
Minimizing Spatial Variability of Healthcare Spatial Accessibility—The Case of a Dengue Fever Outbreak

Abstract
:1. Introduction
2. Materials and Methods
2.1. 3SFCA
2.2. Optimal Resource Allocation
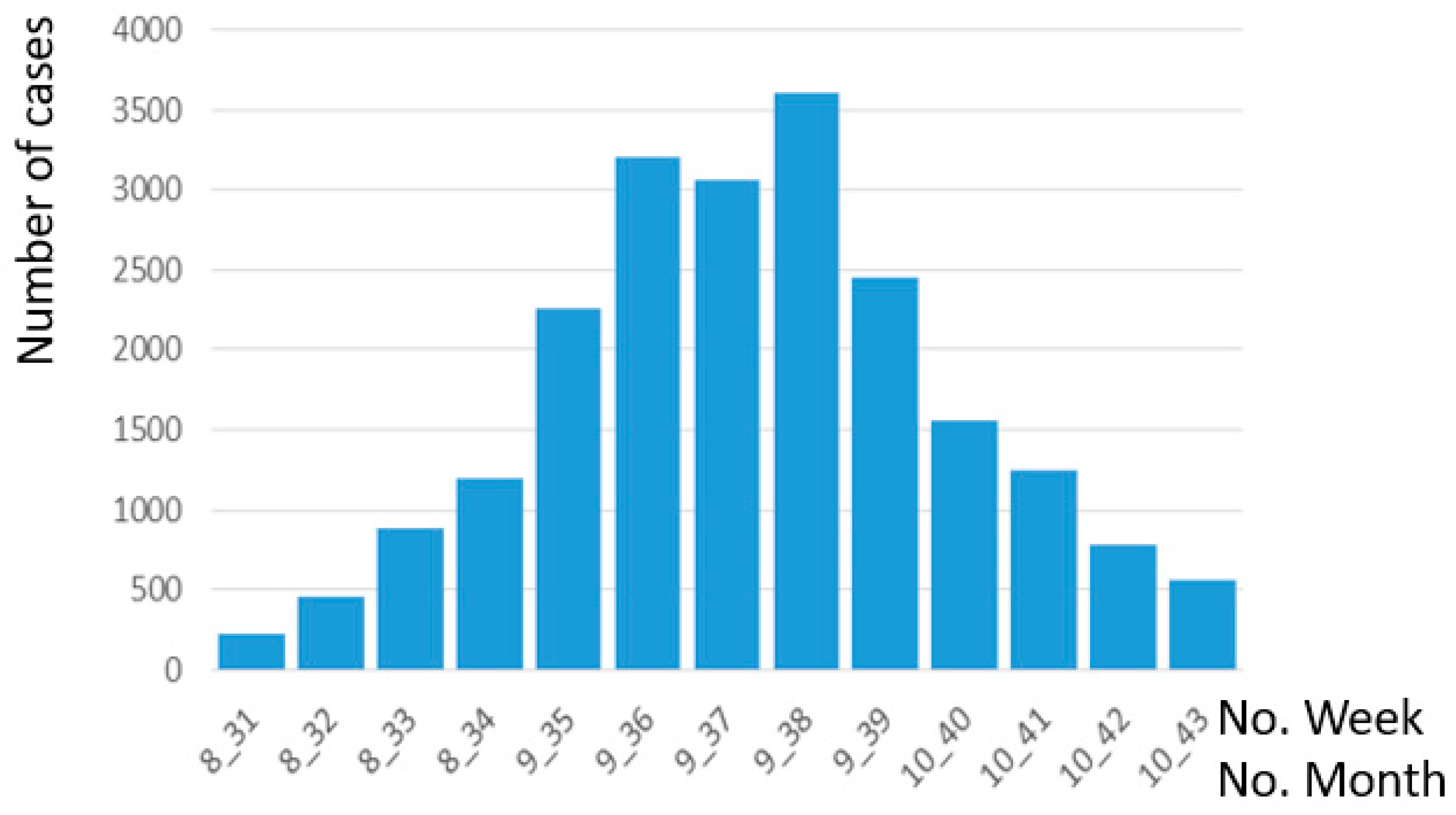
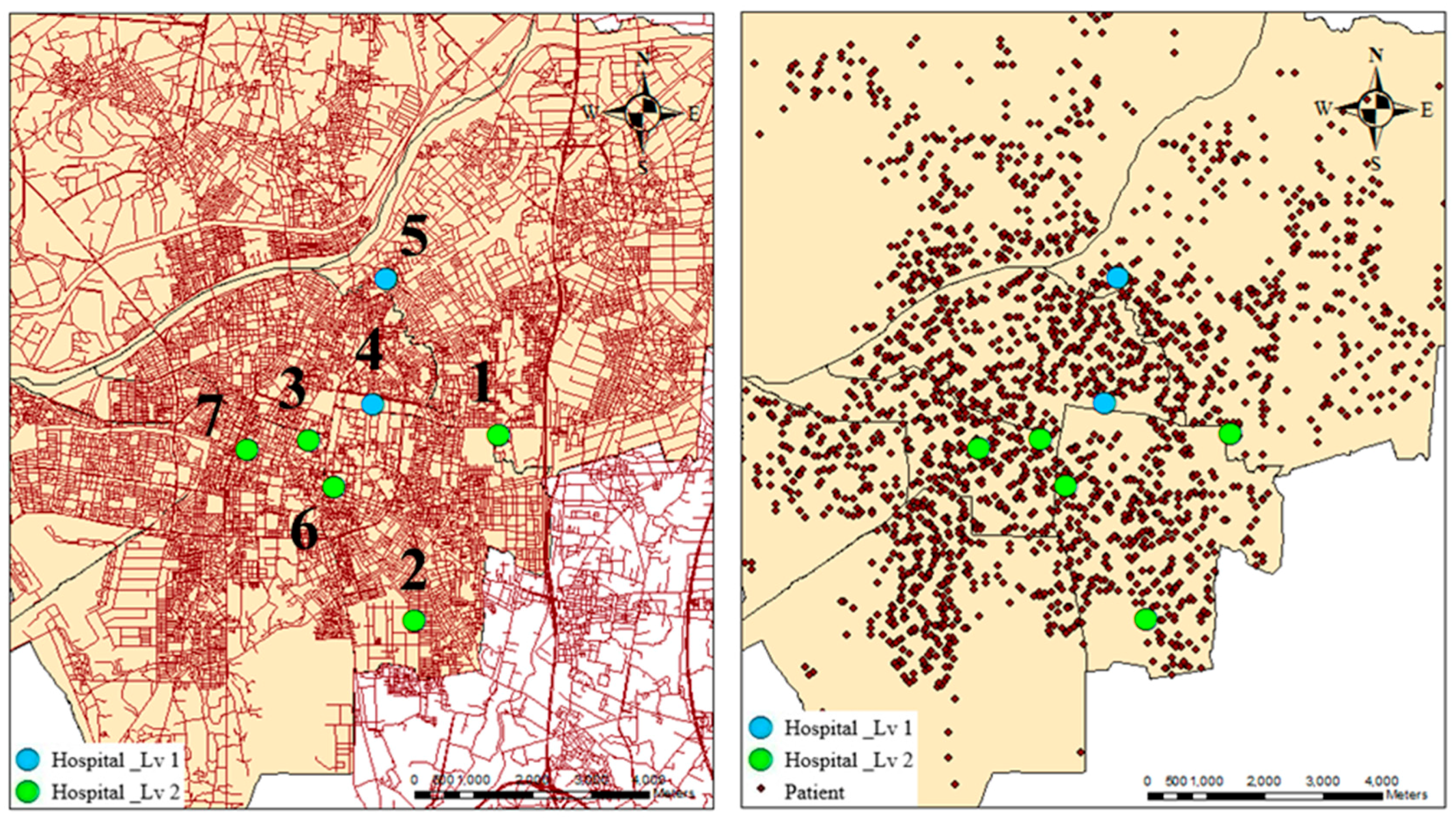
2.3. Data and Material
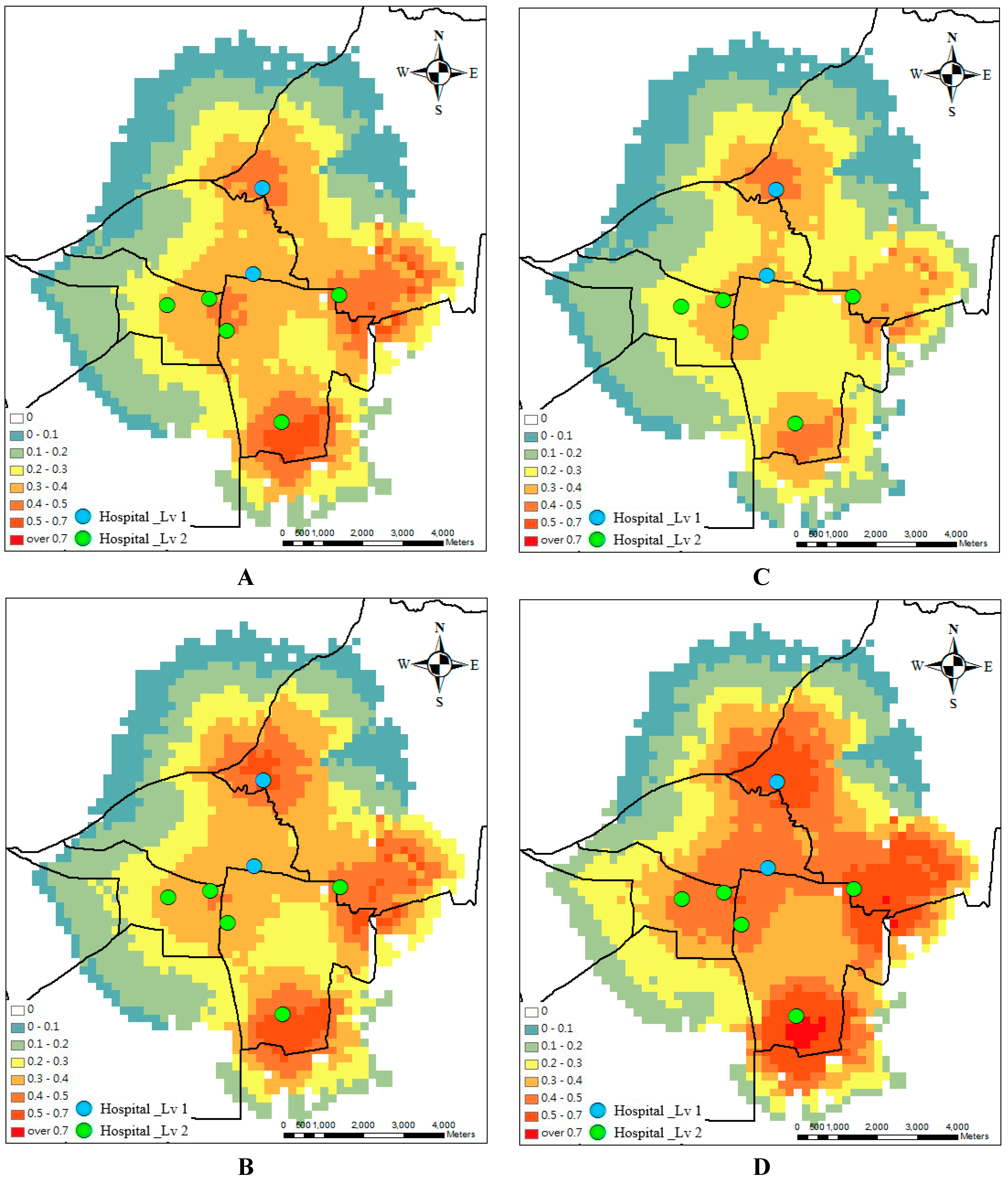
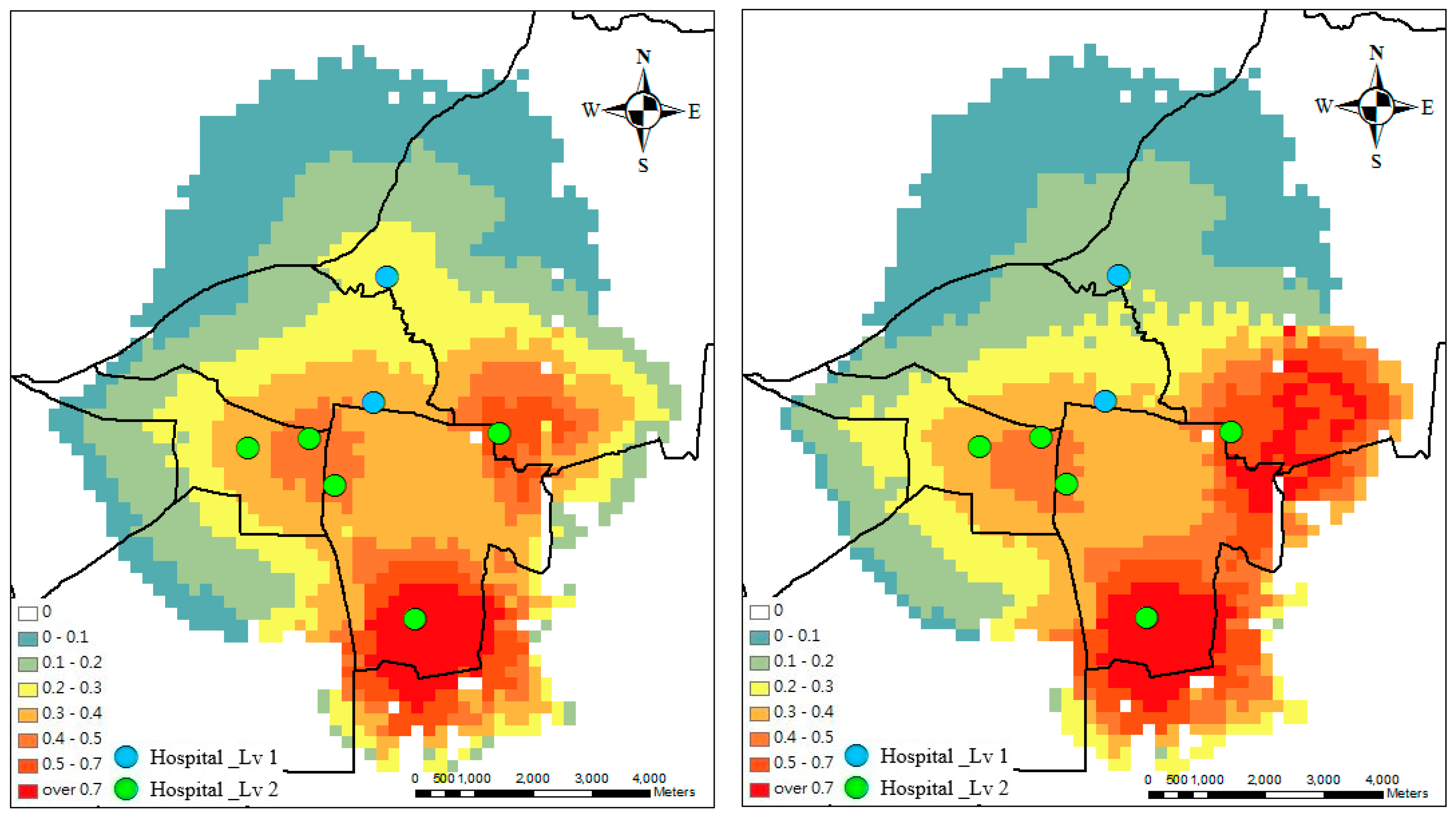
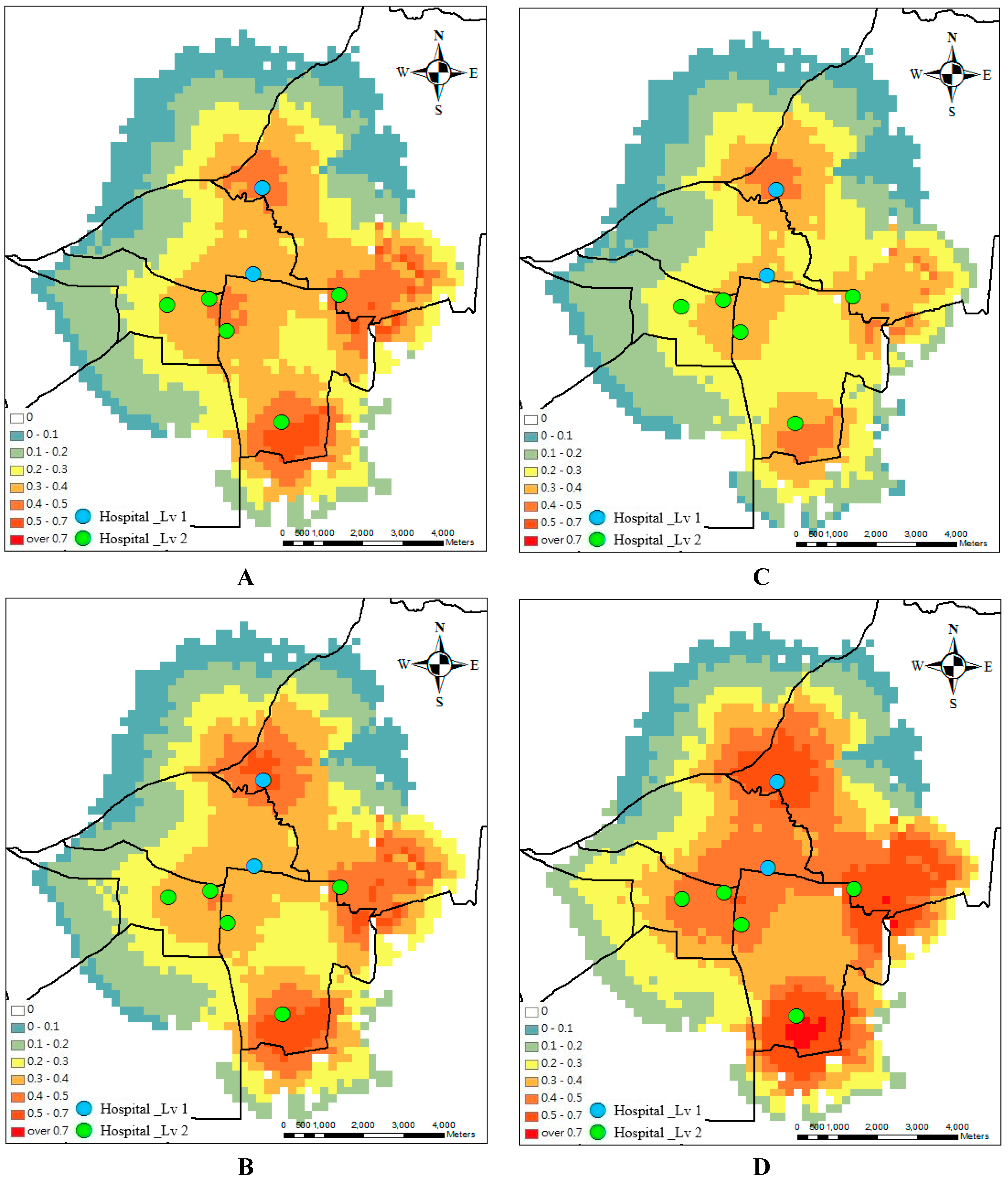
3. Results
4. Discussion
Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Gubler, D.J. Epidemic dengue/dengue hemorrhagic fever as a public health, social and economic problem in the 21st century. Trends Microbiol. 2002, 10, 100–103. [Google Scholar] [CrossRef]
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The global distribution and burden of dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taiwan National Infectious Disease Statistics System. Available online: http://nidss.cdc.gov.tw/en/SingleDisease.aspx?dc=1&dt=2&disease=061 (accessed on 10 March 2016).
- Harper, P.R. A Framework for Operational Modelling of Hospital Resources. Health Care Manag. Sci. 2002, 5, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Gossart, D.; Meskens, N.; Guinet, A. Strategic and Tactical Hospital Bed Management in Belgium and in France. In Proceedings of the Working Conference on Virtual Enterprises, Saint Etienne, France, 11–13 October 2010; Springer: Saint Etienne, France; pp. 243–250.
- World Health Organization. Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Khan, A.A. An integrated approach to measuring potential spatial access to health care services. Socio-Econ. Plan. Sci. 1992, 26, 275–287. [Google Scholar] [CrossRef]
- Harper, R.P.; Shahani, K.A. Modelling for the planning and management of bed capacities in hospitals. J. Oper. Res. Soc. 2002, 53, 11–18. [Google Scholar] [CrossRef]
- Luo, W.; Wang, F. Measures of spatial accessibility to health care in a GIS environment: Synthesis and a case study in the Chicago region. Environ. Plan. B Plan. Des. 2003, 30, 865–884. [Google Scholar] [CrossRef]
- Langford, M.; Higgs, G. Measuring Potential Access to Primary Healthcare Services: The Influence of Alternative Spatial Representations of Population. Prof. Geogr. 2006, 58, 294–306. [Google Scholar] [CrossRef]
- Polo, G.; Acosta, C.M.; Ferreira, F.; Dias, R.A. Location-Allocation and Accessibility Models for Improving the Spatial Planning of Public Health Services. PLoS ONE 2015, 10, e0119190. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; McLafferty, S.; Escamilla, V.; Luo, L. Late-Stage Breast Cancer Diagnosis and Health Care Access in Illinois. Prof. Geogr. J. Assoc. Am. Geogr. 2008, 60, 54–69. [Google Scholar] [CrossRef] [PubMed]
- Luo, W.; Qi, Y. An enhanced two-step floating catchment area (E2SFCA) method for measuring spatial accessibility to primary care physicians. Health Place 2009, 15, 1100–1107. [Google Scholar] [CrossRef] [PubMed]
- Guagliardo, M. Spatial accessibility of primary care: Concepts, methods and challenges. Int. J. Health Geogr. 2004, 3, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, D. Black residential segregation, disparities in spatial access to health care facilities, and late-stage breast cancer diagnosis in metropolitan Detroit. Health Place 2010, 16, 1038–1052. [Google Scholar] [CrossRef] [PubMed]
- Wan, N.; Zou, B.; Sternberg, T. A three-step floating catchment area method for analyzing spatial access to health services. Int. J. Geogr. Inf. Sci. 2012, 26, 1073–1089. [Google Scholar] [CrossRef]
- Luo, J. Integrating the Huff Model and Floating Catchment Area Methods to Analyze Spatial Access to Healthcare Services. Trans. GIS 2014, 18, 436–448. [Google Scholar] [CrossRef]
- Cheng, G.; Zeng, X.; Duan, L.; Lu, X.; Sun, H.; Jiang, T.; Li, Y. Spatial difference analysis for accessibility to high level hospitals based on travel time in Shenzhen, China. Habitat Int. 2016, 53, 485–494. [Google Scholar] [CrossRef]
- Wang, F.; Tang, Q. Planning toward equal accessibility to services: A quadratic programming approach. Environ. Plan. B: Plan. Des. 2013, 40, 195–212. [Google Scholar] [CrossRef]
- Kennedy, J.; Eberhart, R. Particle swarm optimization. In Proceedings of the 1995 IEEE International Conference on Neural Networks, Perth, Australia, 27 November–1 December 1995; Volume 4, pp. 1942–1948.
- Joseph, A.E.; Phillips, D.R. Accessibility and Utilization: Geographical Perspectives on Health Care Delivery; Harper and Row: New York, NY, USA, 1984. [Google Scholar]
- World Health Organization. Handbook for Clinical Management of Dengue; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Chen, C.M.; Chan, K.S.; Yu, W.L.; Cheng, K.C.; Chao, H.C.; Yeh, C.Y.; Lai, C.C. The outcomes of patients with severe dengue admitted to intensive care units. Medicine (Baltimore) 2016, 95, e4376. [Google Scholar] [CrossRef] [PubMed]
- Casas, I.; Delmelle, E.; Delmelle, E.C. Potential versus revealed access to care during a dengue fever outbreak. J. Transp. Health 2016. [Google Scholar] [CrossRef]
- Wu, T.Y.; Majeed, A.; Kuo, K.N. An overview of the healthcare system in Taiwan. Lond. J. Prim. Care (Abingdon) 2010, 3, 115–119. [Google Scholar] [CrossRef]
- Bagust, A.; Place, M.; Posnett, J.W. Dynamics of Bed Use in Accommodating Emergency Admissions: Stochastic Simulation Model. BMJ 1999, 319, 155–158. [Google Scholar] [CrossRef] [PubMed]
- Günal, M.M.; Pidd, M. Discrete event simulation for performance modelling in health care: A review of the literature. J. Simul. 2010, 4, 42–51. [Google Scholar] [CrossRef]
- Hick, J.L.; Hanfling, D.; Burstein, J.L.; DeAtley, C.; Barbisch, D.; Bogdan, G.M.; Cantrill, S. Health care facility and community strategies for patient care surge capacity. Ann. Emerg. Med. 2004, 44, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Davis, D.P.; Poste, J.C.; Hicks, T.; Polk, D.; Rymer, T.E.; Jacoby, I. Hospital bed surge capacity in the event of a mass-casualty incident. Prehosp. Disaster Med. 2005, 20, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Yi, P.; George, S.K.; Paul, J.A.; Lin, L. Hospital capacity planning for disaster emergency management. Socio-Econ. Plan. Sci. 2010, 44, 151–160. [Google Scholar] [CrossRef]
- Rebmann, T.; Carrico, R.; English, J.F. Hospital infectious disease emergency preparedness: A survey of infection control professionals. Am. J. Infect. Control 2007, 35, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Miro, O.; Antonio, M.; Jimenez, S.; De Dios, A.; Sanchez, M.; Borras, A.; Milla, J. Decreased health care quality associated with emergency department overcrowding. Eur. J. Emerg. Med. 1999, 6, 105–107. [Google Scholar] [CrossRef] [PubMed]
- South Regional Emergency Operations Center, Department of Health, Executive Yuan, Taiwan, R.O.C. Available online: http://seoc.hosp.ncku.edu.tw/eoc/en/eoc_en.htm (accessed on 23 November 2016).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Week | Accessibility SD before Design | Accessibility SD after Design | Differences |
|---|---|---|---|
| 1 | 0.22 | 0.13 | −0.09 |
| 2 | 0.21 | 0.13 | −0.08 |
| 3 | 0.16 | 0.11 | −0.05 |
| 4 | 0.22 | 0.16 | −0.06 |
| Average | 0.20 | 0.13 | −0.07 |
| No. | Hospital Level | Original Supply | Optimal Supply at Week 1 | Optimal Supply at Week 2 | Optimal Supply at Week 3 | Optimal Supply at Week 4 |
|---|---|---|---|---|---|---|
| 1 | 2 | 74 | 45.5 | 48.8 | 48.8 | 51.6 |
| 2 | 2 | 79 | 44.5 | 49.4 | 48.4 | 66.2 |
| 3 | 2 | 160 | 90.0 | 126.0 | 73.9 | 111.9 |
| 4 | 1 | 106 | 148.5 | 136.4 | 141.8 | 142.2 |
| 5 | 1 | 65 | 160.0 | 159.5 | 160.0 | 160.0 |
| 6 | 2 | 87 | 104.5 | 73.1 | 121.5 | 61.0 |
| 7 | 2 | 152 | 130.0 | 129.8 | 128.6 | 130.0 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chu, H.-J.; Lin, B.-C.; Yu, M.-R.; Chan, T.-C. Minimizing Spatial Variability of Healthcare Spatial Accessibility—The Case of a Dengue Fever Outbreak. Int. J. Environ. Res. Public Health 2016, 13, 1235. https://doi.org/10.3390/ijerph13121235
Chu H-J, Lin B-C, Yu M-R, Chan T-C. Minimizing Spatial Variability of Healthcare Spatial Accessibility—The Case of a Dengue Fever Outbreak. International Journal of Environmental Research and Public Health. 2016; 13(12):1235. https://doi.org/10.3390/ijerph13121235
Chicago/Turabian StyleChu, Hone-Jay, Bo-Cheng Lin, Ming-Run Yu, and Ta-Chien Chan. 2016. "Minimizing Spatial Variability of Healthcare Spatial Accessibility—The Case of a Dengue Fever Outbreak" International Journal of Environmental Research and Public Health 13, no. 12: 1235. https://doi.org/10.3390/ijerph13121235