
Gold Mining in Ecuador: A Cross-Sectional Assessment of Mercury in Urine and Medical Symptoms in Miners from Portovelo/Zaruma

Abstract
:1. Introduction
2. Materials and Methods
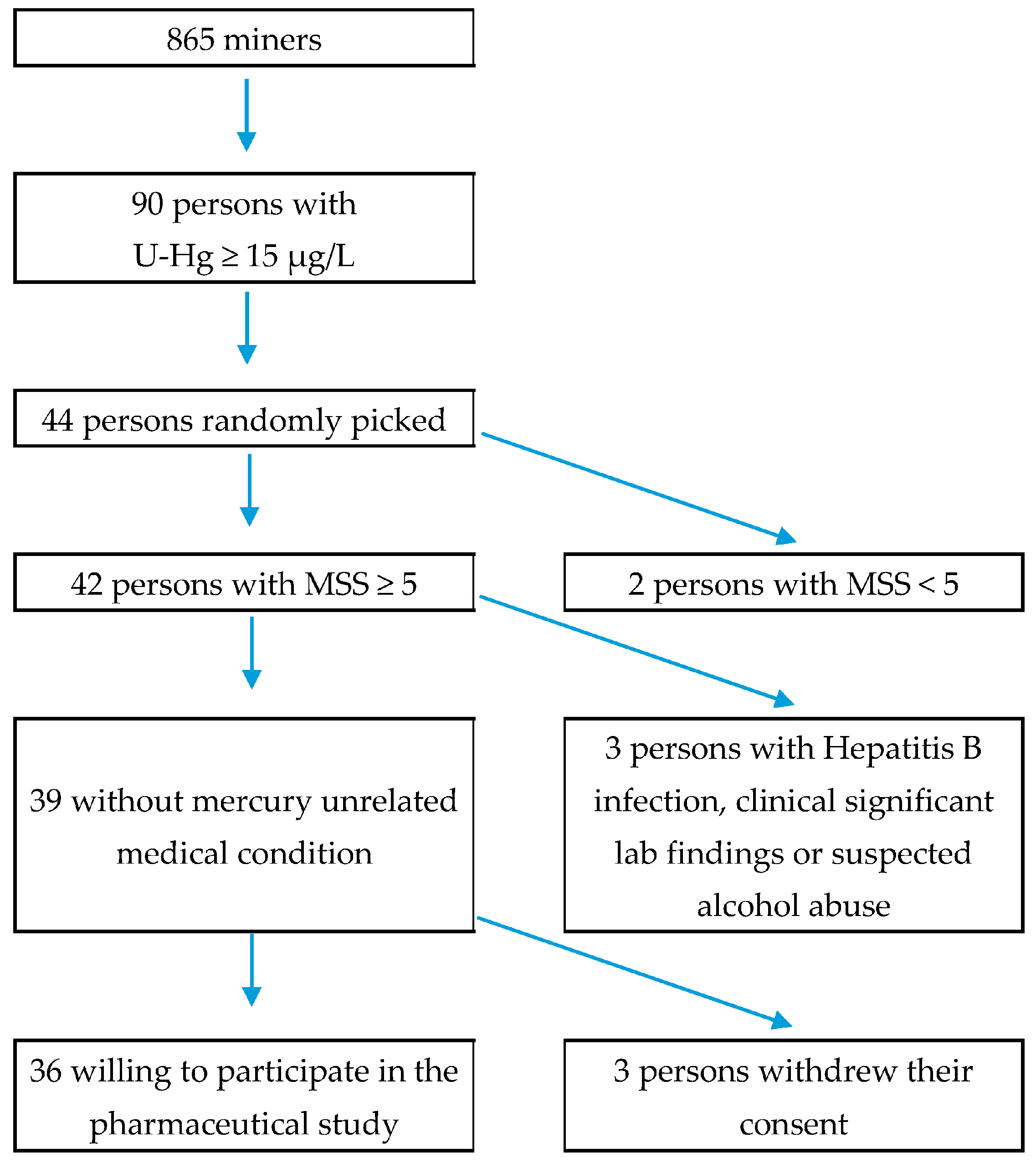
2.1. Subject Selection
2.2. Collection of the Urine Samples
2.3. The Lumex Analyser RA-951+
2.4. Preparation of the Chemical Solutions
2.5. Measurement
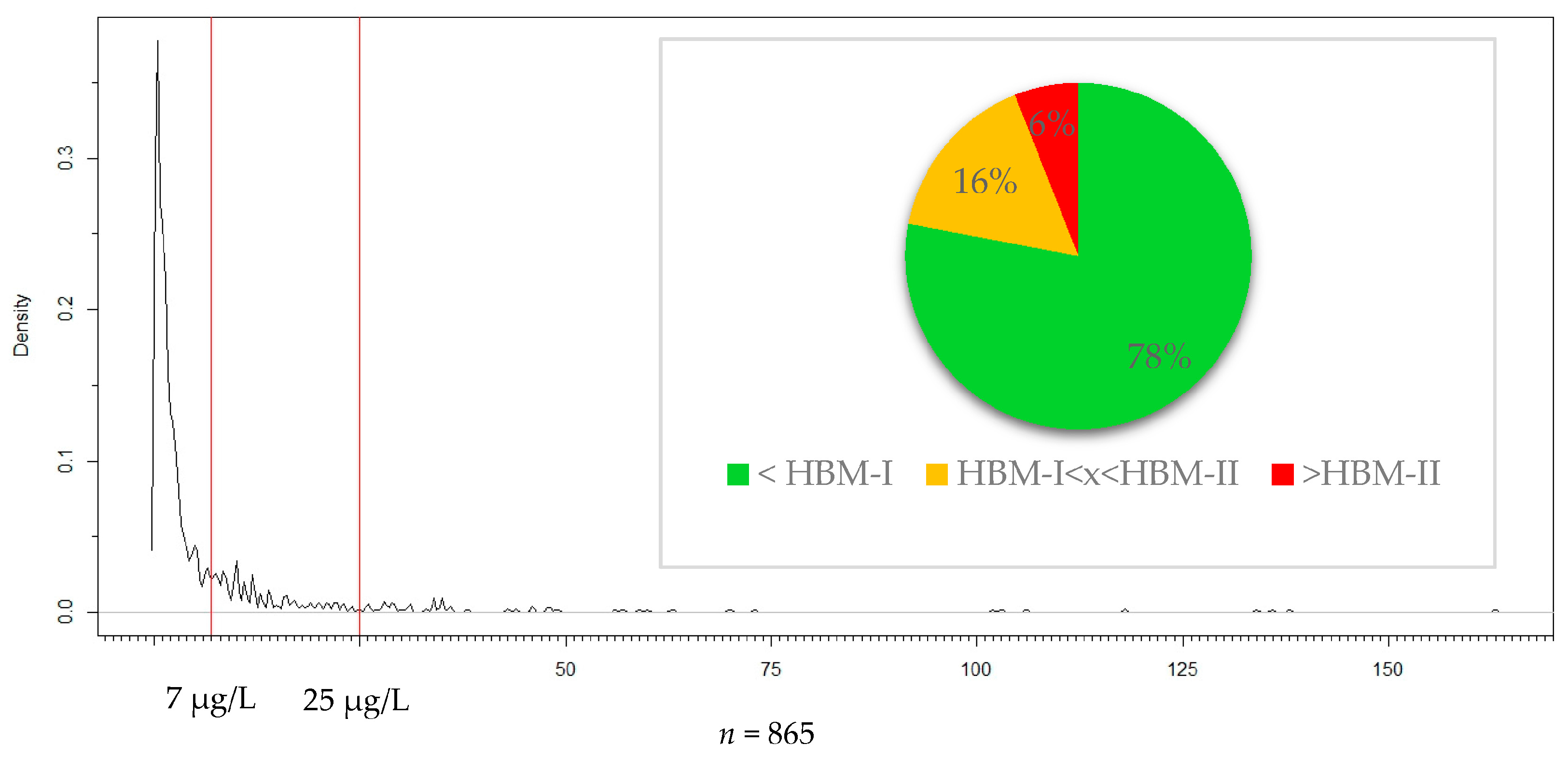
2.6. Threshold Values
2.7. Medical Score Sum and Further Clinical Symptoms
2.8. Statistical Methods
3. Results
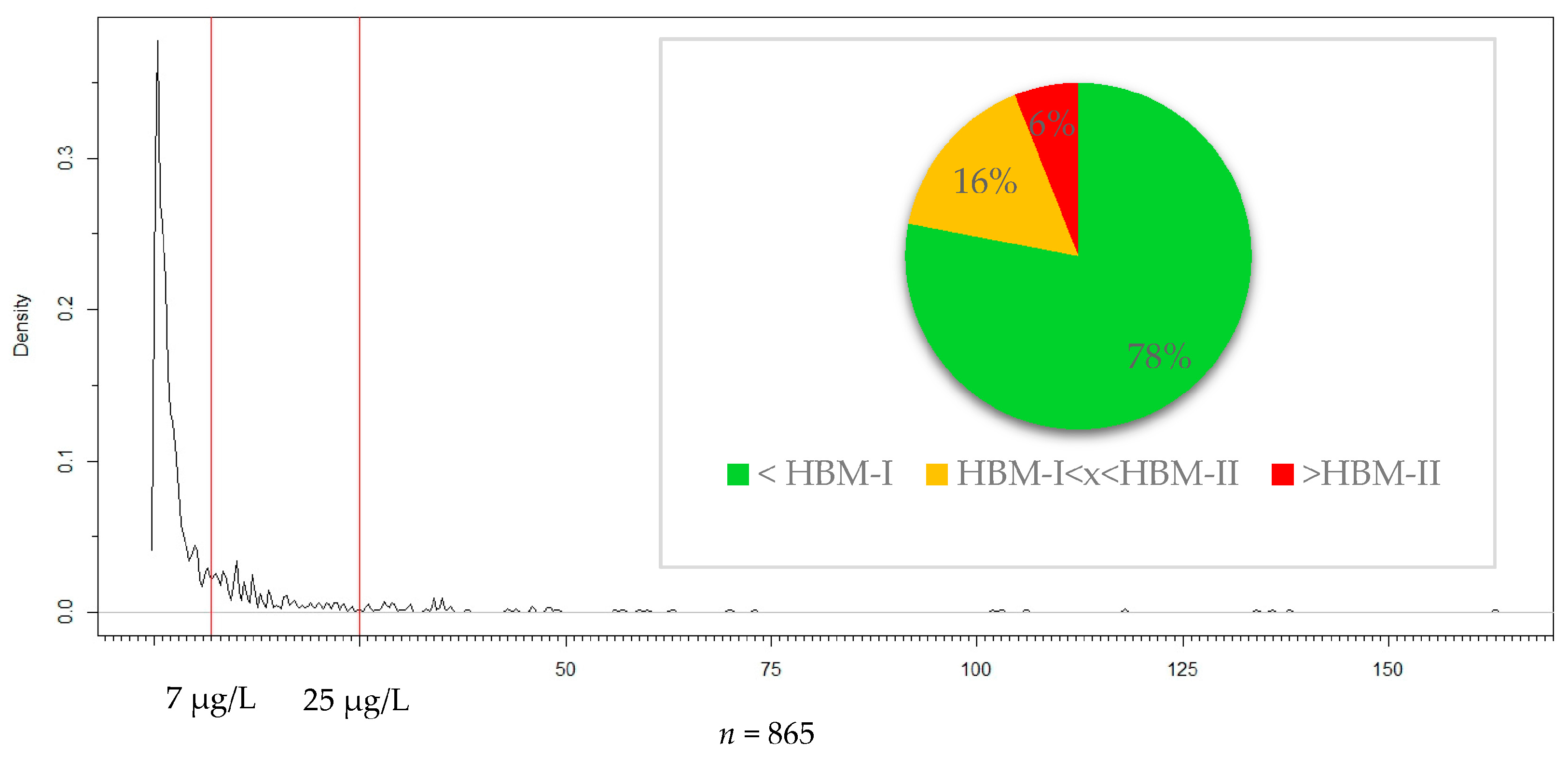
3.1. Prevalence and Distribution
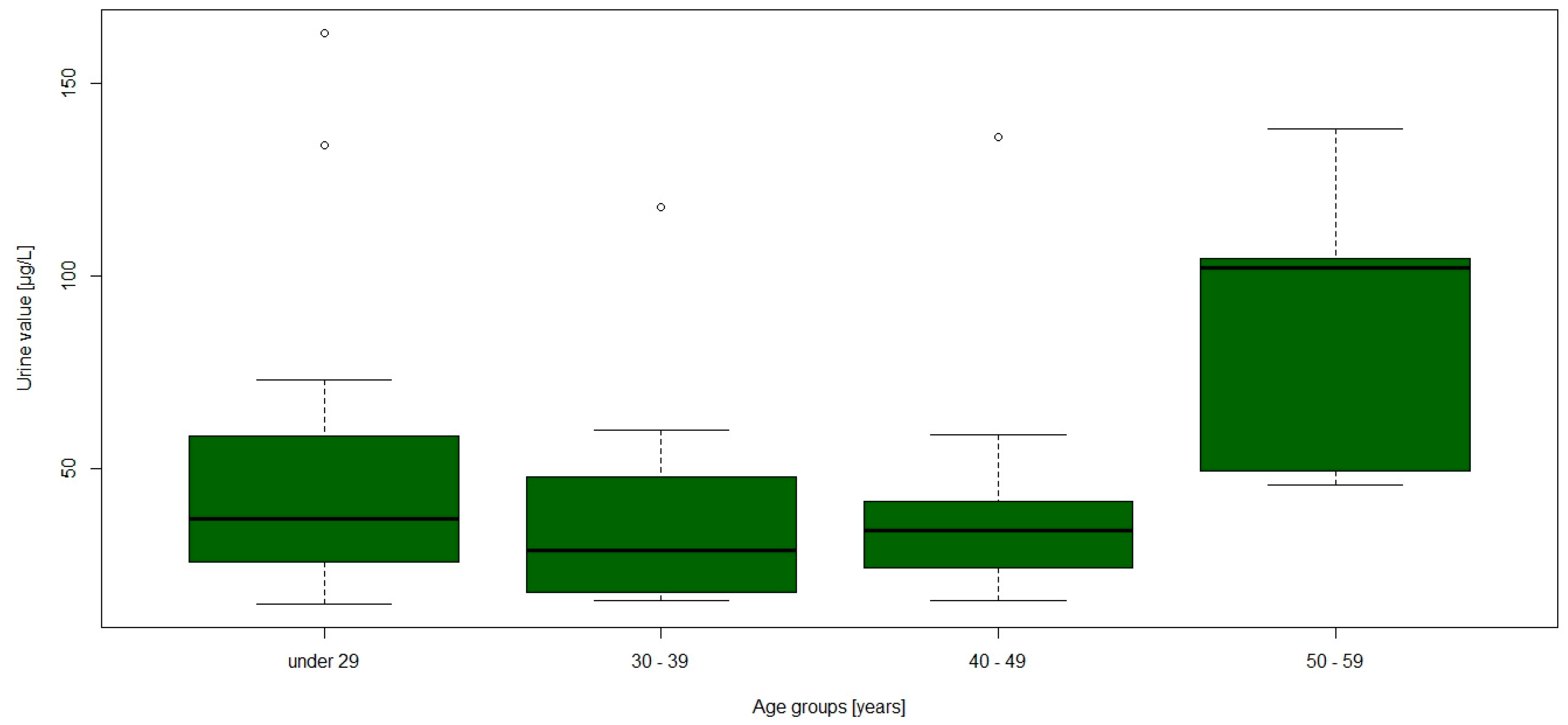
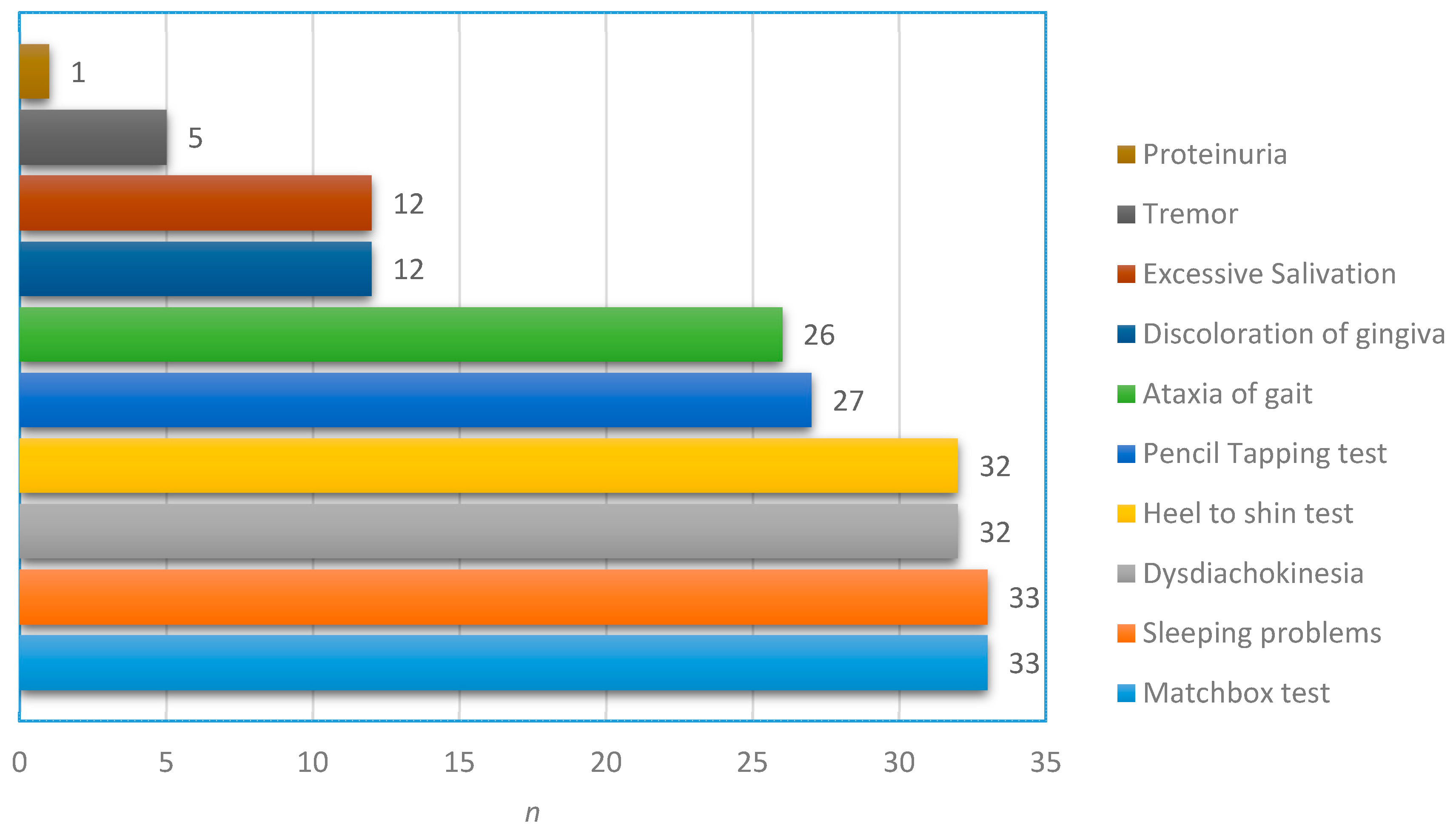
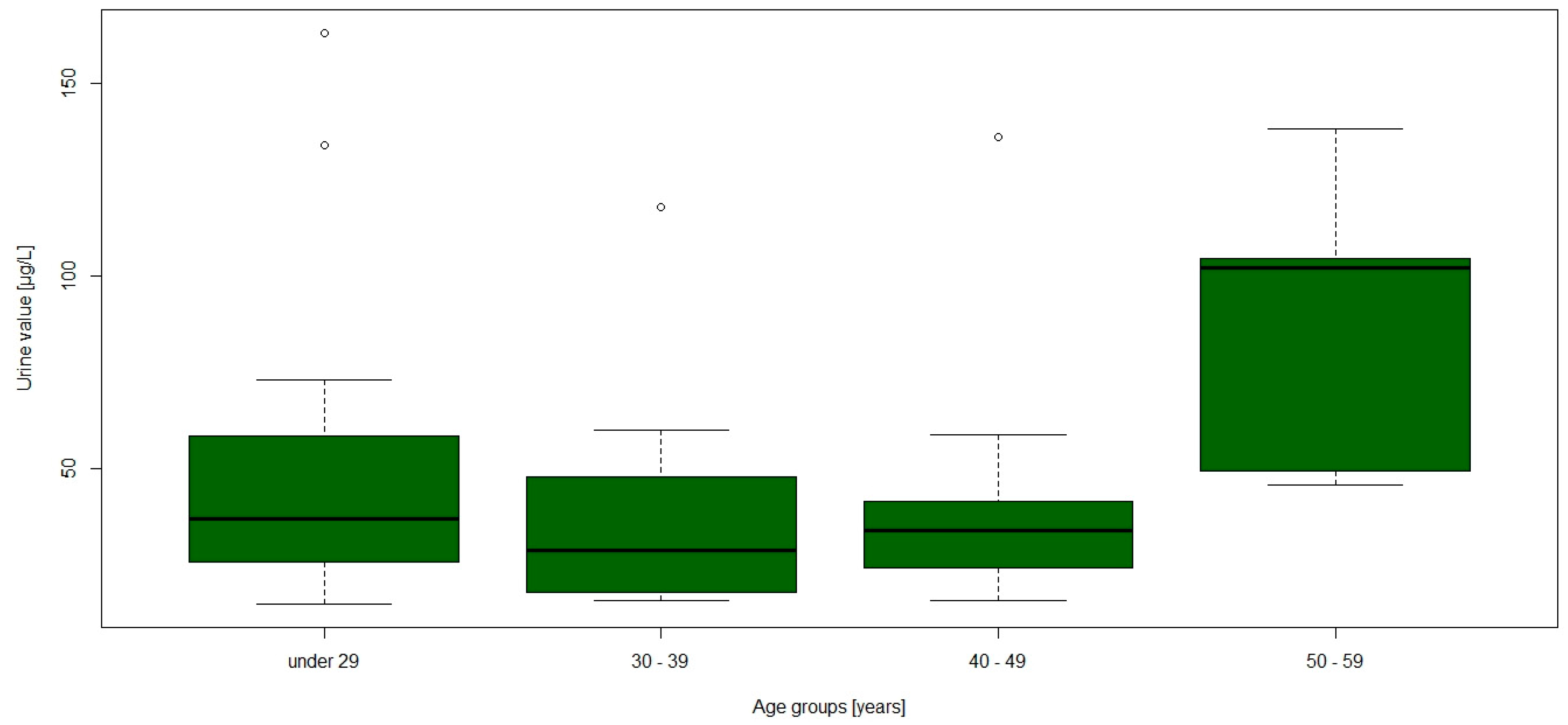
3.2. Population Characteristics and Medical Score Sum
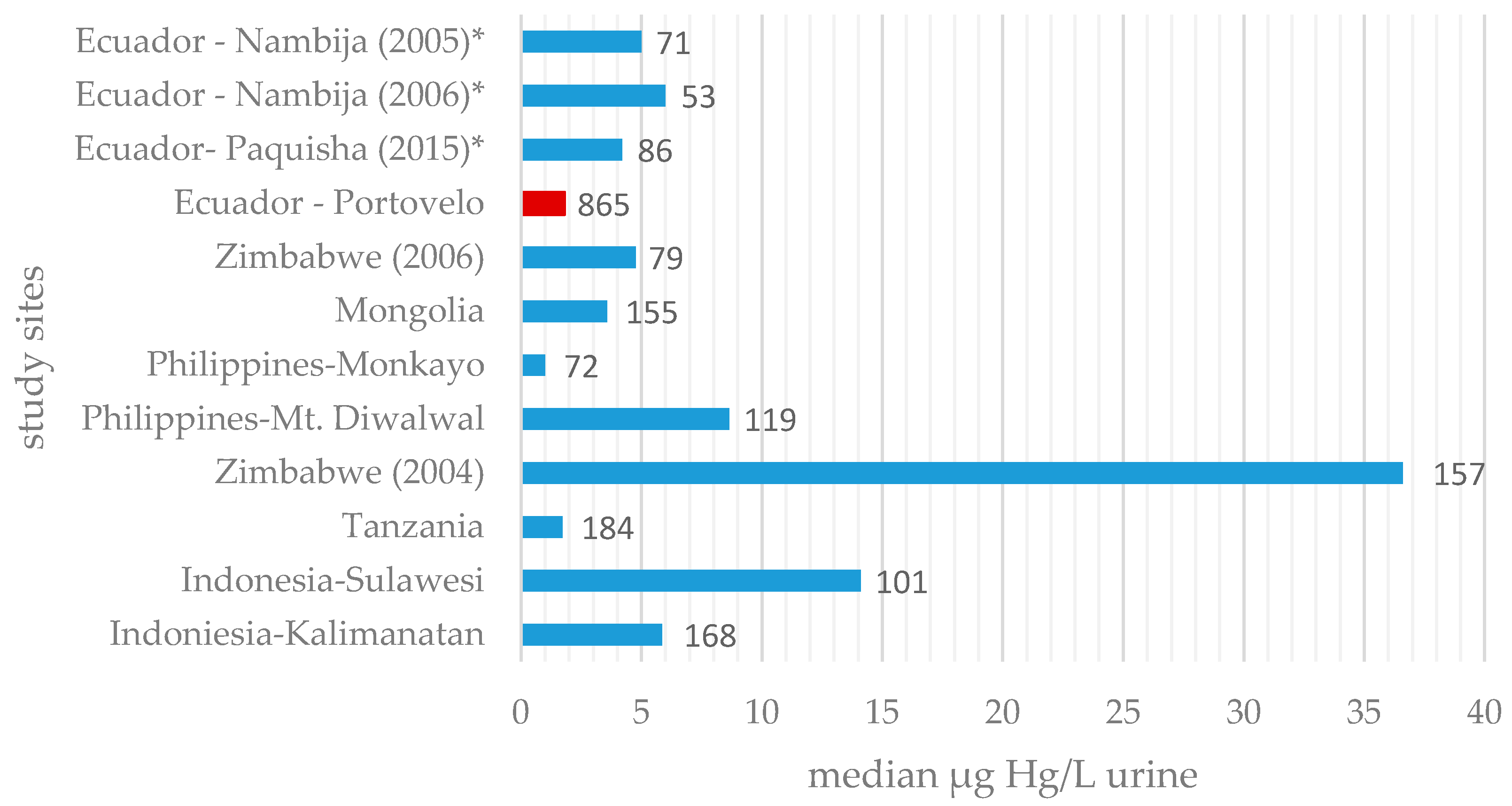
4. Discussion
4.1. The Mercury Ban and the Half-Life of Mercury
4.2. Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A. List of Exclusion Criteria
- History of any clinically significant disease or disorder which, in the opinion of the investigator, may either put the subjects at risk because of participation in the study, or influence the results or the subject’s ability to participate in the study.
- Known or a medical history of renal disorder, significant renal failure, or high risk of renal failure.
- Any clinically significant abnormalities in clinical chemistry or haematology results at the time of screening as judged by the investigator.
- Known or suspected neurodegenerative disorder including but not limited to stroke, polio, Parkinson’s and Alzheimer’s disease.
- Known or suspected drug or alcohol abuse.
- Positive pregnancy test in women.
- Serious bacterial and chronic viral infection such as human immunodeficiency virus (HIV) or hepatitis virus.
- History of severe allergy/hypersensitivity or on-going allergy/hypersensitivity, as judged by the investigator or history of hypersensitivity to drugs with a similar chemical structure or class to NBMI.
- History of allergy/hypersensitivity to bisulphites (e.g., red/white wine).
- Participation in any other clinical study that included drug treatment within three months of the first administration of investigational product.
- Use of other therapies for mercury intoxication including metal chelators within three months.
- Investigator considers subject unlikely to comply with study procedures, restrictions, and requirements.
Appendix B. Medical Score Sum Assessment Tool
| Parameter | Score |
| Anamnestic Data | |
| 1. Excessive salivation |
|
| 2. Tremor at work |
|
| 3. Sleeping problems at night |
|
| Clinical Data | |
| 4. Bluish discoloration of gingiva |
|
| 5. Ataxia of gait |
|
| 6. Dysdiadochokinesia |
|
| 7. Heel-to-shin test |
|
| 8. Proteinuria |
|
| Neuro-psychological tests | |
| 9. Match box test |__|__|__| s |
|
| 10. Pencil tapping test |__|__| taps |
|
| Medical Score Sum |__|__| | |
References
- United Nations Environment Programme (UNEP). A Practical Guide—Reducing Mercury Use in Artisanal and Small-Scale Gold Mining; UNEP: Geneva, Switzerland, 2011. [Google Scholar]
- Telmer, K.H.; Veiga, M.M. World Emissions of Mercury from Artisanal and Small Scale Gold Mining. In Mercury Fate and Transport in the Global Atmosphere. Emissions, Measurements and Models; Pirrone, N., Mason, R., Eds.; Springer: New York, NY, USA, 2009; pp. 131–172. [Google Scholar]
- United Nations Environment Programme (UNEP). The Global Mercury Assessment 2013: Sources, Emissions, Releases and Environmental Transport; Branch, U.C., Ed.; UNEP: Geneva, Switzerland, 2013. [Google Scholar]
- Spiegel, S.J.; Yassi, A.; Spiegel, J.M.; Veiga, M.M. Reducing mercury and responding to the global gold rush. Lancet 2005, 366, 2070–2072. [Google Scholar] [CrossRef]
- Bose-O’Reilly, S.; Drasch, G.; Beinhoff, C.; Rodrigues-Filho, S.; Roider, G.; Lettmeier, B.; Maydl, A.; Maydl, S.; Siebert, U. Health assessment of artisanal gold miners in Indonesia. Sci. Total Environ. 2010, 408, 713–725. [Google Scholar] [CrossRef] [PubMed]
- Bose-O’Reilly, S.; Drasch, G.; Beinhoff, C.; Tesha, A.; Drasch, K.; Roider, G.; Taylor, H.; Appleton, D.; Siebert, U. Health assessment of artisanal gold miners in Tanzania. Sci. Total Environ. 2010, 408, 796–805. [Google Scholar] [CrossRef] [PubMed]
- Counter, S.A.; Buchanan, L.H.; Ortega, F. Neurocognitive screening of mercury-exposed children of Andean gold miners. Int. J. Occup. Environ. Health 2006, 12, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Baeuml, J.; Bose-O’Reilly, S.; Gothe, R.M.; Lettmeier, B.; Roider, G.; Drasch, G.; Siebert, U. Human Biomonitoring Data from Mercury Exposed Miners in Six Artisanal Small-Scale Gold Mining Areas in Asia and Africa. Minerals 2011, 1, 122–143. [Google Scholar] [CrossRef]
- Steckling, N.; Boese-O’Reilly, S.; Gradel, C.; Gutschmidt, K.; Shinee, E.; Altangerel, E.; Badrakh, B.; Bonduush, I.; Surenjav, U.; Ferstl, P.; et al. Mercury exposure in female artisanal small-scale gold miners (ASGM) in Mongolia: An analysis of human biomonitoring (HBM) data from 2008. Sci. Total Environ. 2011, 409, 994–1000. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, A.K.; Thomsen, J.F.; Mikkelsen, S. A review of mercury exposure among artisanal small-scale gold miners in developing countries. Int. Arch. Occup. Environ. Health 2014, 87, 579–590. [Google Scholar] [CrossRef] [PubMed]
- Mining, Minerals and Sustainable Developement. MMSD South America Final Report—Minería y Minerales de América del Sur en la Transición al Desarrollo Sustentable; International Institute for Environment and Development: Santiago, Chile, 2002. [Google Scholar]
- United Nations Environment Programme (UNEP). Ecuador Case Study—Analysis of Formalization Approaches in the Artisanal and Small-Scale Gold Mining Sector Based on Experiences in Ecuador, Mongolia, Peru, Tanzania and Uganda; UNEP: Geneva, Switzerland, 2012. [Google Scholar]
- Veiga, M.M.; Angeloci, G.; Hitch, M.; Colon Velasquez-Lopez, P. Processing centres in artisanal gold mining. J. Clean. Prod. 2014, 64, 535–544. [Google Scholar] [CrossRef]
- Counter, S.A.; Buchanan, L.H.; Ortega, F. Mercury levels in urine and hair of children in an Andean gold-mining settlement. Int. J. Occup. Environ. Health 2005, 11, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Tarras-Wahlberg, N.H.; Flachier, A.; Fredriksson, G.; Lane, S.; Lundberg, B.; Sangfors, O. Environmental Impact of Small-scale and Artisanal Gold Mining in Southern Ecuador. AMBIO J. Hum. Environ. 2000, 29, 484–491. [Google Scholar] [CrossRef]
- Gonzalez-Carrasco, V.; Velasquez-Lopez, P.C.; Olivero-Verbel, J.; Pajaro-Castro, N. Air mercury contamination in the gold mining town of Portovelo, Ecuador. Bull. Environ. Contam. Toxicol. 2011, 87, 250–253. [Google Scholar] [CrossRef] [PubMed]
- Nichols, B.; Veiga, M.; van Zyl, D.; Xavier, A.M. Closure of Artisanal Small Scale Gold Mining Processing Plants in Ecuador. J. Manag. Sustain. 2015, 5. [Google Scholar] [CrossRef]
- Drasch, G.; Bose-O’Reilly, S.; Beinhoff, C.; Roider, G.; Maydl, S. The Mt. Diwata study on the Philippines 1999—Assessing mercury intoxication of the population by small scale gold mining. Sci. Total Environ. 2001, 267, 151–168. [Google Scholar] [CrossRef]
- Doering, S.; Bose-O’Reilly, S.; Berger, U. Essential indicators identifying chronic inorganic mercury intoxication: Pooled analysis across multiple cross-sectional studies. PLoS ONE 2016, 11, e0160323. [Google Scholar] [CrossRef] [PubMed]
- Baeuml, J.; Bose-O’Reilly, S.; Lettmeier, B.; Maydl, A.; Messerer, K.; Roider, G.; Drasch, G.; Siebert, U. Applicability of two mobile analysers for mercury in urine in small-scale gold mining areas. Int. J. Hyg. Environ. Health 2011, 215, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Schulz, C.; Angerer, J.; Ewers, U.; Kolossa-Gehring, M. The German Human Biomonitoring Commission. Int. J. Hyg. Environ. Health 2007, 210, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Ewers, U.; Krause, C.; Schulz, C.; Wilhelm, M. Reference values and human biological monitoring values for environmental toxins. Report on the work and recommendations of the Commission on Human Biological Monitoring of the German Federal Environmental Agency. Int. Arch. Occup. Environ. Health 1999, 72, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, R.; Volkamer, M. Motor Function Test for Children Aged Four to Six; Beltz Test Gesellschaft: Weinheim, Germany, 1987. [Google Scholar]
- Masur, H.; Papke, K.; Althoff, S.; Oberwittler, C.; Heil, U.; Hundenborn, S.; Nedjat, S.; Papke, H.; Speight, I.; Sträter, R.; et al. Scales and Scores in Neurology; Georg Thieme Verlag: Stuttgart, Germany, 2000. [Google Scholar]
- Wessely, S.; Powell, R. Fatigue syndrome. In Scales and Scores in Neurology; Masur, H., Papke, K., Althoff, S., Oberwittler, C., Heil, U., Hundenborn, S., Nedjat, S., Papke, H., Speight, I., Sträter, R., et al., Eds.; Georg Thieme Verlag: Stuttgart, Germany, 2000. [Google Scholar]
- Gonzalez-Merizalde, M.V.; Menezes-Filho, J.A.; Cruz-Erazo, C.T.; Bermeo-Flores, S.A.; Sanchez-Castillo, M.O.; Hernandez-Bonilla, D.; Mora, A. Manganese and Mercury Levels in Water, Sediments, and Children Living Near Gold-Mining Areas of the Nangaritza River Basin, Ecuadorian Amazon. Arch. Environ. Contam. Toxicol. 2016, 71, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Harari, R.; Forastiere, F.; Axelson, O. Unacceptable “occupational” exposure to toxic agents among children in Ecuador. Am. J. Ind. Med. 1997, 32, 185–189. [Google Scholar] [CrossRef]
- Harari, R.; Harari, F.; Gerhardsson, L.; Lundh, T.; Skerfving, S.; Stromberg, U.; Broberg, K. Exposure and toxic effects of elemental mercury in gold-mining activities in Ecuador. Toxicol. Lett. 2012, 213, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Gibb, H.; O’Leary, K.G. Mercury exposure and health impacts among individuals in the artisanal and small-scale gold mining community: A comprehensive review. Environ. Health Perspect. 2014, 122, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Ohlander, J.; Huber, S.M.; Schomaker, M.; Heumann, C.; Schierl, R.; Michalke, B.; Jenni, O.G.; Caflisch, J.; Munoz, D.M.; von Ehrenstein, O.S.; et al. Risk factors for mercury exposure of children in a rural mining town in northern Chile. PLoS ONE 2013, 8, e79756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boese-O’Reilly, S.; Baeuml, J.; Lettmeier, B.; Bernaudat, L.; Siebert, U.; Roider, G.; Nowak, D.; Drasch, G. Signs and symptoms of mercury exposed gold miners. Int. J. Occup. Med. Environ. Health 2015. accepted. [Google Scholar]
- Sallsten, G.; Barregard, L.; Schutz, A. Clearance half life of mercury in urine after the cessation of long term occupational exposure: Influence of a chelating agent (DMPS) on excretion of mercury in urine. Occup. Environ. Med. 1994, 51, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Nordberg, G.; Fowler, B.; Nordberg, M.; Friberg, L. Handbook of the Toxicology of Metals, 3rd ed.; Academic Press, Elsevier B.V.: New York, NY, USA, 2007. [Google Scholar]
- Normierung von Stoffgehalten im Urin—Kreatinin. In Bundesgesundheitsbl-Gesundheitsforsch-Gesundheitsschutz; German Federal Environment Agency: Berlin, Germany, 2005; Volume 48, p. 616.
- Hoet, P.; Deumer, G.; Bernard, A.; Lison, D.; Haufroid, V. Urinary trace element concentrations in environmental settings: Is there a value for systematic creatinine adjustment or do we introduce a bias? J. Expo. Sci. Environ. Epidemiol. 2016, 26, 296–302. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value (µg/L) |
|---|---|
| n | 865 |
| Minimum | <0.5 * |
| 1st Quartile | 0.7 |
| Median | 1.8 |
| 3rd Quartile | 5.4 |
| 95th Quantile | 28.0 |
| Maximum | 163.0 |
| Parameter | Urine-Hg (μg/L) | MSS | Years Working * | Years Living * |
|---|---|---|---|---|
| Minimum | 15.0 | 2.0 | 0.5 | 1.0 |
| 1st Quartile | 26.5 | 5.0 | 3.8 | 7.8 |
| Median | 35.0 | 6.0 | 9.0 | 22.0 |
| Mean | 50.8 | 5.9 | 11.2 | 22.2 |
| 3rd Quartile | 57.5 | 7.0 | 16.0 | 32.0 |
| Maximum | 163.0 | 8.0 | 40.0 | 54.0 |
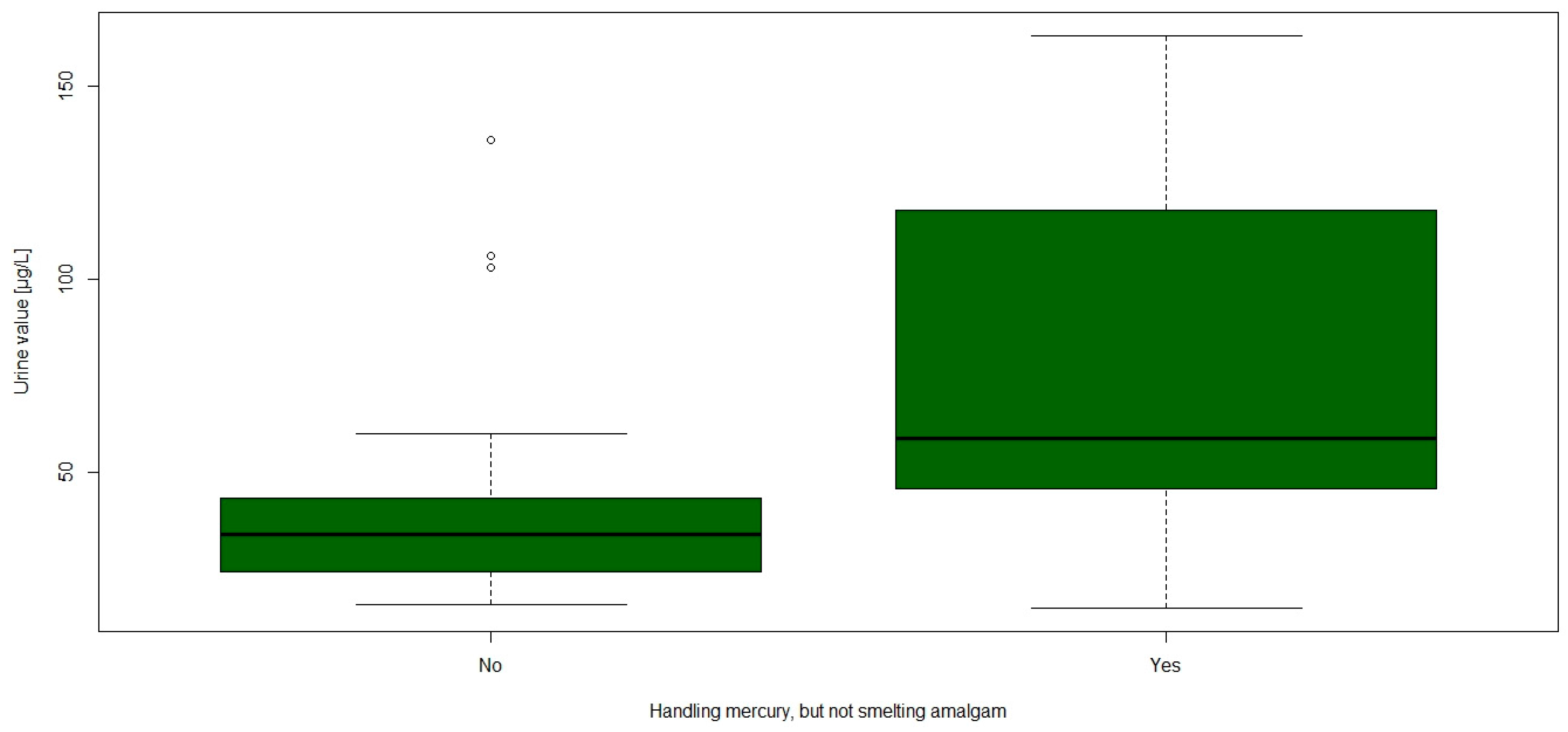
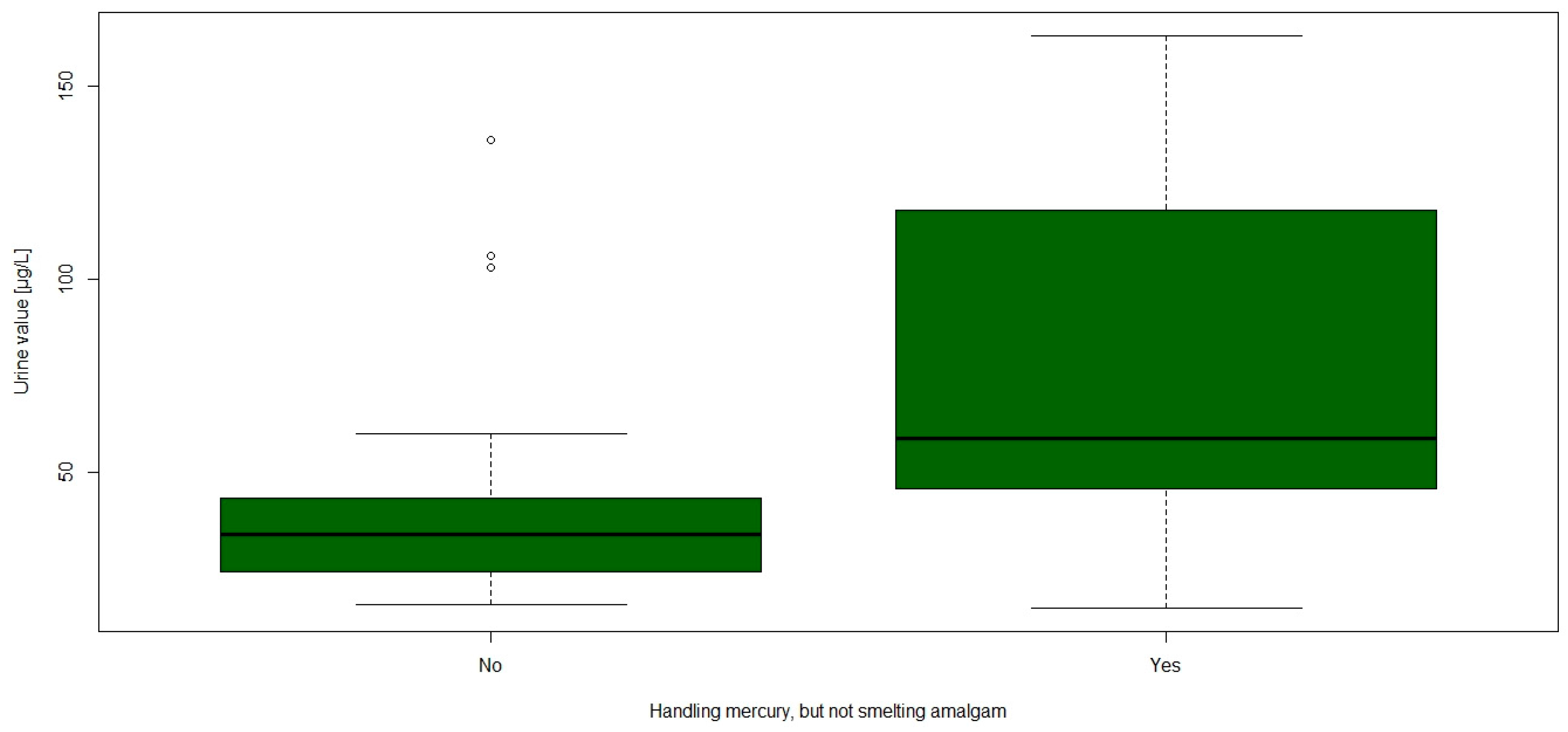
| Parameter | Another Job | Gold Buyer | Handling Only | Smelting |
|---|---|---|---|---|
| n | 3 | 4 | 13 | 37 |
| Urine | ||||
| Minimum | 16.0 | 16.0 | 15.0 | 15.0 |
| 1st Quartile | 23.0 | 25.8 | 46.0 | 27.0 |
| Median | 30.0 | 30.0 | 59.0 | 35.0 |
| 3rd Quartile | 51.5 | 57.3 | 118.0 | 50.0 |
| Maximum | 73.0 | 136.0 | 163.0 | 163.0 |
| W * | 73.5 | 93.5 | 106.5 | 149 |
| p-value | 0.592 | 0.595 | 0.015 | 0.542 |
| MSS | ||||
| Minimum | 5.0 | 4 | 5 | 2 |
| Median | 5 | 5.5 | 6 | 6 |
| Maximum | 5 | 7 | 7 | 8 |
| W * | 93 | 93.5 | 164 | 95 |
| p-value | 0.136 | 0.584 | 0.326 | 0.260 |
| Years working in the mining area | ||||
| Minimum | 3 | 0.5 | 1 | 0.5 |
| Median | 5 | 5.8 | 10 | 10 |
| Maximum | 14 | 16 | 20 | 40 |
| W * | 73.5 | 106 | 206.5 | 80 |
| p-value | 0.591 | 0.297 | 0.908 | 0.115 |
| Years living in the mining area | ||||
| Minimum | 6 | 1.5 | 3 | 1 |
| Median | 29 | 26 | 25 | 22 |
| Maximum | 32 | 42 | 54 | 54 |
| W * | 55 | 75 | 193 | 116 |
| p-value | 0.780 | 0.854 | 0.837 | 0.676 |
| Age | ||||
| Minimum | 29 | 32 | 25 | 19 |
| Mean | 32 | 39.8 | 39.9 | 39.3 |
| Maximum | 35 | 46 | 56 | 59 |
| W * | 86.5 | 73.5 | 179.5 | 82.5 |
| p-value | 0.253 | 0.806 | 0.580 | 0.135 |
| Fish consumption | ||||
| >1/week | 2 (66.7%) | 3 (75.0%) | 7 (53.8%) | 25 (67.6%) |
| Weight | ||||
| Minimum | 70 | 63 | 54.5 | 63 |
| Median | 87.5 | 74 | 78 | 77 |
| Maximum | 96 | 82 | 107 | 96 |
| W * | 60 | 111 | 258 | 95.5 |
| p-value | 0.963 | 0.213 | 0.150 | 0.282 |
| Amalgam fillings | ||||
| persons with AF | 0 | 0 | 0 | 7 (18.9%) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schutzmeier, P.; Berger, U.; Bose-O’Reilly, S. Gold Mining in Ecuador: A Cross-Sectional Assessment of Mercury in Urine and Medical Symptoms in Miners from Portovelo/Zaruma. Int. J. Environ. Res. Public Health 2017, 14, 34. https://doi.org/10.3390/ijerph14010034
Schutzmeier P, Berger U, Bose-O’Reilly S. Gold Mining in Ecuador: A Cross-Sectional Assessment of Mercury in Urine and Medical Symptoms in Miners from Portovelo/Zaruma. International Journal of Environmental Research and Public Health. 2017; 14(1):34. https://doi.org/10.3390/ijerph14010034
Chicago/Turabian StyleSchutzmeier, Paul, Ursula Berger, and Stephan Bose-O’Reilly. 2017. "Gold Mining in Ecuador: A Cross-Sectional Assessment of Mercury in Urine and Medical Symptoms in Miners from Portovelo/Zaruma" International Journal of Environmental Research and Public Health 14, no. 1: 34. https://doi.org/10.3390/ijerph14010034