The Short-Term Effects of Visibility and Haze on Mortality in a Coastal City of China: A Time-Series Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Site
2.2. Data Collection
2.3. Statistical Analysis
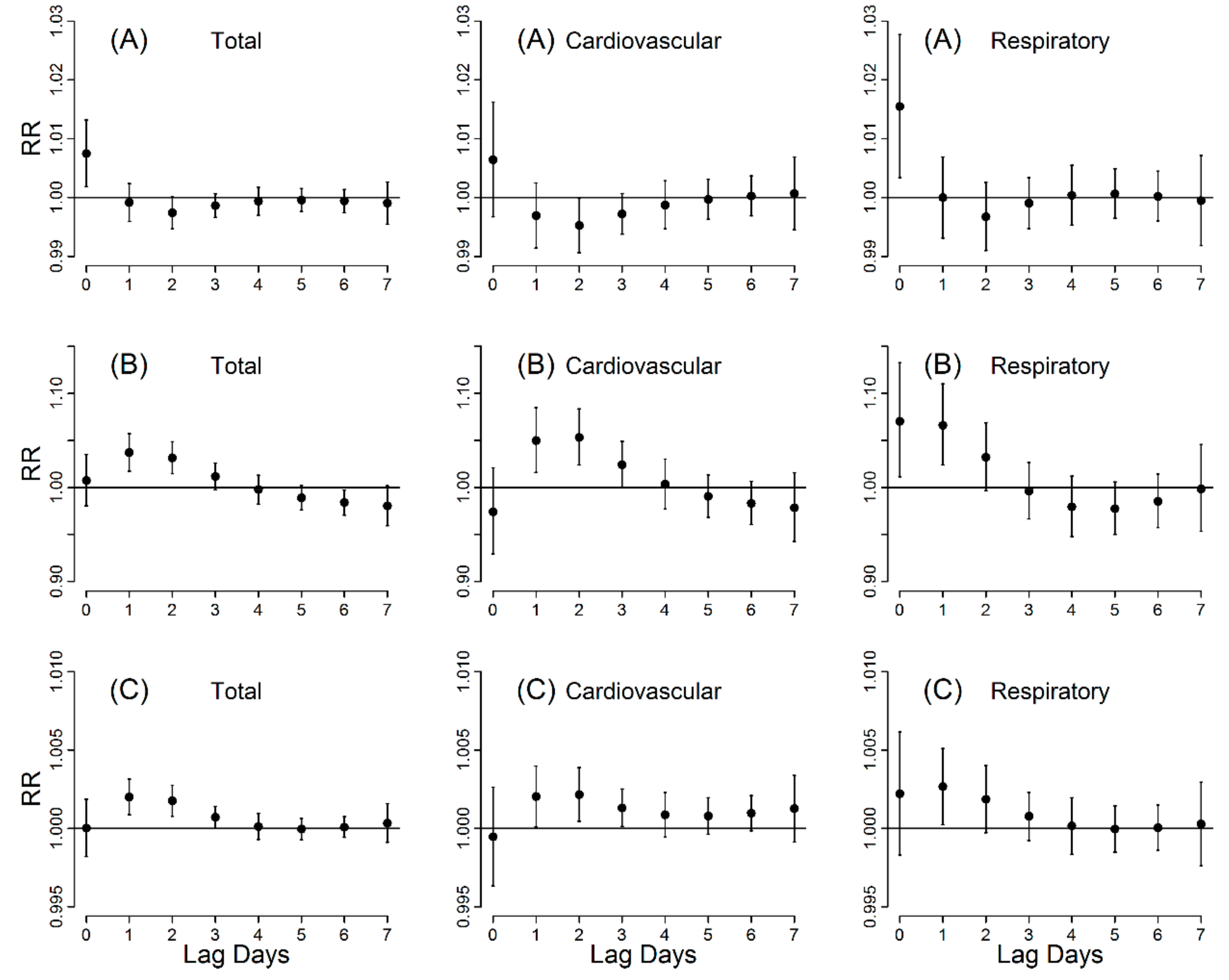
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Gehring, U.; Gruzieva, O.; Agius, R.M.; Beelen, R.; Custovic, A.; Cyrys, J.; Eeftens, M.; Flexeder, C.; Fuertes, E.; Heinrich, J.; et al. Air pollution exposure and lung function in children: The ESCAPE project. Environ. Health Perspect. 2013, 121, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Geravandi, S.; Sicard, P.; Khaniabadi, Y.O.; De Marco, A.; Ghomeishi, A.; Goudarzi, G.; Mahboubi, M.; Yari, A.R.; Dobaradaran, S.; Hassani, G.; et al. A comparative study of hospital admissions for respiratory diseases during normal and dusty days in Iran. Environ. Sci. Pollut. Res. 2017, 24, 18152–18159. [Google Scholar] [CrossRef] [PubMed]
- Khaniabadi, Y.O.; Hopke, P.K.; Goudarzi, G.; Daryanoosh, S.M.; Jourvand, M.; Basiri, H. Cardiopulmonary mortality and COPD attributed to ambient ozone. Environ. Res. 2017, 152, 336–341. [Google Scholar] [CrossRef] [PubMed]
- He, T.; Yang, Z.; Liu, T.; Shen, Y.; Fu, X.; Qian, X.; Zhang, Y.; Wang, Y.; Xu, Z.; Zhu, S.; et al. Ambient air pollution and years of life lost in Ningbo, China. Sci. Rep. 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Shang, Y.; Sun, Z.; Cao, J.; Wang, X.; Zhong, L.; Bi, X.; Li, H.; Liu, W.; Zhu, T.; Huang, W. Systematic review of Chinese studies of short-term exposure to air pollution and daily mortality. Environ. Int. 2013, 54, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Zhao, A.; Chen, R.; Kuang, X.; Kan, H. Ambient air pollution and daily outpatient visits for cardiac arrhythmia in Shanghai, China. J. Epidemiol. 2014, 24, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Ou, C.; Song, Y.; Li, L.; Chen, P.; Liu, Q. Estimating years of life lost from cardiovascular mortality related to air pollution in Guangzhou, China. Sci. Total Environ. 2016, 573, 1566–1572. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.; Brauer, M.; Burnett, R.; Anderson, R.H.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the global burden of diseases study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef]
- Donkelaar, A.; Martin, R.V.; Brauer, M.; Kahn, R.; Levy, R.; Verduzco, C.; Villeneuve, P.J. Global estimates of ambient fine particulate matter concentrations from satellite-based aerosol optical depth: Development and application. Environ. Health Perspect. 2010, 118, 847–855. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Tan, J.; Kan, H.; Zhao, N.; Song, W.; Song, G.; Chen, G.; Jiang, L.; Jiang, C.; Chen, R.; et al. Visibility, air quality and daily mortality in Shanghai, China. Sci. Total Environ. 2009, 407, 3295–3300. [Google Scholar] [CrossRef] [PubMed]
- Thach, T.Q.; Wong, C.M.; Chan, K.P.; Chau, Y.K.; Chung, Y.N.; Ou, C.Q.; Yang, L.; Hedley, A.J. Daily visibility and mortality: Assessment of health benefits from improved visibility in Hong Kong. Environ. Res. 2010, 110, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Hyslop, N. Impaired visibility: The air pollution people see. Atmos. Environ. 2009, 43, 182–195. [Google Scholar] [CrossRef]
- Cheng, Z.; Wang, S.; Jiang, J.; Fu, Q.; Chen, C.; Xu, B.; Yu, J.; Fu, X.; Hao, J. Long-Term trend of haze pollution and impact of particulate matter in the Yangtze river delta, China. Environ. Pollut. 2013, 182, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Sloane, C.S.; White, W.H. Visibility: An evolving issue. Environ. Sci. Technol. 1986, 20, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Zhang, Y.H.; Xu, Y.J.; Lin, H.L.; Xu, X.J.; Luo, Y.; Xiao, J.; Zeng, W.L.; Zhang, W.F.; Chu, C.; et al. The effects of dust-haze on mortality are modified by seasons and individual characteristics in Guangzhou, China. Environ. Pollut. 2014, 187, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.; Hu, X.; Sayer, A.M.; Levy, R.; Zhang, Q.; Xue, Y.; Tong, S.; Bi, J.; Huang, L.; Liu, Y. Satellite-Based spatiotemporal trends in PM2.5 concentrations: China, 2004–2013. Environ. Health Perspect. 2016, 124, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Xu, P.; Chen, Y.; Ye, X. Haze, air pollution, and health in China. Lancet 2013, 382, 2067. [Google Scholar] [CrossRef]
- Zhang, Z.; Wu, W.; Wei, J.; Song, Y.; Yan, X.; Zhu, L.; Wang, Q. Aerosol optical depth retrieval from visibility in China during 1973–2014. Atmos. Environ. 2017, 171, 38–48. [Google Scholar] [CrossRef]
- China Meteorological Administration. 2010. Available online: http://www.cma.gov.cn/ (accessed on 20 January 2010).
- Wu, D.; Wu, X.; Li, F.; Tan, H.; Chen, J.; Cao, Z.Q.; Sun, X.; Chen, H.; Li, H. Temporal and spatial variation of haze during 1951–2005 in Chinese mainland. Acta Meteorol. Sin. 2010, 68, 680–688. [Google Scholar]
- Bhaskaran, K.; Gasparrini, A.; Hajat, S.; Smeeth, L.; Armstrong, B. Time series regression studies in environmental epidemiology. Int. J. Epidemiol. 2013, 42, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Armstrong, B.; Kenward, M.G. Distributed lag non-linear models. Stat. Med. 2010, 29, 2224–2234. [Google Scholar] [CrossRef] [PubMed]
- Bai, L.; Ding, G.; Gu, S.; Bi, P.; Su, B.; Qin, D.; Xu, G.; Liu, Q. The effects of summer temperature and heat waves on heat-related illness in a coastal city of China, 2011–2013. Environ. Res. 2014, 132, 212–219. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Yin, P.; Ou, C-Q.; Li, M.; Li, J.; Liu, X.; Gao, J.; Liu, Y.; Qin, R.; et al. The burden of stroke mortality attributable to cold and hot ambient temperatures: Epidemiological evidence from china. Environ. Int. 2016, 92–93, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Ou, C.; Ding, Y.; Zhou, Y.; Chen, P. Daily temperature and mortality: A study of distributed lag non-linear effect and effect modification in Guangzhou. Environ. Health 2012, 11, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Kan, H.; London, S.J.; Chen, G.; Zhang, Y.; Song, G.; Zhao, N.; Jiang, L.; Chen, B. Season, sex, age, and education as modifiers of the effects of outdoor air pollution on daily mortality in Shanghai, China: The public health and air pollution in Asia (PAPA) study. Environ. Health Perspect. 2008, 116, 1183–1188. [Google Scholar] [CrossRef] [PubMed]
- Stieb, D.M.; Burnett, R.T.; Smith-Doiron, M.; Brion, O.; Shin, H.H.; Economou, V. A new multipollutant, no-threshold air quality health index based on short-term associations observed in daily time-series analyses. J. Air Waste Manag. Assoc. 2008, 58, 435–450. [Google Scholar] [PubMed]
- To, T.; Shen, S.; Atenafu, E.G.; Guan, J.; McLimont, S.; Stocks, B.; Licskai, C. The air quality health index and asthma morbidity: A population-based study. Environ. Health Perspect. 2013, 121, 46–52. [Google Scholar] [PubMed]
- Nel, A. Air pollution-related illness: Effects of particles. Science 2005, 308, 804–806. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Rajagopalan, S.; Pope, C.A.; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A.; et al. Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American heart association. Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef] [PubMed]
- Bateson, T.; Schwartz, J. Who is sensitive to the effects of particulate air pollution on mortality? A Case-Crossover analysis of effect modifiers. Epidemiology 2004, 15, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Samoli, E.; Peng, R.; Ramsay, T.; Pipikou, M.; Touloumi, G.; Dominici, F.; Burnett, R.; Cohen, A.; Krewski, D.; Samet, J.; et al. Acute effects of ambient particulate matter on mortality in Europe and North America: Results from the APHENA study. Environ. Health Perspect. 2008, 116, 1480–1486. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.; Zanobetti, A.; Dominici, F. Evidence on vulnerability and susceptibility to health risks associated with short-term exposure to particulate matter: A systematic review and Meta-Analysis. Am. J. Epidemiol. 2013, 178, 865–876. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Mean ± SD | Minimum | Percentiles | Maximum | ||
|---|---|---|---|---|---|---|
| 25th | 50th | 75th | ||||
| Daily death counts | ||||||
| Total | 99.6 ± 19.9 | 55 | 85 | 96 | 112 | 177 |
| Cardiovascular | 27.6 ± 8.3 | 8 | 22 | 27 | 33 | 60 |
| Respiratory | 16.0 ± 6.6 | 2 | 11 | 15 | 20 | 45 |
| Gender | ||||||
| Male | 56.0 ± 11.4 | 27 | 48 | 55 | 63 | 96 |
| Female | 43.7 ± 11.0 | 19 | 35 | 42 | 51 | 85 |
| Age (years) | ||||||
| <65 | 24.1 ± 5.3 | 10 | 20 | 24 | 28 | 41 |
| ≥65 | 75.6 ± 18.0 | 35 | 62 | 72 | 87 | 143 |
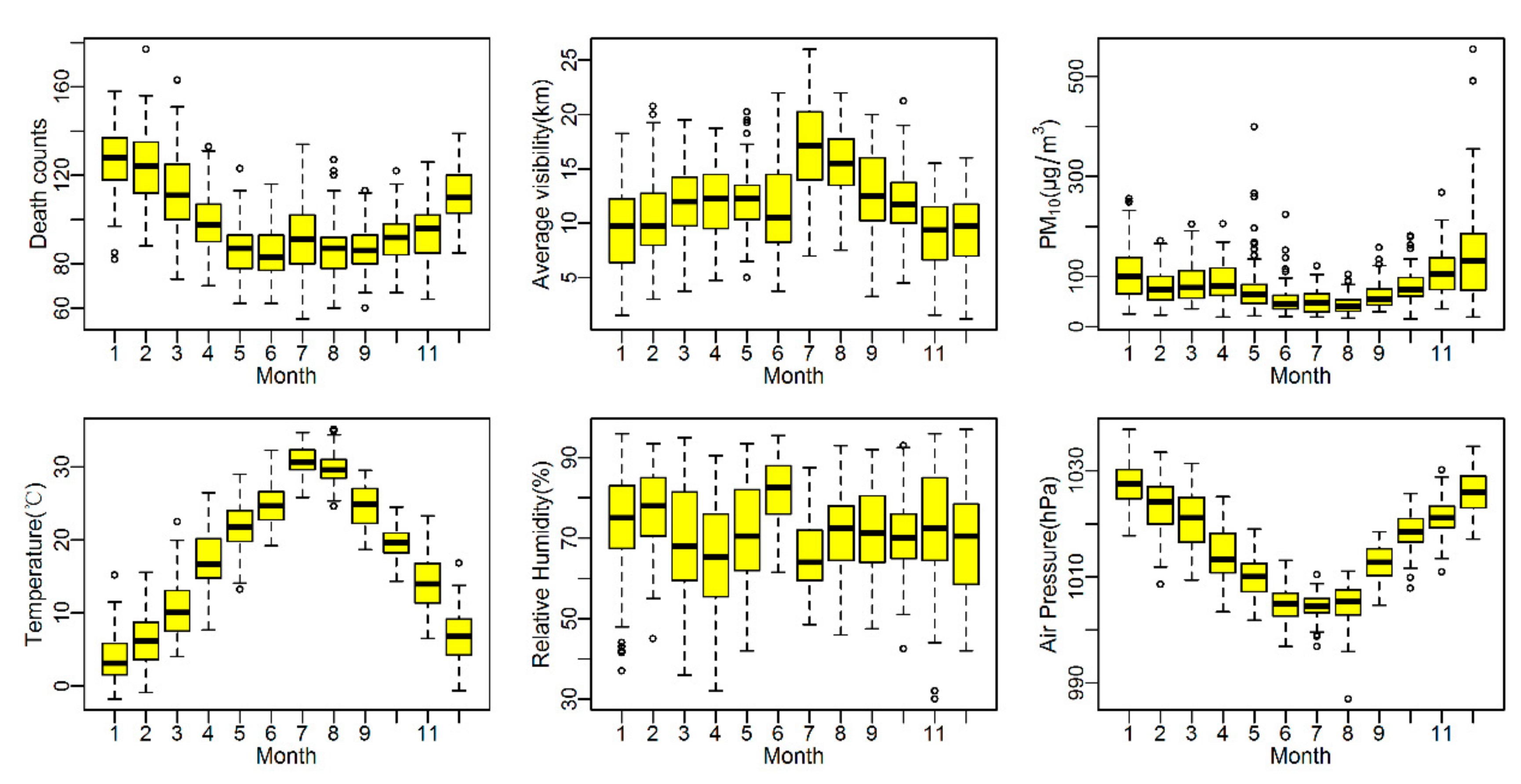
| Meteorological variables | ||||||
| Visibility (km) | 11.9 ± 4.2 | 1.2 | 9.0 | 11.8 | 14.5 | 26.0 |
| Temperature (°C) | 17.6 ± 9.4 | −1.8 | 9.3 | 18.9 | 25.3 | 35.1 |
| Relative humidity (%) | 71.7 ± 12.7 | 30.0 | 63.0 | 71.8 | 81.0 | 97.0 |
| Atmosphere pressure (hPa) | 1015.7 ± 9.1 | 987.0 | 1007.6 | 1016.1 | 1022.7 | 1037.8 |
| Air pollution | ||||||
| PM10 (μg/m3) | 82.1 ± 53.4 | 15 | 47 | 69 | 104 | 554 |
| SO2 (μg/m3) | 22.5 ± 17.6 | 2 | 10 | 17 | 31 | 131 |
| NO2 (μg/m3) | 45.8 ± 22.7 | 1 | 29 | 44 | 61 | 154 |
| Variables | Visibility | Haze | PM10 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Warm Season | Cold Season | Full Year | Warm Season | Cold Season | Full Year | Warm Season | Cold Season | Full Year | |
| Mortality | |||||||||
| Total | −0.59 (−1.79–0.63) | 1.18 (0.50–1.86) | 0.78 (0.22–1.36) | 6.41 (−3.61–17.47) | 10.01 (5.03–15.40) | 7.76 (3.29–12.42) | 0.47 (−0.09–1.02) | 0.43 (0.18–0.68) | 0.38 (0.17–0.59) |
| Cardiovascular | −1.91 (−3.97–0.20) | 1.30 (0.11–2.50) | 0.71 (−0.27–1.70) | 6.11 (−10.70–26.08) | 12.08 (3.29–21.62) | 7.73 (0.12–15.92) | 0.25 (−0.72–1.23) | 0.49 (0.07–0.92) | 0.37 (0.01–0.73) |
| Respiratory | 1.63 (−1.24–4.58) | 1.53 (0.10–2.98) | 1.61 (0.39–2.85) | 12.40 (−11.16–42.22) | 23.70 (12.24–36.32) | 17.77 (7.64–28.86) | 0.67 (−0.65–2.01) | 0.82 (0.31–1.33) | 0.68 (0.22–1.13) |
| Gender | |||||||||
| Male | 0.12 (−1.41–1.67) | 1.30 (0.45–2.16) | 1.01 (0.29–1.74) | 4.73 (−7.64–18.75) | 9.87 (3.56–16.56) | 6.88 (1.27–12.79) | 0.58 (−0.12–1.29) | 0.29 (−0.02–0.60) | 0.33 (0.06–0.60) |
| Female | −1.52 (−3.29–0.29) | 1.03 (0.11–1.96) | 0.50 (−0.30–1.30) | 8.64 (−6.37–26.06) | 10.47 (3.68–17.71) | 8.93 (2.62–15.64) | 0.32 (−0.51–1.14) | 0.60 (0.27–0.93) | 0.44 (0.15–0.74) |
| Age (years) | |||||||||
| <65 | −0.90 (−3.05–1.30) | 1.00 (−0.24–2.26) | 0.60 (−0.44–1.64) | −3.07 (−19.05–16.08) | 1.84 (−6.66–11.12) | 0.24 (−7.34–8.44) | 0.34 (−0.64–1.33) | 0.03 (−0.42–0.49) | 0.11 (−0.28–0.50) |
| ≥65 | −0.48 (−1.85–0.91) | 1.23 (0.45–2.01) | 0.84 (0.19–1.49) | 10.09 (−1.70–23.29) | 12.61 (6.80–18.73) | 10.09 (4.94–15.49) | 0.51 (−0.12–1.15) | 0.54 (0.26–0.82) | 0.46 (0.22–0.70) |
| Air Pollution and Model | Total | Cardiovascular | Respiratory | |||
|---|---|---|---|---|---|---|
| ER (%) | 95% CI | ER (%) | 95% CI | ER (%) | 95% CI | |
| Visibility | ||||||
| Single model | 0.78 | 0.22–1.36 | 0.71 | −0.27–1.70 | 1.61 | 0.39–2.85 |
| +PM10 | 0.70 | 0.05–1.35 | 0.83 | −0.29–1.97 | 1.03 | 0.36–2.45 |
| +SO2 | 0.67 | 0.07–1.28 | 0.59 | −0.45–1.63 | 1.22 | −0.09–2.54 |
| +NO2 | 0.69 | 0.09–1.29 | 0.61 | −0.42–1.66 | 1.42 | 0.12–2.74 |
| +PM10 + SO2 + NO2 | 0.71 | 0.04–1.38 | 0.90 | −0.26–2.06 | 0.87 | −0.57–2.33 |
| Haze | ||||||
| Single model | 7.76 | 3.29–12.42 | 7.73 | 0.12–15.92 | 17.77 | 7.64–28.86 |
| +PM10 | 5.44 | 0.34–10.79 | 6.04 | −2.67–15.53 | 13.85 | 2.44–26.53 |
| +SO2 | 5.43 | 0.90–10.17 | 3.16 | −4.39–11.31 | 14.05 | 3.78–25.34 |
| +NO2 | 6.09 | 1.50–10.89 | 4.96 | −2.76–13.31 | 15.76 | 5.29–27.27 |
| +PM10 + SO2 + NO2 | 5.59 | 0.35–11.12 | 5.61 | −3.27–15.31 | 13.11 | 1.36–26.23 |
| Variables | Visibility | Haze | ||
|---|---|---|---|---|
| ER (%) | 95% CI | ER (%) | 95% CI | |
| 1. Maximum lag days | ||||
| 3 | 0.79 | 0.22–1.37 | 8.98 | 4.33–13.85 |
| 7 | 0.78 | 0.22–1.36 | 7.76 | 3.29–12.42 |
| 10 | 0.78 | 0.23–1.34 | 6.79 | 2.37–11.39 |
| 2. df for time | ||||
| 6 | 0.74 | 0.17–1.31 | 8.29 | 3.80–12.98 |
| 7 | 0.78 | 0.22–1.36 | 7.76 | 3.29–12.42 |
| 8 | 0.73 | 0.17–1.30 | 7.77 | 3.30–12.43 |
| 3. df for temperature | ||||
| 3 | 0.80 | 0.23–1.37 | 7.62 | 3.13–2.31 |
| 6 | 0.78 | 0.22–1.36 | 7.76 | 3.29–12.42 |
| 4. df for air pressure and relative humidity | ||||
| 3 | 0.78 | 0.22–1.36 | 7.76 | 3.29–12.42 |
| 6 | 0.70 | 0.12–1.27 | 7.37 | 2.88–12.06 |
| 5. Definition of haze day | ||||
| Humidity < 80% * | - | - | 7.76 | 3.29–12.42 |
| Humidity <90%# | - | - | 6.45 | 2.42–10.64 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gu, S.; Yang, J.; Woodward, A.; Li, M.; He, T.; Wang, A.; Lu, B.; Liu, X.; Xu, G.; Liu, Q. The Short-Term Effects of Visibility and Haze on Mortality in a Coastal City of China: A Time-Series Study. Int. J. Environ. Res. Public Health 2017, 14, 1419. https://doi.org/10.3390/ijerph14111419
Gu S, Yang J, Woodward A, Li M, He T, Wang A, Lu B, Liu X, Xu G, Liu Q. The Short-Term Effects of Visibility and Haze on Mortality in a Coastal City of China: A Time-Series Study. International Journal of Environmental Research and Public Health. 2017; 14(11):1419. https://doi.org/10.3390/ijerph14111419
Chicago/Turabian StyleGu, Shaohua, Jun Yang, Alistair Woodward, Mengmeng Li, Tianfeng He, Aihong Wang, Beibei Lu, Xiaobo Liu, Guozhang Xu, and Qiyong Liu. 2017. "The Short-Term Effects of Visibility and Haze on Mortality in a Coastal City of China: A Time-Series Study" International Journal of Environmental Research and Public Health 14, no. 11: 1419. https://doi.org/10.3390/ijerph14111419