
Association between Floods and Acute Cardiovascular Diseases: A Population-Based Cohort Study Using a Geographic Information System Approach


Abstract
:1. Introduction
2. Methods
2.1. Design
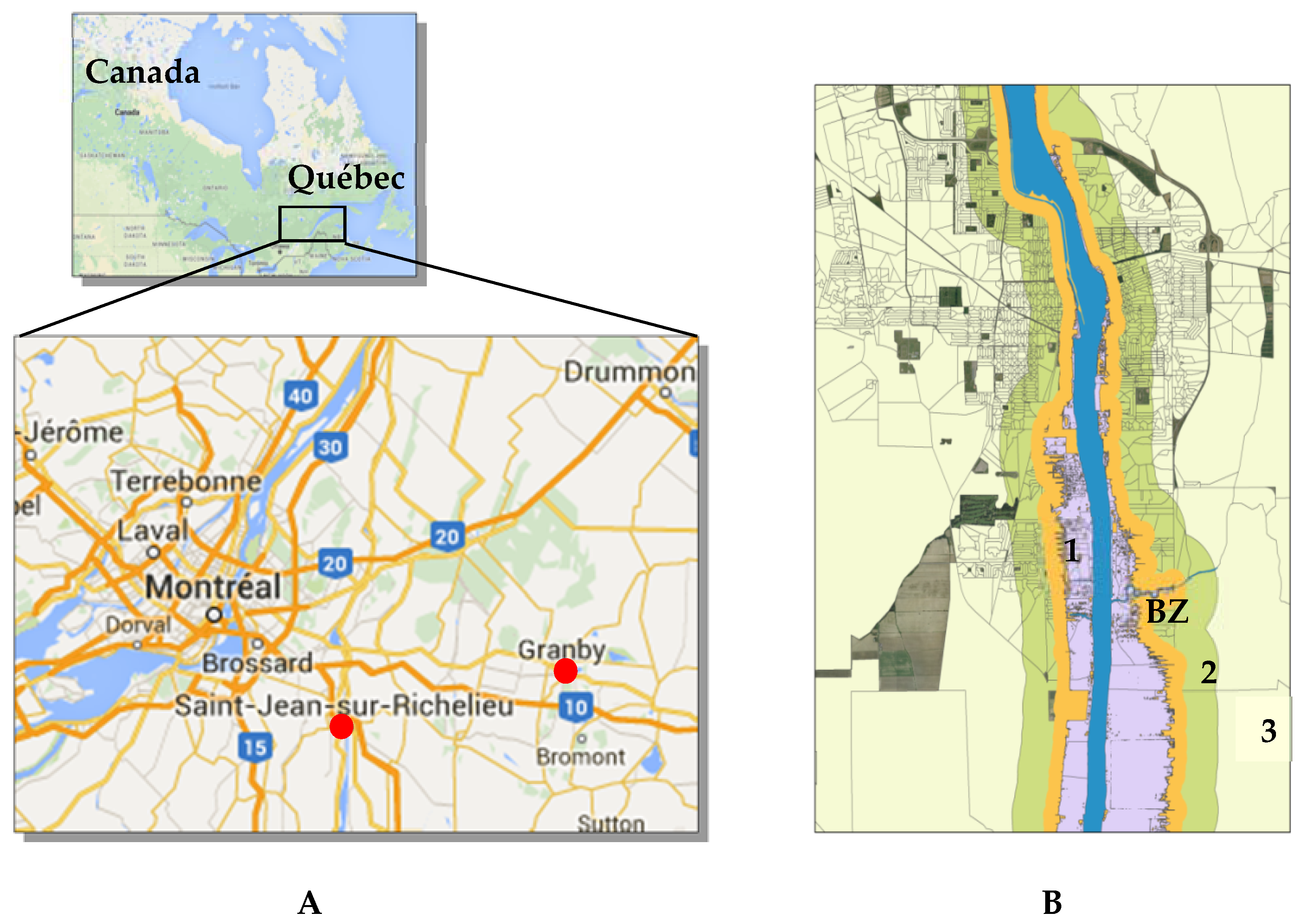
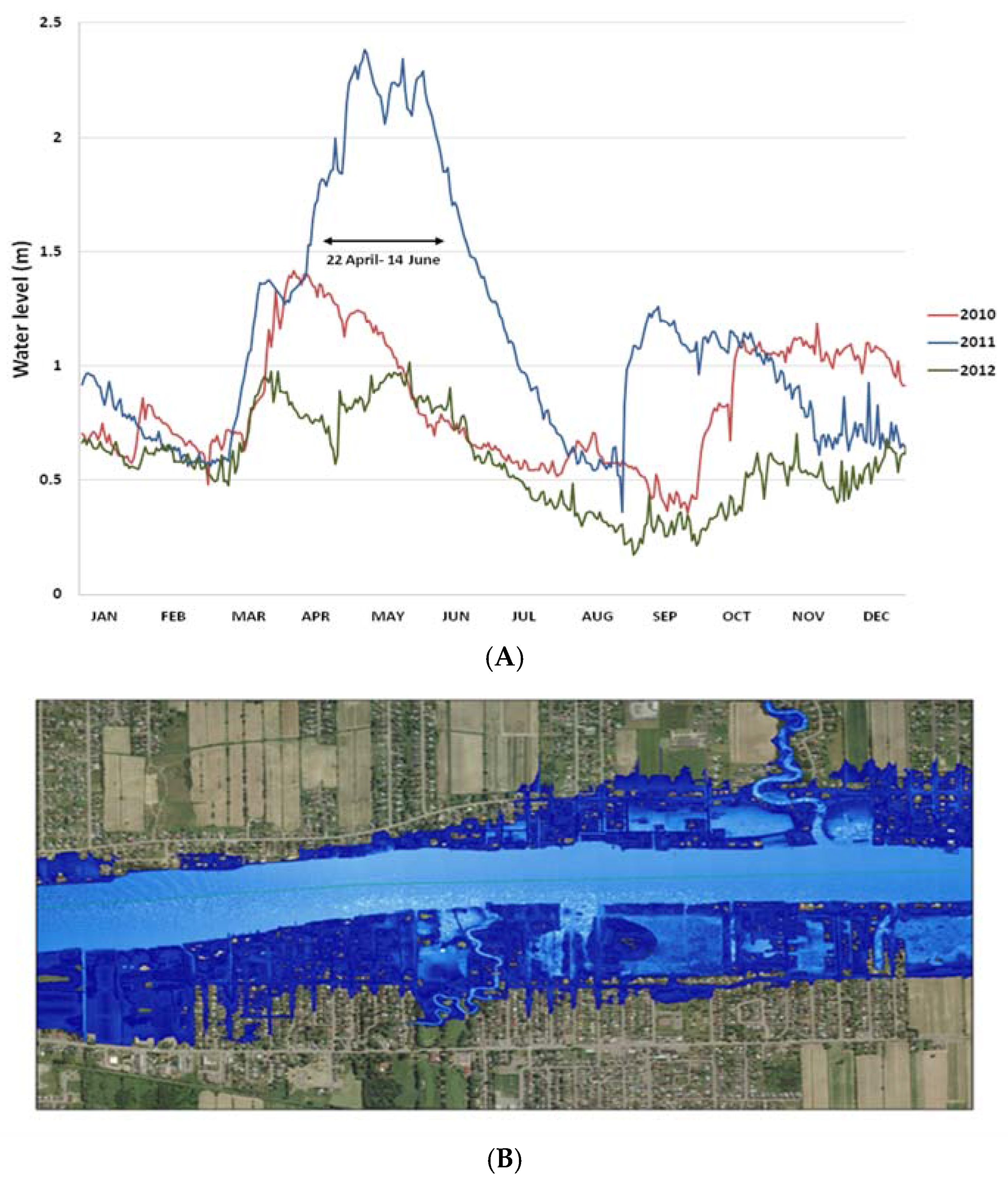
Defining the Study Areas Using a Geographic Information System (GIS) Approach


2.2. Health Data Sources
2.3. Study Population
2.4. Cardiovascular Outcomes
2.5. Confounders
2.6. Statistical Analysis
2.7. Ethical Aspects
3. Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Flooded Area | Control Areas | p-Value | ||
|---|---|---|---|---|---|
| Area 1 | Area 2 | Area 3 | Area 4 | ||
| n | 10,081 | 22,654 | 40,119 | 38,463 | |
| Male sex, n (%) | 5168 (51.3%) | 10,874 (48.0%) | 19,402 (48.4%) | 18,270 (47.5%) | <0.001 |
| Age (year), mean ± SD | 49.6 ± 16.6 | 49.1 ± 17.7 | 48.5 ± 17.3 | 51.7 ± 18.3 | <0.001 |
| Comorbidity score, n (%) | |||||
| 0 | 9154 (90.8%) | 20,325 (89.7%) | 36,377 (90.7%) | 33,844 (88.0%) | <0.001 |
| 1 | 760 (7.5%) | 1843 (8.1%) | 2995 (7.4%) | 3625 (9.4%) | |
| ≥2 | 167 (1.7%) | 486 (2.2%) | 747 (1.9%) | 994 (2.6%) | |
| Mental disorders, n (%) | 548 (5.4%) | 1546 (6.8%) | 2334 (5.8%) | 2243 (5.8%) | <0.001 |
| Diabetes, n (%) | 790 (7.8%) | 2041 (9.0%) | 3221 (8.0%) | 3792 (9.9%) | <0.001 |
| Hypertension, n (%) | 2328 (23.1%) | 5475 (24.2%) | 9282 (23.1%) | 9989 (26.0%) | <0.001 |
| History of CVD, n (%) | 1021 (10.1%) | 2620 (11.6%) | 4170 (10.4%) | 4906 (12.8%) | <0.001 |
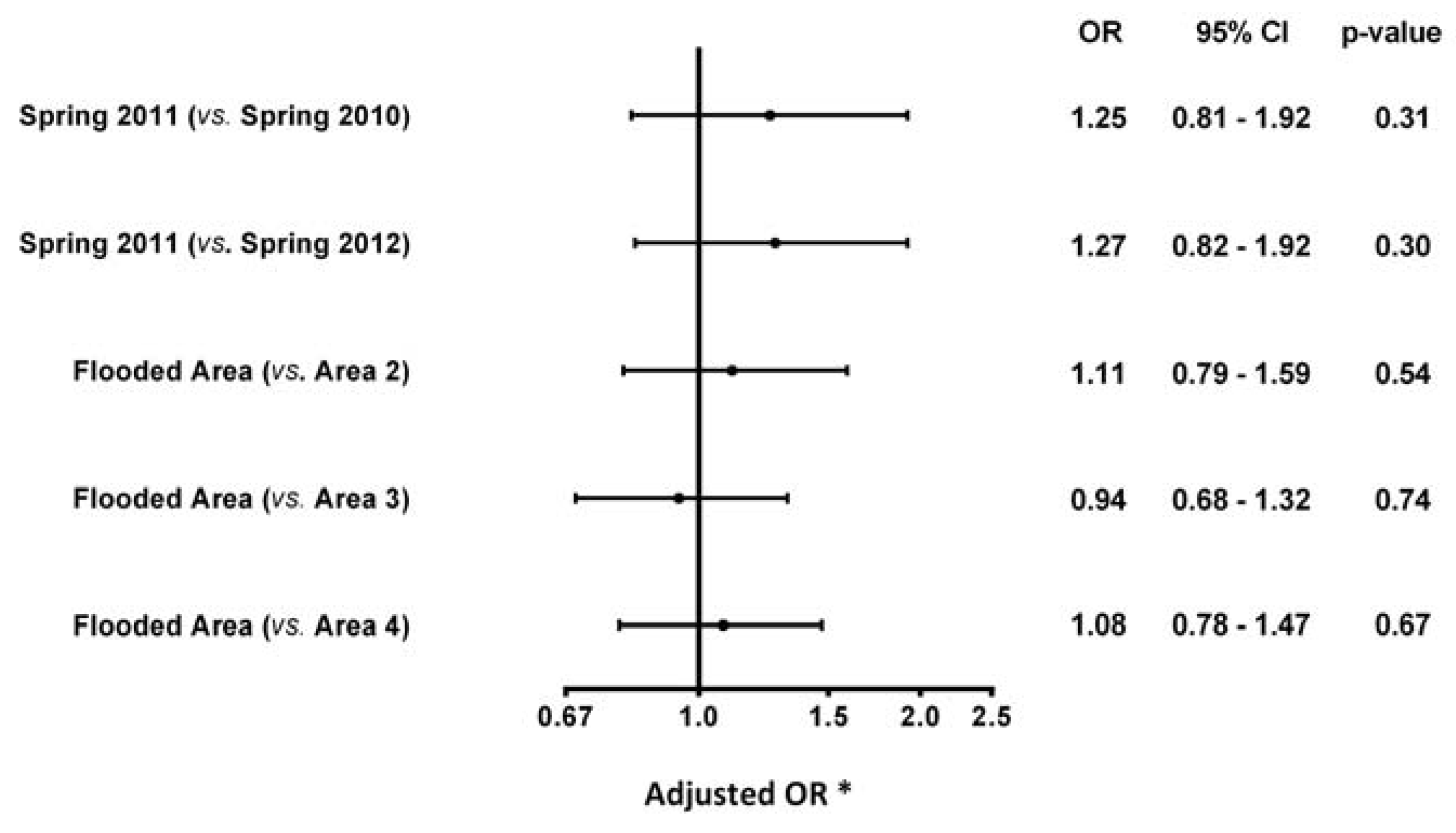
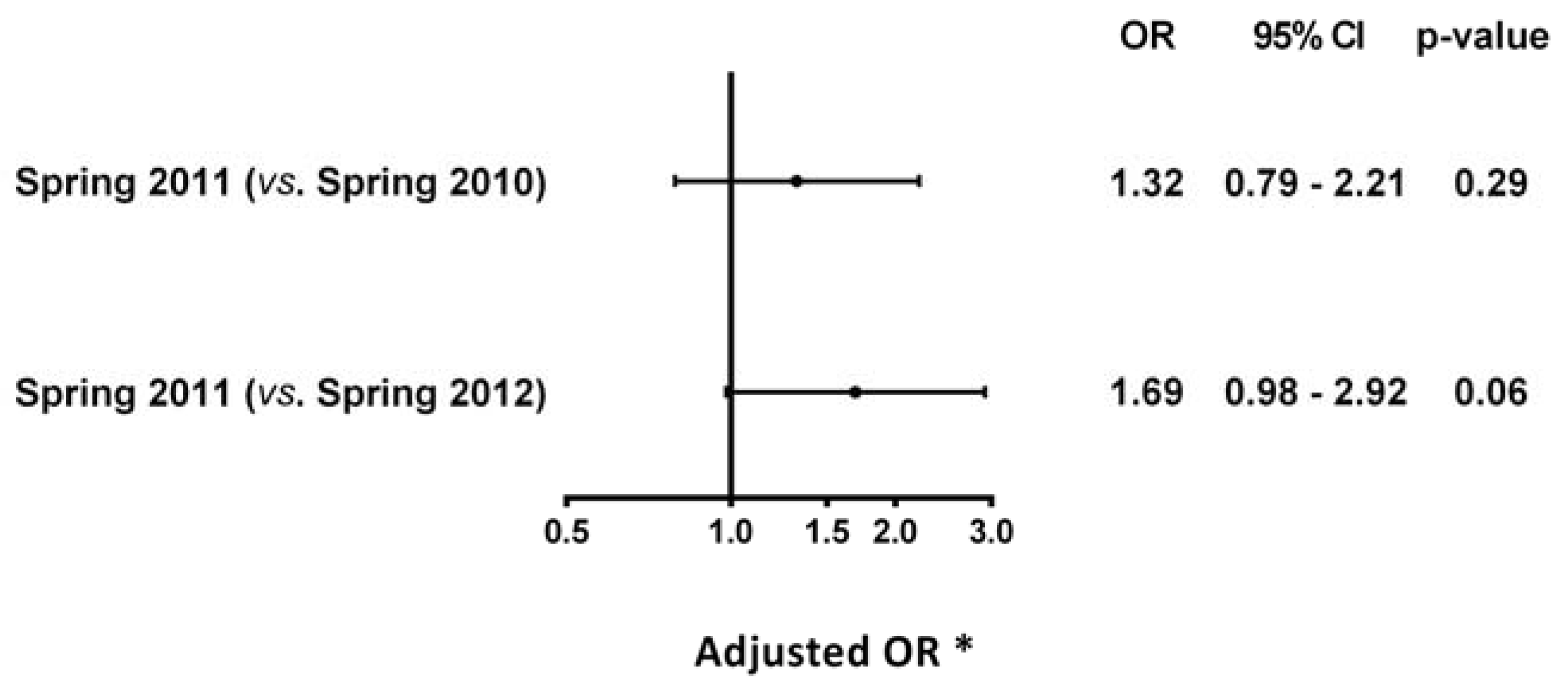
3.1. Flooded Area in Spring 2011 vs. Spring 2010 and Spring 2012
| Areas | Spring 2010; n (%) | Spring 2011; n (%) | Spring 2012; n (%) |
|---|---|---|---|
| Flooded Area | 37/10,006 (0.37%) | 47/10,081 (0.47%) | 38/10,128 (0.38%) |
| Area 2 | 122/22,456 (0.54%) | 113/22,654 (0.50%) | 121/22,789 (0.53%) |
| Area 3 | 220/39,807 (0.55%) | 208/40,119 (0.52%) | 193/40,408 (0.48%) |
| Area 4 | 207/38,162 (0.54%) | 230/38,463 (0.60%) | 234/38,517 (0.61%) |


3.2. Flooded Area (Area 1) vs. Control Areas (Areas 2, 3 and 4) in Spring 2011
4. Discussion
5. Strengths and Limitations
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Working group II. Intergovernmental Panel on Climat Change. Climat Change 2001: Impacts, Adaptation, and Vulnerability. 2001. Available online: http://www.preventionweb.net/files/8387_wg2TARfrontmatter1.pdf. (accessed on 11 June 2015).
- Sandink, D.; Kovacs, P.; Oulahen, G.; McGillivray, G. Making Flood Insurable for Canadian Homeowners: A Discussion Paper. 2010. Available online: http://www.iclr.org/images/Making_Flood_Insurable_for_Canada.pdf (accessed on 16 September 2015).
- Ouranos Vers, L’adaptation. Synthèse Des Connaissances Sur Les Changements Climatiques Au Québec. Partie 1: Évolution Climatique Au Québec. Available online: http://www.ouranos.ca/fr/synthese2014/doc/Partie_I.pdf (accessed on 3 October 2015).
- Alderman, K.; Turner, L.R.; Tong, S. Floods and human health: A systematic review. Environ. Int. 2012, 47, 37–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization Regional Office for Europe. Floods: Climate Change and Adaptation Strategies for Human Health. 2002. Available online: http://www.euro.who.int/__data/assets/pdf_file/0007/74734/E77096.pdf (accessed on 3 October 2015).
- Ahern, M.; Kovats, R.S.; Wilkinson, P.; Few, R.; Matthies, F. Global health impacts of floods: Epidemiologic evidence. Epidemiol. Rev. 2005, 27, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Few, R.; Ahern, M.; Matthies, F.; Kovats, S. Floods, Health and Climate Change : A Strategic Review. Available online: http://www.tyndall.ac.uk/sites/default/files/wp63.pdf (accessed on 3 October 2015).
- Chen, W.K.; Cheng, Y.C.; Ng, K.C.; Hung, J.J.; Chuang, C.M. Were there enough physicians in an emergency department in the affected area after a major earthquake? An analysis of the Taiwan Chi-Chi earthquake in 1999. Ann. Emerg. Med. 2001, 38, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.Y.; Wu, C.C.; Liu, Y.B.; Ho, Y.L.; Liau, C.S.; Lee, Y.T. Derangement of heart rate variability during a catastrophic earthquake: A possible mechanism for increased heart attacks. Pacing Clin. Electrophysiol. 2001, 24, 1596–1601. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Tanaka, F.; Nakajima, S.; Honma, M.; Sakai, T.; Kawakami, M.; Endo, H.; Onodera, M.; Niiyama, M.; Komatsu, T.; et al. Comparison of the Incidence of Acute Decompensated Heart Failure Before and After the Major Tsunami in Northeast Japan. Am. J. Cardiol. 2012, 110, 1856–1860. [Google Scholar] [CrossRef] [PubMed]
- Canadian Best Practices Portal—CBPP: Cardiovascular Disease. Available online: http://cbpp-pcpe.phac-aspc.gc.ca/chronic-diseases/cardiovascular-diseases/ (accessed on 11 June 2015).
- Environment Canada. Flooding Events in Canada. Available online: https://ec.gc.ca/eau-water/default.asp?lang=En&n=C0122DA3-1 (accessed on 16 September 2015).
- Environnement Canada: ARCHIVÉE—Inondations du Richelieu: La Plus Longue Catastrophe au Québec—Conditions Atmosphériques et Météorologie. Available online: http://www.ec.gc.ca/meteo-weather/default.asp?lang=Fr&n=D7CF8BE3-1 (accessed on 5 October 2015).
- Organisation de la sécurité civile du Québec. Rapport D’événements: Inondations Printanières, Montégérie 2011. 2013. Available online: http://www.securitepublique.gouv.qc.ca/fileadmin/Documents/securite_civile/inondations_monteregie_2011/rapport_evenement_inondations_monteregie.pdf (accessed on 5 October 2015). [Google Scholar]
- Canadian Disaster Database. Available online: http://bdc.securitepublique.gc.ca/dtpg-eng.aspx?cultureCode=en-Ca&provinces=11&eventTypes=%27FL%27&eventStartDate=%2720110101%27%2c%2720111231%27&normalizedCostYear=1&eventId=1010 (accessed on 16 September 2015).
- Lyseen, A.K.; Nøhr, C.; Sørensen, E.M.; Gudes, O.; Geraghty, E.M.; Shaw, N.T.; Bivona-Tellez, C.; IMIA Health GIS Working Group. A Review and Framework for Categorizing Current Research and Development in Health Related Geographical Information Systems (GIS) Studies. Yearb. Med. Inform. 2014, 9, 110–124. [Google Scholar] [CrossRef] [PubMed]
- Environment Canada: HYDAT Database. Available online: https://ec.gc.ca/rhc-wsc/default.asp?lang=En&n=9018B5EC-1 (accessed on 5 October 2015).
- Environnement Canada: Recherche de Données Hydrométriques Historiques. Available online: http://eau.ec.gc.ca/search/search_f.html?sType=h2oArc (accessed on 11 June 2015).
- Blais, C.; Jean, S.; Sirois, C.; Rochette, L.; Plante, C.; Larocque, I.; Doucet, M.; Ruel, G.; Simard, M.; Gamache, P.; et al. Quebec Integrated Chronic Disease Surveillance System (QICDSS), an innovative approach. Chronic Dis. Inj. Can. 2014, 34, 226–235. [Google Scholar] [PubMed]
- RAMQ: Mission. Available online: http://www.ramq.gouv.qc.ca/en/regie/Pages/mission.aspx (accessed on 11 June 2015).
- WHO: International Classification of Diseases (ICD). Available online: http://www.who.int/classifications/icd/en/ (accessed on 11 June 2015).
- D’Hoore, W.; Bouckaert, A.; Tilquin, C. Practical considerations on the use of the Charlson comorbidity index with administrative data bases. J. Clin. Epidemiol. 1996, 49, 1429–1433. [Google Scholar] [CrossRef]
- Tu, K.; Mitiku, T.; Lee, D.S.; Guo, H.; Tu, J.V. Validation of physician billing and hospitalization data to identify patients with ischemic heart disease using data from the Electronic Medical Record Administrative data Linked Database (EMRALD). Can. J. Cardiol. 2013, 26, e225–e228. [Google Scholar] [CrossRef]
- Tu, K.; Wang, M.; Young, J.; Green, D.; Ivers, N.M.; Butt, D.; Jaakkimainen, L.; Kapral, M.K. Validity of administrative data for identifying patients who have had a stroke or transient ischemic attack using EMRALD as a reference standard. Can. J. Cardiol. 2013, 29, 1388–1394. [Google Scholar] [CrossRef] [PubMed]
- Schultz, S.E.; Rothwell, D.M.; Chen, Z.; Tu, K. Identifying cases of congestive heart failure from administrative data: A validation study using primary care patient records. Chronic. Dis. In. J. Can. 2013, 33, 160–166. [Google Scholar]
- Quan, H.; Khan, N.; Hemmelgarn, B.R.; Tu, K.; Chen, G.; Campbell, N.; Hill, M.D.; Ghali, W.A.; McAlister, F.A.; Hypertension Outcome and Surveillance Team of the Canadian Hypertension Education Programs. Validation of a Case Definition to Define Hypertension Using Administrative Data. Hypertension 2009, 54, 1423–1428. [Google Scholar] [CrossRef] [PubMed]
- Hux, J.E.; Ivis, F.; Flintoft, V.; Bica, A. Diabetes in Ontario: Determination of prevalence and incidence using a validated administrative data algorithm. Diabetes Care 2002, 25, 512–516. [Google Scholar] [CrossRef] [PubMed]
- Hanley, J.A.; Negassa, A.; Edwardes, M.D.; de Forrester, J.E. Statistical analysis of correlated data using generalized estimating equations: An orientation. Am. J. Epidemiol. 2003, 157, 364–375. [Google Scholar] [CrossRef] [PubMed]
- Comité d’éthique de santé publique. Avis du Comité d’éthique de Santé Publique, Projet de Plan Ministériel de Surveillance Multithématique. 2010. Available online: http://www.preventionweb.net/files/8387_wg2TARfrontmatter1.pdf (accessed on 26 January 2016).
- Jiao, Z.; Kakoulides, S.V.; Moscona, J.; Whittier, J.; Srivastav, S.; Delafontaine, P.; Irimpen, A. Effect of Hurricane Katrina on incidence of acute myocardial infarction in New Orleans three years after the storm. Am. J. Cardiol. 2012, 109, 502–505. [Google Scholar] [CrossRef] [PubMed]
- Aoki, T.; Fukumoto, Y.; Yasuda, S.; Sakata, Y.; Ito, K.; Takahashi, J.; Miyata, S.; Tsuji, I.; Shimokawa, H. The Great East Japan Earthquake Disaster and cardiovascular diseases. Eur. Heart J. 2012, 33, 2796–2803. [Google Scholar] [CrossRef] [PubMed]
- Tomio, J.; Sato, H.; Mizumura, H. Interruption of medication among outpatients with chronic conditions after a flood. Prehosp. Disaster Med. 2010, 25, 42–50. [Google Scholar] [PubMed]
- Rozanski, A.; Blumenthal, J.; Davidson, K.W.; Saab, P.G.; Kubzansky, L. The epidemiology, pathophysiology, and management of psychosocial risk factors in cardiac practice: The emerging field of behavioral cardiology. J. Am. Coll. Cardiol. 2005, 45, 637–651. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.C.; Jalal, S.; Khan, N.U. Posttraumatic stress disorder and psychiatric comorbidity following the 2010 flood in Pakistan: Exposure characteristics, cognitive distortions, and emotional suppression. Psychiatry 2014, 77, 289–304. [Google Scholar] [CrossRef] [PubMed]
- Auger, C.; Latour, S.; Trudel, M.; Fortin, M. Post-traumatic stress disorder. After the flood in Saguenay. Can. Fam. Physician 2000, 46, 2420–2427. [Google Scholar] [PubMed]
- Yokoyama, Y.; Otsuka, K.; Kawakami, N.; Kobayashi, S.; Ogawa, A.; Tannno, K.; Onoda, T.; Yaegashi, Y.; Sakata, K. Mental health and related factors after the Great East Japan earthquake and tsunami. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Fergusson, D.M.; Horwood, L.J.; Boden, J.M.; Mulder, R.T. Impact of a major disaster on the mental health of a well-studied cohort. JAMA Psychiatry 2014, 71, 1025–1031. [Google Scholar] [CrossRef] [PubMed]
- Malpas, S. Sympathetic nervous system overactivity and its role in the development of cardiovascular disease. Physiol. Rev. 2010, 90, 513–557. [Google Scholar] [CrossRef] [PubMed]
- Esler, M.; Kaye, D. Sympathetic nervous system activation in essential hypertension, cardiac failure and psychosomatic heart disease. J. Cardiovasc. Pharmacol. 2000, 35, S1–S7. [Google Scholar] [CrossRef] [PubMed]
- Dimsdale, J.E. Psychological stress and cardiovascular disease. J. Am. Coll. Cardiol. 2008, 51, 1237–1246. [Google Scholar] [CrossRef] [PubMed]
- Kershaw, K.N.; Brenes, G.; Charles, L.E.; Coday, M.; Daviglus, M.L.; Denburg, N.L.; Kroenke, C.H.; Safford, M.M.; Savla, T.; Tindle, H.A.; et al. Associations of Stressful Life Events and Social Strain with Incident Cardiovascular Disease in the Women’s Health Initiative. J. Am. Heart Assoc. 2014, 3. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vanasse, A.; Cohen, A.; Courteau, J.; Bergeron, P.; Dault, R.; Gosselin, P.; Blais, C.; Bélanger, D.; Rochette, L.; Chebana, F. Association between Floods and Acute Cardiovascular Diseases: A Population-Based Cohort Study Using a Geographic Information System Approach. Int. J. Environ. Res. Public Health 2016, 13, 168. https://doi.org/10.3390/ijerph13020168
Vanasse A, Cohen A, Courteau J, Bergeron P, Dault R, Gosselin P, Blais C, Bélanger D, Rochette L, Chebana F. Association between Floods and Acute Cardiovascular Diseases: A Population-Based Cohort Study Using a Geographic Information System Approach. International Journal of Environmental Research and Public Health. 2016; 13(2):168. https://doi.org/10.3390/ijerph13020168
Chicago/Turabian StyleVanasse, Alain, Alan Cohen, Josiane Courteau, Patrick Bergeron, Roxanne Dault, Pierre Gosselin, Claudia Blais, Diane Bélanger, Louis Rochette, and Fateh Chebana. 2016. "Association between Floods and Acute Cardiovascular Diseases: A Population-Based Cohort Study Using a Geographic Information System Approach" International Journal of Environmental Research and Public Health 13, no. 2: 168. https://doi.org/10.3390/ijerph13020168