Factors Associated with Activities of Daily Life Disability among Centenarians in Rural Chongqing, China: A Cross-Sectional Study


 and
and
Abstract
:1. Introduction
2. Materials and Methods
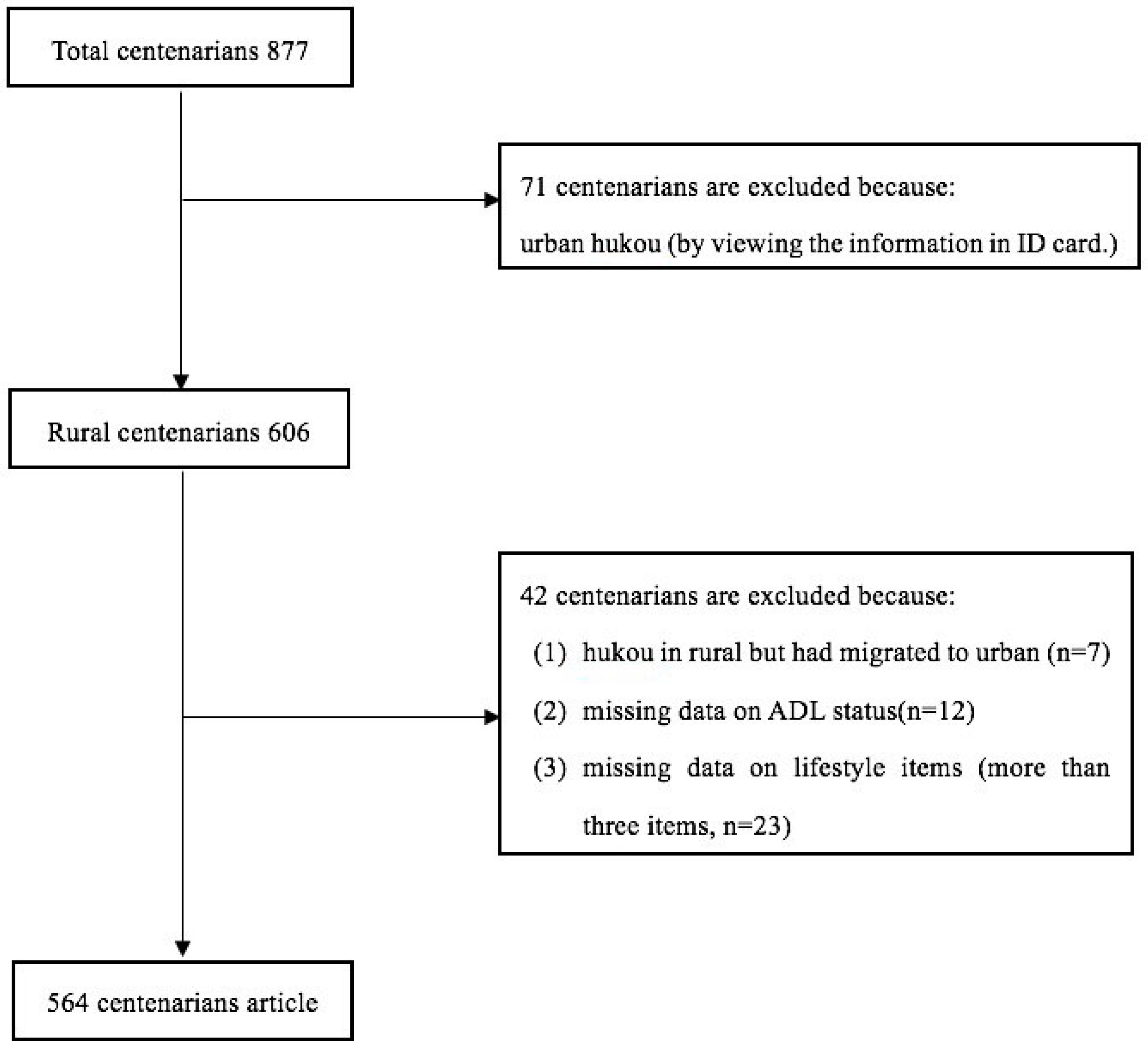
2.1. Study Population and Method
2.2. Ethics Approval
2.3. Measures
2.3.1. Demographic Characteristics and Health Condition
2.3.2. Self-Reported Lifestyle Behaviors
2.3.3. ADL Status
2.4. Statistical Analyses
3. Results
3.1. Distribution of Characteristics
3.2. Bivariate Logistic Regression Analysis
3.3. Multivariable Logistic Regression Analysis
4. Discussion
Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Statistical Yearbook of Chongqing 2016. Available online: http://www.cqtj.gov.cn/tjnj/2016/indexch.htm (accessed on 9 October 2017).
- Poon, L.W.; Woodard, J.L.; Stephen, M.L.; Green, R.; Gearing, M.; Davey, A.; Arnold, J.; Martin, P.; Siegler, I.C.; Nahapetyan, L.; et al. Understanding dementia prevalence among centenarians. J. Gerontol. 2012, 67, 358. [Google Scholar] [CrossRef] [PubMed]
- United Nations. World Population Ageing 2009; United Nations Publication: New York, NY, USA, 2010.
- The Number of Centenarians Approaching 60,000 in China. Available online: http://www.chinanews.com/sh/2014/10-21/6701888.shtml (accessed on 21 October 2014). (In Chinese).
- Franceschi, C.; Bonafè, M. Centenarians as a model for healthy aging. Biochem. Soc. Trans. 2003, 31, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Poon, L.W.; Jazwinski, M.; Green, R.C.; Woodard, J.L.; Martin, P.; Rodgers, W.L.; Johnson, M.A.; Hausman, D.; Arnold, J.; Davey, A.; et al. Methodological Considerations in Studying Centenarians: Lessons Learned from the Georgia Centenarian Studies. Annu. Rev. Gerontol. Geriatr. 2007, 27, 231–264. [Google Scholar] [PubMed]
- Li, Y.; Bai, Y.; Tao, Q.L.; Zeng, H.; Han, L.L.; Luo, M.Y.; Zhang, N.; Zhong, X.N.; Xie, Y.J.; Zhao, Y. Lifestyle of Chinese centenarians and their key beneficial factors in Chongqing, China. Asia Pac. J. Clin. Nutr. 2014, 23, 309–314. [Google Scholar] [PubMed]
- Randall, G.K.; Martin, P.; McDonald, M.; Poon, L.W. Social resources and longevity: Findings from the Georgia centenarian study. Gerontology 2010, 56, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Covinsky, K. Aging, arthritis, and disability. Arthritis Rheum. 2006, 55, 175–176. [Google Scholar] [CrossRef] [PubMed]
- Motta, M.; Bennati, E.; Ferlito, L.; Malaguarnera, M.; Motta, L.; Italian Multicenter Study on Centenarians (IMUSCE). Successful aging in centenarians: Myths and reality. Arch. Gerontol. Geriatr. 2005, 40, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Liu, Y.; George, L.K. Gender differentials of the oldest old in China. Res. Aging 2003, 25, 65–80. [Google Scholar]
- Ozaki, A.; Uchiyama, M.; Tagaya, H.; Ohida, T.; Ogihara, R. The Japanese Centenarian Study: ADL ability was associated with health practices as well as physical status. J. Am. Geriatr. Soc. 2007, 55, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Lee, T.; Lee, S.; Kim, K.; Lee, S.; Kam, S.; Ahn, S.; Cho, J.; Ory, M.G. Factors associated with ADL and IADL dependency among Korean centenarians: Reaching the 100-year-old life transition. Int. J. Aging Hum. Dev. 2012, 74, 243–264. [Google Scholar] [CrossRef] [PubMed]
- Andersen-Ranberg, K.; Schroll, M.; Jeune, B. Healthy Centenarians Do Not Exist, but Autonomous Centenarians Do: A Population-Based Study of Morbidity Among Danish Centenarians. J. Am. Geriatr. Soc. 2001, 49, 900–908. [Google Scholar] [CrossRef] [PubMed]
- Rochat, S.; Cumming, R.G.; Blyth, F.; Creasey, H.; Handelsman, D.; Le Couteur, D.G.; Naganathan, V.; Sambrook, P.N.; Seibel, M.J.; Waite, L. Frailty and use of health and community services by community-dwelling older men: the concord health and ageing in men project. Age Ageing 2010, 1, 1–6. [Google Scholar] [CrossRef] [PubMed]
- The Central People’s Government of the People’s Republic of China. The Marriage Law of the People’s Republic of China, Section 3, Article 21. 2001. Available online: http://www.gov.cn/banshi/2005-05/25/content_847.htm (accessed on 20 October 2015). (In Chinese)
- Freeman, S.; Kurosawa, H.; Ebihara, S.; Kohzuki, M. Caregiving burden for the oldest old: A population based study of centenarian caregivers in Northern Japan. Arch. Gerontol. Geriatr. 2010, 50, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen, J.; Neyens, J.C.; Rossum, E.V.; Spreeuwenberg, M.D.; Witte, L.P.D. Predicting ADL disability in community-dwelling elderly people using physical frailty indicators: A systematic review. BMC Geriatr. 2011, 11, 33. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Kim, J.; Back, J.H.; Kim, S.; Ryu, M. Changes in combined lifestyle risks and disability transition in older adults: Korean Longitudinal Study of Aging, 2006–2008. Prev. Med. 2013, 56, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Stuck, A.E.; Walthert, J.M.; Nikolaus, T.; Büla, C.J.; Hohmann, C.; Beck, J.C. Risk factors for functional status decline in community-living elderly people: A systematic literature review. Soc. Sci. Med. 1999, 48, 445–469. [Google Scholar] [CrossRef]
- Lee, Y.; Park, K.H. Health practices that predict recovery from functional limitations in older adults. Am. J. Prev. Med. 2006, 31, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Fei, S.; Norman, I.J.; While, A.E. Physical activity in older people: A systematic review. BMC Public Health 2013, 13, 449. [Google Scholar]
- Komatsu, M.; Mitsuhashi, M.; Yamagata, E.; Manabe, E.; Okayama, Y.; Kimura, M. Evaluation of lifestyle of adl-independent elderly people for designing care to improve the sleep quality. Jpn. J. Physiol. Anthropol. 2012, 17, 117–124. [Google Scholar]
- Einarsson, U.; Gottberg, K.; Fredrikson, S.; Von, K.L.; Holmqvist, L.W. Activities of daily living and social activities in people with multiple sclerosis in stockholm county. Clin. Rehabil. 2006, 20, 543. [Google Scholar] [CrossRef] [PubMed]
- Roberts, K.D. China’s Tidal Wave of Migrant Labor: What Can We Learn from Mexican Undocumented Migration to the United States? Int. Migr. Rev. 1997, 31, 249–291. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.W. Post-Mao China: A two-class urban society in the making. Int. J. Urban Reg. Res. 1996, 20, 134–150. [Google Scholar] [CrossRef]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. The index of ADL: A standardized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Beydoun, M.A.; Popkin, B.M. The impact of socio-economic factors on functional status decline among community-dwelling older adults in China. Soc. Sci. Med. 2005, 60, 2045–2057. [Google Scholar] [CrossRef] [PubMed]
- Davey, A.; Elias, M.F.; Siegler, I.C.; Lele, U.; Martin, P.; Johnson, M.A.; Hausman, D.B.; Poon, L.W. Cognitive function, physical performance, health, and disease: Norms from the georgia centenarian study. Exp. Aging Res. 2010, 36, 394–425. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Ferrucci, L. Assessing the building blocks of function: Utilizing measures of functional limitation. Am. J. Prev. Med. 2003, 25, 112–121. [Google Scholar] [CrossRef]
- Wolff, J.L.; Boult, C.; Boyd, C.; Anderson, G. Newly reported chronic conditions and onset of functional dependency. J. Am. Geriatr. Soc. 2005, 53, 851–855. [Google Scholar] [CrossRef] [PubMed]
- Kriegsman, D.M.; Deeg, D.J.; Stalman, W.A. Comorbidity of somatic chronic diseases and decline in physical functioning: The Longitudinal Aging Study Amsterdam. J. Clin. Epidemiol. 2004, 57, 55–65. [Google Scholar] [CrossRef]
- Houston, D.K.; Stevens, J.; Cai, J.; Haines, P.S. Dairy, fruit, and vegetable intakes and functional limitations and disability in a biracial cohort: The Atherosclerosis Risk in Communities Study. Am. J. Clin. Nutr. 2005, 81, 515–522. [Google Scholar] [PubMed]
- Féart, C.; Pérès, K.; Samieri, C.; Letenneur, L.; Dartigues, J.F.; Barberger-Gateau, P. Adherence to a Mediterranean diet and onset of disability in older persons. Eur. J. Epidemiol. 2011, 26, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Kimura, Y.; Okumiya, K.; Sakamoto, R.; Ishine, M.; Wada, T.; Kosaka, Y.; Wada, C.; Ishimoto, Y.; Hirosaki, M.; Kasahara, Y.; et al. Comprehensive geriatric assessment of elderly highlanders in Qinghai, China IV: Comparison of food diversity and its relation to health of Han and Tibetan elderly. Geriatr. Gerontol. Int. 2009, 9, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Kimura, Y.; Wada, T.; Ishine, M.; Ishimoto, Y.; Kasahara, Y.; Konno, A.; Nakatsuka, M.; Sakamoto, R.; Okumiya, K.; Fujisawa, M.; et al. Food diversity is closely associated with activities of daily living, depression, and quality of life in community-dwelling elderly people. J. Am. Geriatr. Soc. 2009, 57, 922–924. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; MacGregor, G.A. A comprehensive review on salt and health and current experience of worldwide salt reduction programmes. J. Hum. Hypertens. 2009, 23, 363–384. [Google Scholar] [CrossRef] [PubMed]
- Huh, J.H.; Lim, J.S.; Lee, M.Y.; Chung, C.H.; Shin, J.Y. Gender-specific association between urinary sodium excretion and body composition: Analysis of the 2008–2010 Korean National Health and Nutrition Examination Surveys. Metabolism 2015, 64, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Cawthon, P.M.; Fox, K.M.; Gandra, S.R.; Delmonico, M.J.; Chiou, C.F.; Anthony, M.S. Do muscle mass, muscle density, strength, and physical function similarly influence risk of hospitalization in older adults? J. Am. Geriatr. Soc. 2009, 57, 1411–1419. [Google Scholar] [CrossRef] [PubMed]
- Pes, G.M.; Dore, M.P.; Errigo, A.; Poulain, M. Analysis of physical activity among free-living nonagenarians from a Sardinian Longevous population. Rehabil. Psychol. 2017, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Avlund, K.; Lund, R.; Holstein, B.E.; Due, P.; Sakari-Rantala, R.; Heikkinen, R.L. The impact of structural and functional characteristics of social relations as determinants of functional decline. J. Gerontol. B Psychol. Sci. Soc. Sci. 2004, 59, S44–S51. [Google Scholar] [CrossRef] [PubMed]
- Martin, P.; MacDonald, M.; Margrett, J.; Siegler, I.; Poon, L.W.; Jazwinski, S.M.; Green, R.C.; Gearing, M.; Markesbery, W.R.; Woodard, J.L.; et al. Correlates of functional capacity among centenarians. J. Appl. Gerontol. 2013, 32, 324–346. [Google Scholar] [CrossRef] [PubMed]
- Mendes de Leon, C.F.; Glass, T.A.; Berkman, L.F. Social engagement and disability in a community population of older adults: The New Haven EPESE. Am. J. Epidemiol. 2003, 157, 633–642. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y. Reliability of age reporting among the Chinese oldest-old in the CLHLS datasets. Demogr. Methods Popul. Anal. 2008, 20, 61–78. [Google Scholar]
- Wang, Z.; Zeng, Y.; Jeune, B.; Vaupel, J.W. Age validation of Han Chinese centenarians. Genus 1998, 54, 123–141. [Google Scholar] [PubMed]
- Coale, A.J.; Li, S.M. The effect of age misreporting in China on the calculation of mortality rates at very high ages. Demography 1991, 28, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Poston, D.L., Jr.; Ashbaugh Vlosky, D.; Gu, D. Healthy Longevity in China: Demographic, Socioeconomic, and Psychological Dimensions; Springer: Dordrecht, The Netherlands, 2008; pp. 312–313. [Google Scholar]
- Gustafson, D.R.; Mazzuco, S.; Ongaro, F.; Antuono, P.; Forloni, G.; Albani, D.; Gajo, G.B.; Durante, E.; Caberlotto, L.; Zanardo, A.; et al. Body mass index, cognition, disability, APOE genotype, and mortality: The “Treviso Longeva” Study. Am. J. Geriatr. Psychiatry 2012, 20, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Yin, Z.; Shi, X.; Kraus, V.B.; Brasher, M.S.; Chen, H.; Liu, Y.; Lv, Y.; Zeng, Y. Gender-dependent association of body mass index and waist circumference with disability in the Chinese oldest old. Obesity 2014, 22, 1918–1925. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | No ADL Disability | ADL Disability | p-Value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Demographic characteristics | |||||
| Age | 0.234 | ||||
| 100–105 | 180 | 92.7 | 332 | 89.7 | |
| 106–110 | 14 | 7.3 | 38 | 10.3 | |
| Gender | 0.031 * | ||||
| Male | 41 | 21.1 | 52 | 14.1 | |
| Female | 153 | 78.9 | 318 | 85.9 | |
| Ethnicity | 0.595 | ||||
| Han | 183 | 94.3 | 344 | 93.2 | |
| Ethnic minority | 11 | 5.7 | 26 | 6.8 | |
| Current diseases | 0.001 ** | ||||
| No | 144 | 74.2 | 161 | 43.5 | |
| Yes | 50 | 25.8 | 209 | 56.5 | |
| Lifestyle factors | |||||
| Living arrangement | 0.061 | ||||
| Living alone | 2 | 1.0 | 14 | 3.8 | |
| Living with others | 192 | 99.0 | 356 | 96.2 | |
| Smoking | 0.938 | ||||
| Yes | 19 | 9.8 | 37 | 10.0 | |
| No | 175 | 90.2 | 333 | 90.0 | |
| Drinking habits | 0.000 * | ||||
| No | 161 | 83.0 | 307 | 83.0 | |
| Yes | 33 | 17.0 | 63 | 17.0 | |
| Good diet habits | 0.003 ** | ||||
| Yes | 144 | 74.2 | 225 | 60.8 | |
| No | 50 | 25.8 | 145 | 39.2 | |
| Avoiding sweet, fatty and high cholesterol food | 0.22 | ||||
| Yes | 17 | 8.8 | 45 | 12.2 | |
| No | 177 | 91.2 | 325 | 87.8 | |
| Salt preference | 0.028 * | ||||
| Yes | 4 | 0.5 | 23 | 6.2 | |
| No | 190 | 99.5 | 347 | 93.8 | |
| Social activities | 0.011 * | ||||
| Yes | 50 | 25.8 | 62 | 16.8 | |
| No | 144 | 74.2 | 308 | 83.2 | |
| Physical activity | 0.005 ** | ||||
| Yes | 56 | 28.9 | 68 | 18.4 | |
| No | 138 | 71.1 | 301 | 82.6 | |
| Reading | 0.077 | ||||
| Yes | 7 | 3.6 | 5 | 0.8 | |
| No | 187 | 96.4 | 363 | 99.2 | |
| Watching TV or listening to radio | 0.061 | ||||
| Yes | 61 | 31.4 | 146 | 39.5 | |
| No | 133 | 68.6 | 224 | 60.5 | |
| Variables | OR | 95% CI | p-Value |
|---|---|---|---|
| Age | |||
| 100–105 | 1 | ||
| 106–110 | 1.366 | 0.718–2.600 | 0.342 |
| Ethnicity | |||
| Han nationality | 1 | ||
| National minority | 1.318 | 0.633–2.742 | 0.461 |
| Present diseases | |||
| No | 1 | ||
| Yes | 3.773 | 2.570–5.539 | 0.000 ** |
| Living arrangement | |||
| Living with others | 1 | ||
| Living alone | 3.861 | 0.865–17.236 | 0.077 |
| Smoking | |||
| Yes | 1 | ||
| No | 0.644 | 0.326–1.269 | 0.203 |
| Drinking habits | |||
| No | 1 | ||
| Yes | 1.171 | 0.719–1.906 | 0.526 |
| Good diet habits | |||
| Yes | 0.543 | 0370–0.798 | 0.002 ** |
| No | 1 | ||
| Avoiding sweet, fatty and high cholesterol food | |||
| Yes | 1.429 | 0.793–2.576 | 0.235 |
| No | 1 | ||
| Salt preference | |||
| No | 1 | ||
| Yes | 3.016 | 1.026–8.867 | 0.045 * |
| Social activities | |||
| Yes | 0.588 | 0.304–0.844 | 0.014 * |
| No | 1 | ||
| Physical activity | |||
| Yes | 0.561 | 0.373–0.845 | 0.006 ** |
| No | 1 | ||
| Reading | |||
| Yes | 0.395 | 0.123–1.272 | 0.120 |
| No | 1 | ||
| Watching TV or listening to radio | |||
| No | |||
| Yes | 1.413 | 0.977–2.044 | 0.066 |
| Variables | OR | 95% CI | p-Value |
|---|---|---|---|
| Age | |||
| 100–105 | 1 | ||
| 106–110 | 0.843 | 0.415–1.714 | 0.637 |
| Gender | |||
| Male | 1 | ||
| Female | 1.921 | 1.072–3.442 | 0.028 * |
| Ethnicity | |||
| Han | 1 | ||
| Ethnic minority | 1.422 | 0.639–3.163 | 0.388 |
| Present diseases | |||
| No | 1 | ||
| Yes | 3.581 | 2.357–5.442 | 0.000 ** |
| Living arrangement | |||
| Living with others | 1 | ||
| Living alone | 3.259 | 0.653–16.277 | 0.150 |
| Smoking | |||
| Yes | 1 | ||
| No | 0.516 | 0.217–1.228 | 0.135 |
| Drinking habits | |||
| No | 1 | ||
| Yes | 0.746 | 0.398–1.397 | 0.360 |
| Good diet habits | |||
| Yes | 0.489 | 0.322–0.741 | 0.001 ** |
| No | 1 | ||
| Avoiding sweet, fatty and high cholesterol food | |||
| Yes | 1.213 | 0.624–2.359 | 0.569 |
| No | 1 | ||
| Salt preference | |||
| No | 1 | ||
| Yes | 3.585 | 1.142–11.256 | 0.029 * |
| Social activities | |||
| Yes | 0.543 | 0.328–0.900 | 0.018 * |
| No | 1 | ||
| Physical activity | |||
| Yes | 0.551 | 0.336–0.904 | 0.018 * |
| No | 1 | ||
| Reading | |||
| Yes | 0.645 | 0.181–2.293 | 0.498 |
| No | 1 | ||
| Watching TV or listening to radio | |||
| No | 1 | ||
| Yes | 0.880 | 0.557–1.392 | 0.585 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, T.; Lu, L.; Luo, L.; Guo, Y.; Ying, L.; Tao, Q.; Zeng, H.; Han, L.; Shi, Z.; Zhao, Y. Factors Associated with Activities of Daily Life Disability among Centenarians in Rural Chongqing, China: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2017, 14, 1364. https://doi.org/10.3390/ijerph14111364
Wu T, Lu L, Luo L, Guo Y, Ying L, Tao Q, Zeng H, Han L, Shi Z, Zhao Y. Factors Associated with Activities of Daily Life Disability among Centenarians in Rural Chongqing, China: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2017; 14(11):1364. https://doi.org/10.3390/ijerph14111364
Chicago/Turabian StyleWu, Tingting, Lu Lu, Li Luo, Yingqi Guo, Liying Ying, Qingliu Tao, Huan Zeng, Lingli Han, Zumin Shi, and Yong Zhao. 2017. "Factors Associated with Activities of Daily Life Disability among Centenarians in Rural Chongqing, China: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 14, no. 11: 1364. https://doi.org/10.3390/ijerph14111364