
Perception of Environmental Risks and Health Promotion Attitudes of French Perinatal Health Professionals

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
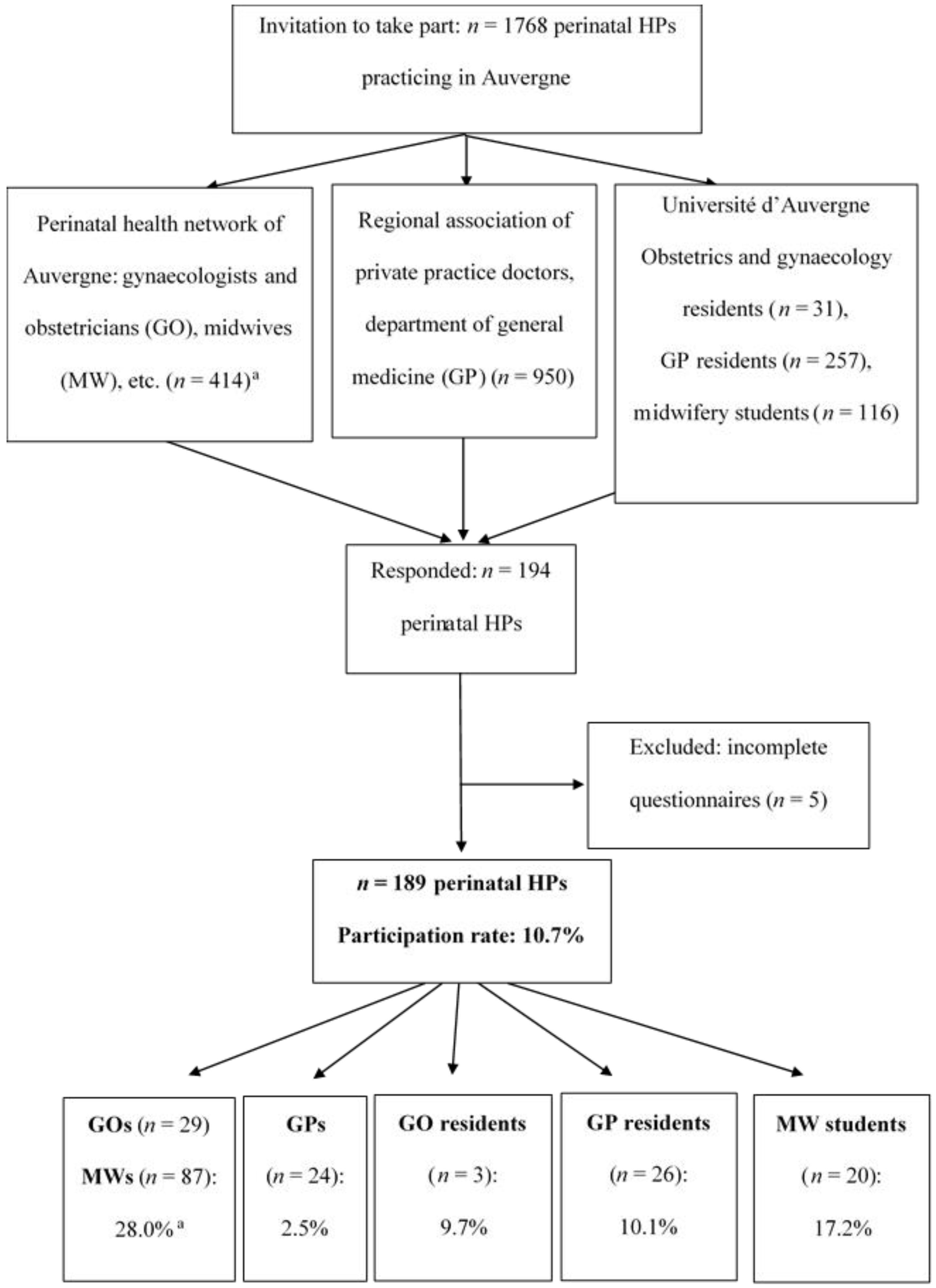
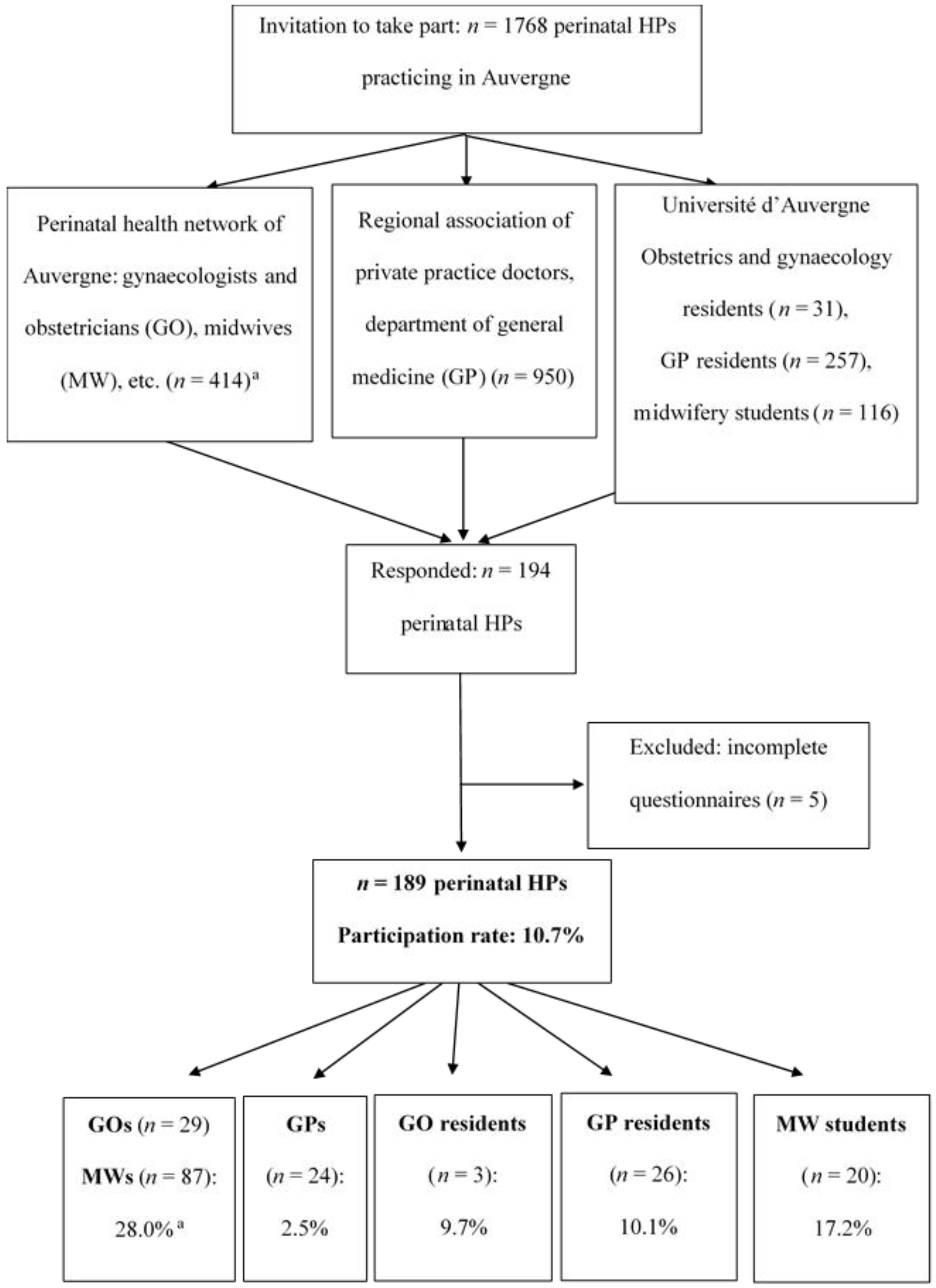
2.1. Subjects
2.2. Study Design
2.3. Data Collection
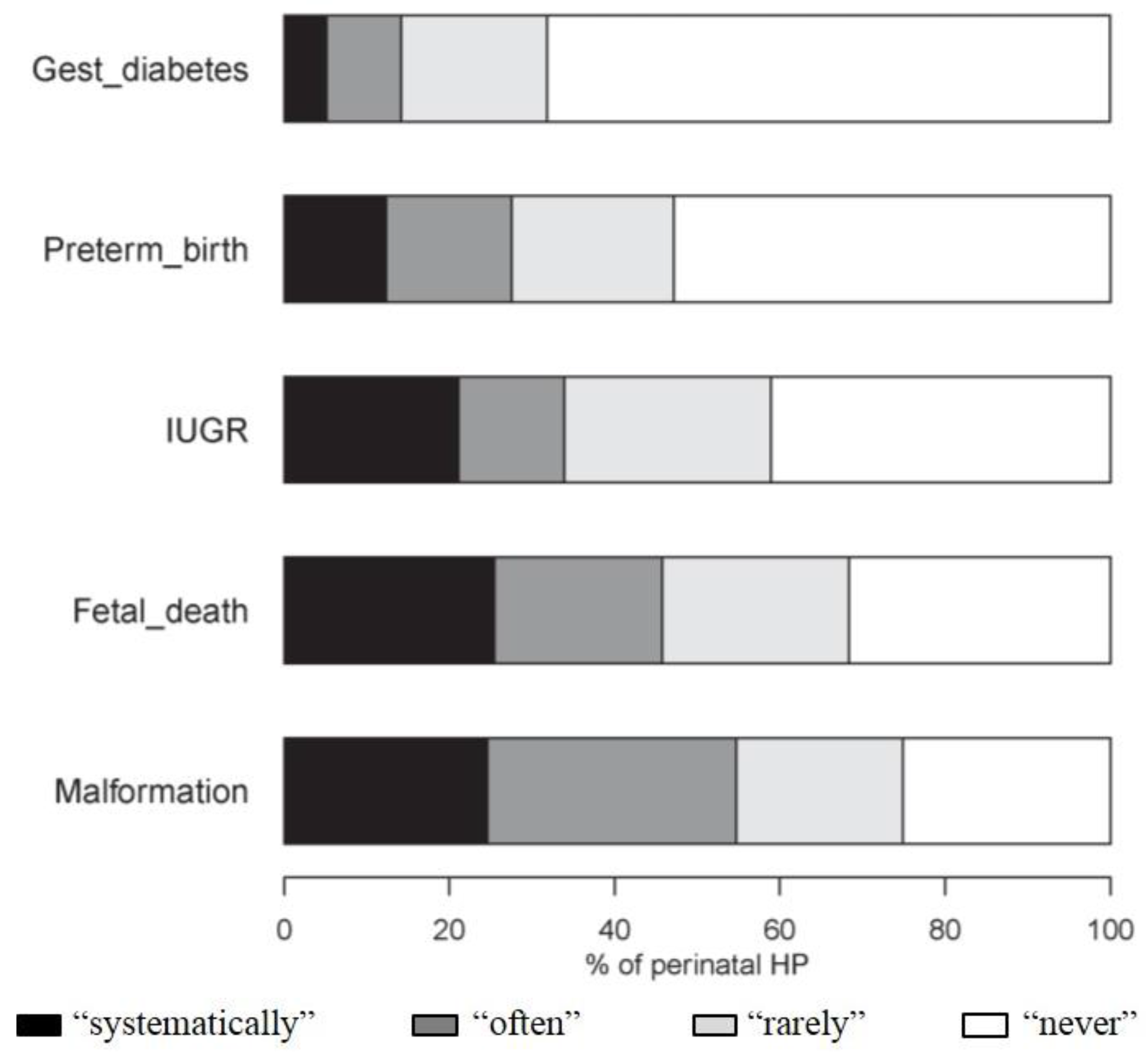
2.4. Assessment of Perception of the Risk to the in Utero Exposure of 19 Environmental Factors
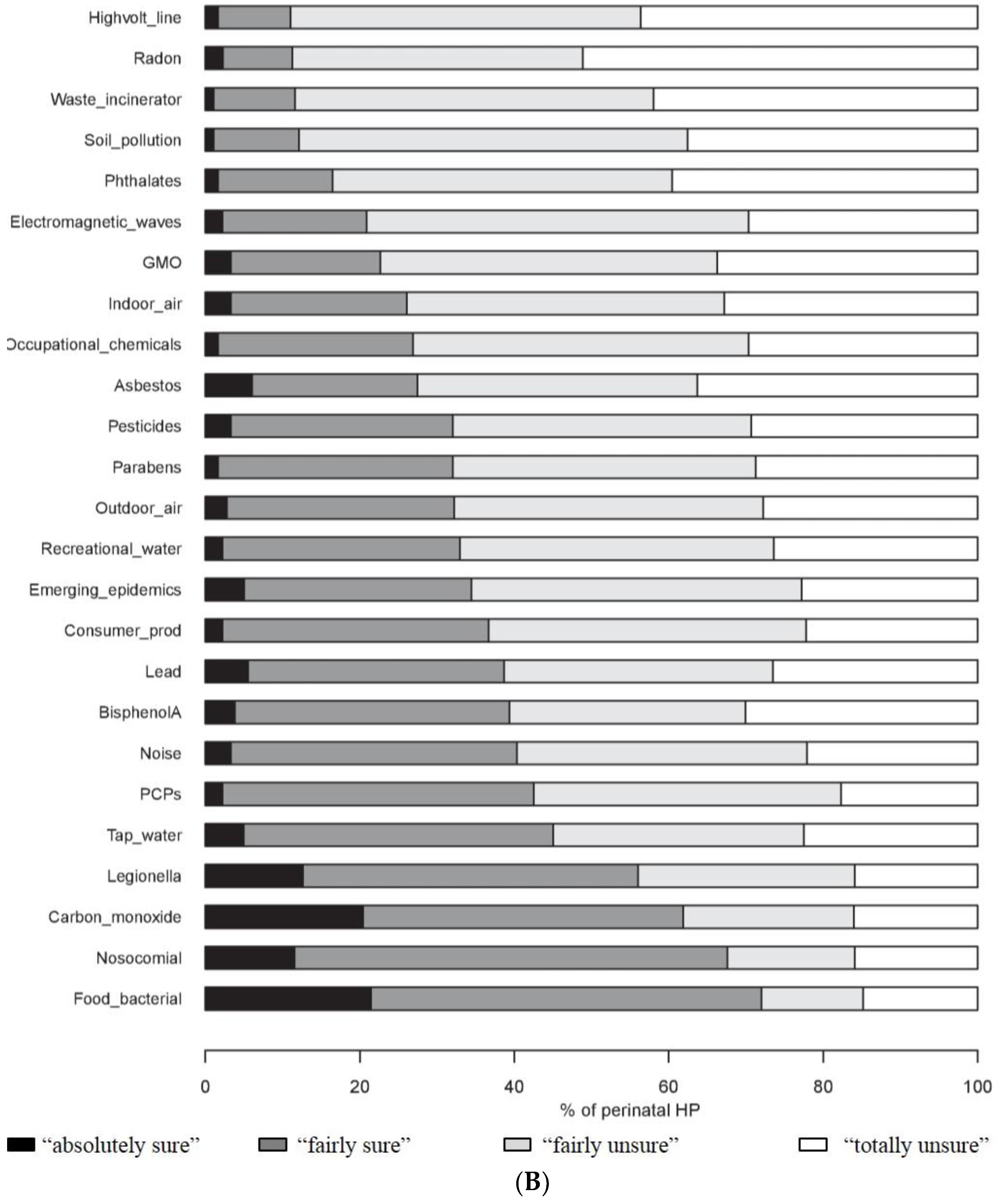
2.5. Assessment of the Extent of Knowledge about Environmental Factors
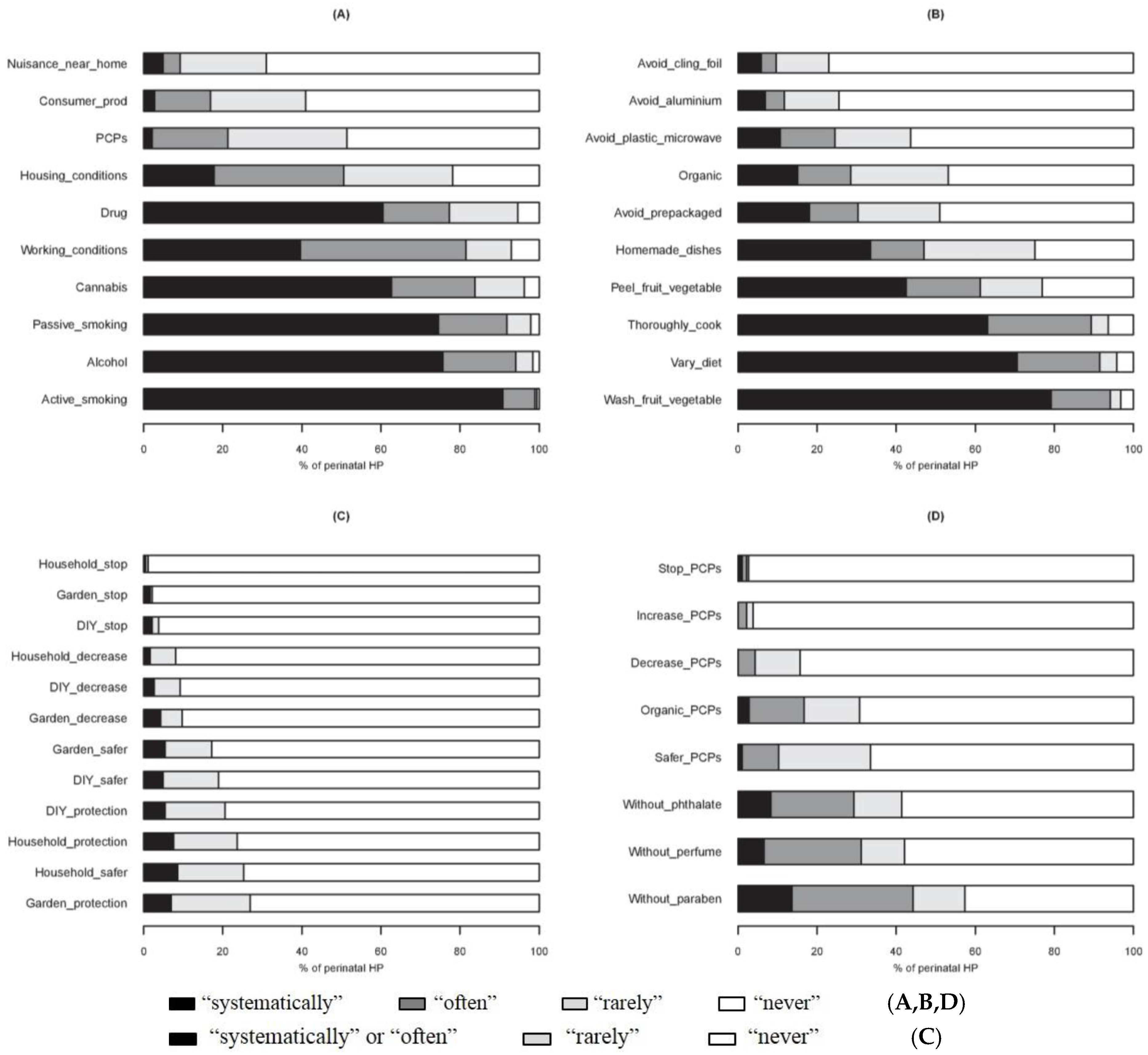
2.6. Assessment of Preventive Attitudes towards Chemical Exposure of Pregnant Women
2.7. Statistical Analysis
3. Results
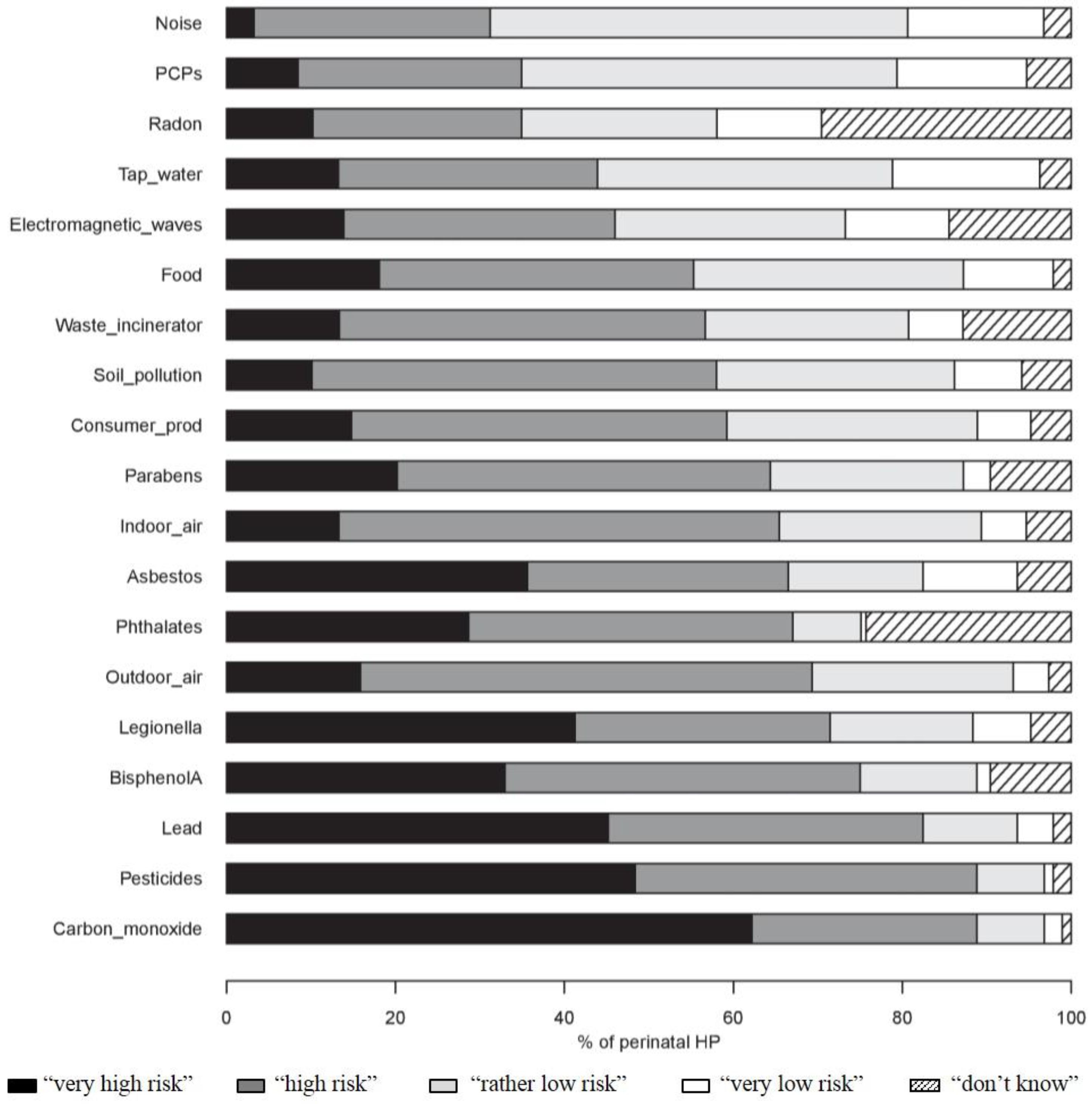
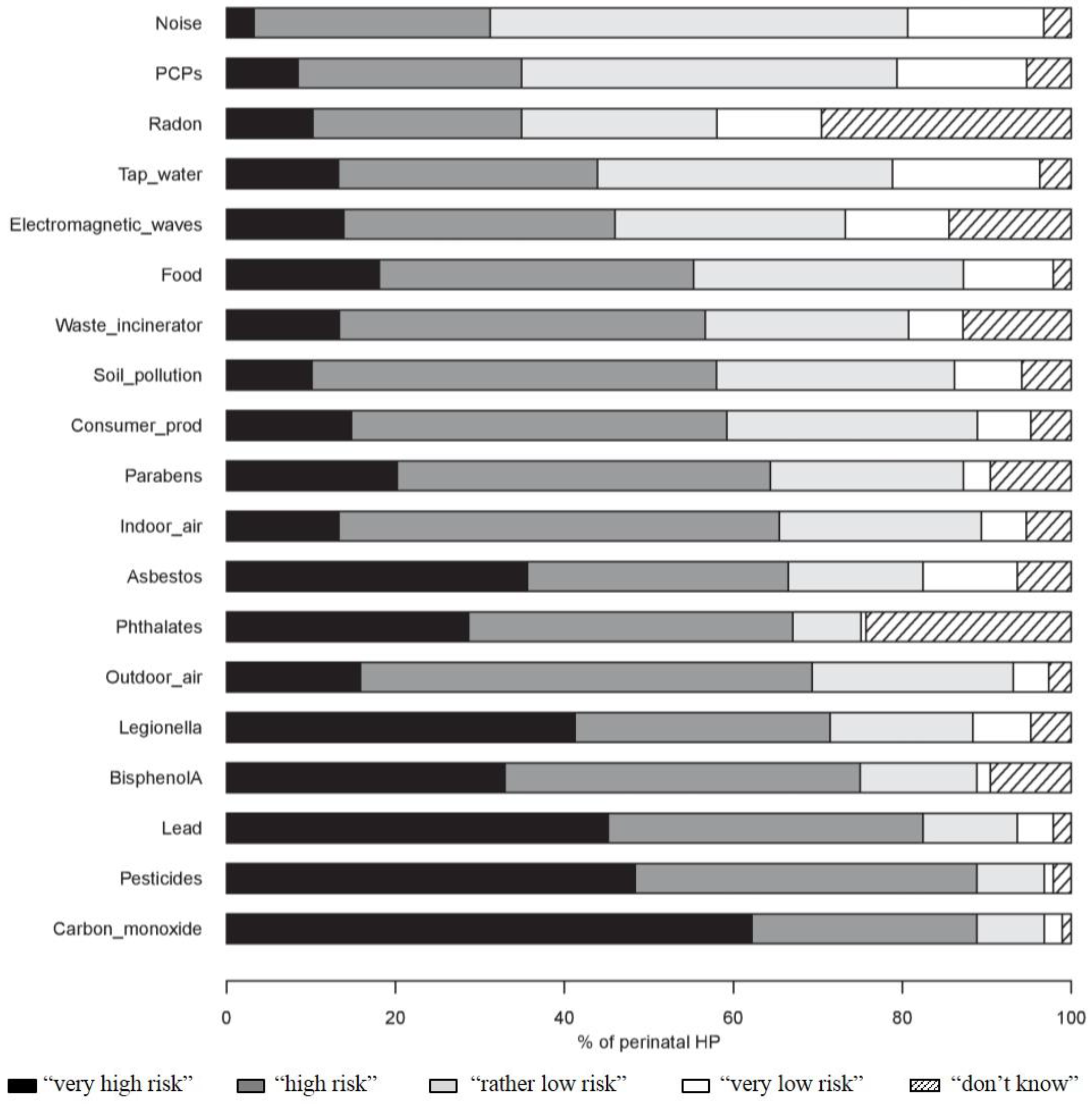
3.1. Risk Perception of Exposure to Environmental Factors for Pregnant Women and Their Unborn Baby
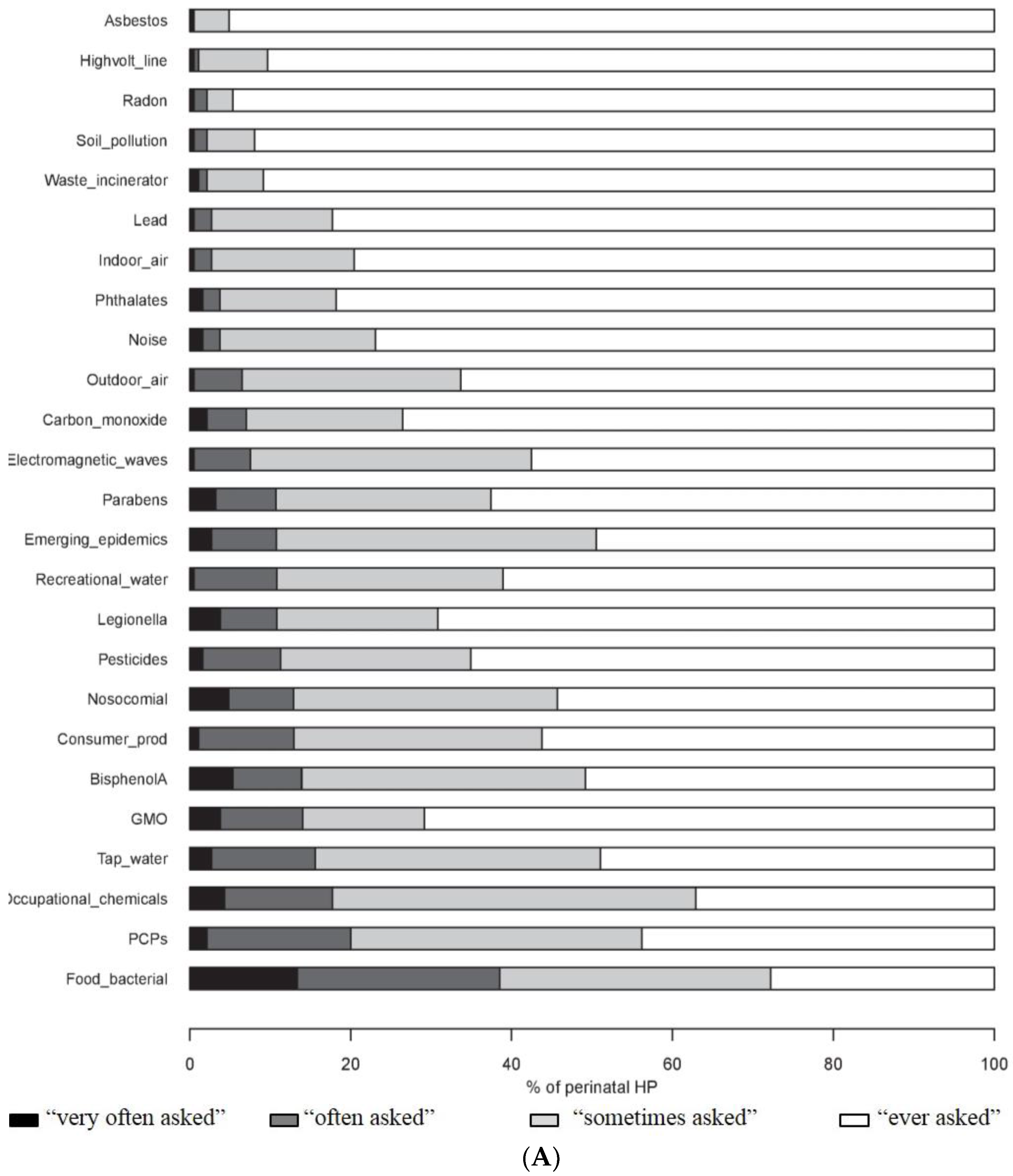
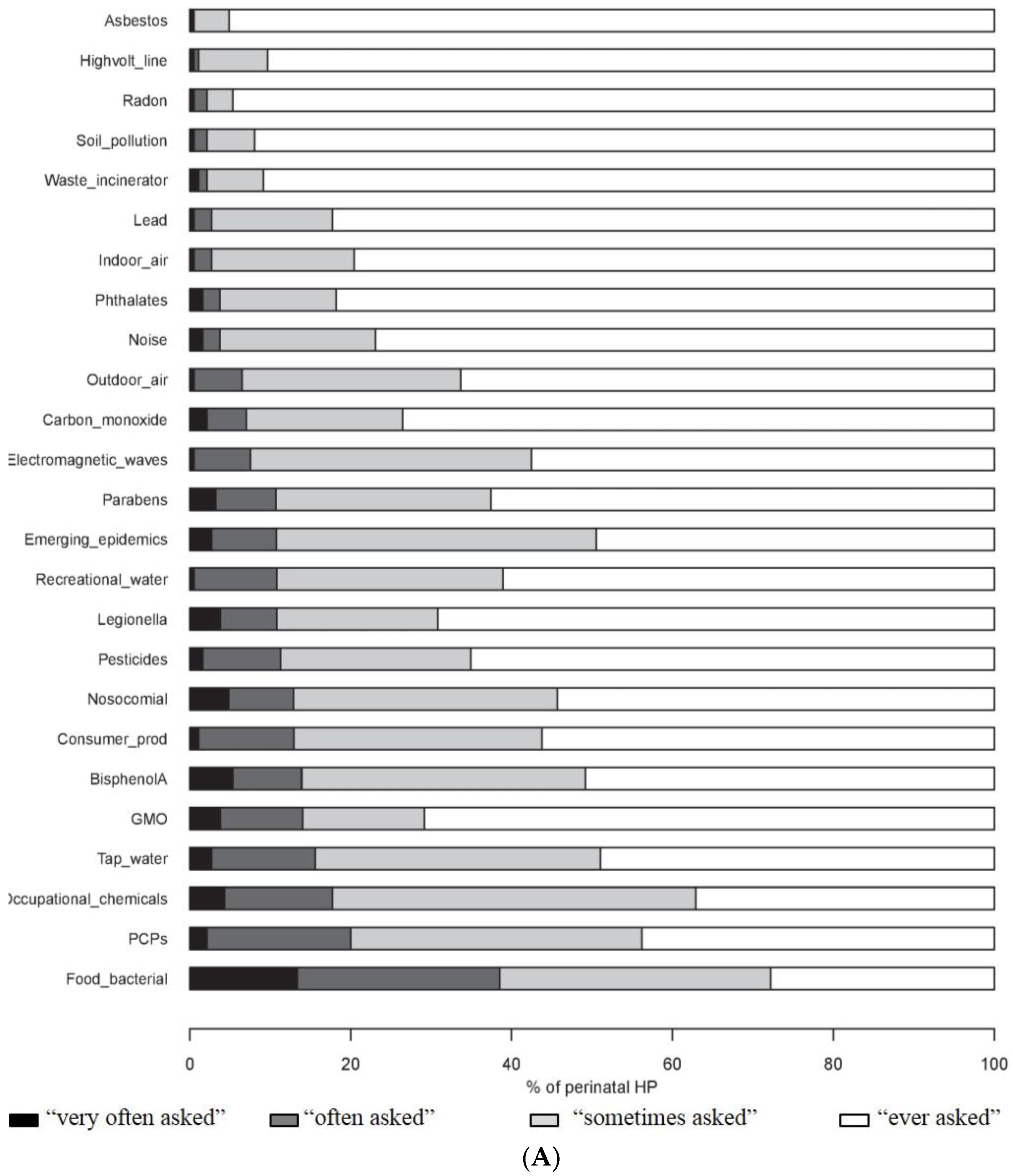
3.2. Enquiries to HPs by Pregnant Women about Environmental Issues
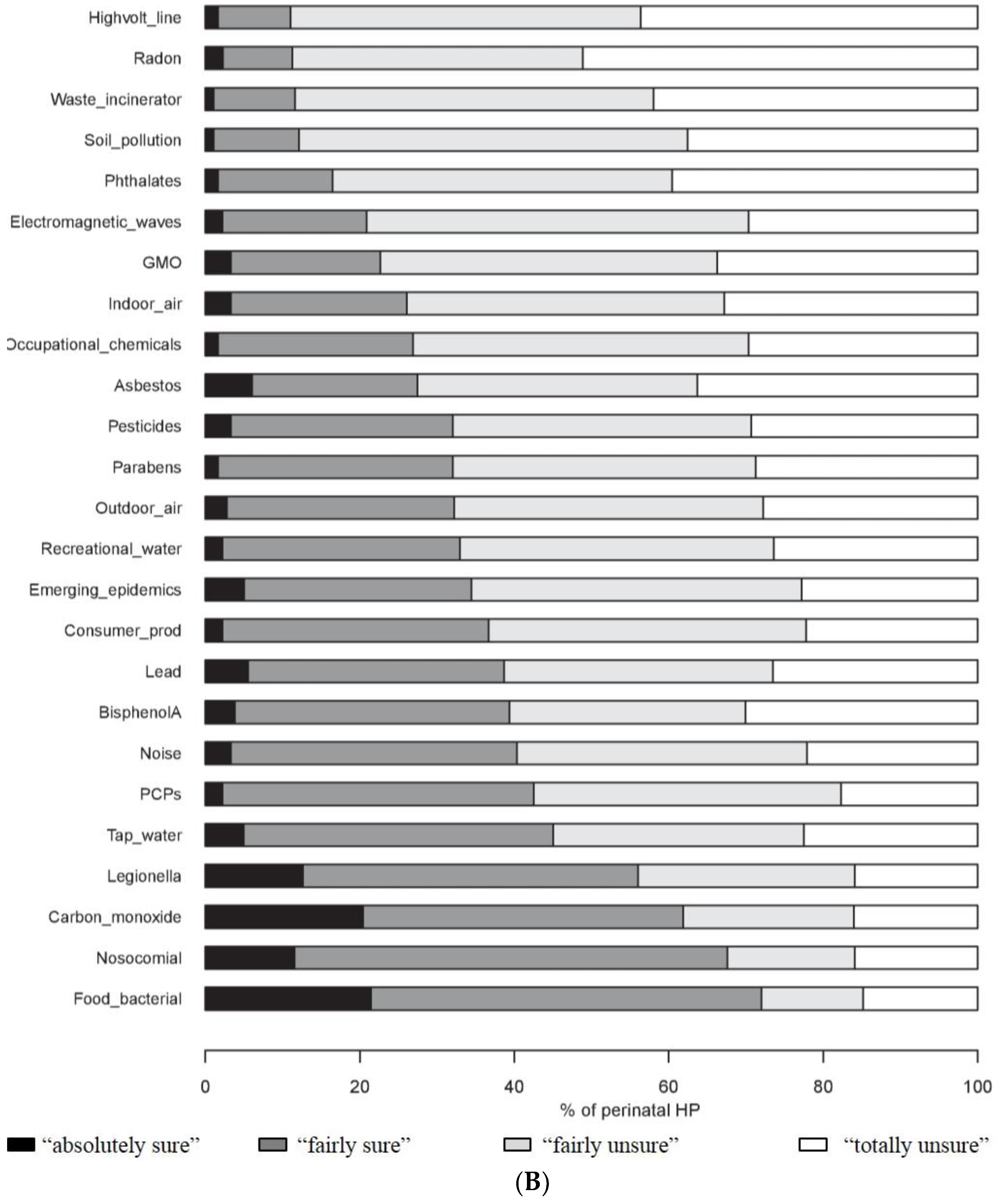
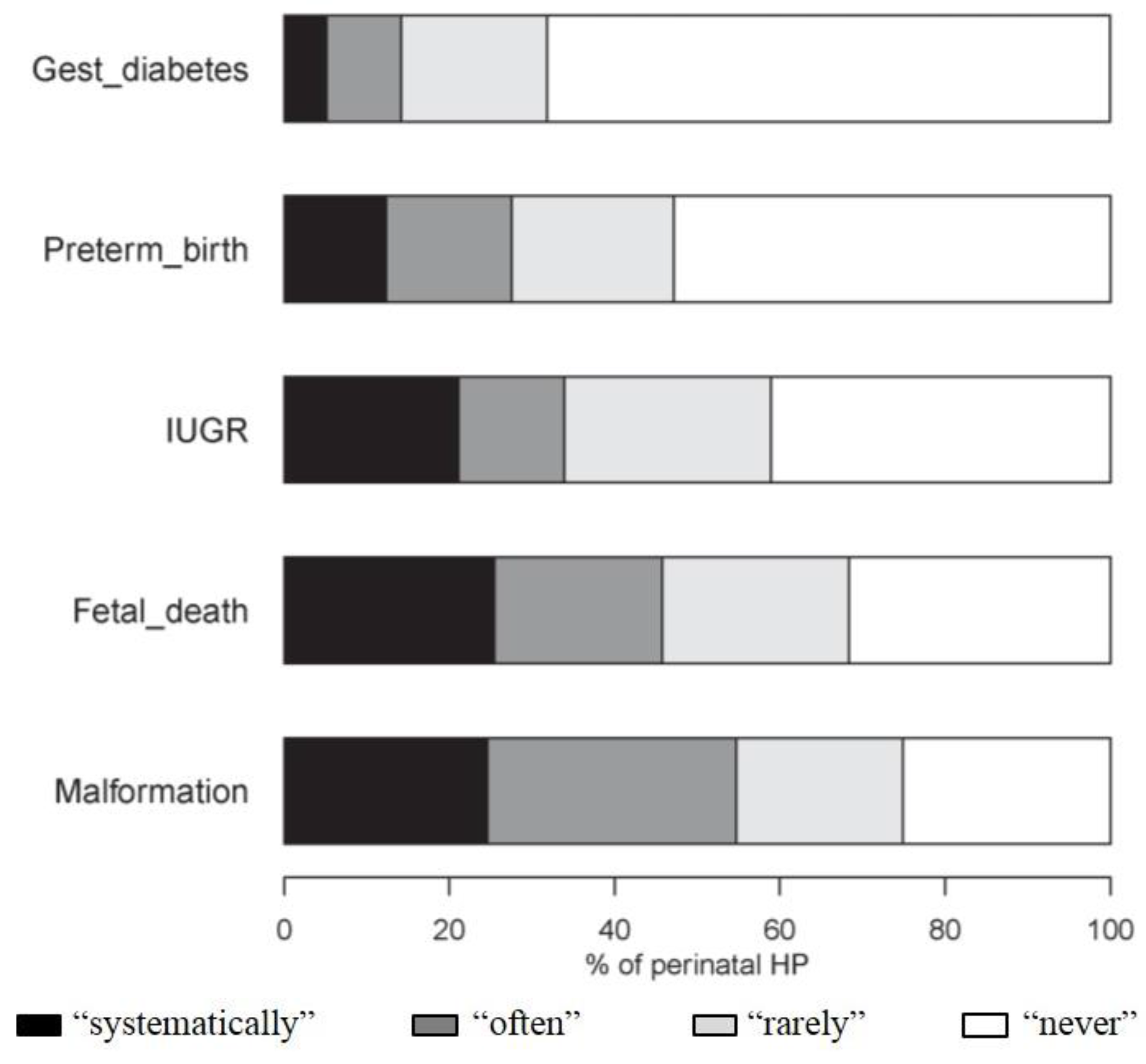
3.3. Attitude of Perinatal HPs about Chemical Exposure of Pregnant Women
3.4. Factors Limiting the Health Promotion Attitudes of Perinatal HPs in Environmental Health
4. Discussion
4.1. Perception of Environmental Risks by Perinatal HPs
4.2. Health Promotion Attitudes of Perinatal HPs
4.3. Differences of Perception According to Health Professionals
4.4. Need to Support the Involvement of Perinatal HPs in Environmental Health
4.5. Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| FIGO | International Federation of Gynecology and Obstetrics |
| GO | gynaecologist-obstetricians |
| GP | general practitioner |
| HP | health professionals |
| MW | midwife |
| PCPs | personal care products |
| PERI-HELPE study | Perception of RIsk—HEaLth Professionals & Environment Study |
References
- Di Renzo, G.C.; Conry, J.A.; Blake, J.; DeFrancesco, M.S.; DeNicola, N.; Martin, J.N., Jr.; McCue, K.A.; Richmond, D.; Shah, A.; Sutton, P.; et al. International federation of gynecology and obstetrics opinion on reproductive health impacts of exposure to toxic environmental chemicals. Int. J. Gynaecol. Obstet. 2015, 131, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Ejaredar, M.; Nyanza, E.C.; Ten Eycke, K.; Dewey, D. Phthalate exposure and childrens neurodevelopment: A systematic review. Environ. Res. 2015, 142, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Grandjean, P.; Weihe, P.; White, R.F.; Debes, F.; Araki, S.; Yokoyama, K.; Murata, K.; Sørensen, N.; Dahl, R.; Jørgensen, P.J. Cognitive deficit in 7-year-old children with prenatal exposure to methylmercury. Neurotoxicol. Teratol. 1997, 19, 417–428. [Google Scholar] [CrossRef]
- Marie, C.; Vendittelli, F.; Sauvant-Rochat, M.P. Obstetrical outcomes and biomarkers to assess exposure to phthalates: A review. Environ. Int. 2015, 83, 116–136. [Google Scholar] [CrossRef] [PubMed]
- Diamanti-Kandarakis, E.; Bourguignon, J.P.; Giudice, L.C.; Hauser, R.; Prins, G.S.; Soto, A.M.; Zoeller, R.T.; Gore, A.C. Endocrine-disrupting chemicals: An Endocrine Society scientific statement. Endocr. Rev. 2009, 30, 293–342. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Parker, J.; Bell, M.L.; Bonzini, M.; Brauer, M.; Darrow, L.A.; Gehring, U.; Glinianaia, S.V.; Gouveia, N.; Ha, E.H.; et al. Maternal exposure to particulate air pollution and term birth weight: A multi-country evaluation of effect and heterogeneity. Environ. Health Perspect. 2013, 121, 267–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Washino, N.; Saijo, Y.; Sasaki, S.; Kato, S.; Ban, S.; Konishi, K.; Ito, R.; Nakata, A.; Iwasaki, Y.; Saito, K.; et al. Correlations between prenatal exposure to perfluorinated chemicals and reduced fetal growth. Environ. Health Perspect. 2009, 117, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Rauh, V.; Arunajadai, S.; Horton, M.; Perera, F.; Hoepner, L.; Barr, D.B.; Whyatt, R. Seven-year neurodevelopmental scores and prenatal exposure to chlorpyrifos, a common agricultural pesticide. Environ. Health Perspect. 2011, 119, 1196–1201. [Google Scholar] [CrossRef] [PubMed]
- Karakis, I.; Landau, D.; Yitshak-Sade, M.; Hershkovitz, R.; Rotenberg, M.; Sarov, B.; Grotto, I.; Novack, L. Exposure to metals and congenital anomalies: A biomonitoring study of pregnant Bedouin-Arab women. Sci. Total Environ. 2015, 517, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Sathyanarayana, S.; Focareta, J.; Dailey, T.; Buchanan, S. Environmental exposures: How to counsel preconception and prenatal patients in the clinical setting. Am. J. Obstet. Gynecol. 2012, 207, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Sutton, P.; Giudice, L.C.; Woodruff, T.J. Reproductive environmental health. Curr. Opin. Obstet. Gynecol. 2010, 22, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Haruty, B.; Friedman, J.; Hopp, S.; Daniels, R.; Pregler, J. Reproductive health and the environment: Counseling patients about risks. Clevel. Clin. J. Med. 2016, 83, 367–372. [Google Scholar]
- McDiarmid, M.A.; Gehle, K. Preconception brief: Occupational/environmental exposures. Matern. Child Health J. 2006, 10, S123–S128. [Google Scholar] [CrossRef] [PubMed]
- Grason, H.A.; Misra, D.P. Reducing exposure to environmental toxicants before birth: Moving from risk perception to risk reduction. Public Health Rep. 2009, 124, 629–641. [Google Scholar] [PubMed]
- Kasemsup, R.; Neesanan, N. Knowledge, attitudes and practices relating to plastic containers for food and drinks. J. Med. Assoc. Thail. 2011, 94, S121–S125. [Google Scholar]
- Ménard, C.; Léon, C.; Benmarhnia, T. Médecins Généralistes et Sante Environnement. In Evolutions; Institut National de Prévention et d’Education Pour la Santé (INPES), 2013; 26, pp. 1–6. Available online: http://inpes.santepubliquefrance.fr/CFESBases/catalogue/detaildoc.asp?numfiche=1402 (accessed on 23 June 2016). [Google Scholar]
- Stevens, E.; Cullinan, P.; Colvile, R. Urban air pollution and children’s asthma: What do parents and health professionals think? Pediatr. Pulmonol. 2004, 37, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Stotland, N.E.; Sutton, P.; Trowbridge, J.; Atchley, D.S.; Conry, J.; Trasande, L.; Gerbert, B.; Charlesworth, A.; Woodruff, T.J. Counseling patients on preventing prenatal environmental exposures—A mixed-methods study of obstetricians. PLoS ONE 2014, 9, e98771. [Google Scholar] [CrossRef] [PubMed]
- Haute Autorité de Santé (HAS). Comment Mieux Informer Les Femmes Enceintes? Recommandations Pour Les Professionnels de Santé. 2005. Available online: http://www.has-sante.fr/portail/jcms/c_454394/fr/comment-mieux-informer-les-femmes-enceintes (accessed on 23 June 2016).
- Agence Régionale de Santé Auvergne. Résultats de l’enquête sur la perception du risque radon pour les médecins libéraux d’Auvergne. 2011. Available online: http://www.bdsp.ehesp.fr/Base/450977/ (accessed on 23 October 2016).
- Braun, J.M.; Just, A.C.; Williams, P.L.; Smith, K.W.; Calafat, A.M.; Hauser, R. Personal care product use and urinary phthalate metabolite and paraben concentrations during pregnancy among women from a fertility clinic. J. Expo. Sci. Environ. Epidemiol. 2014, 24, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Calafat, A.M.; Wong, L.Y.; Ye, X.; Reidy, J.A.; Needham, L.L. Concentrations of the sunscreen agent benzophenone-3 in residents of the United States: National Health and Nutrition Examination Survey 2003–2004. Environ. Health Perspect. 2008, 116, 893–897. [Google Scholar] [CrossRef] [PubMed]
- Den Hond, E.; Paulussen, M.; Geens, T.; Bruckers, L.; Baeyens, W.; David, F.; Dumont, E.; Loots, I.; Morrens, B.; de Bellevaux, B.N.; et al. Biomarkers of human exposure to personal care products: Results from the Flemish Environment and Health Study (FLEHS 2007–2011). Sci. Total Environ. 2013, 463–464, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Mendelsohn, E.; Hagopian, A.; Hoffman, K.; Butt, C.M.; Lorenzo, A.; Congleton, J.; Webster, T.F.; Stapleton, H.M. Nail polish as a source of exposure to triphenyl phosphate. Environ. Int. 2016, 86, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Philippat, C.; Bennett, D.; Calafat, A.M.; Picciotto, I.H. Exposure to select phthalates and phenols through use of personal care products among Californian adults and their children. Environ. Res. 2015, 140, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Rudel, R.A.; Gray, J.M.; Engel, C.L.; Rawsthorne, T.W.; Dodson, R.E.; Ackerman, J.M.; Rizzo, J.; Nudelman, J.L.; Brody, J.G. Food packaging and bisphenol A and bis(2-ethyhexyl) phthalate exposure: Findings from a dietary intervention. Environ. Health Perspect. 2011, 119, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Mertz, C.K.; Slovic, P.; Purchase, I.F. Judgments of chemical risks: Comparisons among senior managers, toxicologists, and the public. Risk Anal. 1998, 18, 391–404. [Google Scholar] [CrossRef] [PubMed]
- Blondel, B.; Kermarrec, M. Enquête Nationale Périnatale 2010. In Les Naissances en 2010 et Leur Évolution Depuis 2003; Institut National de la Santé et de la Recherche Médicale (INSERM): Paris, France, 2011. Available online: http://www.sante.gouv.fr/IMG/pdf/Les_naissances_en_2010_et leur_evolution_depuis_2003.pdf (accessed on 19 October 2016). [Google Scholar]
- Röske, K.; Hannöver, W.; Thyrian, J.R.; John, U.; Hannich, H.J. Smoking cessation counselling for pregnant and postpartum women among midwives, gynaecologists and paediatricians in Germany. Int. J. Environ. Res. Public Health 2009, 6, 96–107. [Google Scholar] [CrossRef] [PubMed]
- Institut National de Prévention et d’Education Pour la Santé (INPES). Guide de la Pollution de l’air Intérieur 2009. Available online: http://inpes.santepubliquefrance.fr/30000/actus2009/014.asp (accessed on 20 September 2016).
- Danish Ministry of the Environment. Expecting a Baby? Advice about Chemicals and Pregnancy. 2012. Available online: http://www.wecf.eu/english/articles/2012/04/broshure-expecting-a-baby.php (accessed on 19 June 2016).
- Gérardin, M.; Victorri-Vigneau, C.; Louvigné, C.; Rivoal, M.; Jolliet, P. Management of cannabis use during pregnancy: An assessment of healthcare professionals’ practices. Pharmacoepidemiol. Drug Saf. 2011, 20, 464–473. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Ashley, J.M.; Hodgson, A.; Nisker, J. Views of pregnant women and clinicians regarding discussion of exposure to phthalate plasticizers. Reprod. Health 2014, 11, 47. [Google Scholar] [CrossRef] [PubMed]
- Dunkley, J. Training midwives to help pregnant women stop smoking. Nurs. Times 1997, 93, 64–66. [Google Scholar] [PubMed]
- Chamberlain, C.; O’Mara-Eves, A.; Oliver, S.; Caird, J.R.; Perlen, S.M.; Eades, S.J.; Thomas, J. Psychosocial interventions for supporting women to stop smoking in pregnancy. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Csajka, C.; Jaquet, A.; Winterfeld, U.; Meyer, Y.; Einarson, A.; Panchaud, A. Risk perception by healthcare professionals related to drug use during pregnancy: A Swiss survey. Swiss Med. Wkly. 2014, 144, w13936. [Google Scholar] [CrossRef] [PubMed]
- De Ruddere, L.; Goubert, L.; Stevens, M.A.L.; Deveugele, M.; Craig, K.D.; Crombez, G. Health care professionals’ reactions to patient pain: Impact of knowledge about medical evidence and psychosocial influences. J. Pain 2014, 15, 262–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saylor, A.; Prokopy, L.S.; Amberg, S. What’s wrong with the tap? Examining perceptions of tap water and bottled water at Purdue University. Environ. Manag. 2011, 48, 588–601. [Google Scholar] [CrossRef] [PubMed]
- Berg-Beckhoff, G.; Breckenkamp, J.; Larsen, P.V.; Kowall, B. General practitioners’ knowledge and concern about electromagnetic fields. Int. J. Environ. Res. Public Health 2014, 11, 12969–12982. [Google Scholar] [CrossRef] [PubMed]
- Direction de la Recherche, des Études, de L’évaluation et des Statistiques (DREES). Les Médecins au 1er Janvier 2013; Série Statistiques; DREES: Paris, France, 2013. Available online: http://drees.social-sante.gouv.fr/etudes-et-statistiques/publications/documents-de-travail/serie-statistiques/article/les-medecins-au-1er-janvier-2013 (accessed on 3 November 2016).
- Direction de la Recherche, des Études, de L’évaluation et des Statistiques (DREES). La Profession de Sage-Femme: Constat Démographique et Projections D’effectifs; Etudes et résultats; DREES: Paris, France, 2013.
- Tourangeau, R.; Yan, T. Sensitive questions in surveys. Psychol. Bull. 2007, 133, 859–883. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total n = 189 (%) | GP a n = 50 (26.5%) | GO a n = 32 (16.9%) | MW a n = 107 (56.6%) | p-Value | |
|---|---|---|---|---|---|
| Sex | n = 188 | n = 50 | n = 32 | n = 106 | |
| Female | 164 (87.2) | 37 (74.0) | 21 (65.6) | 106 (100.0) | <0.001 |
| Male | 24 (12.8) | 13 (26.0) | 11 (34.4) | 0 | |
| Age (years) | n = 188 | n = 50 | n = 32 | n = 106 | |
| <45 years | 135 (71.8) | 35 (70.0) | 22 (68.8) | 78 (73.6) | 0.82 |
| ≥45 years | 53 (28.2) | 15 (30.0) | 28 (31.2) | 63 (26.4) | |
| Parity | n = 182 | n = 47 | n = 31 | n = 104 | |
| ≥1 | 120 (65.9) | 24 (51.1) | 26 (83.9) | 70 (67.3) | 0.01 |
| Occupational status | n = 189 | n = 50 | n = 32 | n = 107 | |
| Resident/mid-wife’s student | 49 (25.9) | 26 (52.0) | 3 (9.4) | 20 (18.7) | <0.001 |
| Senior | 140 (74.1) | 24 (48.0) | 29 (90.6) | 87 (81.3) | |
| Length of service | n = 155 | n = 39 | n = 29 | n = 87 | |
| ≤10 years | 80 (51.6) | 23 (59.0) | 18 (62.1) | 39 (44.8) | 0.16 |
| >10 years | 75 (48.4) | 16 (41.0) | 11 (37.9) | 48 (55.2) | |
| Place of work b | n = 189 | n = 50 | n = 32 | n = 107 | |
| Private practice | 63 (33.3) | 38 (76.0) | 5 (15.6) | 20 (18.7) | <0.001 |
| Private health institution | 3 (1.6) | 1 (2.0) | 1 (3.1) | 1 (0.9) | 0.40 |
| Public health institution | 112 (59.3) | 11 (22.0) | 26 (81.3) | 75 (70.1) | <0.001 |
| Contact with pregnant women | n = 183 | n = 48 | n = 32 | n = 103 | |
| Consultation | 52 (28.4) | 36 (75.0) | 8 (25.0) | 8 (7.8) | <0.001 |
| Hospital | 17 (9.3) | 1 (2.1) | 2 (6.2) | 14 (13.6) | |
| Both | 91 (49.7) | 11 (22.9) | 22 (68.8) | 58 (56.3) | |
| Others c | 23 (12.6) | 0 | 0 | 23 (22.3) |
| Number of Respondents a | Number (%) of Perinatal HPs Perceiving a “Very high” or “High” Risk b | |||||
|---|---|---|---|---|---|---|
| n = 189 | Total n (%) | GP c n (%) | GO c n (%) | MW c n (%) | p-Value | |
| Pesticides | 184 | 167 (90.8) | 45 (93.8) | 26 (81.3) | 96 (92.3) | 0.12 |
| Carbon monoxide | 186 | 167 (89.8) | 41 (85.4) | 26 (81.3) | 100 (94.3) | 0.05 |
| Phthalates | 140 | 124 (88.6) | 28 (87.5) | 17 (77.3) | 79 (91.9) | 0.15 |
| Lead | 184 | 155 (84.2) | 39 (81.3) | 25 (80.7) | 91 (86.7) | 0.58 |
| Bisphenol A | 170 | 141 (82.9) | 34 (79.1) | 20 (69.0) | 87 (88.8) | 0.03 |
| Legionella | 180 | 135 (75.0) | 39 (79.6) | 10 (33.3) | 86 (85.2) | <0.001 |
| Outdoor air pollution | 184 | 131 (71.2) | 31 (64.6) | 19 (59.4) | 82 (77.9) | 0.06 |
| Parabens | 170 | 121 (71.2) | 32 (71.1) | 14 (50.0) | 75 (77.3) | 0.02 |
| Asbestos | 176 | 125 (71.0) | 28 (57.1) | 16 (57.1) | 81 (81.8) | 0.002 |
| Indoor air pollution | 178 | 123 (69.1) | 32 (66.7) | 14 (48.3) | 77 (76.2) | 0.02 |
| Waste incinerator | 163 | 106 (65.0) | 29 (63.0) | 15 (53.6) | 62 (69.7) | 0.28 |
| Use of consumer products d | 180 | 112 (62.2) | 29 (61.7) | 13 (40.6) | 70 (69.3) | 0.01 |
| Soil pollution | 177 | 109 (61.6) | 26 (54.2) | 13 (44.8) | 70 (70.0) | 0.02 |
| Food risk | 184 | 104 (56.5) | 24 (50.0) | 9 (28.1) | 71 (68.3) | <0.001 |
| Electromagnetic waves e | 160 | 86 (53.8) | 13 (34.2) | 7 (25.0) | 66 (70.2) | <0.001 |
| Radon | 131 | 65 (49.6) | 16 (37.2) | 3 (14.3) | 46 (68.7) | <0.001 |
| Tap water quality | 182 | 83 (45.6) | 16 (33.3) | 8 (25.0) | 59 (57.8) | <0.001 |
| Use of PCPs | 179 | 66 (36.9) | 14 (39.8) | 2 (6.7) | 50 (49.0) | <0.001 |
| Noise | 180 | 58 (32.2) | 16 (33.3) | 7 (21.9) | 35 (35.0) | 0.38 |
| Total n = 189 (%) | GP a n = 50 (%) | GO a n = 32 (%) | MW a n = 107 (%) | p-Value | |
|---|---|---|---|---|---|
| Declared level of EH knowledge | |||||
| Environmental contaminants | n = 189 | n = 50 | n = 32 | n = 107 | |
| “Well informed” b | 38 (20.1) | 11 (22.0) | 3 (9.4) | 24 (22.4) | 0.39 |
| “Poorly informed” | 125 (66.1) | 30 (60.0) | 24 (75.0) | 71 (66.4) | |
| “Very poorly informed” | 26 (13.8) | 9 (18.0) | 5 (15.6) | 12 (11.2) | |
| Health outcomes | n = 188 | n = 49 | n = 32 | n = 107 | |
| “Well informed” b | 34 (18.1) | 12 (24.5) | 6 (18.8) | 16 (15.0) | 0.57 |
| “Poorly informed” | 117 (62.2) | 29 (57.1) | 18 (56.3) | 71 (66.4) | |
| “Very poorly informed” | 37 (19.7) | 9 (18.4) | 8 (25.0) | 20 (18.7) | |
| Training in EH (“Yes”) c | n = 189 | n = 50 | n = 32 | n = 107 | |
| 11 (5.8) | 2 (4.0) | 1 (3.1) | 8 (7.5) | 0.36 | |
| Desire training in EH (“Yes”) | n = 186 | n = 50 | n = 32 | n = 104 | |
| 142 (76.3) | 38 (76.0) | 22 (68.8) | 82 (78.9) | 0.50 | |
| Sources of information about EH | n = 189 | n = 50 | n = 32 | n = 107 | |
| Media, Internet | 154 (81.5) | 35 (70.0) | 25 (78.1) | 94 (87.9) | 0.02 |
| Scientific article | 109 (57.7) | 31 (62.0) | 17 (53.1) | 61 (57.0) | 0.71 |
| Health agency or institution | 40 (21.1) | 15 (30.0) | 2 (6.3) | 23 (21.5) | 0.04 |
| Environmental association | 37 (19.6) | 11 (22.0) | 5 (15.6) | 21 (19.6) | 0.78 |
| Other health professionals | 28 (14.8) | 5 (10.0) | 4 (12.5) | 19 (17.8) | 0.41 |
| Other source | 10 (5.3) | 4 (8.0) | 2 (6.3) | 4 (3.7) | 0.49 |
| Difficulties | n = 189 | n = 50 | n = 32 | n = 107 | |
| Lack of knowledge | 110 (58.2) | 27 (54.0) | 15 (46.9) | 68 (63.6) | 0.19 |
| Insufficient/contradictory scientific evidence | 103 (54.5) | 28 (56.0) | 20 (62.5) | 55 (51.4) | 0.53 |
| Lack of time during consultation | 95 (50.3) | 23 (46.0) | 15 (46.9) | 57 (53.2) | 0.64 |
| Lack of interest of women | 66 (34.9) | 14 (28.0) | 12 (37.5) | 40 (37.4) | 0.49 |
| Low contribution of environmental factor to disorder | 48 (25.4) | 13 (26.0) | 18 (56.3) | 17 (15.9) | <0.001 |
| Contact with women too late in pregnancy | 38 (20.1) | 5 (10.0) | 5 (15.6) | 28 (26.2) | 0.05 |
| Lack of interest | 16 (8.5) | 6 (12.0) | 2 (6.3) | 8 (7.5) | 0.56 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marie, C.; Lémery, D.; Vendittelli, F.; Sauvant-Rochat, M.-P. Perception of Environmental Risks and Health Promotion Attitudes of French Perinatal Health Professionals. Int. J. Environ. Res. Public Health 2016, 13, 1255. https://doi.org/10.3390/ijerph13121255
Marie C, Lémery D, Vendittelli F, Sauvant-Rochat M-P. Perception of Environmental Risks and Health Promotion Attitudes of French Perinatal Health Professionals. International Journal of Environmental Research and Public Health. 2016; 13(12):1255. https://doi.org/10.3390/ijerph13121255
Chicago/Turabian StyleMarie, Cécile, Didier Lémery, Françoise Vendittelli, and Marie-Pierre Sauvant-Rochat. 2016. "Perception of Environmental Risks and Health Promotion Attitudes of French Perinatal Health Professionals" International Journal of Environmental Research and Public Health 13, no. 12: 1255. https://doi.org/10.3390/ijerph13121255