
Seroprevalence of Antibodies against Measles, Rubella and Varicella among Asylum Seekers Arriving in Lower Saxony, Germany, November 2014–October 2015

Abstract
:1. Introduction
2. Materials and Methods
2.1. Microbiological Analysis
2.2. Statistical Analysis
3. Results
3.1. Descriptive Statistics
3.2. Seroprevalence
3.2.1. Sex and Age Groups
3.2.2. Countries of Origin
Measles
Rubella
Varicella
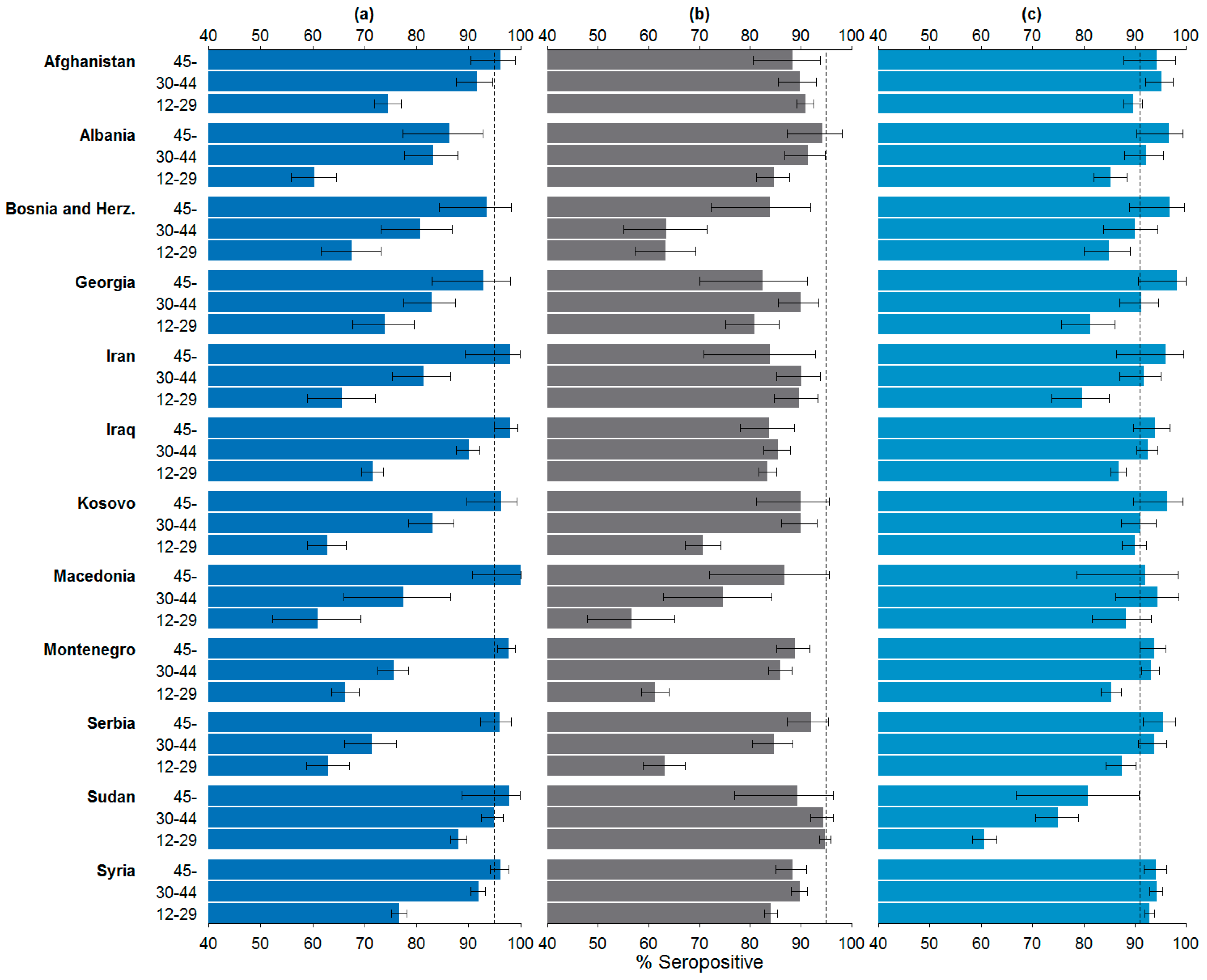
3.2.3. Countries of Origin by Age Groups
Measles
Rubella
Varicella
3.2.4. Factors Associated with Seropositivity
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Federal Office for Migration and Refugees (BAMF). Asylgeschäftsstatistik für den Monat Dezember 2015 (Official Statistics on Asylum Seekers in December 2015). Available online: http://www.bamf.de/SharedDocs/Anlagen/DE/Downloads/Infothek/Statistik/Asyl/201512-statistik-anlage-asyl-geschaeftsbericht.pdf?__blob=publicationFile (accessed on 6 January 2016).
- Federal Ministry of the Interior (BMI). Mehr Asylanträge in Deutschland als Jemals Zuvor (More Applications for Asylum in Germany than ever before). Available online: http://www.bmi.bund.de/SharedDocs/Pressemitteilungen/DE/2016/01/asylantraege-dezember-2015.htm (accessed on 11 January 2016).
- Kühne, A.; Gilsdorf, A. Ausbrüche von meldepflichtigen Infektionskrankheiten in Gemeinschaftsunterkünften von Asylbewerbern in Deutschland 2001–2003. In Proceedings of the 65 Wissenschaftliche Kongress des BVÖGD, Rostock, Germany, 23–25 April 2015.
- Robert Koch-Institute (RKI). Berliner Masernausbruch 2014/2015. Epidemiologisches Bull. 2015, 47/48. [Google Scholar] [CrossRef]
- Robert Koch-Institute (RKI). Dem Robert Koch-Institut Übermittelte Meldepflichtige Infektionskrankheiten bei Asylsuchenden in Deutschland (Notifiable Infectious Diseases among Asylum Seekers Reported to Robert Koch-Institute). Available online: https://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GesundAZ/Content/A/Asylsuchende/Inhalt/meldepflichtige_Infektionskrankheiten_bei_Asylsuchenden.html (accessed on 16 December 2015).
- Federal Office for Migration and Refugees (BAMF). Verteilung der Asylbewerber (Distribution of Asylum Seekers). Available online: http://www.bamf.de/DE/Migration/AsylFluechtlinge/Asylverfahren/Verteilung/verteilung.html (accessed on 21 December 2015).
- Ministry of Social Affairs, Health and Equal Opportunities of Lower Saxony (MS). Gesundheitsuntersuchung für Ausländerinnen und Ausländer nach § 62 Asylverfahrensgesetz (AsylVfG) und § 36 Abs. 4 Infektionsschutzgesetz (IfSG); Unpublished Internal Document; MS: Hanover, Germany, 2014. [Google Scholar]
- Andrews, N.; Tischer, A.; Siedler, A.; Pebody, R.G.; Barbara, C.; Cotter, S.; Duks, A.; Gacheva, N.; Bohumir, K.; Johansen, K.; et al. Towards elimination: Measles susceptibility in Australia and 17 European countries. Bull. World Health Organ. 2008, 86, 161–240. [Google Scholar] [CrossRef]
- Nardone, A.; Tischer, A.; Andrews, N.; Backhouse, J.; T2heeten, H.; Gatcheva, N.; Zarvou, M.; Kriz, B.; Pebody, R.G.; Bartha, K.; et al. Comparison of rubella seroepidemiology in 17 countries: Progress towards international disease control targets. Bull. World Health Organ. 2008, 86, 81–160. [Google Scholar] [CrossRef]
- WHO World Health organization (WHO). Eliminating Measles and Rubella. Framework for the Verification Process in the WHO European Region. Copenhagen: WHO Regional Office for Europe, 2014. Available online: http://www.euro.who.int/en/health-topics/communicable-diseases/measles-and-rubella/publications/2014/eliminating-measles-and-rubella.-framework-for-the-verification-process-in-the-who-european-region (accessed on 16 January 2015).
- Plans-Rubió, P. Evaluation of the establishment of herd immunity in the population by means of serological surveys and vaccination coverage. Hum. Vaccines Immunother. 2012, 8, 184–188. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing; 2016. Available online: http://www.R-project.org/ (accessed on 16 March 2016).
- United Nations (UN) Statistics Division. Composition of Macro Geographical (Continental) Regions, Geographical Sub-Regions, and Selected Economic and Other Groupings. Available online: http://unstats.un.org/unsd/methods/m49/m49regin.htm (accessed on 11 November 2015).
- Barnett, E.D.; Christiansen, D.; Figueira, M. Seroprevalence of measles, rubella and varicella in refugees. Clin. Infect. Dis. 2002, 35, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Robert Koch-Institute (RKI). Empfehlungen der Ständigen Impfkommission (STIKO) am Robert Koch-Institut/Stand: August 2014 (Recommendations of the Standing Committee on Vaccination (STIKO) at Robert Koch-Institute/August 2014). Available online: http://www.rki.de/DE/Content/Infekt/EpidBull/Archiv/2014/Ausgaben/34_14.pdf?__blob=publicationFile (accessed on 20 May 2016).
- Fine, P.; Eames, K.; Heymann, D.L. “Herd immunity”: A rough guide. Clin. Infect. Dis. 2011, 52, 911–916. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Social Affairs, Health and Equal Opportunities. Informationen für Die Leitungen von Gemeinschaftseinrichtungen für Asylsuchende des Landes Niedersachsen in Bezug auf die Vermeidung von Infektionskrankheiten (Information on the Management of Community Facilities for Asylum Seekers in Lower Saxony with Regard to the Prevention of Infectious Diseases). Available online: http://www.nlga.niedersachsen.de/download/101379 (accessed on 16 January 2016).
- Robert Koch-Institute (RKI). Konzept zur Umsetzung Frühzeitiger Impfungen bei Asylsuchenden Nach Ankunft in Deutschland (Concept of Implementation of Early Vaccinations among Asylum Seekers after the Arrival in Germany). Epidemiol. Bull. 2015, 41. [Google Scholar] [CrossRef]
- Takla, A.; Barth, A.; Siedler, A.; Stöcker, P.; Wichmann, O.; Deleré, Y. Measles outbreak in an asylum-seekers’ shelter in Germany: Comparison of the implemented with a hypothetical containment strategy. Epidemiol. Infect. 2012, 140, 1589–1598. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Country of Origin (N = 23,581) | No. | % |
|---|---|---|
| Syrian Arab Republic | 5135 | 21.8 |
| Iraq | 2822 | 12.0 |
| Montenegro | 2525 | 10.7 |
| Sudan | 2196 | 9.3 |
| Afghanistan | 1535 | 6.5 |
| Algeria | 1107 | 4.7 |
| Serbia | 1083 | 4.6 |
| Kosovo | 1045 | 4.4 |
| Albania | 799 | 3.4 |
| Ivory Coast | 632 | 2.7 |
| Sex | No. Positive | No. Tested | % Positive (95% CI) | |
|---|---|---|---|---|
| Measles | Male | 12,880 | 15,928 | 80.9 (80.2–81.5) |
| Female | 4030 | 5131 | 78.5 (77.4–79.7) | |
| Total | 18,896 | 23,647 | 79.9 (79.4–80.4) | |
| Rubella | Male | 13,907 | 15,926 | 87.3 (86.8–87.8) |
| Female | 4104 | 5129 | 80.0 (78.9–81.1) | |
| Total | 20,132 | 23,643 | 85.1 (84.7–85.6) | |
| Varicella | Male | 13,828 | 15,928 | 86.8 (86.3–87.3) |
| Female | 4610 | 5131 | 89.8 (89.0–90.7) | |
| Total | 20,693 | 23,647 | 87.5 (87.1–87.9) |
| Age Group | No. Positive | No. Tested | % Positive (95% CI) | |
|---|---|---|---|---|
| Measles | 12–29 | 11,328 | 15,121 | 74.9 (74.2–75.6) |
| 30–44 | 5682 | 6567 | 86.5 (85.7–87.3) | |
| 45– | 1886 | 1959 | 96.3 (95.3–97.1) | |
| Rubella | 12–29 | 12,600 | 15,119 | 83.3 (82.7–83.9) |
| 30–44 | 5803 | 6567 | 88.4 (87.6–89.1) | |
| 45– | 1729 | 1957 | 88.3 (86.8–89.7) | |
| Varicella | 12–29 | 12,835 | 15,121 | 84.9 (84.3–85.4) |
| 30–44 | 6011 | 6567 | 91.5 (90.8–92.2) | |
| 45– | 1847 | 1959 | 94.3 (93.2–95.3) |
| Factor | OR (95% CI) | Z-Statistic | p-Value | ||
|---|---|---|---|---|---|
| Measles | Sex | Female | (Ref.) | ||
| Male | 1.01 (0.93–1.10) | 0.24 | 0.813 | ||
| Age | 1.06 (1.06–1.07) | 27.7 | <0.001 | ||
| Rubella | Sex | Female | (Ref.) | ||
| Male | 1.32 (1.20–1.44) | 6.03 | <0.001 | ||
| Age | 1.03 (1.03–1.04) | 15.2 | <0.001 | ||
| Varicella | Sex | Female | (Ref.) | ||
| Male | 1.03 (0.92–1.15) | 0.54 | 0.590 | ||
| Age | 1.04 (1.03–1.04) | 13.3 | <0.001 | ||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toikkanen, S.E.; Baillot, A.; Dreesman, J.; Mertens, E. Seroprevalence of Antibodies against Measles, Rubella and Varicella among Asylum Seekers Arriving in Lower Saxony, Germany, November 2014–October 2015. Int. J. Environ. Res. Public Health 2016, 13, 650. https://doi.org/10.3390/ijerph13070650
Toikkanen SE, Baillot A, Dreesman J, Mertens E. Seroprevalence of Antibodies against Measles, Rubella and Varicella among Asylum Seekers Arriving in Lower Saxony, Germany, November 2014–October 2015. International Journal of Environmental Research and Public Health. 2016; 13(7):650. https://doi.org/10.3390/ijerph13070650
Chicago/Turabian StyleToikkanen, Salla E., Armin Baillot, Johannes Dreesman, and Elke Mertens. 2016. "Seroprevalence of Antibodies against Measles, Rubella and Varicella among Asylum Seekers Arriving in Lower Saxony, Germany, November 2014–October 2015" International Journal of Environmental Research and Public Health 13, no. 7: 650. https://doi.org/10.3390/ijerph13070650