind. 1996, 189, 4–7. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean * | SD | Minimum * | Maximum * | |
|---|---|---|---|---|
| SUS | 79.29 | 23.57 | 30.00 | 100.00 |
| Mean * | SD | Minimum * | Maximum * | |
|---|---|---|---|---|
| WHOQOL DOM 1 | 3.25 | 0.73 | 2.14 | 4.29 |
| WHOQOL DOM 2 | 3.71 | 0.46 | 2.83 | 4.33 |
| WHOQOL DOM 3 | 3.54 | 0.79 | 2.33 | 4.50 |
| WHOQOL DOM 4 | 4.10 | 0.44 | 3.75 | 4.88 |
| Mean * | SD | Minimum * | Maximum * | |
|---|---|---|---|---|
| HR at the beginning | 78.00 | 19.31 | 63.00 | 120.00 |
| HR at the end | 77.14 | 14.68 | 68.00 | 110.00 |
| Correlation Coefficient (R) | p-Value | |
|---|---|---|
| Game with MYO | 0.098 | 0.761 |
| Game without MYO | −0.429 | 0.176 |
| QUIS (general impression) | 0.617 | 0.06 |
| QUIS (screen section) | 0.293 | 0.362 |
| QUIS (information section) | 0.683 * | 0.033 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopez-Samaniego, L.; Garcia-Zapirain, B. A Robot-Based Tool for Physical and Cognitive Rehabilitation of Elderly People Using Biofeedback. Int. J. Environ. Res. Public Health 2016, 13, 1176. https://doi.org/10.3390/ijerph13121176
Lopez-Samaniego L, Garcia-Zapirain B. A Robot-Based Tool for Physical and Cognitive Rehabilitation of Elderly People Using Biofeedback. International Journal of Environmental Research and Public Health. 2016; 13(12):1176. https://doi.org/10.3390/ijerph13121176
Chicago/Turabian StyleLopez-Samaniego, Leire, and Begonya Garcia-Zapirain. 2016. "A Robot-Based Tool for Physical and Cognitive Rehabilitation of Elderly People Using Biofeedback" International Journal of Environmental Research and Public Health 13, no. 12: 1176. https://doi.org/10.3390/ijerph13121176