FRED: Exergame to Prevent Dependence and Functional Deterioration Associated with Ageing. A Pilot Three-Week Randomized Controlled Clinical Trial



Abstract
:1. Introduction
- The application of technological solutions in health care is a field that is constantly expanding and about which there are great expectations both on the part of users and healthcare professionals and carers, despite the reticence existing in this area known as a technology gap [4].
- It is of the utmost importance to continue working to reduce the gap existing between technology, frail elderly persons, healthcare professionals and carers by bringing together the different views about technology and thus stimulate dialogue, an increased awareness and knowledge about the respective fields in order to engage in collaboration on projects that may reduce costs and improve health and quality of life [4].
2. Materials and Methods
2.1. Participants
2.2. Experimental Design
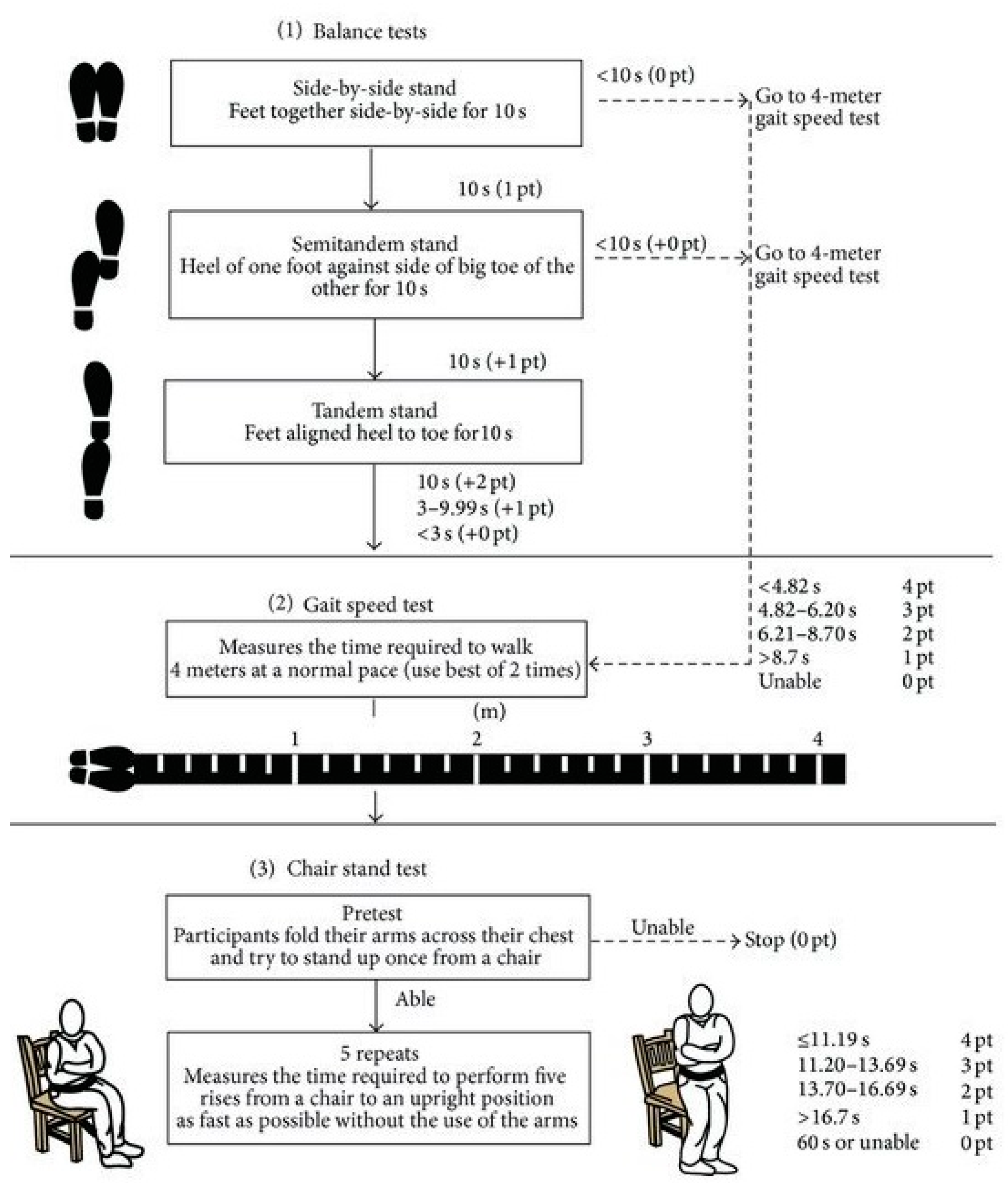
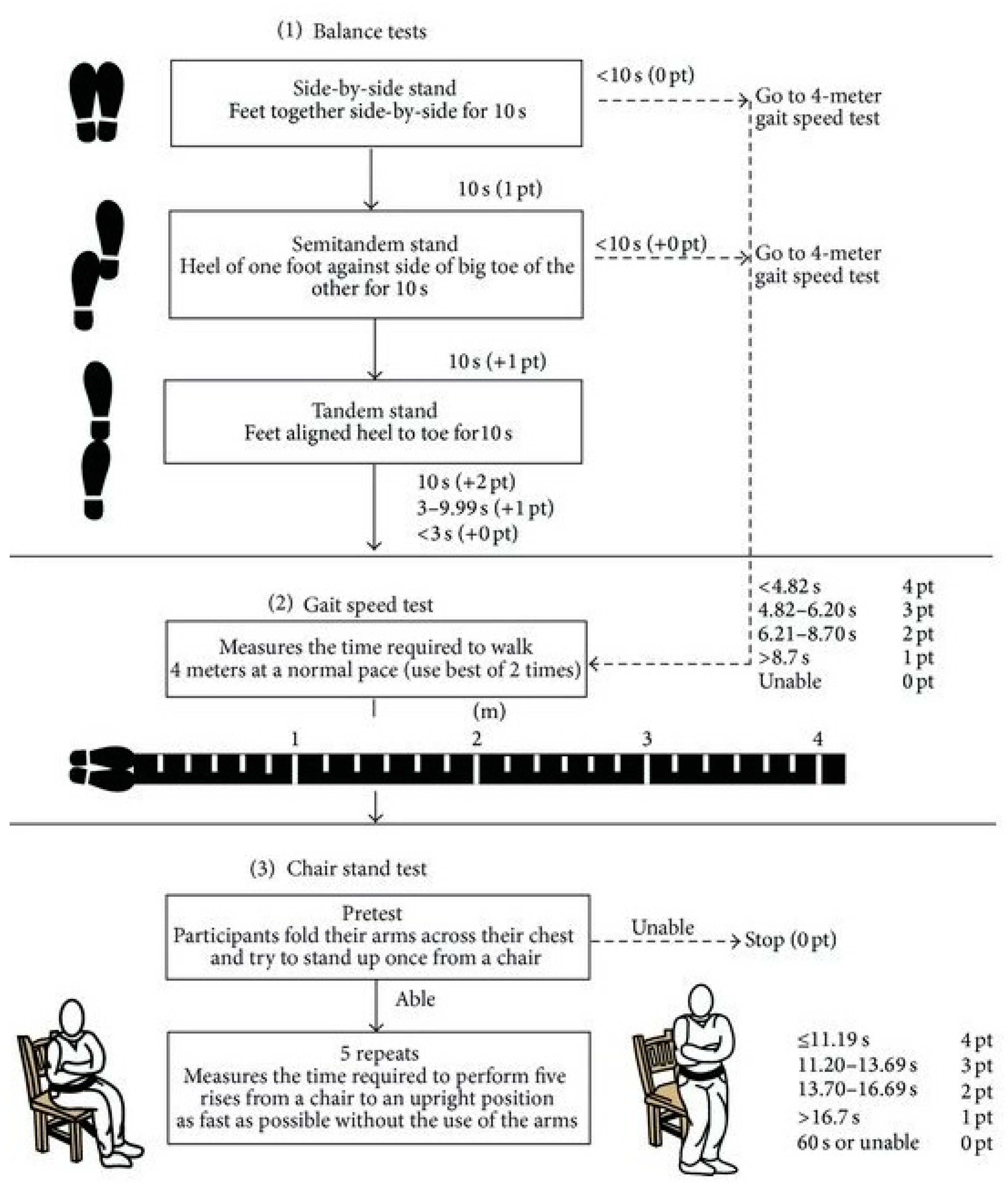
2.2.1. Evaluation Test
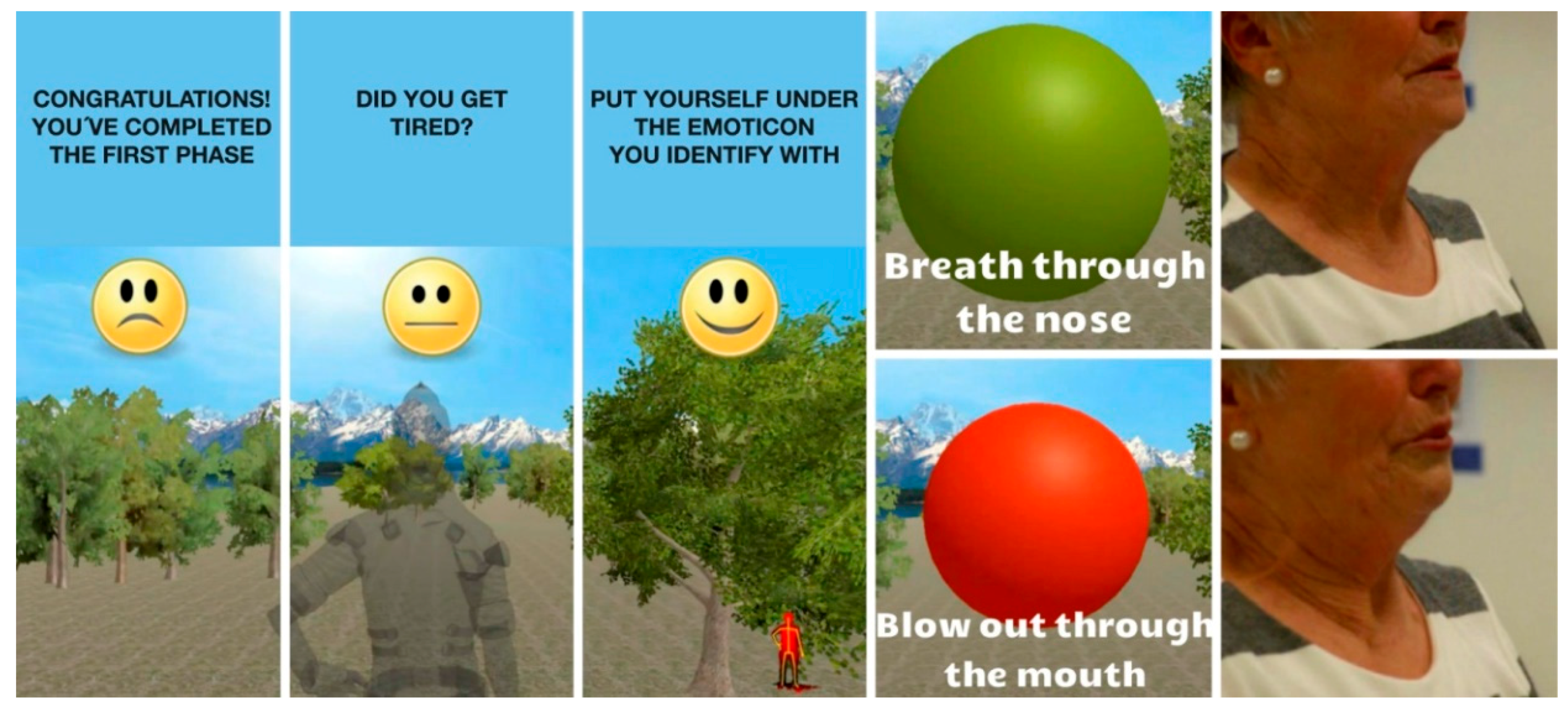
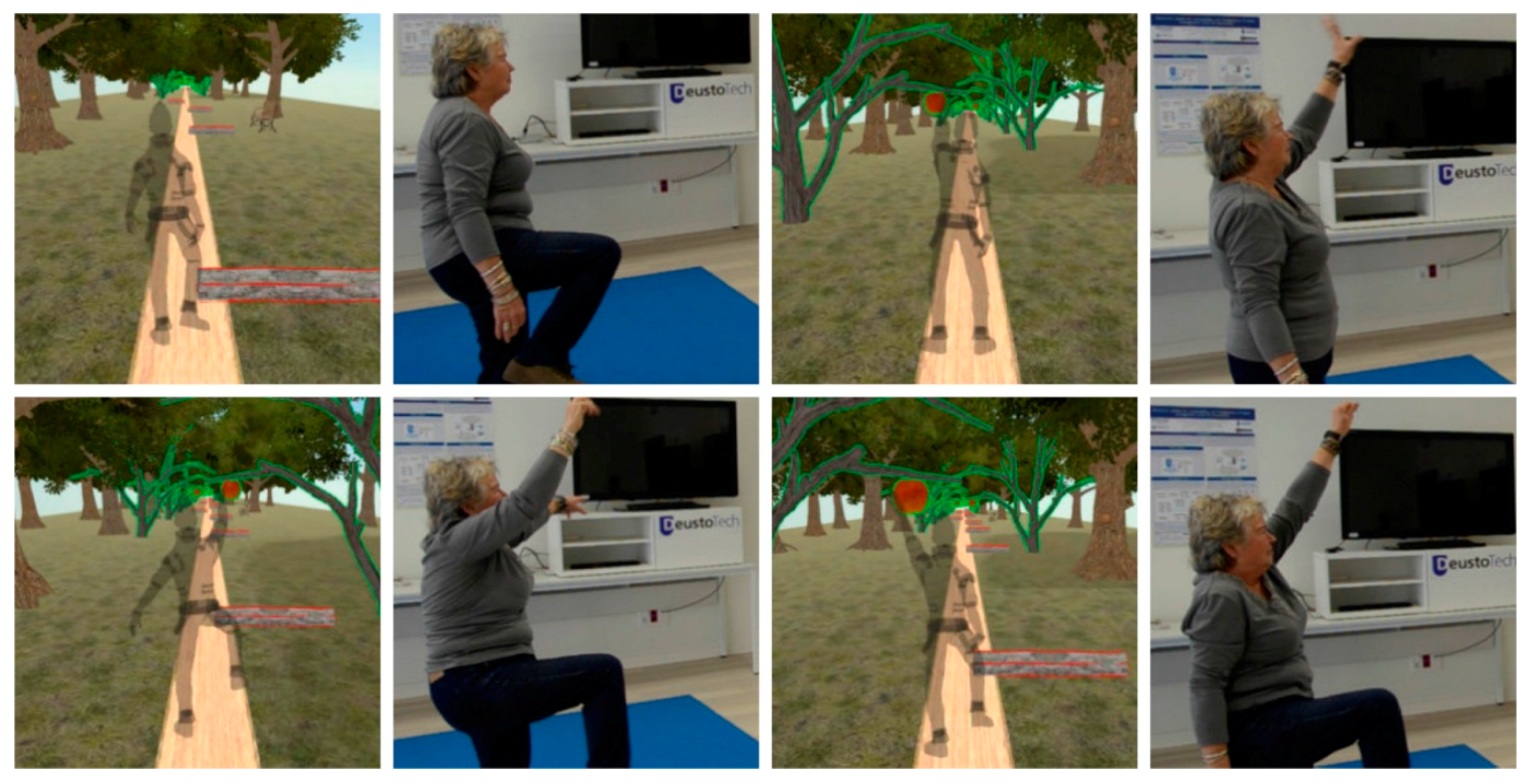
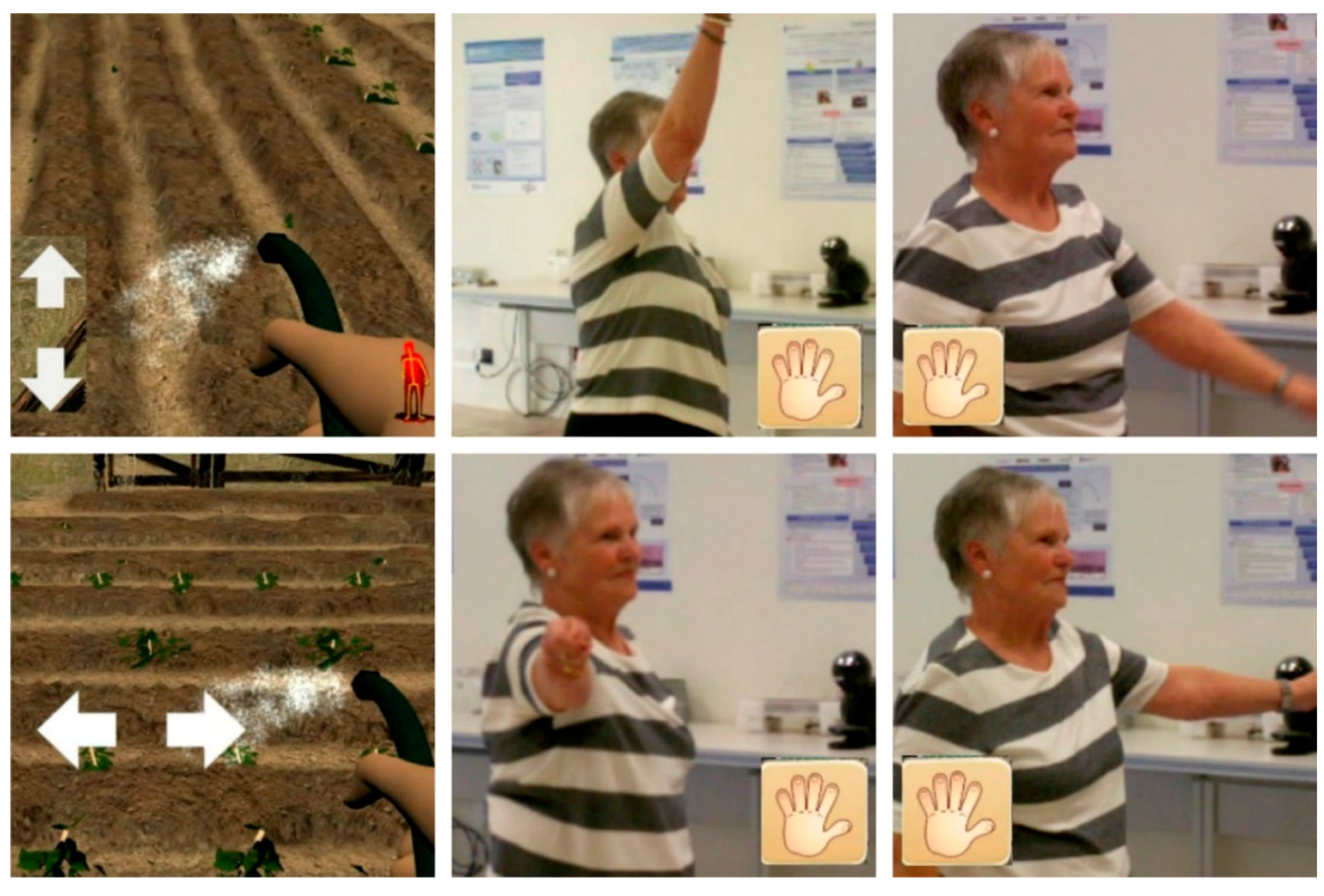
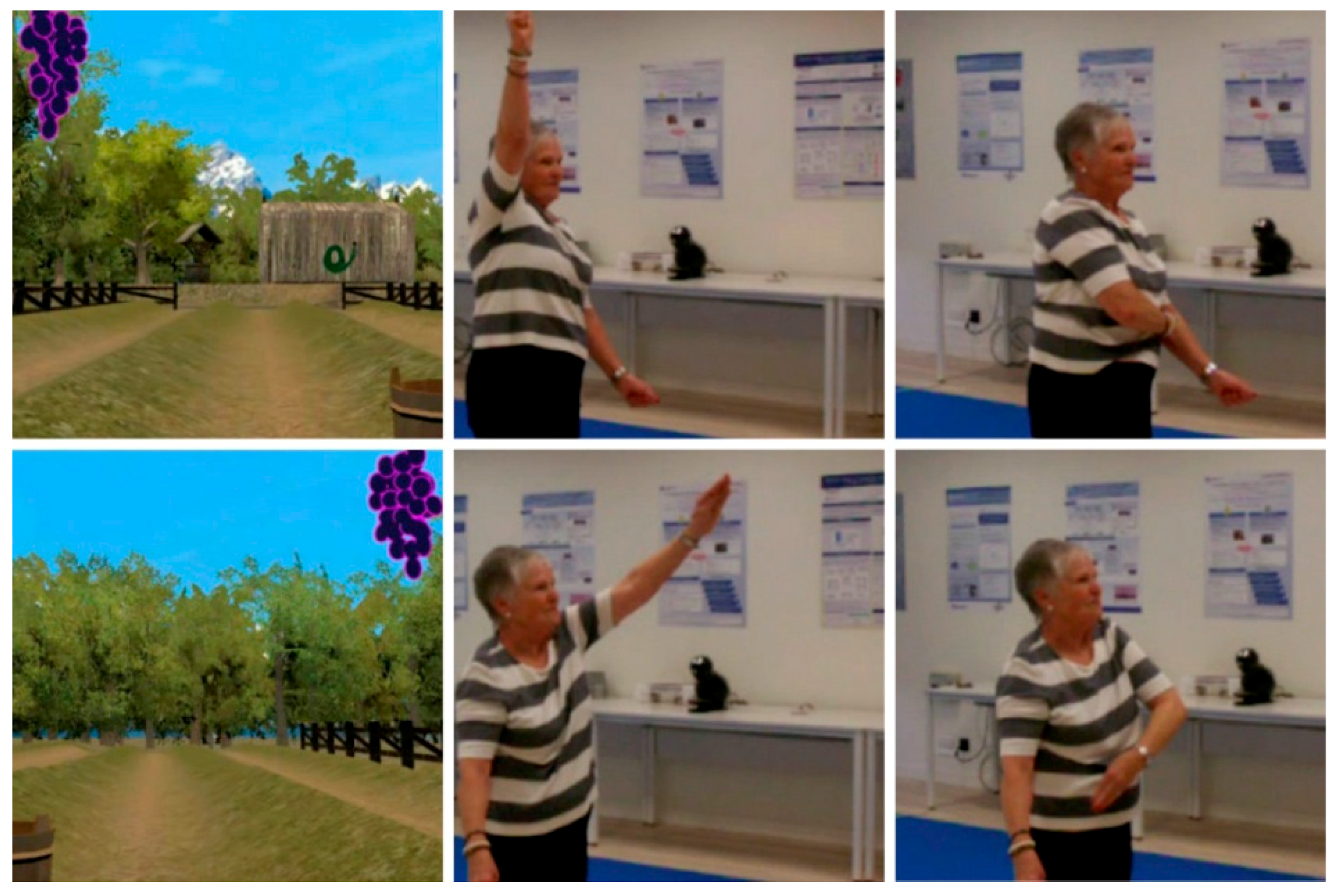
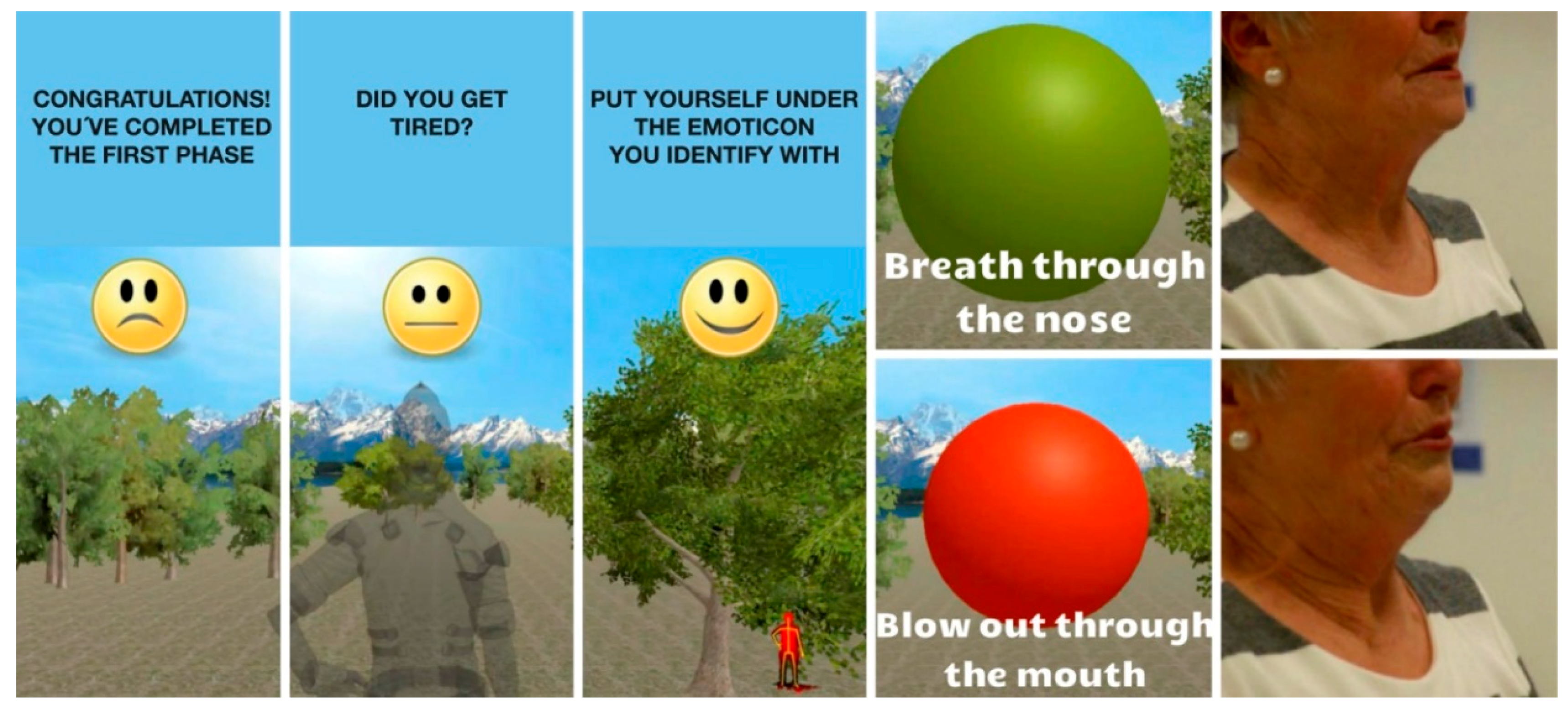
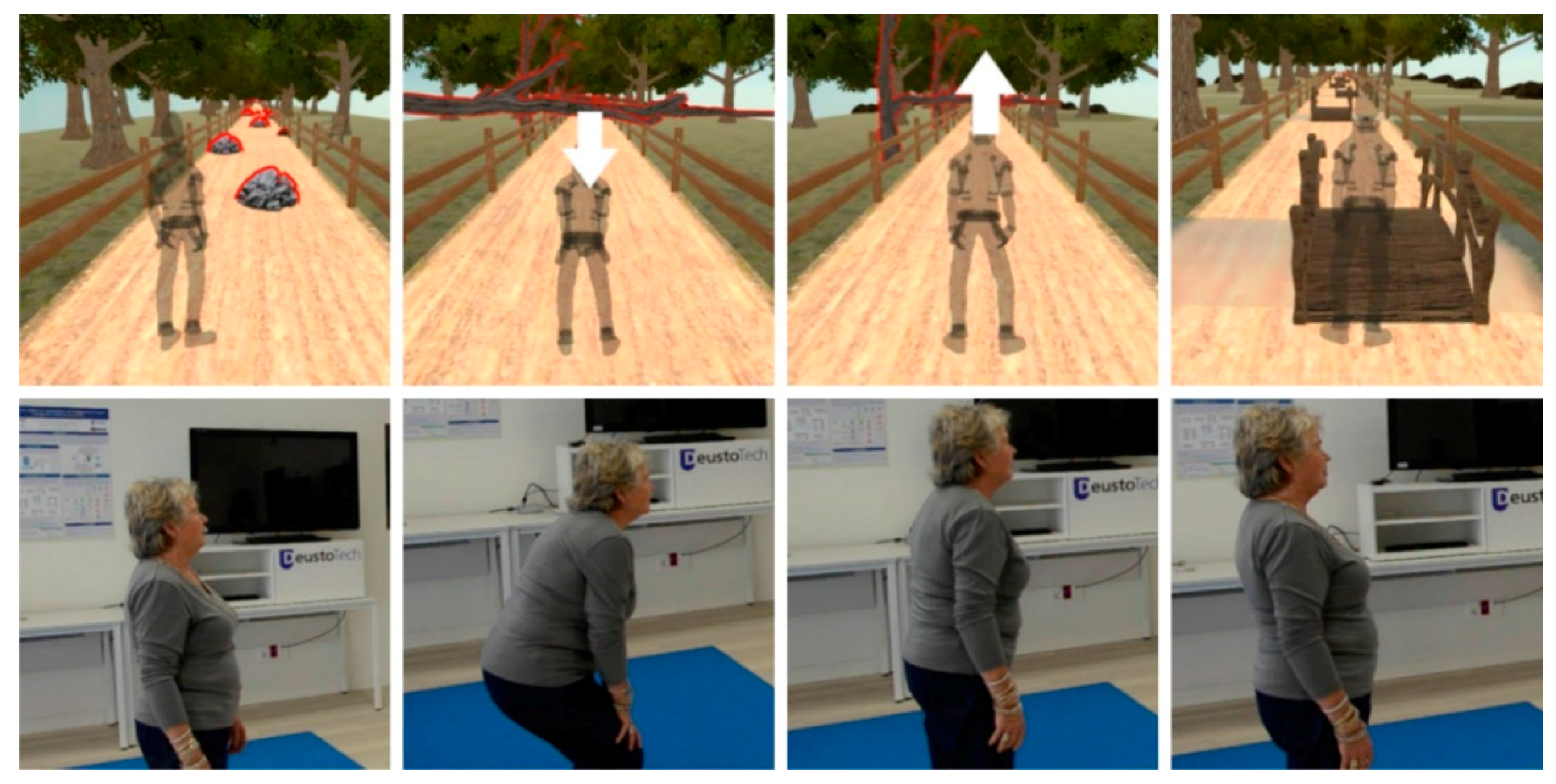
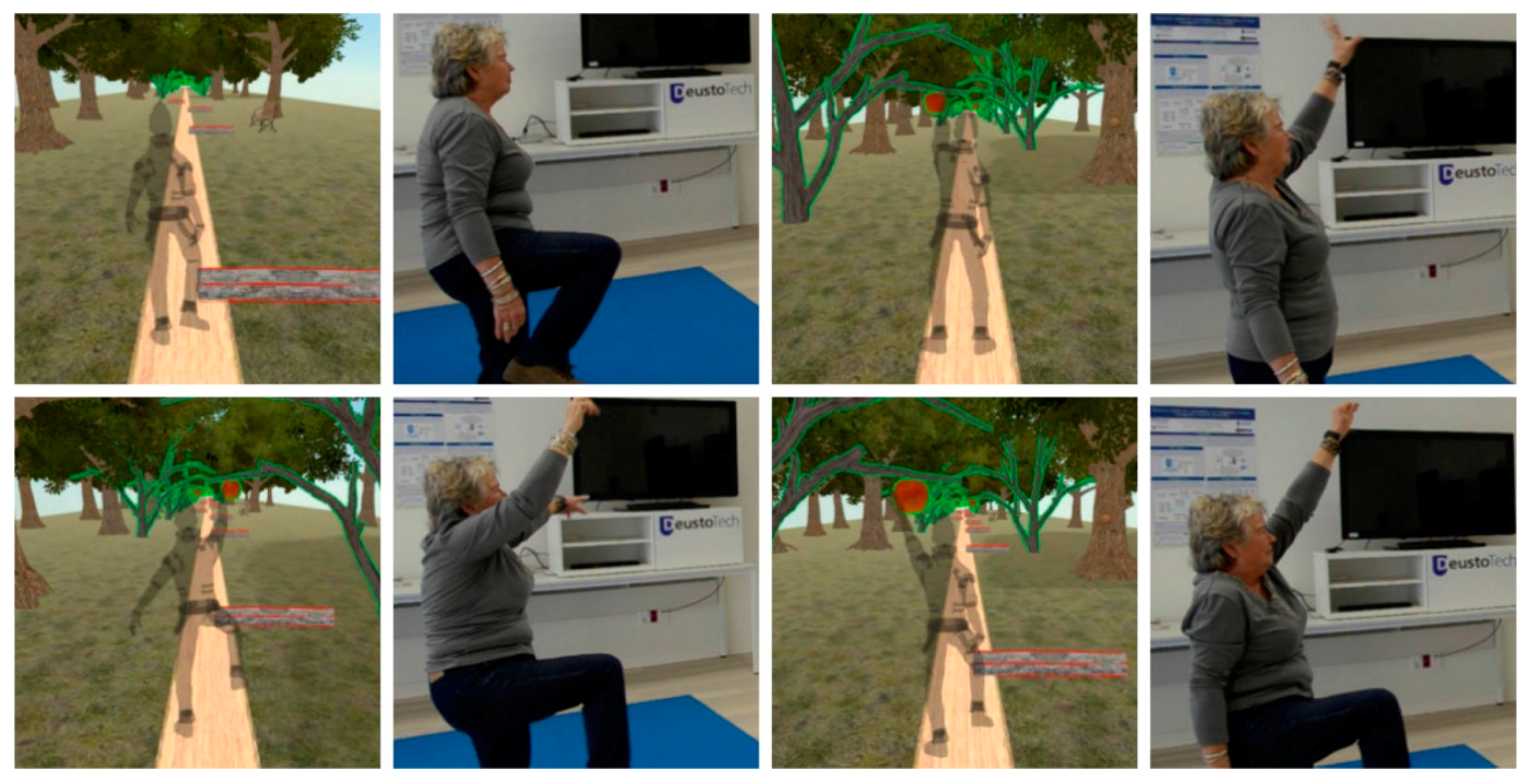
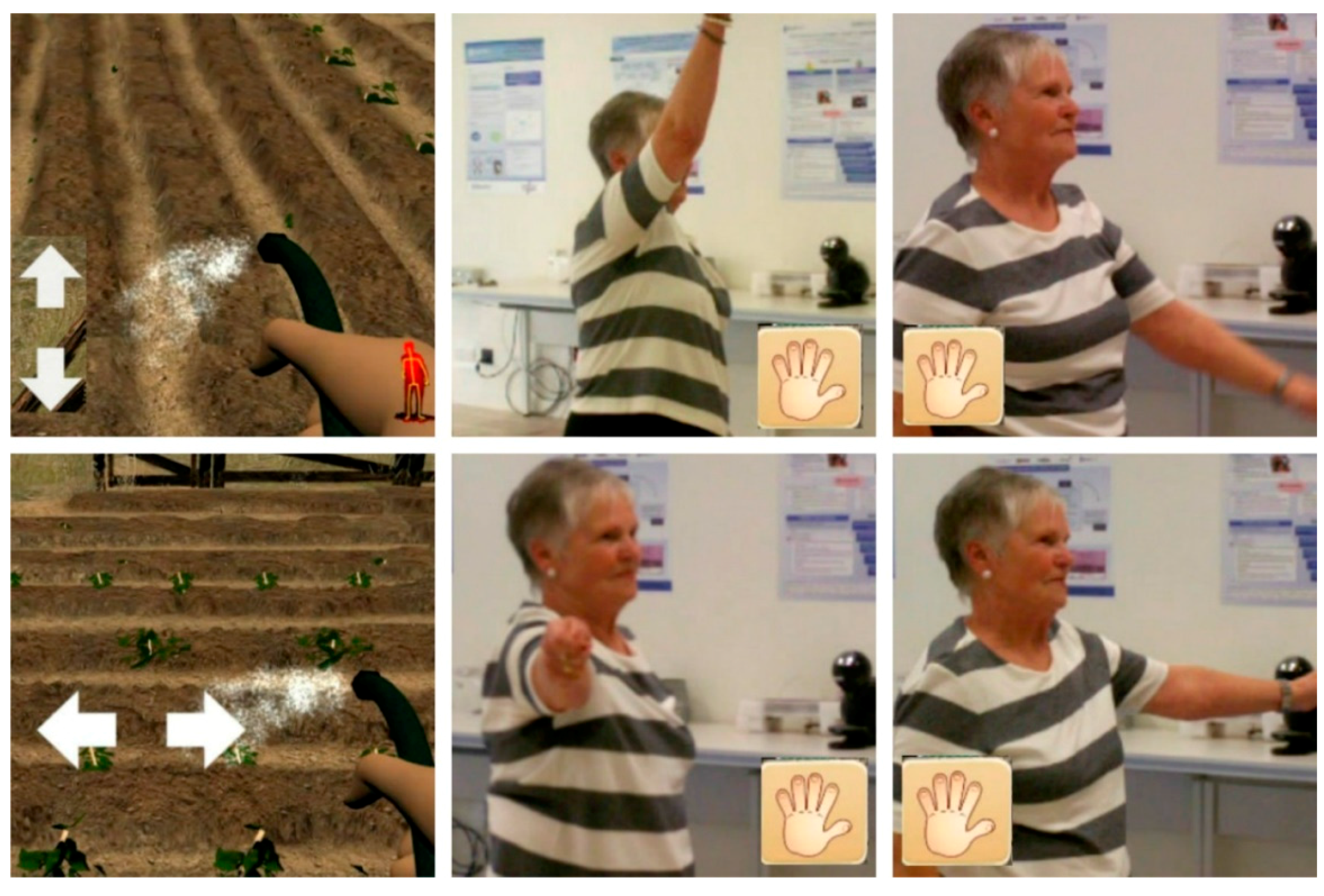
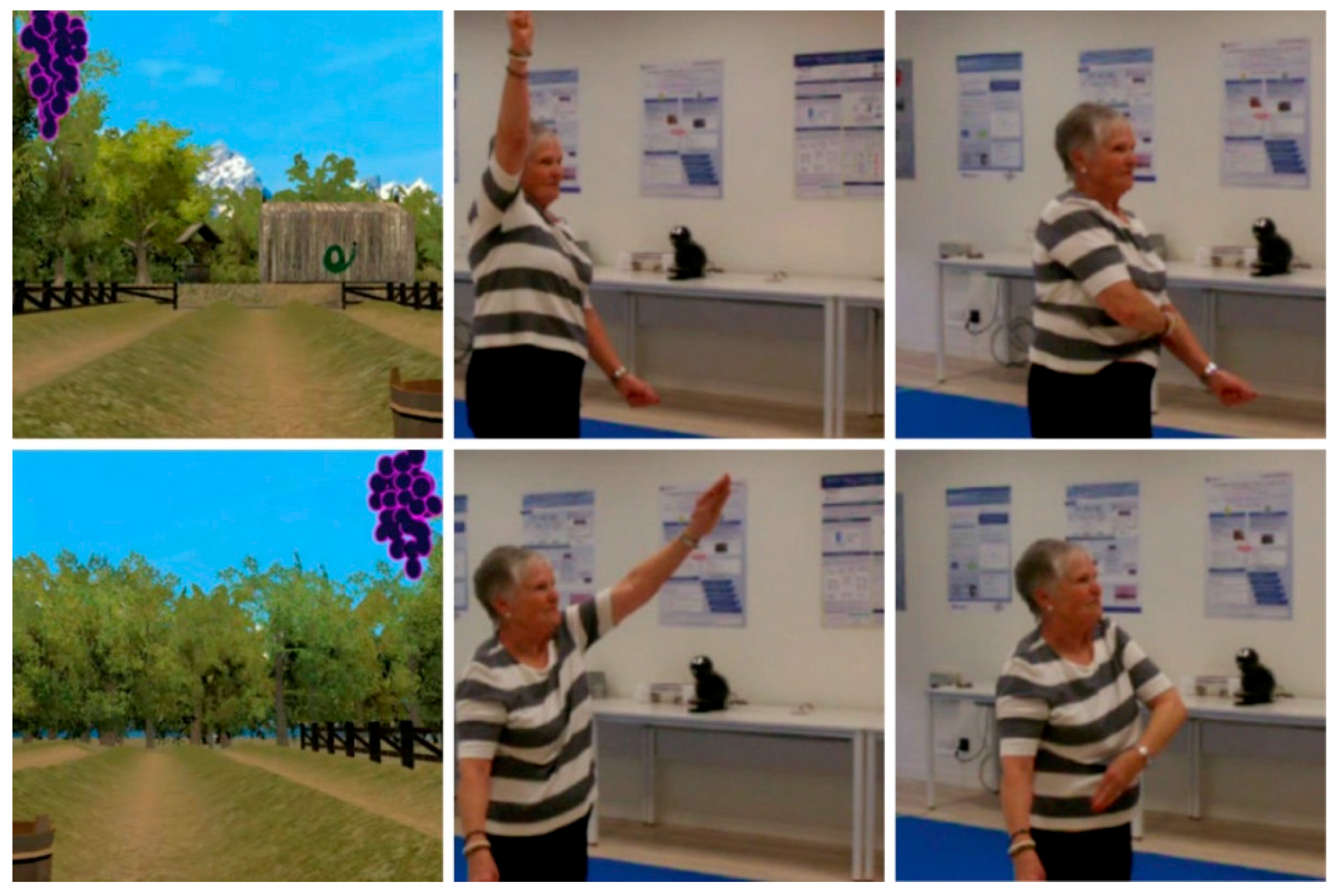
2.2.2. The Game
2.3. Statistical Analysis
3. Results
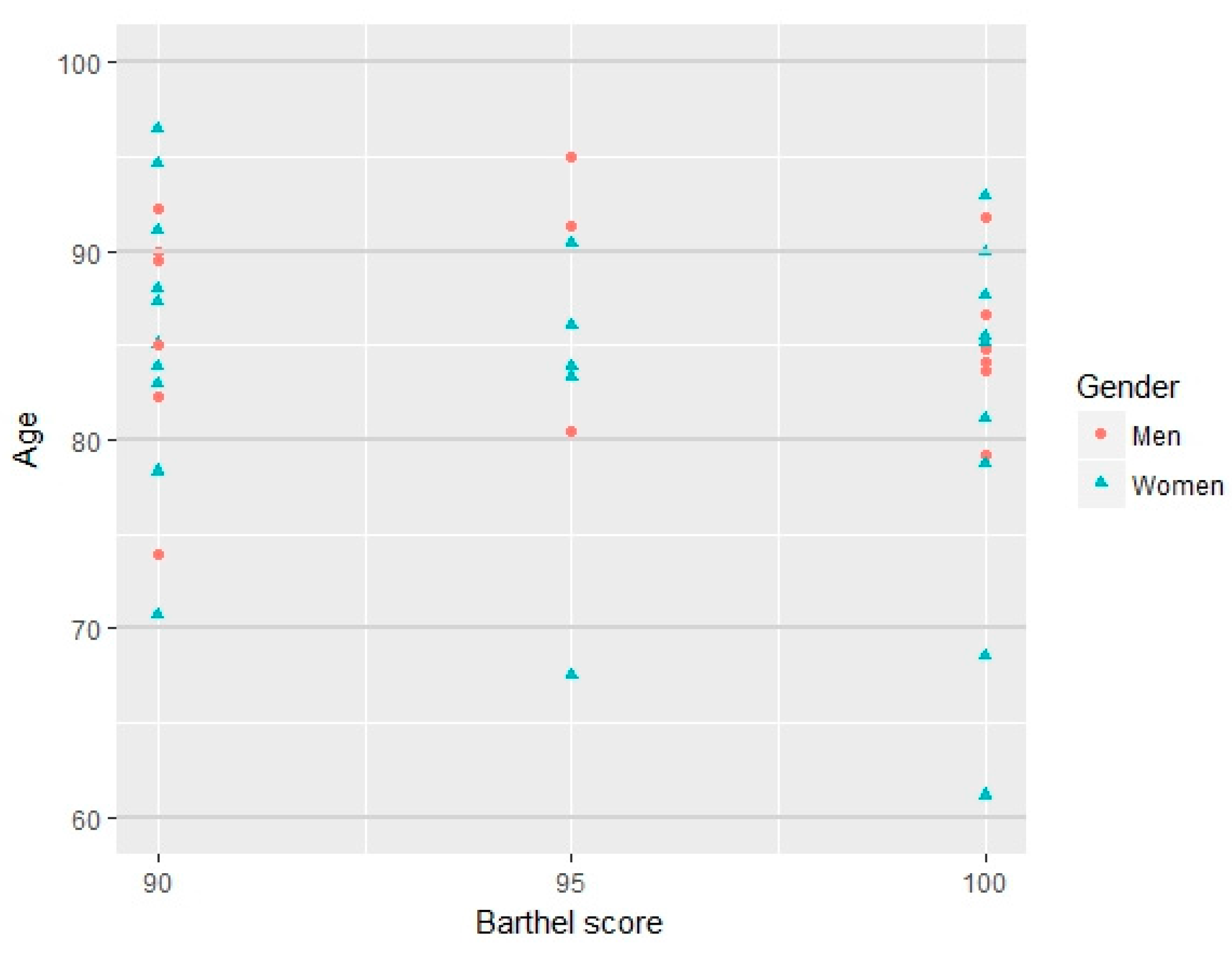
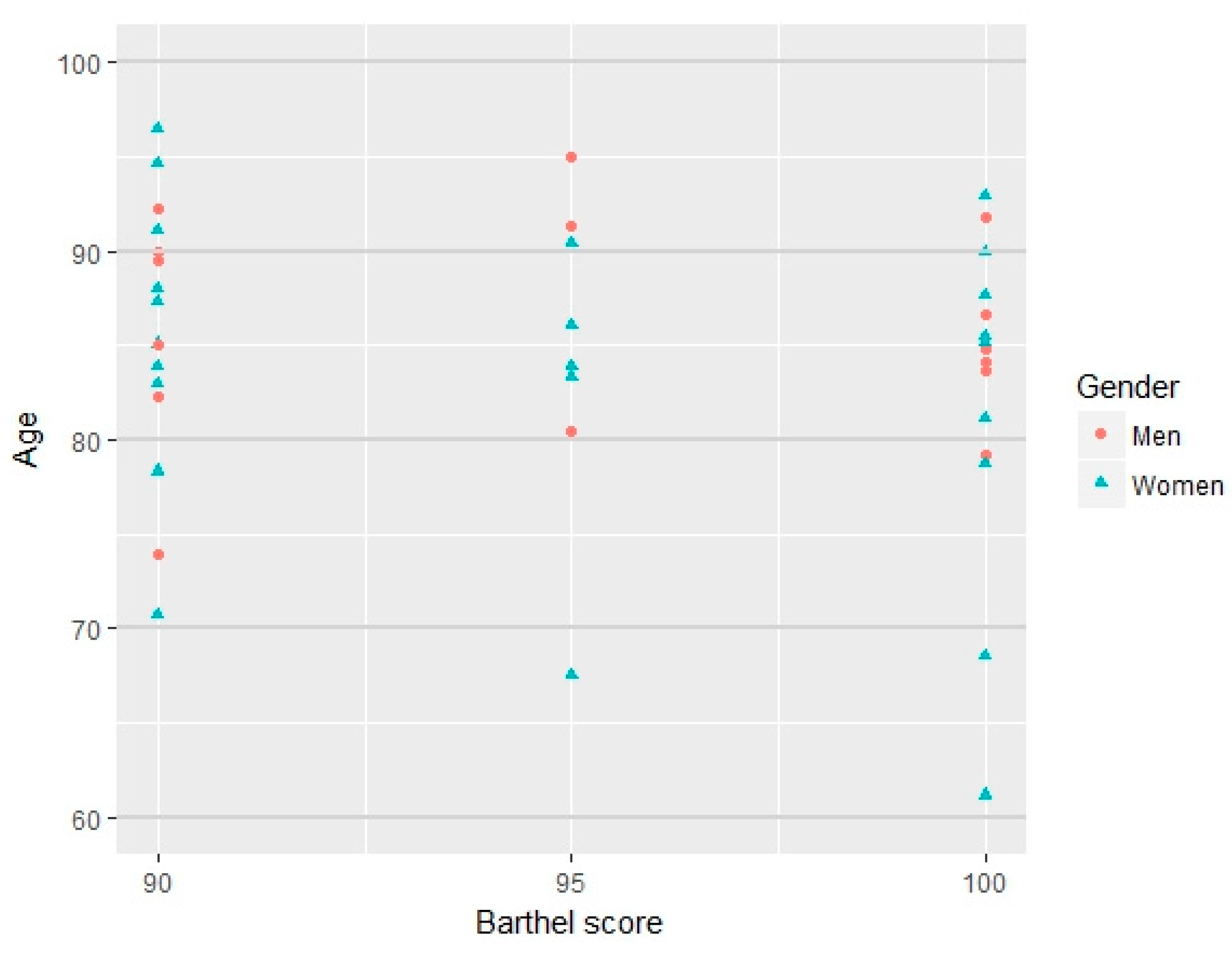
3.1. Description of the Sample in Week 1
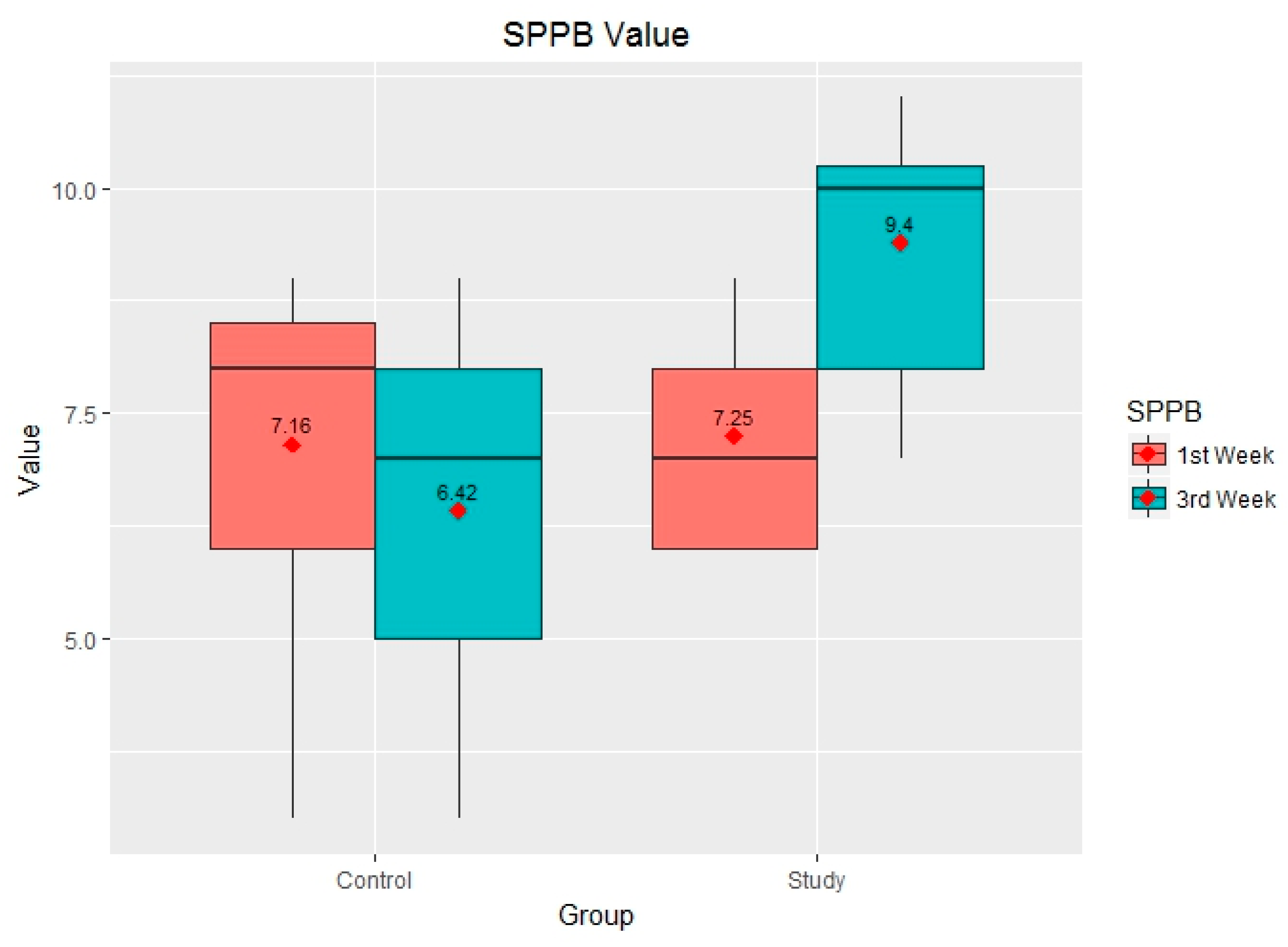
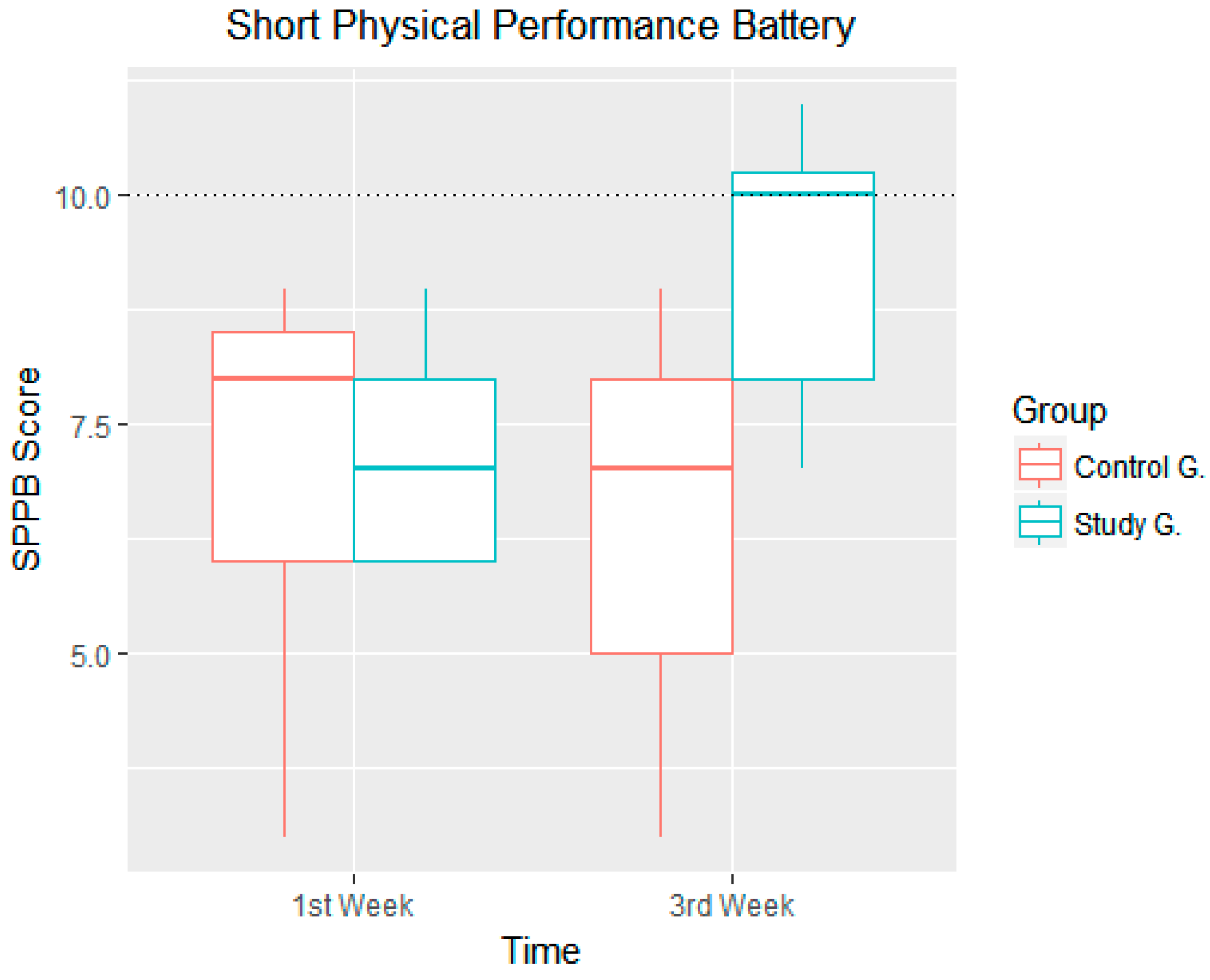
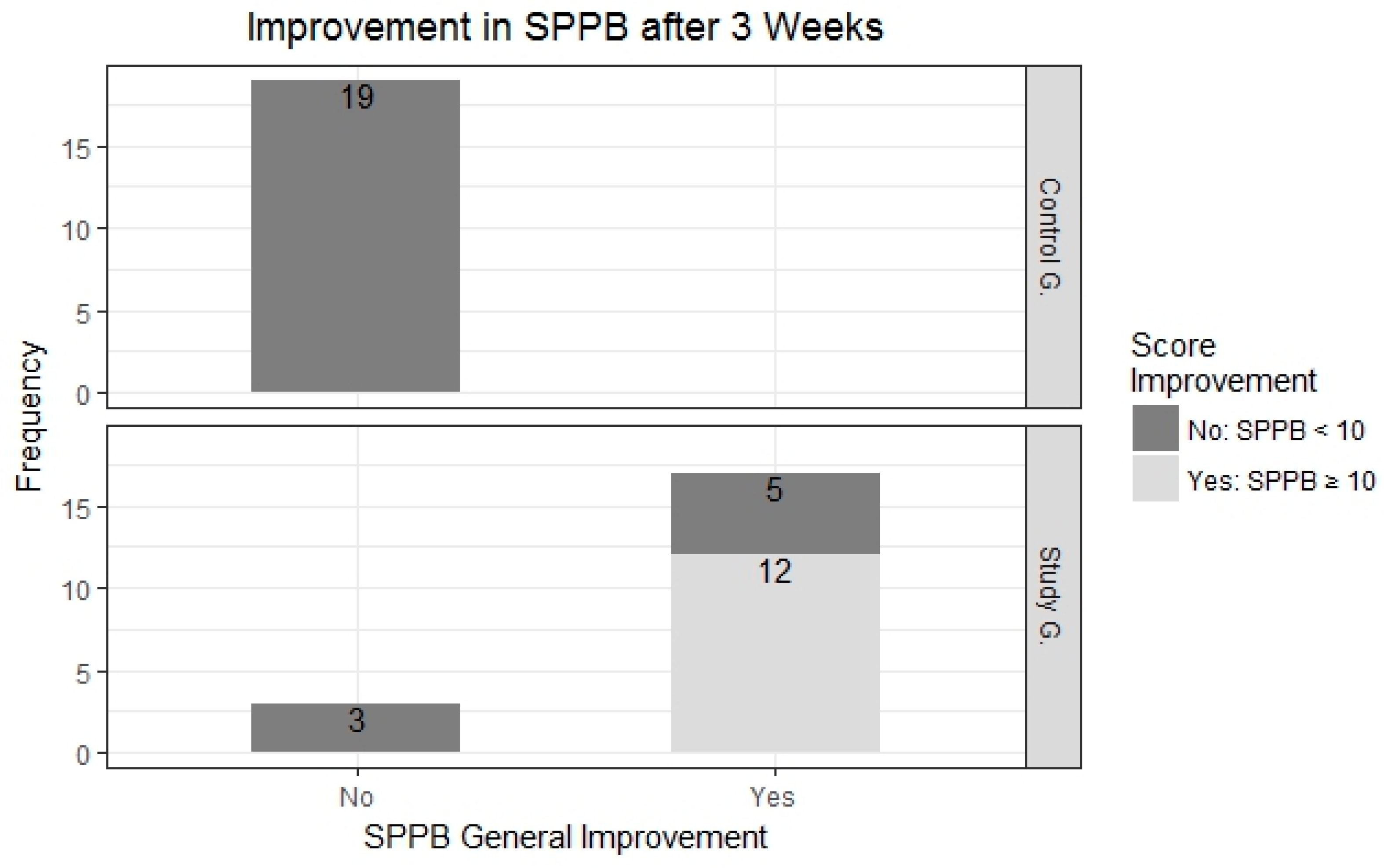
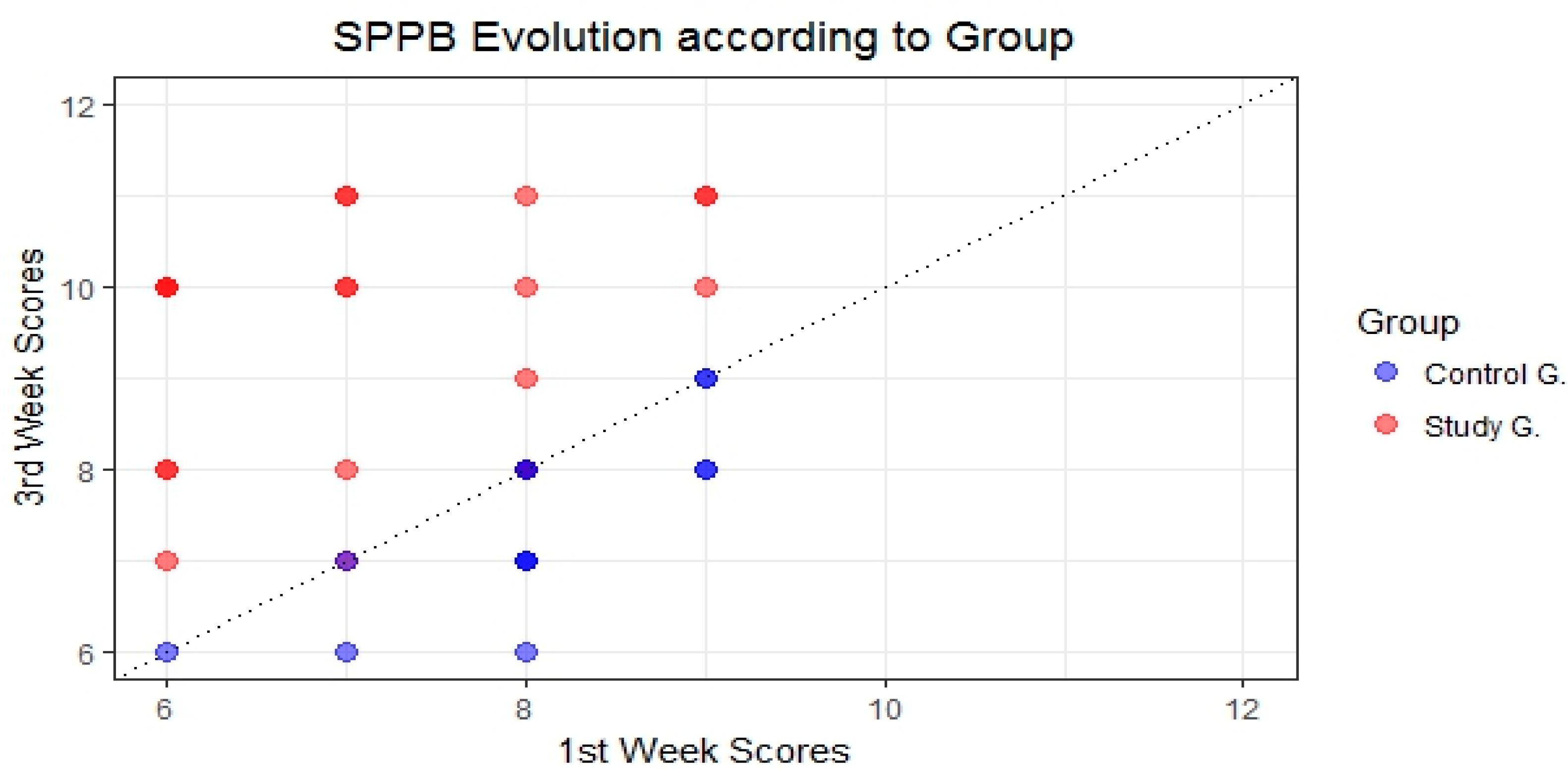
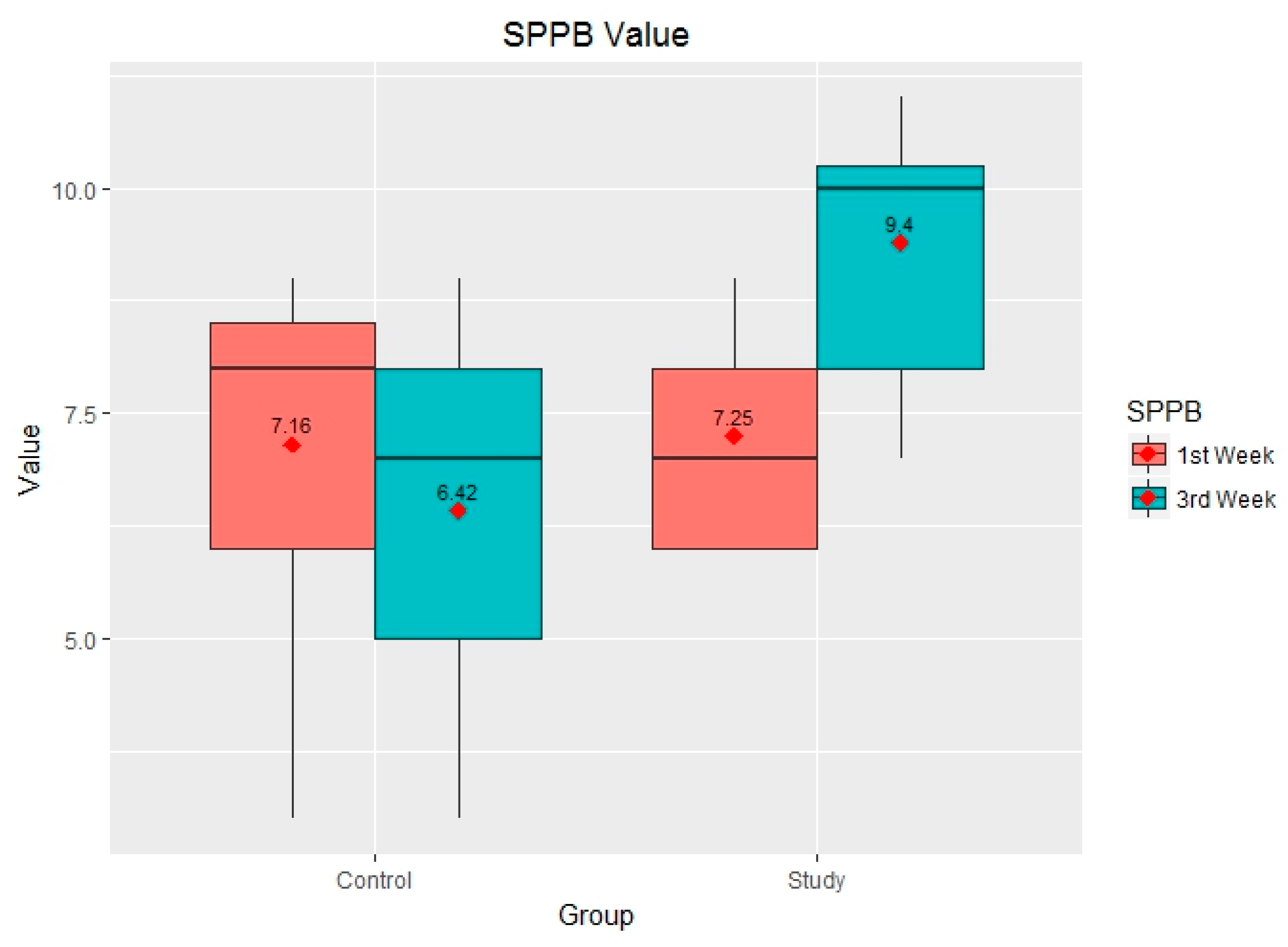
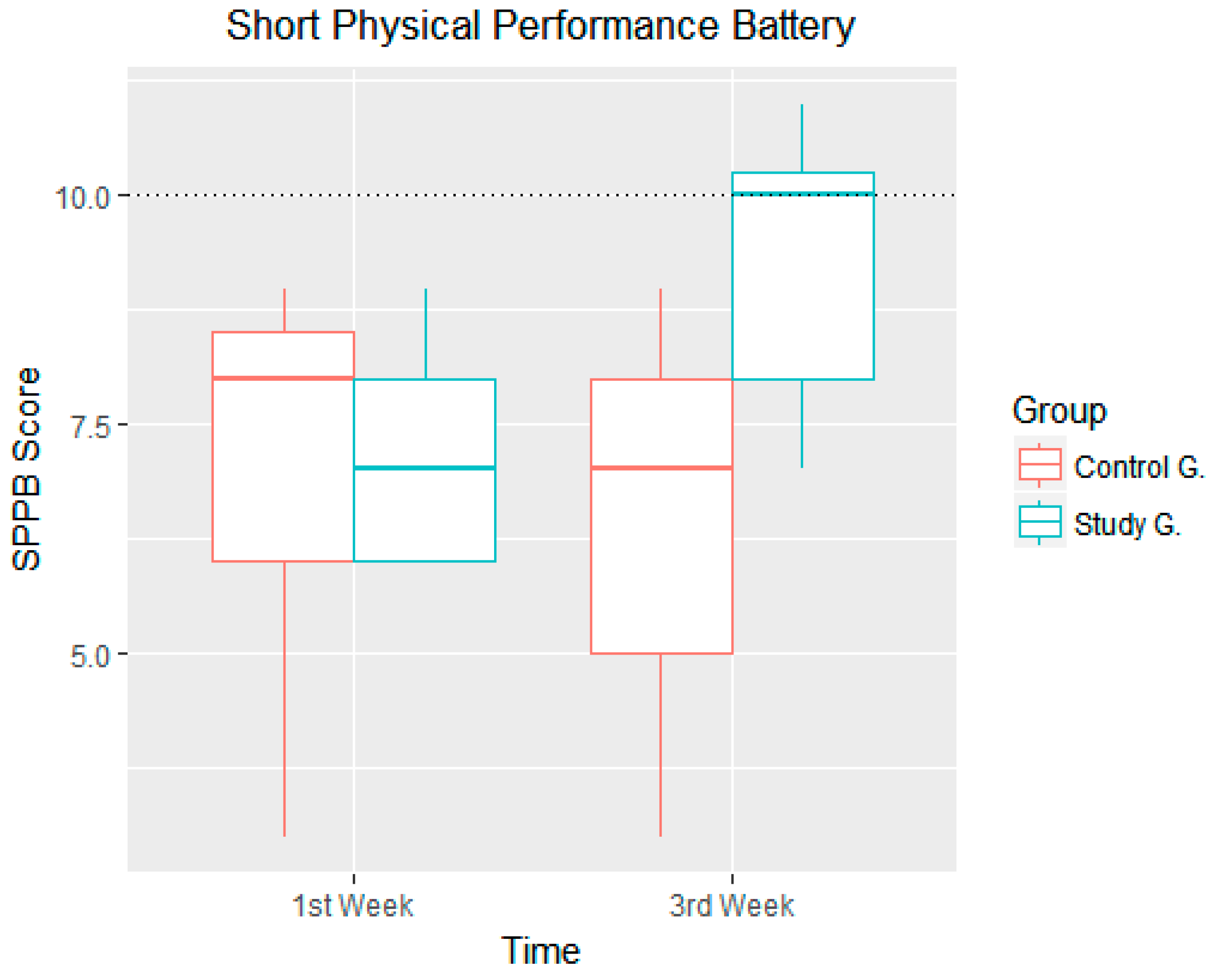
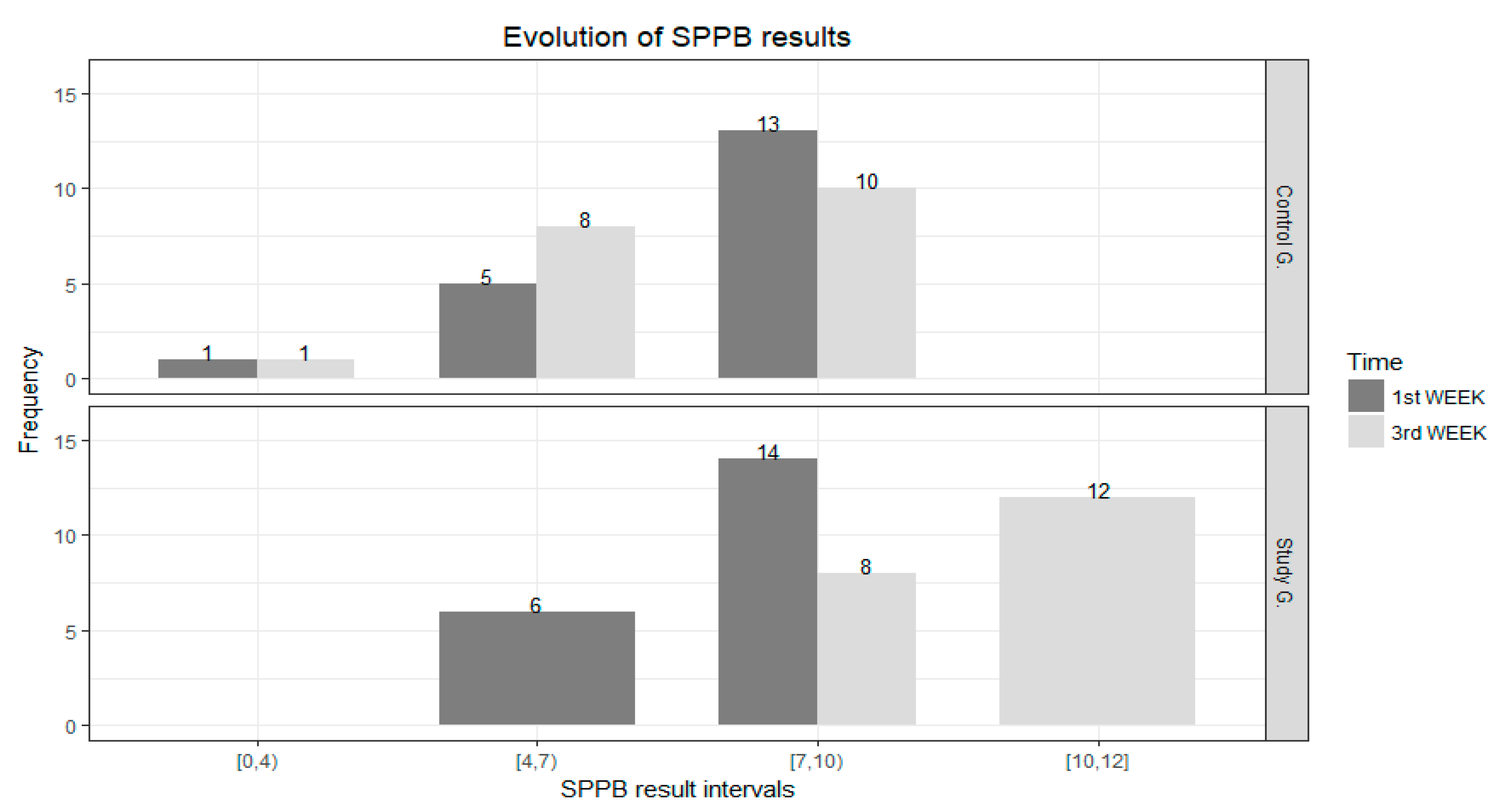
3.2. SPPB after Three Weeks
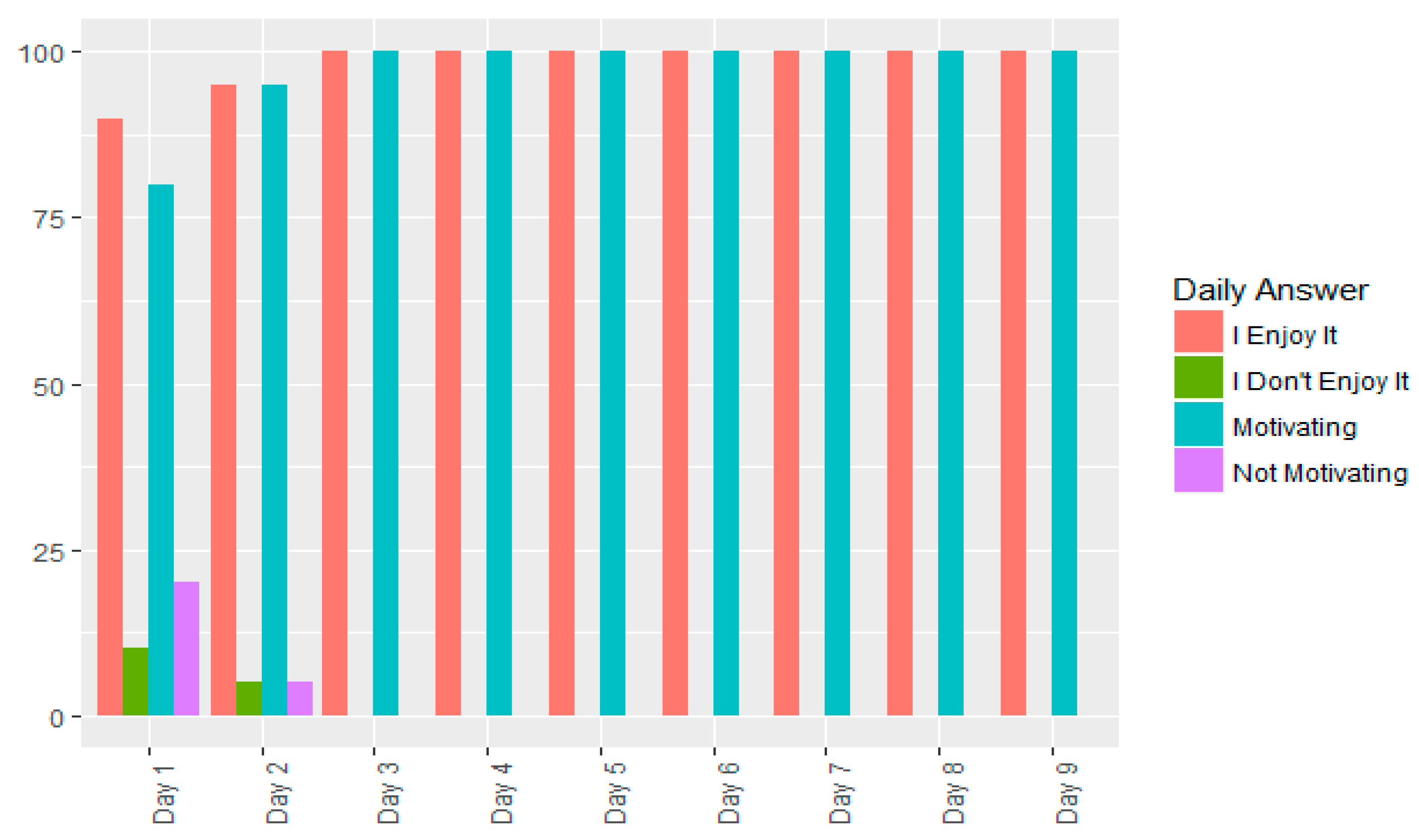
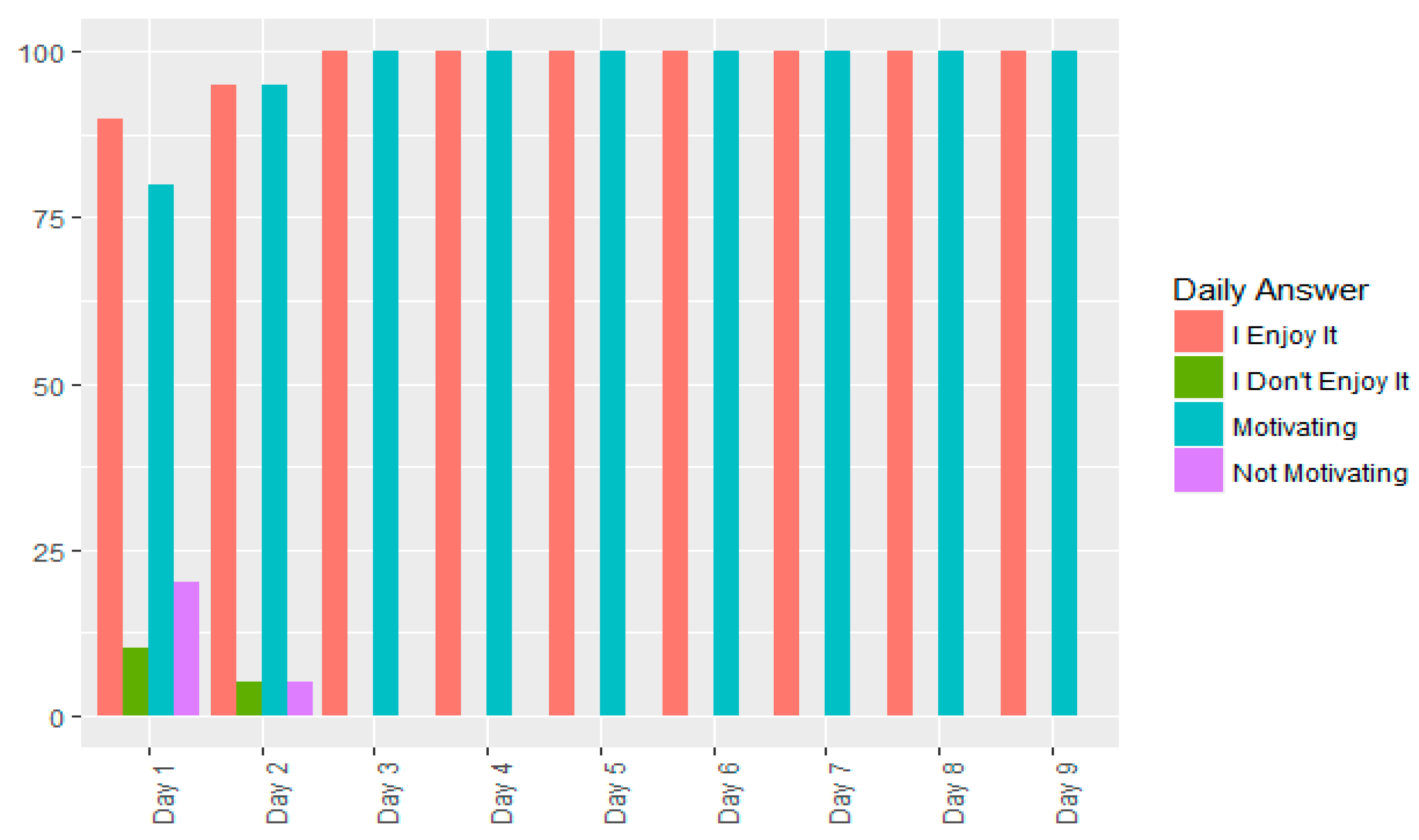
3.3. Game Satisfaction
- Do you like the game?
- Do you find it motivating for the purpose of improving your physical condition?
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Morley, J.E.; Vellas, B.; van Kan, G.A.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.C.; Doehner, W.; Evans, J.; et al. Frailty consensus: A call to action. J. Am. Med. Dir. Assoc. 2013, 14, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Vaca, J.; de la Rica-Escuin, M.; Silva-Iglesias, M.; Arjonilla-Garcia, M.D.; Varela-Perez, R.; Oliver-Carbonell, J.L.; Abizanda, P. Frailty in INstitutionalized older adults from ALbacete. The FINAL Study: Rationale, design, methodology, prevalence and attributes. Maturitas 2014, 77, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Prince, M.; Thiyagarajan, J.A.; De Carvalho, I.A.; Bernabei, R.; Chan, P.; Gutierrez-Robledo, L.M.; Michel, J.P.; Morley, J.E.; Ong, P.; et al. Frailty: An emerging public health priority. J. Am. Med. Dir. Assoc. 2016, 17, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Mugueta-Aguinaga, I.; Garcia-Zapirain, B. Is technology present in frailty? Technology a back-up tool for dealing with frailty in the elderly: A systematic review. Aging Dis. 2017, 8, 176–195. [Google Scholar] [CrossRef] [PubMed]
- Lange, B.; Requejo, P.; Flynn, S.M.; Rizzo, A.; Valero-Cuevas, F.; Baker, L.; Winstein, C. The potential of virtual reality and gaming to assist successful aging with disability. Phys. Med. Rehabil. Clin. N. Am. 2010, 21, 339–356. [Google Scholar] [CrossRef] [PubMed]
- Bruin, E.D.; Schoene, D.; Pichierri, G.; Smith, S. Use of virtual reality technique for the training of motor control in the elderly. Z. Gerontol. Geriatr. 2010, 4, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Primack, B.A.; Carroll, M.V.; McNamara, M.; Klem, M.L.; King, B.; Rich, M.; Chan, C.W.; Nayak, S. Role of video games in improving health-related outcomes: A systematic review. Am. J. Prev. Med. 2012, 42, 630–638. [Google Scholar] [CrossRef] [PubMed]
- Ijsselsteijn, W.; Nap, H.H.; de Kort, Y.; Poels, K. Digital game design for elderly users. In Proceedings of the 2007 Conference on Future Play, Toronto, ON, Canada, 15–17 November 2007; ACM: New York, NY, USA, 2017. [Google Scholar]
- Van Diest, M.; Lamoth, C.J.; Stegenga, J.; Verkerke, G.J.; Postema, K. Exergaming for balance training of elderly: State of the art and future developments. J. Neuroeng. Rehabil. 2013, 10, 101. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, J.E.; Villada, J.F.; Trujillo, G.; Carlos, J. Exergames: Una herramienta tecnológica para la actividad física. Rev. Méd. Risaralda 2013, 19, 126–130. [Google Scholar]
- Gerling, K.; Livingston, I.; Nacke, L.; Mandryk, R. Full-body motion-based game interaction for older adults. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Austin, TX, USA, 5–10 May 2012; ACM: New York, NY, USA, 2012. [Google Scholar]
- Skjaeret, N.; Nawaz, A.; Ystmark, K.; Dahl, Y.; Helbostad, J.L.; Svanaes, D.; Vereijken, B. Designing for movement quality in exergames: Lessons learned from observing senior citizens playing stepping games. Gerontology 2015, 61, 186–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Diest, M.; Stegenga, J.; Wortche, H.J.; Verkerke, G.J.; Postema, K.; Lamoth, C.J. Exergames for unsupervised balance training at home: A pilot study in healthy older adults. Gait Posture 2016, 44, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Daniel, K. Wii-hab for pre-frail older adults. Rehabil. Nurs. 2012, 37, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Wee, C.E.; Ames, T.D.; Le, K.M.; Wang, T.; Phieffer, L.S.; Quatman, C.E. Fear of falling correlates with subtle neuromuscular balance and strength deficits of fragility fracture patients. Aging Dis. 2016, 7, 585–592. [Google Scholar] [CrossRef] [PubMed]
- De Vette, F.; Tabak, M.; Dekker-van Weering, M.; Vollenbroek-Hutten, M. Engaging elderly people in telemedicine through gamification. J. Med. Internet Res. Serious Games 2015, 18, e9. [Google Scholar] [CrossRef] [PubMed]
- Cabañero-Martínez, M.J.; Cabrero-García, J.; Richart-Martínez, M.; Muñoz-Mendoza, C.L. The Spanish versions of the Barthel index (BI) and the Katz index (KI) of activities of dailyliving (ADL): A structured review. Arch. Gerontol. Geriatr. 2009, 49, e77–e84. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I. Functional evaluation: The Barthel index. MD State Med. J. 1965, 14, 61–65. [Google Scholar] [PubMed]
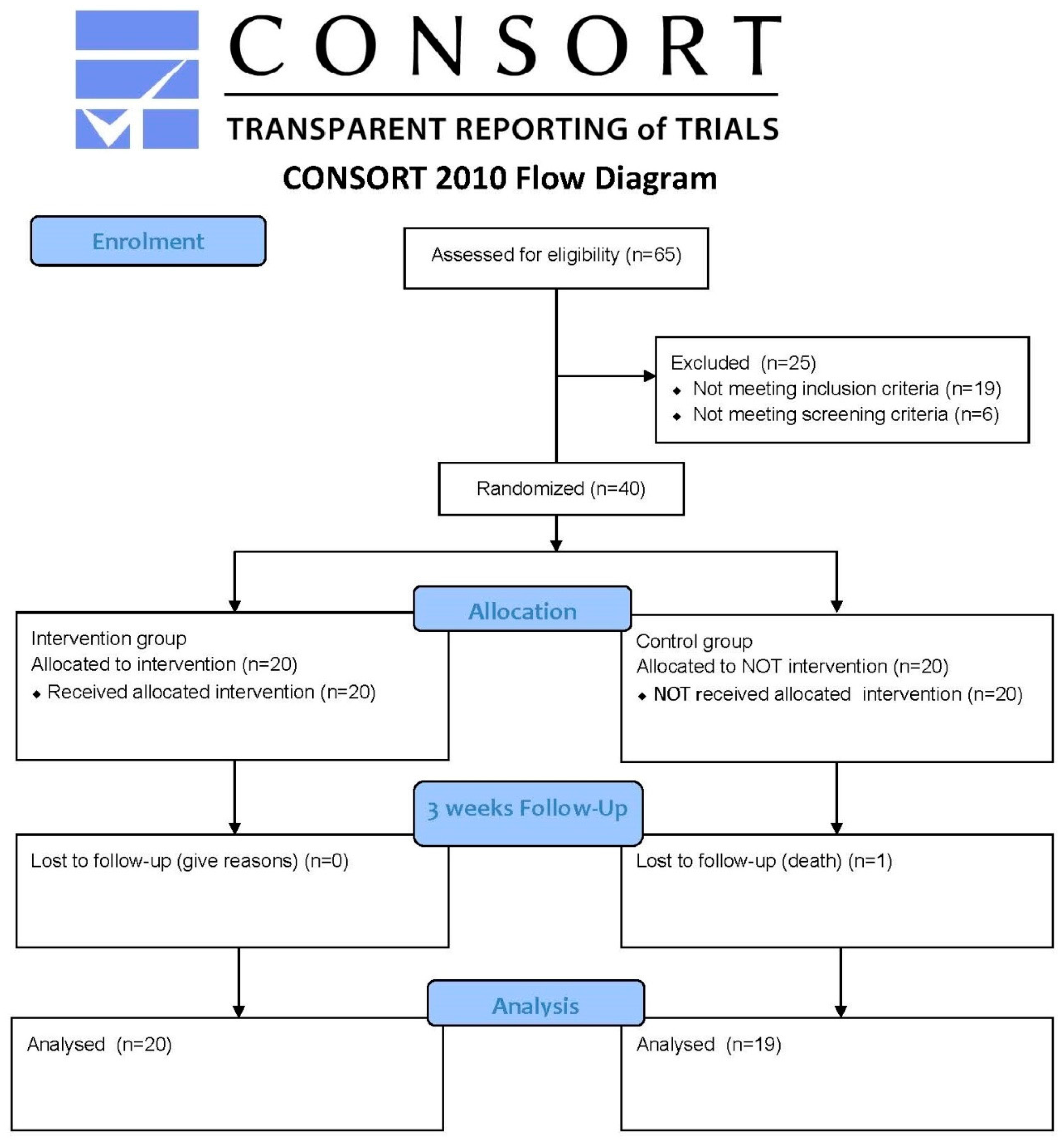
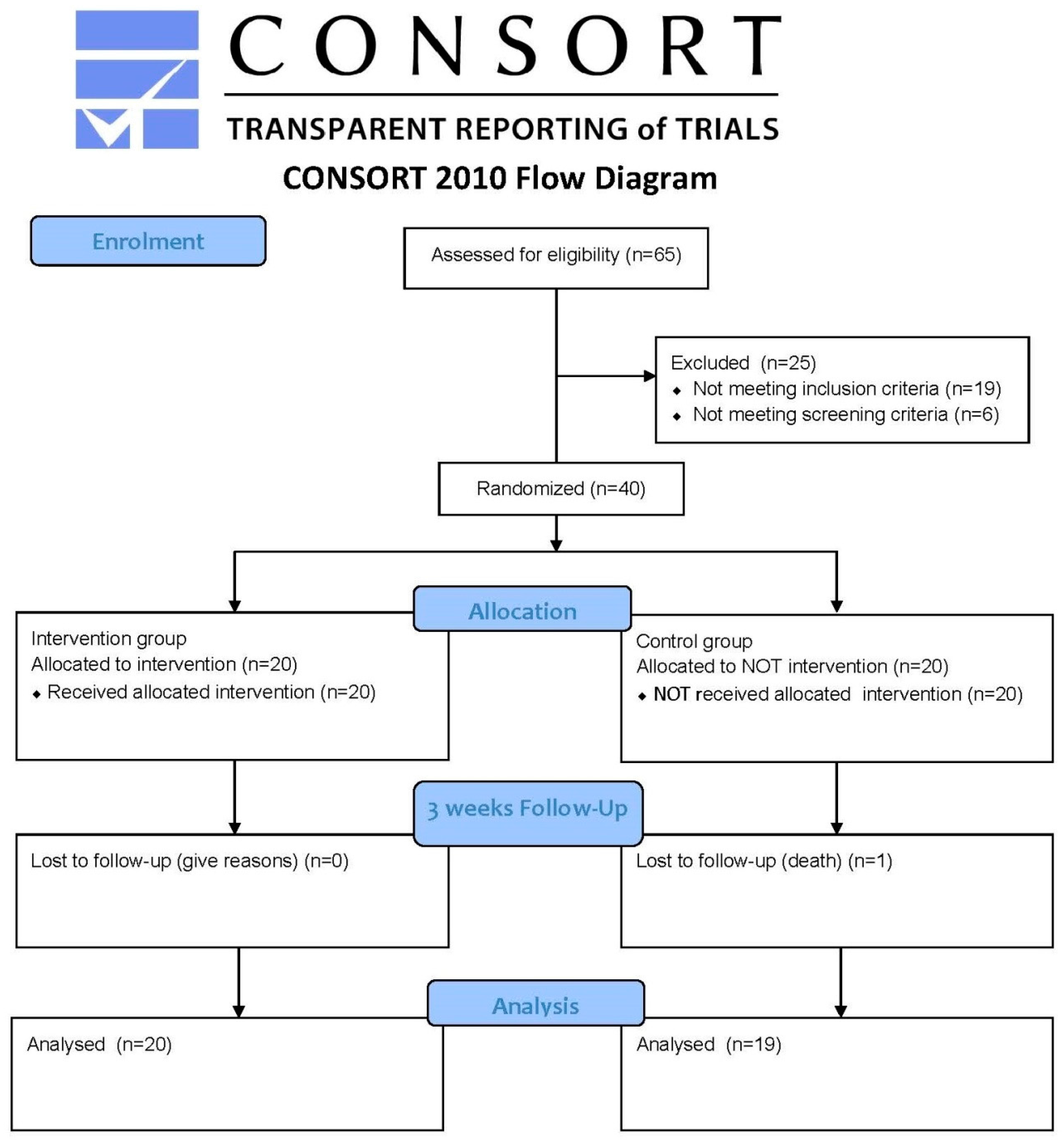
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef] [PubMed]
- CONSORT Group. The CONSORT Flow Diagram. 2017. Available online: http://www.consort-statement.org/consort-statement/flow-diagram (accessed on 21 November 2017).
- Cabrero-García, J.; Munoz-Mendoza, C.L.; Cabanero-Martínez, M.J.; González-Llopís, L.; Ramos-Pichardo, J.D.; Reig-Ferrer, A. Valores de referencia de la Short Physical Performance Battery para pacientes de 70 y más años en atención primaria de salud. Aten. Prim. 2012, 44, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Freiberger, E.; de Vreede, P.; Schoene, D.; Rydwik, E.; Mueller, V.; Frandin, K.; Hopman-Rock, M. Performance-based physical function in older community-dwelling persons: A systematic review of instruments. Age Ageing 2012, 41, 712–721. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Ferrucci, L.; Pieper, C.F.; Leveille, S.G.; Markides, K.S.; Ostir, G.V.; Studenski, S.; Berkman, L.F.; Wallace, R.B. Lower extremity function and subsequent disability: Consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J. Gerontol. Ser. A 2000, 55, M221–M231. [Google Scholar] [CrossRef]
- Kwon, S.; Perera, S.; Pahor, M.; Katula, J.; King, A.; Groessl, E.; Studenski, S.A. What is a meaningful change in physical performance? Findings from a clinical trial in older adults (the LIFE-P study). J. Nutr. Health Aging 2009, 13, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Kiel, D.P.; Schmader, K.; Lin, F. Falls in Older Persons: Risk Factors and Patient Evaluation; UpToDate: Waltham, MA, USA, 2014. [Google Scholar]
- Riskowski, J.; Hagedorn, T.; Dufour, A.; Hannan, M. Functional foot symmetry and its relation to lower extremity physical performance in older adults: The Framingham Foot Study. J. Biomech. 2012, 45, 1796–1802. [Google Scholar] [CrossRef] [PubMed]
- Berg, P.V.D.; Kemperman, A.; de Kleijn, B.; Borgers, A. Locations that support social activity participation of the aging population. Int. J. Environ. Res. Public Health 2015, 12, 10432–10449. [Google Scholar] [CrossRef] [PubMed]
- Saito, Y.; Oguma, Y.; Inoue, S.; Tanaka, A.; Kobori, Y. Environmental and individual correlates of various types of physical activity among community-dwelling middle-aged and elderly Japanese. Int. J. Environ. Res. Public Health 2013, 10, 2028–2042. [Google Scholar] [CrossRef] [PubMed]
- Lun, R.; Zhao, W. A survey of applications and human motion recognition with microsoft kinect. Int. J. Patttern Recognit. Artif. Intell. 2015, 29, 1555008. [Google Scholar] [CrossRef]
- Lapitz, M.; Juan, J. La Resurrección del Txakoli/por Juan José Lapitz. Available online: http://www.memoriadigitalvasca.es/handle/10357/3769/browse?type=subject&order=ASC&rpp=20&value=Txakoli+Elaboraci%C3%B3n+Art%C3%ADculos+period%C3%ADsticos (accessed on 9 September 2014).
- Wilson, R.C.; Jones, P.W. A comparison of the visual analogue scale and modified Borg scale for the measurement of dyspnoea during exercise. Clin. Sci. 1989, 76, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.; Fitzpatrick, N.; Andrews, M.; DiCroce, N. Determinants of sedentary behavior, motivation, barriers and strategies to reduce sitting time in older women: A qualitative investigation. Int. J. Environ. Res. Public Health 2014, 11, 773–791. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Vellas, B.; Hsu, F.C.; Newman, A.B.; Doss, H.; King, A.C.; Manini, T.M.; Church, T.; Gill, T.M.; Miller, M.E.; et al. A physical activity intervention to treat the frailty syndrome in older persons-results from the LIFE-P study. J. Gerontol. Ser. A 2015, 70, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Giné-Garriga, M.; Guerra, M.; Unnithan, V.B. The effect of functional circuit training on self-reported fear of falling and health status in a group of physically frail older individuals: A randomized controlled trial. Aging Clin. Exp. Res. 2013, 25, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Barber, S.; Young, J.; Iliffe, S.; Forster, A. The Home-based Older People’s Exercise (HOPE) trial: A pilot randomised controlled trial of a home-based exercise intervention for older people with frailty. Age Ageing 2014, 43, 687–695. [Google Scholar] [CrossRef] [PubMed]
- Bieryla, K.A. Xbox Kinect training to improve clinical measures of balance in older adults: A pilot study. Aging Clin. Exp. Res. 2016, 28, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Scheer, K.S.; Siebrant, S.M.; Brown, G.A.; Shaw, B.S.; Shaw, I. Wii, Kinect, and Move. Heart rate, oxygen consumption, energy expenditure, and ventilation due to different physically active video game systems in college students. Int. J. Exerc. Sci. 2014, 7, 22–32. [Google Scholar] [PubMed]
- O’Donovan, C.; Hirsch, E.; Holohan, E.; McBride, I.; McManus, R.; Hussey, J. Energy expended playing Xbox Kinect™ and Wii™ games: A preliminary study comparing single and multiplayer modes. Physiotherapy 2012, 98, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Holmes, H.; Wood, J.; Jenkins, S.; Winship, P.; Lunt, D.; Bostock, S.; Hill, K. Xbox Kinect™ represents high intensity exercise for adults with cystic fibrosis. J. Cyst. Fibros. 2013, 12, 604–608. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group (n = 19) | Study Group (n = 20) | |
|---|---|---|
| Barthel | Slightly dependent 60% Independent 40% | Slightly dependent 60% Independent 40% |
| Age | 83.11 ± 9.01 years | 85.47 ± 6.46 years |
| Gender | Men 40% Women 60% | Men 40% Women 60% |
| Frailty RISK | 100% | 100% |
| Sppb | 7.16 ± 1.07 | 7.25 ± 1.86 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mugueta-Aguinaga, I.; Garcia-Zapirain, B. FRED: Exergame to Prevent Dependence and Functional Deterioration Associated with Ageing. A Pilot Three-Week Randomized Controlled Clinical Trial. Int. J. Environ. Res. Public Health 2017, 14, 1439. https://doi.org/10.3390/ijerph14121439
Mugueta-Aguinaga I, Garcia-Zapirain B. FRED: Exergame to Prevent Dependence and Functional Deterioration Associated with Ageing. A Pilot Three-Week Randomized Controlled Clinical Trial. International Journal of Environmental Research and Public Health. 2017; 14(12):1439. https://doi.org/10.3390/ijerph14121439
Chicago/Turabian StyleMugueta-Aguinaga, Iranzu, and Begonya Garcia-Zapirain. 2017. "FRED: Exergame to Prevent Dependence and Functional Deterioration Associated with Ageing. A Pilot Three-Week Randomized Controlled Clinical Trial" International Journal of Environmental Research and Public Health 14, no. 12: 1439. https://doi.org/10.3390/ijerph14121439