
Toward a Socio-Territorial Approach to Health: Health Equity in West Africa

Abstract
:1. Introduction
2. Methods
2.1. Analysis of Socio-Spatial Contexts
2.2. Health Status, Health Behaviour and Health Inequalities
3. Results
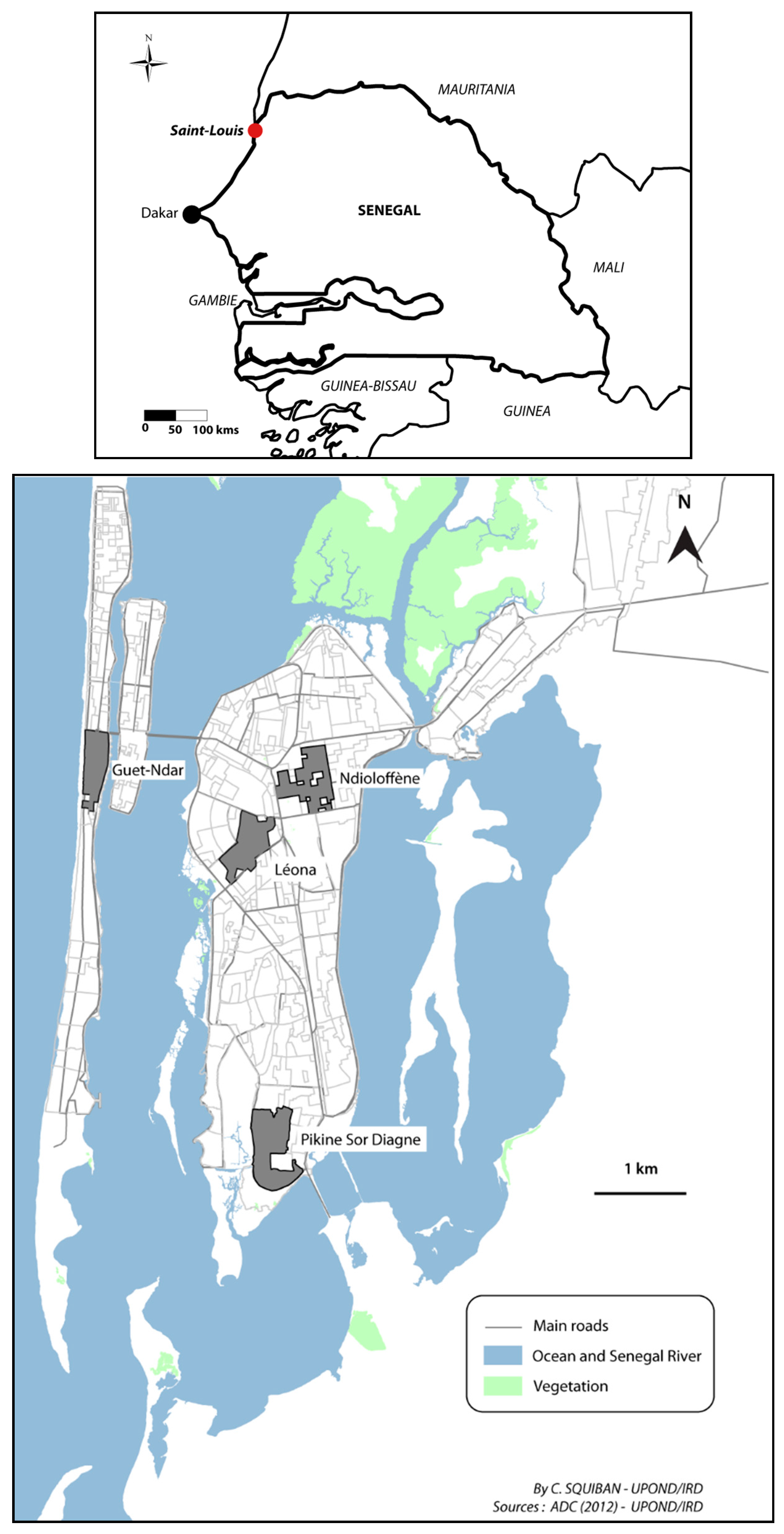
3.1. Socio-Territorial Processes in Saint-Louis
3.1.1. Guet Ndar, from Fishing Village to Economic Hub of Saint-Louis
3.1.2. Ndioloffène and Léona: Two Colonial Neighbourhoods, Two Distinct Histories
3.1.3. Pikine Sor Diagne, the Face of Urban Sprawl
3.1.4. How Politics Materialize in Physical Space: The Example of Local Development
3.2. Spatial Variations in Health Status and Statistical Associations
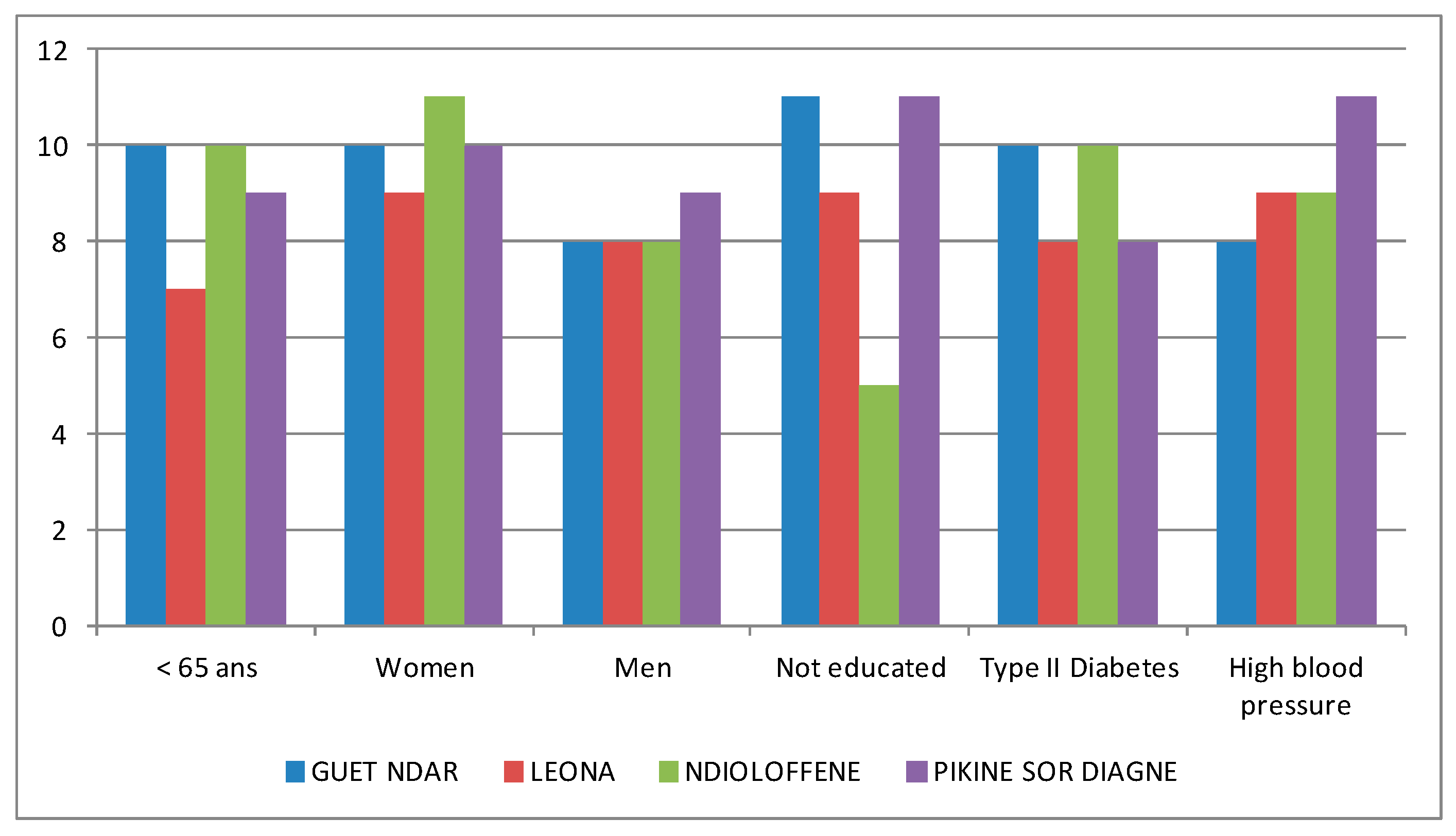
3.3. Health Inequalities and Care-Seeking Behaviour
4. Discussion
4.1. Socio-Territorial Processes and Risk of Non-Communicable Disease
4.2. Socio-Territorial Processes, Health Behaviour and Therapeutic Itineraries
4.3. Limitations of the Study
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kearns, R.; Moon, G. From medical to health geography: Novelty, place and theory after a decade of change. Prog. Hum. Geogr. 2002, 26, 605–625. [Google Scholar] [CrossRef]
- Logan, J.R. Making a place for space: Spatial thinking in social science. Annu. Rev. Soc. 2012, 38, 507–524. [Google Scholar] [CrossRef] [PubMed]
- Macintyre, S.; Ellaway, A.; Cummins, S. Place effects on health: How can we conceptualise, operationalise and measure them? Soc. Sci. Med. 2002, 55, 125–139. [Google Scholar] [CrossRef]
- Entwisle, B. Putting people into place. Demography 2002, 44, 687–703. [Google Scholar] [CrossRef]
- Gatrell, A.C.; Popay, J.; Thomas, C. Mapping the social determinants of health inequalities in social space: Can Bourdieu help us? Health Place 2004, 10, 245–257. [Google Scholar] [CrossRef] [PubMed]
- Cummins, S.; Curtis, S.; Diez-Roux, A.; Macintyre, S. Understanding and representing “place“ in health research: A relational approach. Soc. Sci. Med. 2007, 65, 1825–1838. [Google Scholar] [CrossRef] [PubMed]
- Salem, G.; Rican, S.; Kürzinger, M.L. Atlas de la Santé en France: Volume 2. Comportements et Maladies; John Libbey Eurotext: Montrouge, France, 2006; p. 222. [Google Scholar]
- Gregory, D.; Johnston, R.; Pratt, G.; Watts, M.; Whatmore, S. The Dictionary of Human Geography, 5th ed.; Wiley-Blackwell: New York, NY, USA, 2009. [Google Scholar]
- Salem, G. La Santé Dans la Ville—Géographie d’un Petit Espace Dense Pikine (Sénégal); Karthala ORSTOM: Paris, France, 1998; p. 360. [Google Scholar]
- Foley, E.E. Your Pocket Is What Cures You: The Politics of Health in Senegal; Rutgers U Press: Chapel Hill, NC, USA, 2010; p. 216. [Google Scholar]
- Janzen, J. The Quest for Therapy in Lower Zaire; University of California Press: Berkeley, CA, USA, 1978; p. 328. [Google Scholar]
- Hiatt, R.A.; Breen, N. The social determinants of cancer, a challenge for transdisciplinary science. Am. J. Prev. Med. 2008, 35, S141–S150. [Google Scholar] [CrossRef] [PubMed]
- Mackenbach, J.P.; Kunst, A.E.; Cavelaars, A.; Groenhof, F.; Geurts, J.M. Socioeconomic inequalities in morbidity and mortality in Western Europe. Lancet 1997, 349, 1655–1659. [Google Scholar] [CrossRef]
- Vinnakota, S.; Lam, N.S.N. Socioeconomic inequality of cancer mortality in the United States: A spatial data mining approach. Int. J. Health Geogr. 2006, 5, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Drame, F.M.; Foley, E.E. HIV/AIDS in mid-sized cities in Senegal: From individual to place-based vulnerability. Soc. Sci. Med. 2015, 133C, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Vaillant, Z. La Réunion, Koman I lé ? Territoires, Santé, Société; PUF Le Monde Partage du Savoir: Paris, France, 2008; p. 253. [Google Scholar]
- Oppong, J.; Kutch, L.; Tiwari, C.; Arbona, S. Vulnerable places: Prison locations, socioeconomic status, and HIV infection in Texas. Prof. Geogr. 2014, 66, 653–663. [Google Scholar] [CrossRef]
- Harvey, D. Le capitalisme Contre le Droit à la Ville, Néolibéralisme, Urbanisation, Résistances; Editions Amsterdam: Paris, France, 2011; p. 93. [Google Scholar]
- Bonnardel, R. Saint-Louis du Sénégal: Mort ou Naissance; L’Harmattan: Paris, France, 2000; p. 424. [Google Scholar]
- Ngalamulume, K. Keeping the city totally clean: Yellow fever and the politics of prevention in Colonial Saint Louis-du-Senegal, 1850–1914. J. Afr. Hist. 2004, 45, 183–202. [Google Scholar] [CrossRef]
- Ngalamulume, K. Plague and Violence in Saint-Louis-du-Senegal, 1917–1920. Cahiers d’Etudes Africaines 2006, 183, 539–565. [Google Scholar] [CrossRef]
- Fouchard, L. De la Ville Coloniale à la Cour Africaine. Espaces, Pouvoirs et Sociétés à Ouagadougou et à Bobo-Dioulasso (Haute-Volta), Fin XIXe Siècle—1960; L’Harmattan: Paris, France, 2001; p. 427. [Google Scholar]
- Labazee, P. Emploi, revenus, statuts sociaux et réseaux de sociabilité dans les villes secondaires du Burkina Faso, du Mali et de la Côte d’Ivoire. In La Ville de Bobo-Dioulasso au Burkina Faso. Urbanités et Appartenances en Afrique de L’Ouest; Werthmann, K., Sanogo, M.L., Eds.; Karthala: Paris, France, 2013; p. 324. [Google Scholar]
- Sinou, A. Saint-Louis-du-Sénégal au début du XIXe siècle: Du comptoir à la ville. Cahiers d’Etudes Africaines 1989, 29, 377–395. [Google Scholar] [CrossRef]
- Camera, C. Saint Louis du Sénégal: Evolution d’une Ville en Milieu Africain; Musée Théodore Monod d’Art Africain (IFAN): Dakar, Sénégal, 1968; p. 282. [Google Scholar]
- Nyamnjoh, H.M. We Get Nothing From Fishing: Fishing for Boat Opportunities amongst Senegalese Fisher Migrants; Langaa and African Studies Center: Bamanda, Cameroun, 2010; p. 232. [Google Scholar]
- Niang, D. Gouvernance Locale, Maîtrise D’ouvrage Communale et Stratégies de Développement Local au Sénégal: L’expérience de la Ville de Saint-Louis. Ph.D. Thesis, Université Toulouse Le Mirail, Toulouse, France, 2007; p. 267. [Google Scholar]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef]
- Mbamya, J.C.N.; Motala, A.; Sobngqi, E.; Assah, F.K.; Enoru, S.T. Diabetes in sub-Saharan Africa. Lancet 2010, 375, 2254–2266. [Google Scholar] [CrossRef]
- Gold, C.L.; Clapp, R.A. Negotiating health and identity: Lay healing, medicinal plants, and indigenous healthscapes in Highland Peru. Lat. Am. Res. Rev. 2011, 46, 93–111. [Google Scholar] [CrossRef]
- Thorsen, R.S. Conceptualizations of pluralistic medical fields: Exploring the therapeutic landscapes of Nepal. Health Place 2015, 31, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.M. The barbed walls of China: A contemporary grassland drama. J. Asian Stud. 1996, 55, 665–691. [Google Scholar] [CrossRef]
- Livingston, J. Improvising Medicine: An African Oncology Ward in an Emerging Cancer Epidemic; Duke University Press: Durham, NC, USA, 2012; p. 248. [Google Scholar]
- Whyte, S.R. Knowing hypertension and diabetes: Conditions of treatability in Uganda. Health Place 2016, 39, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Neupane, S.; Prakash, K.C.; Teye, D. Overweight and obesity among women: Analysis of demographic and health survey data from 32 Sub-Saharan African Countries. BMC Public Health 2016, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Renzaho, A. Fat, rich and beautiful: Changing socio-cultural paradigms associated with obesity risk, nutritional status and refugee children from sub-Saharan Africa. Health Place 2004, 10, 105–113. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Participants | Guet Ndar | Léona | Ndioloffène | Pikine sor Diagne | p Value | |
|---|---|---|---|---|---|---|---|
| 815 | 214 | 186 | 224 | 191 | |||
| Age of participants | 35–39 | 196 (24) | 49 (22.9) | 38 (20.4) | 59 (26.3) | 50 (26.2) | N.S |
| 40–44 | 181 (22.2) | 40 (18.7) | 45 (24.2) | 46 (20.5) | 50 (26.2) | ||
| 45–49 | 133 (16.3) | 37 (17.3) | 27 (14.5) | 35 (15.6) | 34 (17.8) | ||
| 50–54 | 155 (19) | 41 (19.2) | 41 (22) | 44 (19.6) | 29 (15.2) | ||
| ≥55 | 146 (17.9) | 47 (21.9) | 32 (17.2) | 40 (17.9) | 27 (14.1) | ||
| Sex of participants | Women | 650 (79.8) | 176 (82.2) | 143 (76.9) | 185 (82.6) | 146 (76.4) | N.S |
| Men | 165 (21.2) | 38 (17.8) | 43 (23.1) | 39 (17.4) | 45 (23.6) | ||
| Education level | Not educated | 345 (42.3) | 148 (69.2) | 52 (28) | 48 (21.4) | 97 (50.8) | p < 0.01 |
| Length of residence | Born in Saint-Louis | 649 (79.6) | 204 (95.3) | 144 (77.4) | 186 (83) | 115 (60.2) | p < 0.05 |
| Neighbourhood satisfaction | Wish to stay in their neighbourhood | 394 (48.3) | 35 (16.4) | 91 (48.9) | 128 (57.1) | 140 (73.3) | p < 0.01 |
| Perception of health status | Poor | 191 (23.4) | 42 (19.6) | 42 (22.6) | 37 (16.5) | 70 (36.6) | p < 0.01 |
| Correct | 270 (33.1) | 77 (36) | 43 (23.1) | 92 (41.1) | 58 (30.4) | ||
| Good to excellent | 348 (42.7) | 95 (44.4) | 98 (52.7) | 92 (41.1) | 63 (33) | ||
| Variables | Scale of Variables | Guet Ndar | Pikine | Ndioloffène | Léona | ||
| Socio-spatial context | Age of the neighbourhood | Neighbourhood level | Precolonial district: traditional Wolof fishing neighbourhood | Precolonial village of fishermen and farmers: late integration to Saint-Louis as an administrative district (1980s) | Created during the colonial period (beginning of the 19th century): socially and ethnically mixed neighbourhood with some gentrification | Created during the colonial period (mid-20th century): middle to upper class households, historically served as colonial civil servants | |
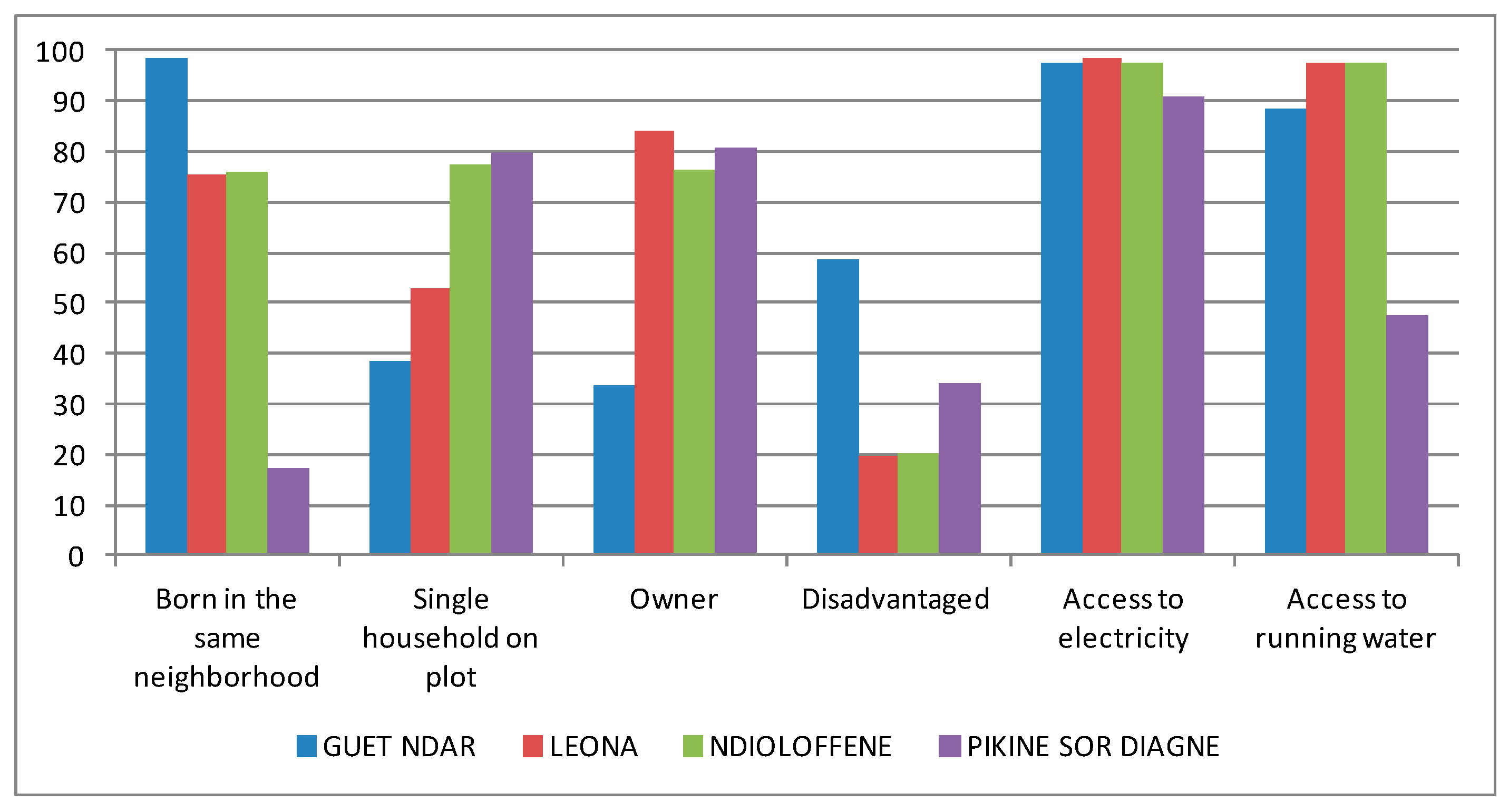
| Length of residence in Saint-Louis (percentage of people born in the city) | Individual level | 96.20% | 60.50% | 83.00% | 78.70% | ||
| Spatial Heterogeneity | Built density | Neighbourhood level | Very high | Low | Low | Medium | |
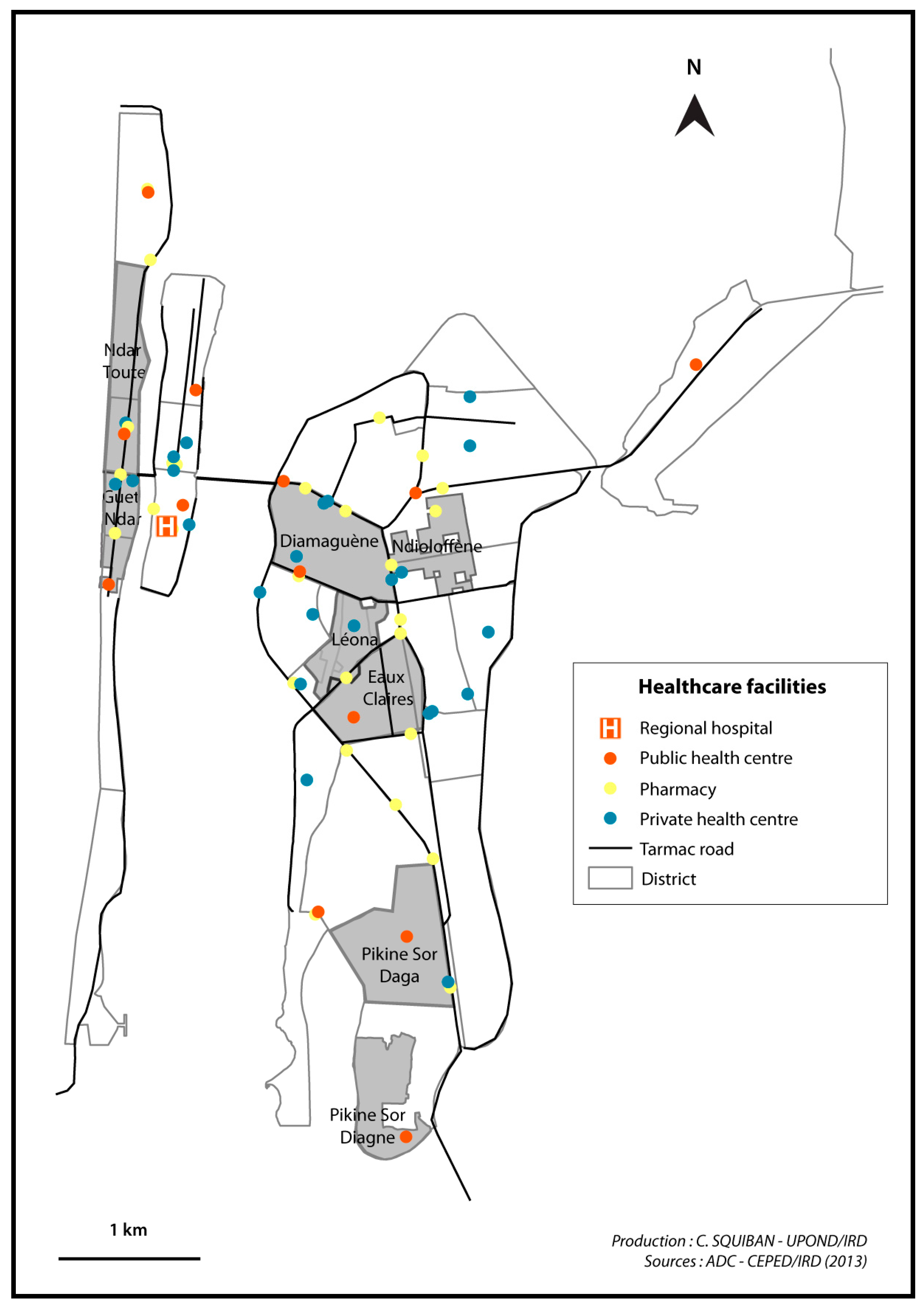
| Physical proximity to health care structures | Very good | Poor | Very poor | Good | |||
| Availability of water and electricity | Household access to water and electricity | Ongoing plans to improve for municipal water and electric supply systems | Household access to water and electricity | Household access to water and electricity | |||
| Economic status | Poor | Household level | 58.50% | 34.20% | 20.30% | 19.50% | |
| Middle class | 31.30% | 33.70% | 28.90% | 38.60% | |||
| Upper class | 10.20% | 32.10% | 50.80% | 41.90% | |||
| Education level | Not educated | Individual level | 69.20% | 50.80% | 21.40% | 28.00% | |
| Socio-territorial organization | Perceptions of the neighbourhood (verbatim records from interviews) | Neighbourhood level | “There is a boundary between Saint-Louis and Guet Ndar.” | “They are sectarian people. It is a neighbourhood of fishermen: they are very close.” | “The neighbourhood is one the hubs of Saint-Louis’ intelligentsia.” | “It is a neighbourhood of intellectuals. […] in Léona, we are urban dwellers, with proper urban practices.” | |
| Organization of political actors and network for local development | Neighbourhood level | Cooperation between the local council and the municipal government which directs external funds to Guet Ndar. But lack of legitimacy of the local council among residents who use their own networks to finance neighbourhood projects. | No representation of Sor Diagne residents in the local council. Modest and sporadic projects of local development led by community associations. | Omnipresence of powerbrokers who govern the local council according to their own political ends. They secure significant amounts of external and internal funding for major projects. | Omnipresence of the local council which coordinates local actors for various large projects. Increasing autonomy from the municipal government thanks to tremendous fundraising capacity. | ||
| Presence of health promotion and prevention projects | Neighbourhood level | Several days of free medical consultations have been organized, and an ambulance was purchased by external donors through a key powerbroker. | A small dispensary was built with external financing. Free medical consultations have been organized for non-communicable diseases screening, implemented by the greater Pikine council at the Sor Daga health post. | Several days of free medical consultations and follow-up for chronic disease patients have been organized and financed by local powerbrokers. | Several campaigns for health prevention and follow-up for chronic disease patients were funded by international donors. Renovation of the local health post was paid for by external funding. | ||
| Variables | Scale of Variables | Guet Ndar | Pikine | Ndioloffène | Léona | ||
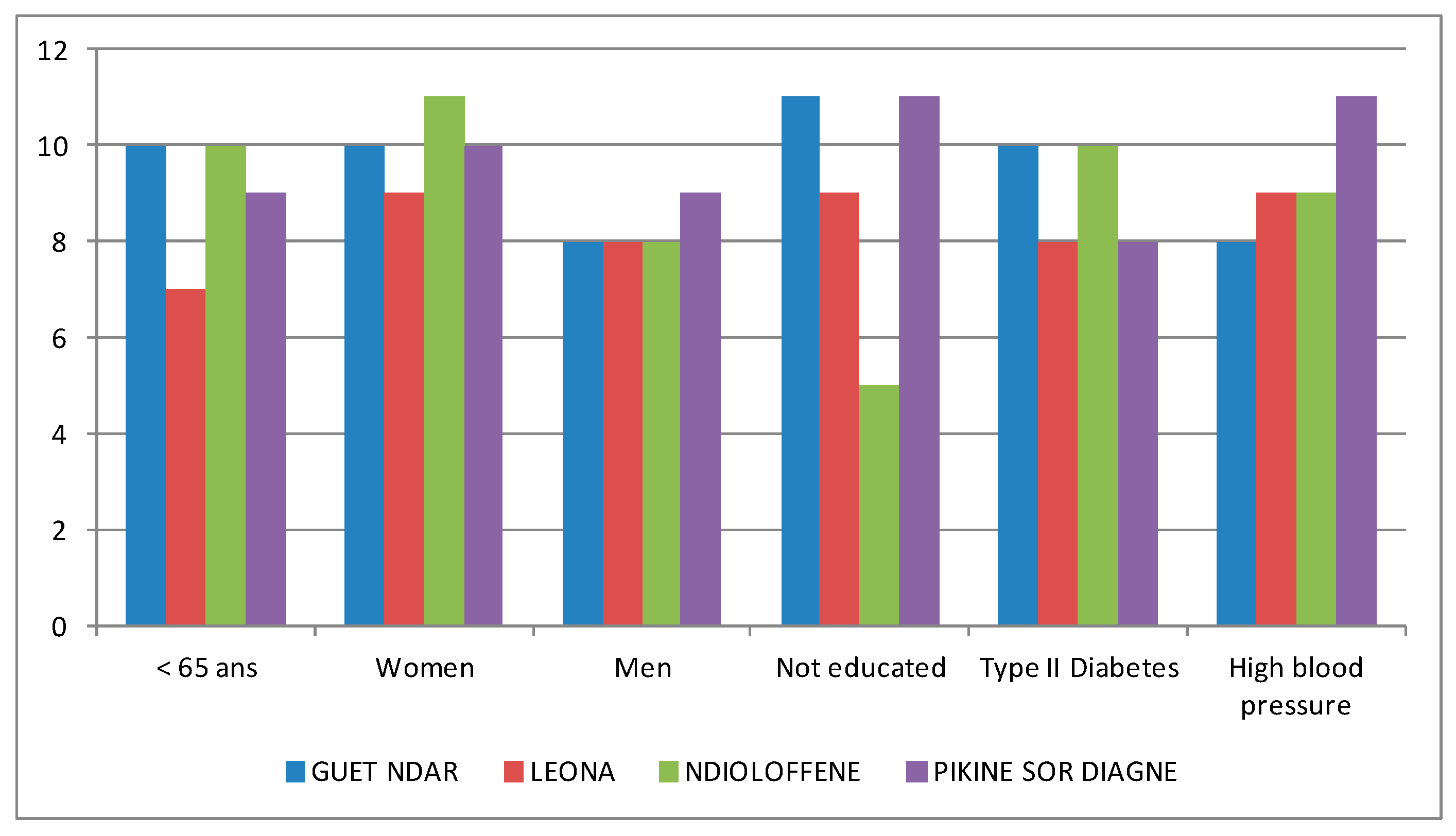
| Health status | Overweight | Neighbourhood level | 77.10% | 56.50% | 59.80% | 56.50% | |
| Prevalence of high blood pressure | 42.50% | 32.50% | 38.40% | 28.50% | |||
| Prevalence of hyperglycaemia | 12.60% | 6.80% | 8.90% | 7.50% | |||
| Health Indicators | Full Sample | Guet Ndar | Léona | Ndioloffène | Pikine Sor Diagne | p Value |
|---|---|---|---|---|---|---|
| 815 | 214 | 186 | 224 | 191 | ||
| Overweight | 512 (62.8) | 165 (77.1) | 105 (56.5) | 134 (59.8) | 108 (56.5) | p < 0.01 |
| High blood pressure | 292 (35.8) | 91 (42.5) | 53 (28.5) | 86 (38.4) | 62 (32.5) | p < 0.05 |
| Hyperglycaemia | 74 (9.1) | 27 (12.6) | 14 (7.5) | 20 (8.9) | 13 (6.8) | N.S |
| Overweight (A = Affected/NA = Non-Affected) | ||||||||||||||||
| Contributing Factor | Total (%) | Guet Ndar (%) | Léona (%) | Ndioloffène (%) | Pikine Sor Diagne (%) | |||||||||||
| A | NA | p Value | A | NA | p Value | A | NA | p Value | A | NA | p Value | A | NA | p Value | ||
| Sex | Female | 56.9 | 22.8 | p < 0.01 | 69.2 | 13.1 | p < 0.01 | 52.7 | 24.2 | p < 0.01 | 54.9 | 27.7 | p < 0.01 | 49.7 | 26.7 | p < 0.01 |
| Male | 5.8 | 14.0 | 7.9 | 9.8 | 3.2 | 18.3 | 4.9 | 12.5 | 6.8 | 16.2 | ||||||
| Age | 35–39 | 11.8 | 12.3 | p < 0.01 | 15.9 | 7.0 | N.S | 7.0 | 13.4 | p < 0.01 | 10.7 | 15.6 | p < 0.01 | 13.1 | 13.1 | N.S |
| 40–44 | 14.2 | 8.0 | 15.0 | 3.7 | 14.5 | 9.7 | 13.8 | 6.7 | 13.6 | 12.6 | ||||||
| 45–49 | 10.2 | 6.1 | 13.6 | 3.7 | 8.6 | 5.9 | 8.9 | 6.7 | 9.4 | 8.4 | ||||||
| 50–54 | 12.8 | 6.3 | 13.6 | 5.6 | 11.3 | 10.8 | 14.3 | 5.4 | 11.5 | 3.7 | ||||||
| ≥55 | 13.6 | 4.3 | 19.2 | 2.8 | 14.0 | 3.2 | 12.1 | 5.8 | 8.9 | 5.2 | ||||||
| Education level | Educated | 32.3 | 23.1 | p < 0.05 | 21.0 | 9.3 | N.S | 34.4 | 29.0 | N.S | 46.9 | 31.7 | N.S | 25.7 | 22.5 | N.S |
| Not educated | 29.4 | 12.9 | 55.6 | 13.6 | 18.3 | 9.7 | 12.9 | 8.5 | 30.4 | 20.4 | ||||||
| Economic status of household | Poor | 21.3 | 11.2 | N.S | 44.9 | 12.1 | N.S | 10.8 | 7.5 | N.S | 9.8 | 10.7 | N.S | 18.8 | 14.1 | N.S |
| Middle class | 21.1 | 12.0 | 23.8 | 7.9 | 23.1 | 14.0 | 19.6 | 11.2 | 17.8 | 15.7 | ||||||
| Upper class | 19.5 | 13.6 | 6.5 | 2.8 | 21.0 | 21.0 | 30.4 | 18.3 | 19.9 | 13.1 | ||||||
| High Blood Pressure (A = Affected/NA = Non-Affected) | ||||||||||||||||
| Contributing Factor | Total (%) | Guet Ndar (%) | Léona (%) | Ndioloffène (%) | Pikine Sor Diagne (%) | |||||||||||
| A | NA | p Value | A | NA | p Value | A | NA | p Value | A | NA | p Value | A | NA | p Value | ||
| Sex | Female | 30.9 | 48.8 | p < 0.01 | 36.9 | 45.3 | N.S | 23.7 | 53.2 | N.S | 32.6 | 50.0 | N.S | 29.3 | 47.1 | p < 0.01 |
| Male | 4.9 | 14.8 | 5.6 | 12.1 | 4.8 | 16.7 | 5.8 | 11.6 | 3.1 | 19.9 | ||||||
| Age | 35–39 | 4.5 | 19.5 | p < 0.01 | 6.5 | 16.4 | p < 0.01 | 2.7 | 17.7 | p < 0.05 | 4.9 | 21.4 | p < 0.01 | 3.7 | 22.5 | p < 0.01 |
| 40–44 | 6.7 | 15.5 | 7.0 | 11.7 | 5.4 | 18.8 | 8.0 | 12.5 | 19.9 | 6.3 | ||||||
| 45–49 | 4.7 | 11.7 | 5.1 | 12.1 | 4.8 | 9.7 | 2.7 | 12.9 | 6.3 | 11.5 | ||||||
| 50–54 | 8.8 | 10.2 | 10.3 | 8.9 | 5.9 | 16.1 | 10.7 | 8.9 | 7.9 | 7.3 | ||||||
| ≥55 | 10.8 | 7.1 | 13.6 | 8.4 | 8.6 | 8.6 | 12.1 | 5.8 | 8.4 | 5.8 | ||||||
| Education level | Educated | 19.6 | 35.7 | N.S | 12.6 | 17.8 | N.S | 18.8 | 44.6 | N.S | 30.8 | 47.8 | N.S | 15.2 | 33.0 | N.S |
| Not educated | 16.0 | 26.4 | 29.9 | 39.3 | 8.6 | 19.4 | 7.6 | 13.8 | 17.3 | 33.5 | ||||||
| Economic status of household | Poor | 12.5 | 20.0 | N.S | 26.2 | 30.8 | N.S | 3.8 | 14.5 | N.S | 8.0 | 12.5 | N.S | 11.0 | 22.0 | N.S |
| Middle class | 11.5 | 21.6 | 10.3 | 21.5 | 12.4 | 24.7 | 13.8 | 17.0 | 9.4 | 24.1 | ||||||
| Upper class | 11.3 | 21.8 | 5.1 | 4.2 | 11.3 | 30.6 | 16.5 | 32.1 | 12.0 | 20.9 | ||||||
| Hyperglycaemia (A = Affected/NA = Non-Affected) | ||||||||||||||||
| Contributing Factor | Total (%) | Guet Ndar (%) | Léona (%) | Ndioloffène (%) | Pikine Sor Diagne (%) | |||||||||||
| A | NA | p Value | A | NA | p Value | A | NA | p Value | A | NA | p Value | A | NA | p Value | ||
| Sex | Woman | 8.0 | 71.8 | p < 0.05 | 11.2 | 71.0 | N.S | 6.5 | 70.4 | N.S | 8.5 | 74.1 | N.S | 5.2 | 71.2 | N.S |
| Man | 1.0 | 19.0 | 1.4 | 16.4 | 0.5 | 21.5 | 0.4 | 17.0 | 1.6 | 22.0 | ||||||
| Age | 35–39 | 1.2 | 22.8 | p < 0.01 | 2.3 | 20.6 | N.S | 0.5 | 19.9 | p < 0.01 | 1.3 | 25.0 | N.S | 0.5 | 25.7 | N.S |
| 40–44 | 1.5 | 20.7 | 1.4 | 17.3 | 1.1 | 23.1 | 1.3 | 19.2 | 2.1 | 24.1 | ||||||
| 45–49 | 1.8 | 14.5 | 3.3 | 14.0 | 1.1 | 13.4 | 1.3 | 14.3 | 1.6 | 16.2 | ||||||
| 50–54 | 1.7 | 17.3 | 2.8 | 16.4 | 1.1 | 21.0 | 1.8 | 17.9 | 1.0 | 14.1 | ||||||
| ≥55 | 2.5 | 15.5 | 2.8 | 19.2 | 2.7 | 14.5 | 3.1 | 14.7 | 1.0 | 13.1 | ||||||
| Education level | Educated | 4.8 | 50.8 | N.S | 2.3 | 28.0 | N.S | 4.8 | 59.1 | N.S | 6.7 | 71.9 | N.S | 5.2 | 43.5 | N.S |
| Not educated | 4.0 | 38.3 | 10.3 | 58.9 | 1.6 | 26.3 | 2.2 | 19.2 | 1.6 | 49.2 | ||||||
| Economic status of household | Poor | 2.9 | 29.6 | N.S | 8.4 | 48.6 | N.S | 0.0 | 18.3 | N.S | 2.2 | 18.3 | N.S | 0.5 | 32.5 | p < 0.05 |
| Middle class | 2.3 | 30.9 | 1.9 | 29.9 | 4.8 | 32.3 | 1.3 | 29.5 | 1.6 | 32.5 | ||||||
| Upper class | 3.7 | 29.6 | 1.9 | 7.5 | 2.7 | 39.8 | 5.4 | 43.3 | 4.7 | 28.3 | ||||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vialard, L.; Squiban, C.; Riveau, G.; Hermann, E.; Diop, D.; Fournet, F.; Salem, G.; Foley, E.E. Toward a Socio-Territorial Approach to Health: Health Equity in West Africa. Int. J. Environ. Res. Public Health 2017, 14, 106. https://doi.org/10.3390/ijerph14010106
Vialard L, Squiban C, Riveau G, Hermann E, Diop D, Fournet F, Salem G, Foley EE. Toward a Socio-Territorial Approach to Health: Health Equity in West Africa. International Journal of Environmental Research and Public Health. 2017; 14(1):106. https://doi.org/10.3390/ijerph14010106
Chicago/Turabian StyleVialard, Lucie, Clara Squiban, Gilles Riveau, Emmanuel Hermann, Doudou Diop, Florence Fournet, Gérard Salem, and Ellen E. Foley. 2017. "Toward a Socio-Territorial Approach to Health: Health Equity in West Africa" International Journal of Environmental Research and Public Health 14, no. 1: 106. https://doi.org/10.3390/ijerph14010106