
Assessment of Food Safety Knowledge, Attitude, Self-Reported Practices, and Microbiological Hand Hygiene of Food Handlers


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Sampling Plan
2.2. Questionnaire Collection
2.3. Hand Hygiene Assessment
2.3.1. Sample Collection
2.3.2. Sample Enrichment and Enumeration by Plate Count Method
2.3.3. Detection and Enumeration of Salmonella spp., V. cholerae and V. parahaemolyticus Enumeration by Polymerase Chain Reaction (PCR)
2.4. Statistical Analysis
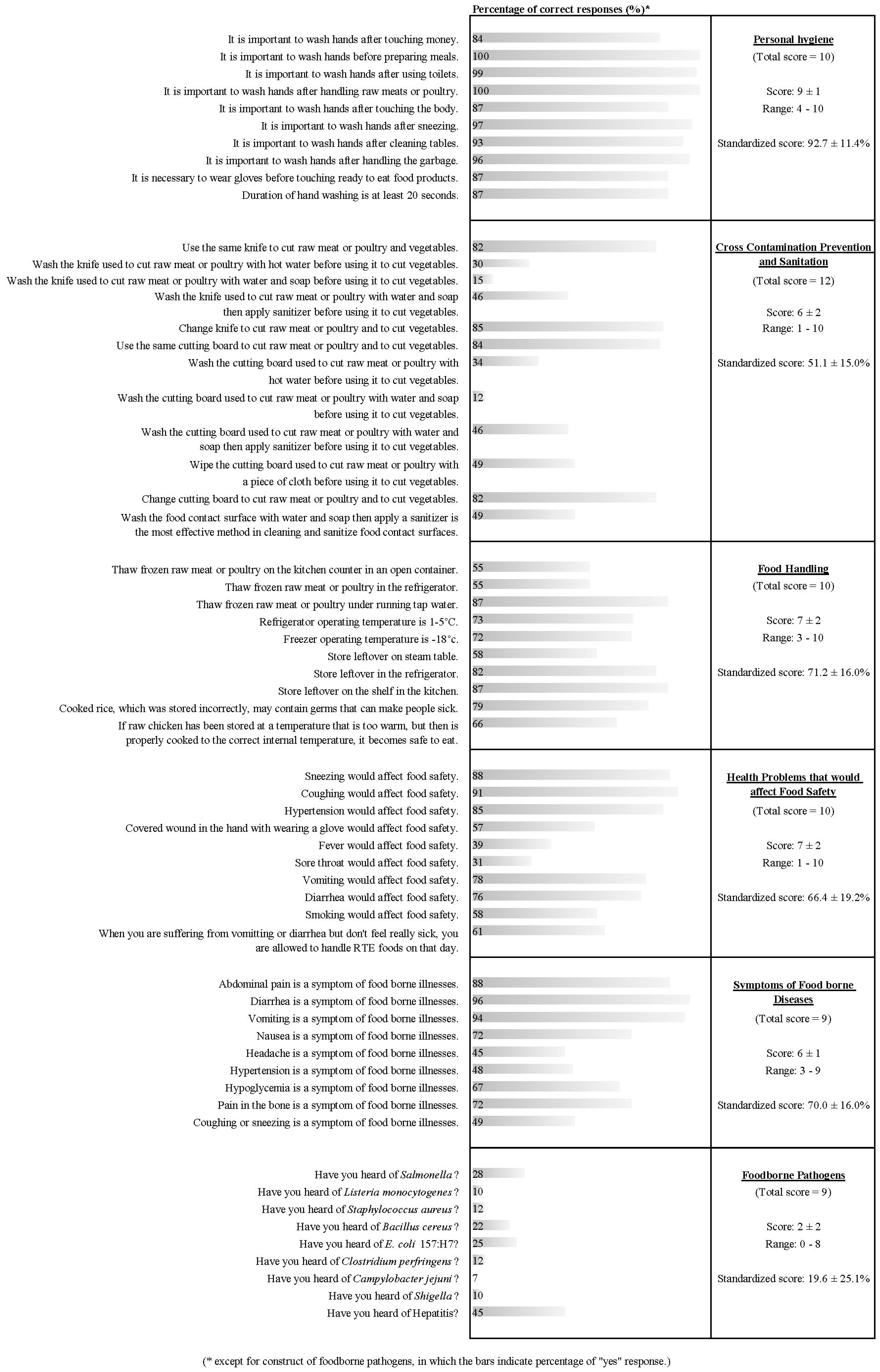
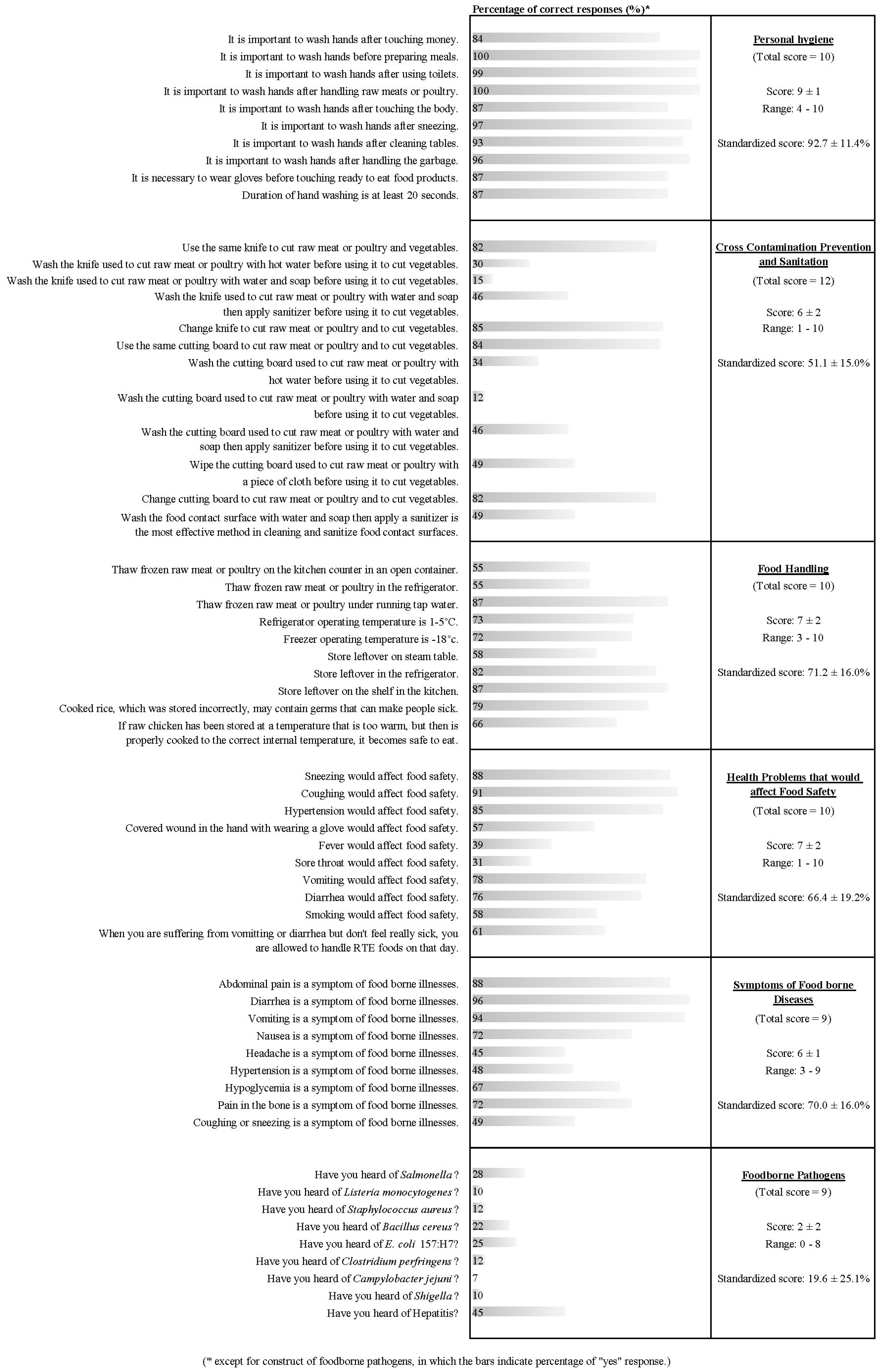
3. Results
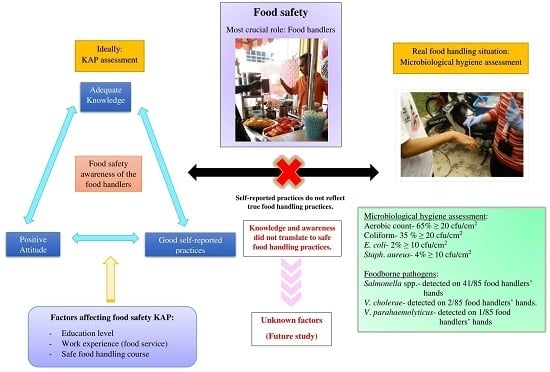
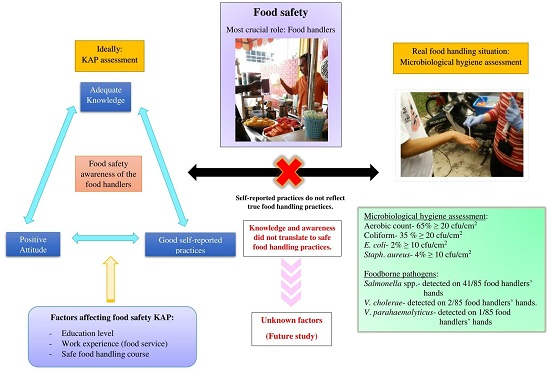
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization (WHO). Food Safety; WHO: Geneva, Switzerland, 2015; Available online: http://www.who.int/mediacentre/factsheets/fs399/en/ (accessed on 19 October 2016).
- Ministry of Health (MOH). Health Facts 2014; MOH: Putrajaya, Malaysia, 2014.
- Ministry of Health (MOH). Annual Report 2007; MOH: Putrajaya, Malaysia, 2007.
- Ministry of Health (MOH). The National Level 2014 Clean, Safe and Healthy Canteen Award; Department of Food Safety and Food Quality, Ed.; MOH: Putrajaya, Malaysia, 2014.
- Ministry of Health (MOH). Annual Report 2010; MOH: Putrajaya, Malaysia, 2012.
- Michaels, B.; Keller, C.; Belvins, M.; Paoli, G.; Ruthman, T.; Todd, E.; Griffith, C.J. Prevention of food worker transmission of foodborne pathogens: Risk assessment and evaluation of effective hygiene intervention strategies. Food Serv. Technol. 2004, 4, 31–49. [Google Scholar] [CrossRef]
- Lunestad, B.T.; Borlaug, K. Persistence of Salmonella enterica serovar agona in oil or fish feed production. J. Aquacult. Feed Sci. Nutr. 2009, 1, 73–77. [Google Scholar]
- Olsen, S.J.; Hansen, G.R.; Bartlett, L.; Fitzgerald, L.; Sonder, A.; Manjrekar, R.; Riggs, T.; Kim, J.; Flahart, R.; Pezzin, G.; et al. An outbreak of Campylobacter jejuni infection associated with food handler contamination; the use of pulsed-field gel electrophoresis. J. Infect. Dis. 2001, 183, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Quiroz, E.S.; Bern, C.; MacArthur, J.R.; Xiao, L.; Fletcher, M.; Arrowood, M.J.; Shay, D.K.; Levy, M.E.; Glass, R.I.; Lal, A. An outbreak of cryptosporidiosis linked to a food handler. J. Infect. Dis. 2000, 181, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Angelillo, I.F.; Viggiani, N.M.; Rizzo, L.; Bianco, A. Food handlers and foodborne diseases: Knowledge, attitudes, and reported behavior in Italy. J. Food Prot. 2000, 63, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Scarborough, M.F. Hand Washing in Georgia’s Public Schools—A Community Needs Assessment and Intervention Study. Master’s Thesis, Emory University, Atlanta, GA, USA, May 2002. [Google Scholar]
- Curtis, V.; Cairncross, S. Effect of washing hands with soap on diarrhea risk in the community: A systemic review. Lancet Infect. Dis. 2003, 3, 275–281. [Google Scholar] [CrossRef]
- World Health Organization. World Health Organization. Evidence of hand hygiene to reduce transmission and infections by multidrug resistant organisms in health-care settings. In WHO Guidelines on Hand Hygiene in Health Care; Clean Care is Safer Care Team, Ed.; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Gibson, L.L.; Rose, J.B.; Haas, C.N.; Gerba, C.P.; Rusin, P.A. Quantitative assessment of risk reduction from hand washing with antibacterial soaps. J. Appl. Microbiol. 2002, 92 (Suppl. S1), 136S–143S. [Google Scholar] [CrossRef] [PubMed]
- Chinakwe, E.C.; Nwogwugwu, N.U.; Nwachukwu, I.N.; Okorondu, S.I.; Onyemekara, N.N.; Ndubuisi-Nnaji, U.U. Microbial quality and public health implications of hand-wash water samples of public adults in Owerri, South-east Nigeria. Int. Res. J. Microbiol. 2013, 3, 144–146. [Google Scholar]
- Soares, L.S.; Almeida, R.C.C.; Cerqueira, E.S.; Carvalho, J.S.; Nunes, I.L. Knowledge, attitudes and practices in food safety and the presence of coagulase-positive staphylococci on hands of food handlers in the schools of Camaçari, Brazil. Food Control 2012, 27, 206–213. [Google Scholar] [CrossRef]
- Perez-Rodriguez, F.; Valero, A.; Carrasco, E.; Garcia, R.M.; Zurera, G. Understanding and modelling bacterial transfer to foods: A review. Trends Food Sci. Technol. 2008, 19, 131–144. [Google Scholar] [CrossRef]
- Noor-Azira, A.-M.; Mohammad-Faid, A.-R.; Shuhaimi, M.; Syafinaz, A.-N.; Hamat, A.H.R.A.; Malina, O. Knowledge, attitude and practices regarding food hygiene and sanitation of food handlers in Kuala Pilah, Malaysia. Food Control 2012, 27, 289–293. [Google Scholar]
- Norrakiah, A.S.; Siow, O.N. Knowledge, attitudes and practices of food handlers on food safety in food service operations at the Universiti Kebangsaan Malaysia. Food Control 2014, 37, 210–217. [Google Scholar]
- Rosnani, A.H.; Son, R.; Mohhidin, O.; Toh, P.S.; Chai, L.C. Assessment of knowledge, attitude and practices concerning food safety among restaurant workers in Putrajaya, Malaysia. Food Sci. Qual. Manag. 2014, 32, 20–27. [Google Scholar]
- Ministry of Health (MOH). Health Facts 2013; MOH: Putrajaya, Malaysia, 2013. Available online: http://vlib.moh.gov.my/cms/content.jsp?id=com.tms.cms.section.Section_3549ea8f-c0a81049-874bd300-302e756b (accessed on 3 May 2015).
- Osaili, T.M.; Jamous, D.O.A.; Obeidat, B.A.; Bawadi, H.A.; Tayyem, R.F. Food safety knowledge among food workers in restaurants in Jordan. Food Control 2013, 31, 145–150. [Google Scholar] [CrossRef]
- Pichler, J.; Ziegler, J.; Aldrian, U.; Allerberger, F. Evaluating levels of knowledge on food safety among food handlers from restaurants and various catering businesses in Vienna, Austria 2011/2012. Food Control 2014, 35, 33–40. [Google Scholar] [CrossRef]
- Lee, J.Y.; Choi, J.W.; Kim, H. Determination of hand surface area by sex and body shape using alginate. J. Physiol. Anthropol. 2007, 26, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.L.; Lee, H.Y.; Abu Bakar, F.; Abdul Karim, M.S.; Rukayadi, Y.; Mahyudin, N.A. Microbiological quality on food handlers’ hands at primary schools in Hulu Langat district, Malaysia. Int. Food Res. J. 2013, 20, 2973–2977. [Google Scholar]
- Sneed, J.; Strohbehn, C.; Gilmore, S.A.; Mendonca, A. Microbiological evaluation of foodservice contact surfaces in Iowa assisted-living facilities. J. Am. Diet. Assoc. 2004, 104, 1722–1724. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, J.; Sota, M.; Vivanco, A.; Perales, I.; Cisterna, R.; Rementeria, A.; Garaizar, J. Development of a multiplex PCR technique for detection and epidemiological typing of Salmonella in human clinical samples. J. Clin. Microbiol. 2004, 42, 1734–1738. [Google Scholar] [CrossRef]
- Teh, C.S.J.; Chua, K.H.; Thong, K.L. Simultaneous differential detection of human pathogenic and non-pathogenic Vibrio species using a multiplex PCR based on gyrB and pntA genes. J. Appl. Microbiol. 2010, 108, 1940–1945. [Google Scholar] [PubMed]
- Saad, M.; Toh, P.S.; Adil, M.A.M. Hygiene practices of food handlers at Malaysian government institutions training centers. Procedia Soc. Behav. Sci. 2013, 85, 118–127. [Google Scholar] [CrossRef]
- Liu, S.; Liu, Z.; Zhang, H.; Lu, L.; Liang, J.; Huang, Q. Knowledge, attitude and practices of food safety amongst food handlers in the coastal resort of Guangdong, China. Food Control 2015, 47, 457–461. [Google Scholar] [CrossRef]
- McIntyre, L.; Vallaster, L.; Wilcott, L.; Henderson, S.; Kosatsky, T. Evaluation of food safety knowledge, attitudes and self-reported hand washing practices in foodsafe trained and untrained food handlers in British Columbia, Canada. Food Control 2013, 30, 150–156. [Google Scholar] [CrossRef]
- Lynch, R.A.; Elledge, B.L.; Griffith, C.C.; Boatright, D.T. A comparison of food safety knowledge among restaurant managers, by source of training and experience, in Oklahoma County, Oklahoma. J. Environ. Health 2003, 66, 9–14. [Google Scholar] [PubMed]
- Toh, P.S.; Birchenough, A. Food safety knowledge and attitudes: Culture and environment impact on hawkers in Malaysia. Knowledge and attitudes are key attributes of concern in hawker food handling practices and outbreaks of food poisoning and their prevention. Food Control 2000, 11, 447–452. [Google Scholar] [CrossRef]
- Todd, E.C.; Greig, J.D.; Batleson, C.A.; Michaels, B.S. Outbreaks where food workers have been implicated in the spread of foodborne disease. Part 3. Factors contributing to outbreaks and description of outbreak categories. J. Food Prot. 2007, 70, 2199–2217. [Google Scholar] [CrossRef] [PubMed]
- Ackerley, L. Consumer awareness of food hygiene and food poisoning. Environ. Health 1994, 102, 69–74. [Google Scholar]
- Curtis, V.; Cousens, S.; Mentens, T.; Kenki, B.; Diallo, I. Structured observations of hygiene behaviours in Burkira Faso: Validity, variability and utility. Bull. World Health Organ. 1993, 71, 23–32. [Google Scholar] [PubMed]
- Pinfold, J.V. Analysis of different communication channels for promoting hygiene behavior. Health Educ. Res. 1999, 14, 629–639. [Google Scholar] [CrossRef] [PubMed]
- Worsfold, D.; Griffth, C.; Worsfold, P. A survey of environmental health officers’ views of food hygiene training. Br. Food J. 2004, 106, 51–64. [Google Scholar] [CrossRef]
- Seaman, P.; Eves, A. Perceptions of hygiene training amongst food handlers, managers and training providers—A qualitative study. Food Control 2010, 21, 1037–1041. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | Item | Number | Percentage (%) |
|---|---|---|---|
| Gender | Male | 27 | 40.3 |
| Female | 40 | 59.7 | |
| Age | <21 years old | 5 | 7.5 |
| 21–41 years old | 43 | 64.2 | |
| >41 years old | 19 | 28.4 | |
| Nationality | Malaysian | 26 | 38.8 |
| Foreigner | 41 | 61.2 | |
| Marital Status | Single | 14 | 20.9 |
| Married | 49 | 73.1 | |
| Divorce | 4 | 6.0 | |
| Education level | No formal education | 11 | 16.4 |
| Primary school | 7 | 10.5 | |
| Secondary school | 37 | 55.2 | |
| College/University | 12 | 17.9 | |
| Work experience | <2 years | 31 | 46.3 |
| 2–4 years | 16 | 23.9 | |
| 5–6 years | 9 | 13.4 | |
| >6 years | 11 | 16.4 | |
| Job responsibility | Cooking | 35 | 52.3 |
| Cleaning and washing dishes | 3 | 4.5 | |
| Serving food | 17 | 25.4 | |
| Preparation of food ingredients | 4 | 6.0 | |
| Others (cashier, manager, etc.) | 8 | 11.9 | |
| Did you attend the Safe Food Handling course? | No | 17 | 25.4 |
| Yes | 50 | 74.6 | |
| When did you attend the Safe Food Handling course? | Never attend before | 17 | 25.4 |
| ≤3 years ago | 29 | 43.3 | |
| >3 years ago | 21 | 31.3 | |
| Total | 67 | 100 | |
| Item | Mean | SD | Min | Max | |
|---|---|---|---|---|---|
| Self-improvement | |||||
| I would read more journals about food safety in order to enhance my food sanitation knowledge. | 3.5 | 0.9 | 1.0 | 4.0 | |
| I think by attending a sanitation seminar, it would increase my sanitation knowledge and ideas. | 3.9 | 0.4 | 1.0 | 4.0 | |
| I would attend a cooking or service competition to improve my professional knowledge. | 3.2 | 1.2 | 1.0 | 4.0 | |
| I would attend food safety seminar to gain more food safety knowledge. | 3.8 | 0.5 | 1.0 | 4.0 | |
| I think I do not need to attend food safety seminar because I think I have sufficient knowledge about food safety. | 1.6 | 1.6 | 1.0 | 4.0 | |
| Food safety concern | |||||
| Food handlers are responsible to prevent food poisoning. | 3.9 | 0.5 | 1.0 | 4.0 | |
| Government is responsible to prevent food poisoning. | 3.2 | 1.3 | 1.0 | 4.0 | |
| University is responsible to prevent food poisoning. | 3.3 | 1.2 | 1.0 | 4.0 | |
| Consumers are responsible to prevent food poisoning. | 3.4 | 1.1 | 1.0 | 4.0 | |
| Maintaining a clean cooking environment is a good way to control food safety. | 4.0 | 0.3 | 2.0 | 4.0 | |
| Self-checking of food safety is important to restaurants and institutions. | 3.8 | 0.4 | 2.0 | 4.0 | |
| Food safety is more important than taste. | 3.8 | 0.4 | 2.0 | 4.0 | |
| Food safety knowledge is important to ensure food is prepared in a safe manner. | 3.9 | 0.5 | 1.0 | 4.0 | |
| Food poisoning is not a serious matter. | 1.7 | 1.3 | 1.0 | 4.0 | |
| Item | Mean | SD | Min | Max |
|---|---|---|---|---|
| Do you wash your hands before touching unwrapped raw foods? | 4.6 | 0.8 | 1.0 | 5.0 |
| Do you wash your hands after touching unwrapped raw foods? | 4.6 | 0.9 | 1.0 | 5.0 |
| Do you use gloves when you touch or distribute unwrapped foods? | 4.3 | 1.2 | 1.0 | 5.0 |
| Do you use protective clothing (apron) when you touch or distribute unwrapped foods? | 4.6 | 1.0 | 1.0 | 5.0 |
| Do you use mask when you touch or distribute unwrapped foods? | 2.8 | 1.5 | 1.0 | 5.0 |
| Do you use cap when you touch or distribute unwrapped foods? | 4.5 | 1.2 | 1.0 | 5.0 |
| Do you use different chopping board for raw meat and fresh produce (vegetables and fruit)? | 4.3 | 1.1 | 1.0 | 5.0 |
| Do you wash and sanitise the working clothes? | 4.8 | 0.6 | 1.0 | 5.0 |
| Do you use a different cloth or towel to dry plates? | 4.6 | 1.0 | 1.0 | 5.0 |
| Do you wash and sanitise the knife after chopping raw chicken or meat? | 4.8 | 0.4 | 4.0 | 5.0 |
| Do you use clean and washed plate for ready-to-eat foods? | 4.9 | 0.3 | 4.0 | 5.0 |
| Do you work when you are sick (flu, cold, diarrhoea, coughing, etc.)? | 4.3 | 1.1 | 1.0 | 5.0 |
| Construct | Education Level | Work Experience | Did You Attend the Safe Food Handling Course? | When Did You Attend the Safe Food Handling Course? | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No Formal Education | Primary School | Secondary School | College/University | ≤2 Years | 2–4 Years | 5–6 Years | >6 Years | No | Yes | Never Attended | ≤3 Years Ago | >3 Years Ago | |
| (n = 11) | (n = 7) | (n = 37) | (n = 12) | (n = 31) | (n = 16) | (n = 9) | (n = 11) | (n = 17) | (n = 50) | (n = 17) | (n = 29) | (n = 21) | |
| Knowledge (%) | |||||||||||||
| Personal hygiene | 95.5 a | 87.1 a | 94.3 a | 88.3 a | 92.3 a | 91.3 a | 94.4 a | 94.6 a | 90.0 a | 93.6 a | 90.0 a | 94.8 a | 91.9 a |
| Cross contamination prevention and sanitation | 49.2 a | 60.7 a | 49.8 a | 53.5 a | 50.5 a | 53.1 a | 50.9 a | 52.3 a | 48.0 a | 52.7 a | 48.0 a | 53.5 a | 51.6 a |
| Food handling | 66.4 a,b | 52.9 a | 75.1 b | 74.2 b,c | 73.2 a,b | 61.3 a | 66.7 a,b | 83.6 b | 73.5 a | 70.4 a | 73.5 a | 68.3 a | 73.3 a |
| Health problems that would affect food safety | 62.7 a | 54.3 a | 69.2 a | 68.3 a | 61.9 a | 63.1 a | 73.3 a | 78.2 a | 72.9 a | 64.2 a | 72.9 a | 60.0 a | 70.0 a |
| Symptoms of foodborne diseases | 78.8 a | 66.7 a | 66.1 a | 75.9 a | 66.7 a | 72.2 a | 70.4 a | 75.8 a | 66.0 a | 71.3 a | 66.0 a | 68.6 a | 75.1 a |
| Foodborne pathogens | 6.1 a | 25.4 a,b | 16.2 a | 38.9 b | 14.7 a | 19.4 a | 19.8 a | 33.3 a | 4.6 a | 24.7 b | 4.6 a | 23.8 b | 25.9 b |
| Overall knowledge score | 60.0 a | 58.3 a | 62.1 a | 66.4 a | 60.2 a | 60.3 a | 62.8 a,b | 69.5 b | 59.6 a | 63.0 a | 59.6 a | 61.7 a | 64.7 a |
| Food safety attitude | |||||||||||||
| Self-improvement | 3.5 a,b | 3.5 a,b | 3.7 a | 3.3 b | 3.6 a | 3.5 a | 3.5 a | 3.9 a | 3.6 a | 3.6 a | 3.6 a | 3.6 a | 3.5 a |
| Food safety concern | 3.5 a | 3.6 a | 3.4 a | 3.5 a | 3.4 a | 3.5 a | 3.5 a | 3.4 a | 3.1 a | 3.5 b | 3.1 a | 3.5 b | 3.5 b |
| Overall attitude score | 3.5 a | 3.6 a | 3.5 a | 3.4 a | 3.4 a | 3.5 a | 3.5 a | 3.6 a | 3.3 a | 3.5 b | 3.3 a | 3.6 b | 3.5 a,b |
| Self-reported practices | |||||||||||||
| Overall practices score | 4.3 a | 4.2 a | 4.2 a | 4.0 a | 4.3 a | 4.2 a | 4.0 a | 4.3 a | 4.3 a | 4.2 a | 4.3 a | 4.2 a | 4.1 a |
| Microbial Indicator | Status | Number | Percentage (%) | Min a (CFU/cm2) | Max a (CFU/cm2) |
| Aerobic count b | |||||
| >Threshold | 55 | 65 | 23 | >29 | |
| <Threshold | 30 | 35 | <1 | 19 | |
| Coliform c | |||||
| >Threshold | 30 | 35 | 20 | >29 | |
| <Threshold | 55 | 65 | <1 | 17 | |
| E. coli d | |||||
| >Threshold | 2 | 2 | 12 | 13 | |
| <Threshold | 83 | 98 | n.d. | 8 | |
| S. aureus e | |||||
| >Threshold | 3 | 4 | 11 | >29 | |
| <Threshold | 82 | 96 | n.d. | 5 | |
| Foodborne Pathogens | Presence | Number | Percentage (%) | MPNmin per Person f | MPNmax per Person f |
| Salmonella | |||||
| Detected | 41 | 48 | 3 | 150 | |
| Not detected | 44 | 52 | <3 | n.a. | |
| V. cholerae | |||||
| Detected | 2 | 2 | 3 | n.a. | |
| Not detected | 83 | 98 | <3 | n.a. | |
| V. parahaemolyticus | |||||
| Detected | 1 | 1 | 23 | n.a. | |
| Not detected | 84 | 99 | <3 | n.a. |
| Item | Aerobic Count a | Coliforms a | E. coli b | S. aureus a | Salmonella | ||||
|---|---|---|---|---|---|---|---|---|---|
| >Threshold (n = 27) | <Threshold (n = 14) | >Threshold (n = 15) | <Threshold (n = 26) | <Threshold (n = 41) | >Threshold (n = 2) | <Threshold (n = 39) | >Threshold (n = 24) | <Threshold (n = 17) | |
| Do you wash your hands before touching unwrapped raw foods? | 4.7 ± 0.5 | 4.1 ± 0.9 | 4.7 ± 0.5 | 4.4 ± 0.9 | 4.5 ± 0.7 | 5.0 ± 0.0 | 4.5 ± 0.8 | 4.7 ± 0.6 | 4.4 ± 0.8 |
| Do you wash your hands after touching unwrapped raw foods? | 4.6 ± 1.0 | 4.6 ± 0.9 | 4.4 ± 1.2 | 4.6 ± 0.8 | 4.6 ± 1.0 | 5.0 ± 0.0 | 4.5 ± 1.0 | 4.4 ± 1.2 | 4.6 ± 0.8 |
| Do you use gloves when you touch or distribute unwrapped foods? | 4.3 ± 1.2 | 3.9 ± 1.2 | 4.7 ± 0.7 | 3.9 ± 1.4 | 4.2 ± 1.2 | 5.0 ± 0.0 | 4.2 ± 1.2 | 4.2 ± 1.4 | 4.2 ± 1.1 |
| Do you use protective clothing (apron) when you touch or distribute unwrapped foods? | 4.4 ± 1.2 | 4.6 ± 0.7 | 4.1 ± 1.5 | 4.7 ± 0.7 | 4.5 ± 1.1 | 5.0 ± 0.0 | 4.5 ± 1.1 | 4.3 ± 1.2 | 4.6 ± 1.0 |
| Do you use mask when you touch or distribute unwrapped foods? | 2.6 ± 1.4 | 2.5 ± 1.2 | 3.1 ± 1.5 | 2.3 ± 1.1 | 2.6 ± 1.3 | 3.5 ± 0.7 | 2.5 ± 1.3 | 2.6 ± 1.4 | 2.8 ± 1.3 |
| Do you use cap when you touch or distribute unwrapped foods? | 4.7 ± 1.1 | 4.6 ± 1.1 | 4.7 ± 1.0 | 4.7 ± 1.1 | 4.7 ± 1.1 | 5.0 ± 0.0 | 4.6 ± 1.1 | 4.2 ± 1.6 | 4.9 ± 0.3 |
| Do you use different chopping board for raw meat and fresh produce (vegetables and fruit)? | 4.3 ± 1.2 | 4.0 ± 0.9 | 4.4 ± 1.2 | 4.1 ± 1.1 | 4.2 ± 1.1 | 5.0 ± 0.0 | 4.2 ± 1.1 | 4.5 ± 0.8 | 4.2 ± 1.1 |
| Do you wash and sanitise the working clothes? | 4.9 ± 0.3 | 4.4 ± 1.1 | 5.0 ± 0.0 | 4.6 ± 0.9 | 4.7 ± 0.7 | 5.0 ± 0.0 | 4.7 ± 0.7 | 4.8 ± 0.4 | 4.6 ± 0.9 |
| Do you use a different cloth or towel to dry plates? | 4.5 ± 1.2 | 4.3 ± 1.1 | 4.7 ± 1.0 | 4.3 ± 1.2 | 4.4 ± 1.2 | 5.0 ± 0.0 | 4.4 ± 1.2 | 4.6 ± 0.9 | 4.5 ± 1.1 |
| Do you wash and sanitise the knife after chopping raw chicken or meat? | 4.9 ± 0.3 | 4.4 ± 0.5 | 4.9 ± 0.3 | 4.7 ± 0.5 | 4.8 ± 0.4 | 5.0 ± 0.0 | 4.8 ± 0.4 | 4.8 ± 0.4 | 4.7 ± 0.5 |
| Do you use clean and washed plate for RTE foods? | 4.9 ± 0.3 | 4.9 ± 0.3 | 4.9 ± 0.3 | 4.9 ± 0.3 | 4.9 ± 0.3 | 5.0 ± 0.0 | 4.9 ± 0.3 | 4.9 ± 0.3 | 4.9 ± 0.3 |
| Do you work when you are sick (flu, cold, diarrhoea, coughing, etc.)? | 4.3 ± 1.2 | 3.6 ± 1.1 | 4.5 ± 0.7 | 3.8 ± 1.3 | 4.0 ± 1.2 | 3.0 ± 2.8 | 4.1 ± 1.1 | 4.2 ± 1.3 | 4.0 ± 1.1 |
© 2017 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.K.; Abdul Halim, H.; Thong, K.L.; Chai, L.C. Assessment of Food Safety Knowledge, Attitude, Self-Reported Practices, and Microbiological Hand Hygiene of Food Handlers. Int. J. Environ. Res. Public Health 2017, 14, 55. https://doi.org/10.3390/ijerph14010055
Lee HK, Abdul Halim H, Thong KL, Chai LC. Assessment of Food Safety Knowledge, Attitude, Self-Reported Practices, and Microbiological Hand Hygiene of Food Handlers. International Journal of Environmental Research and Public Health. 2017; 14(1):55. https://doi.org/10.3390/ijerph14010055
Chicago/Turabian StyleLee, Hui Key, Hishamuddin Abdul Halim, Kwai Lin Thong, and Lay Ching Chai. 2017. "Assessment of Food Safety Knowledge, Attitude, Self-Reported Practices, and Microbiological Hand Hygiene of Food Handlers" International Journal of Environmental Research and Public Health 14, no. 1: 55. https://doi.org/10.3390/ijerph14010055