The Synergetic Effect of Cash Transfers for Families, Child Sensitive Social Protection Programs, and Capacity Building for Effective Social Protection on Children’s Nutritional Status in Nepal

 ,
,
Abstract
:1. Background
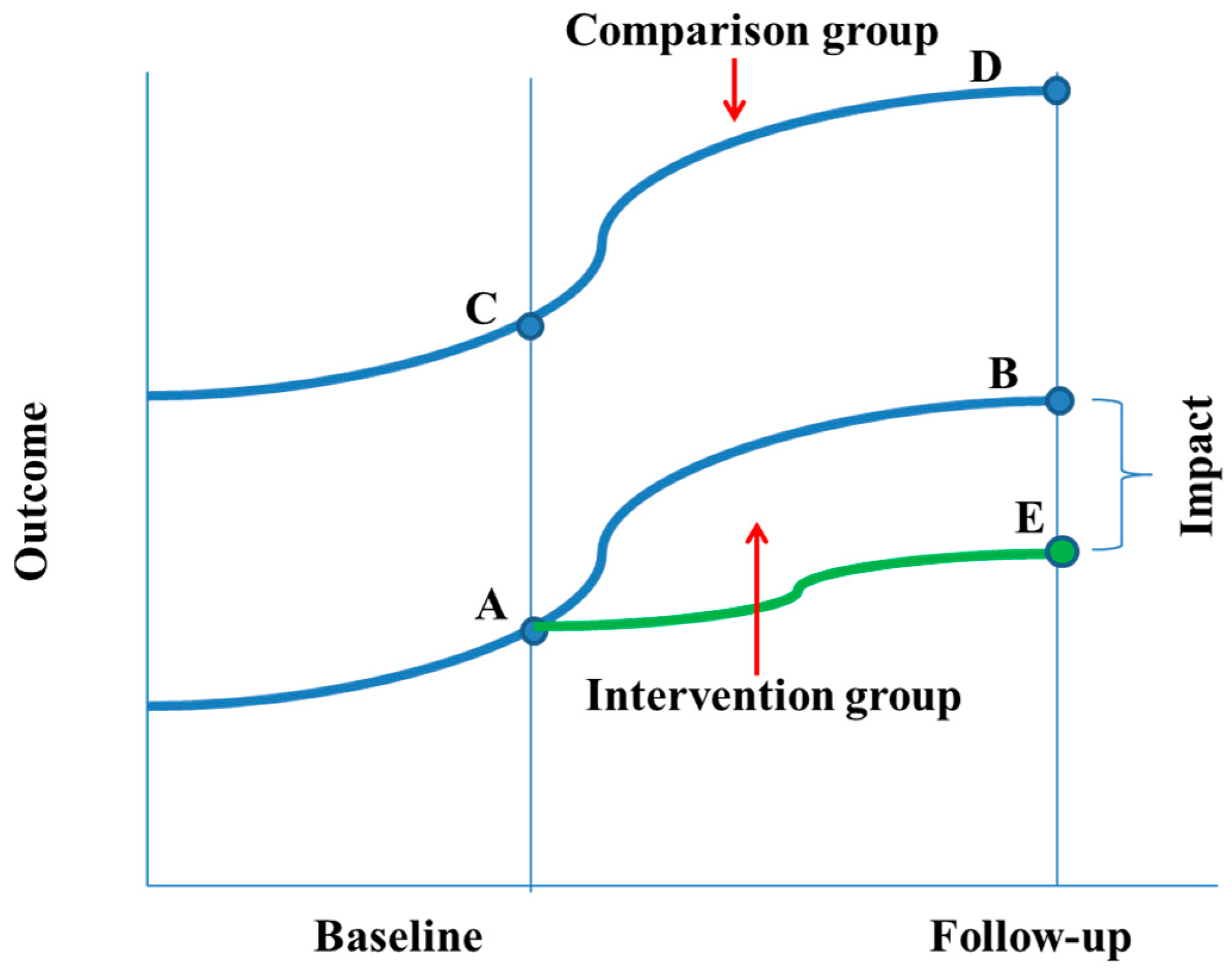
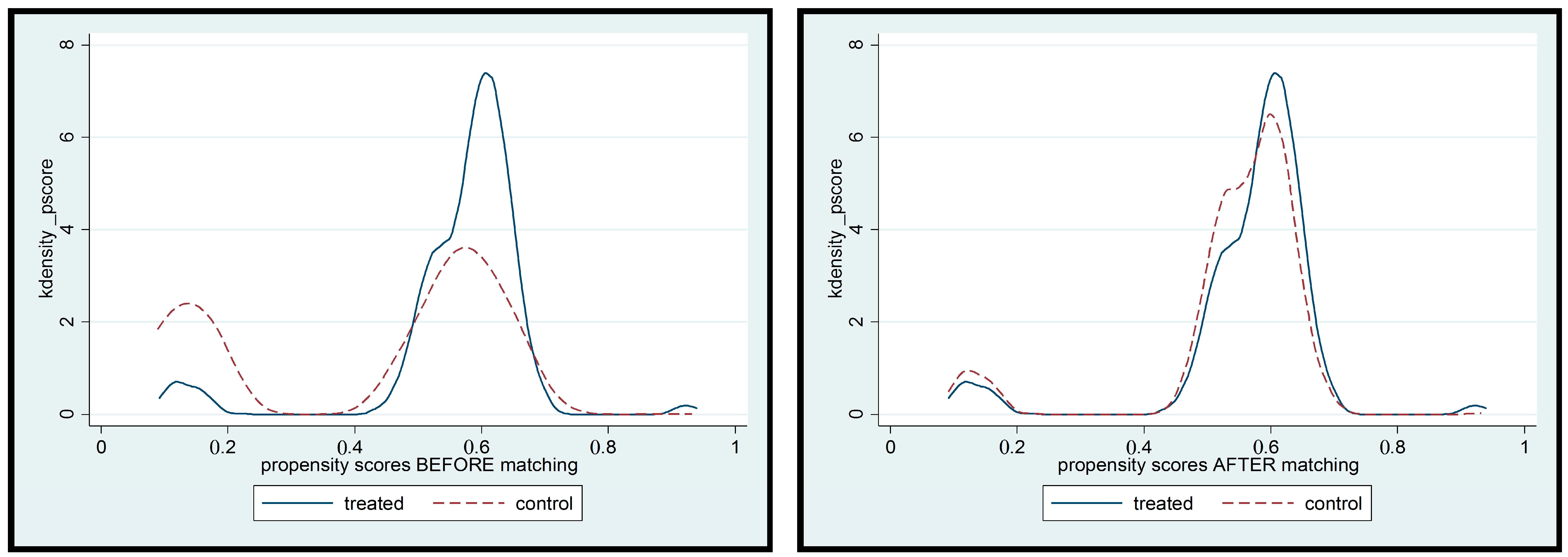
2. Methods
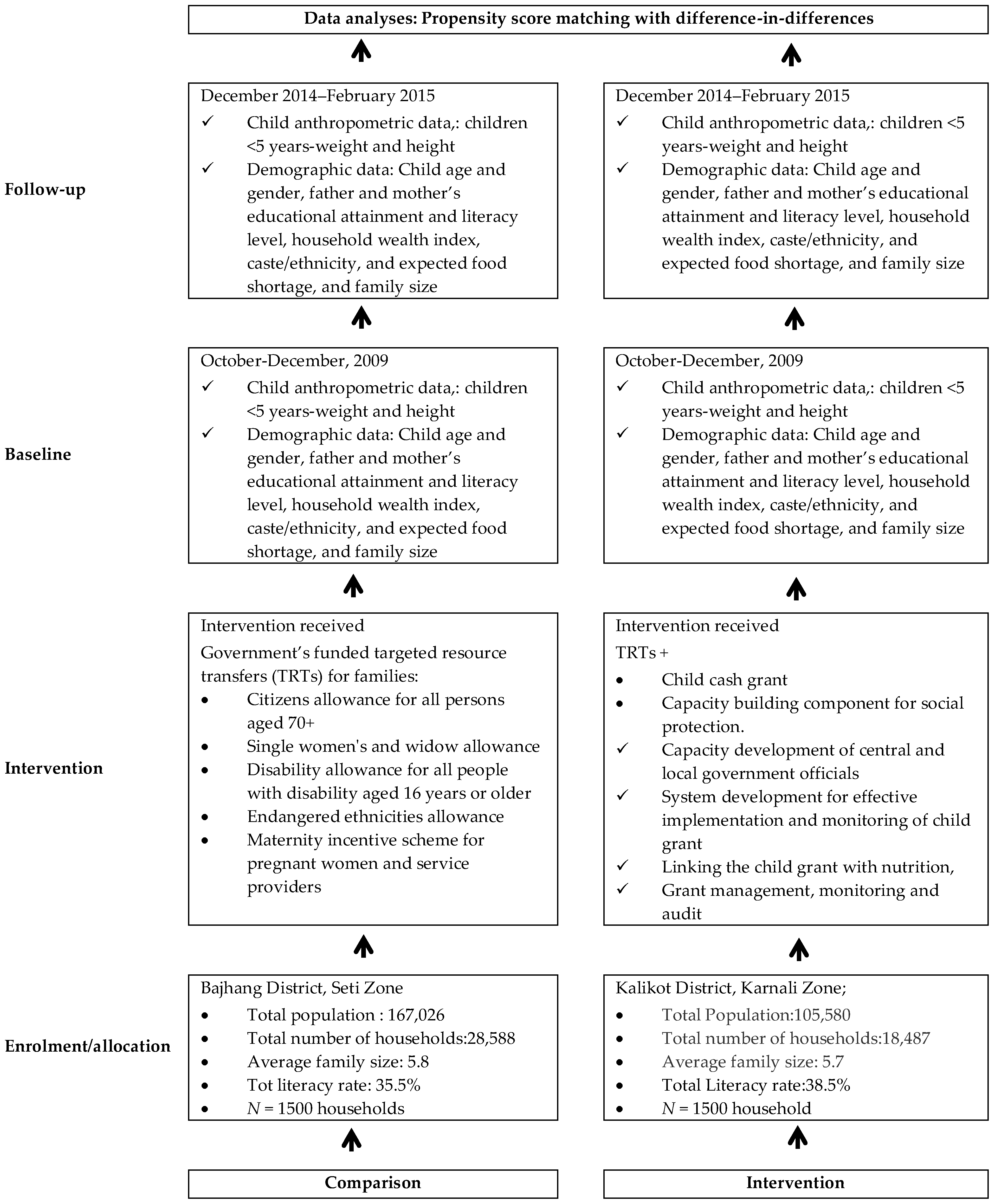
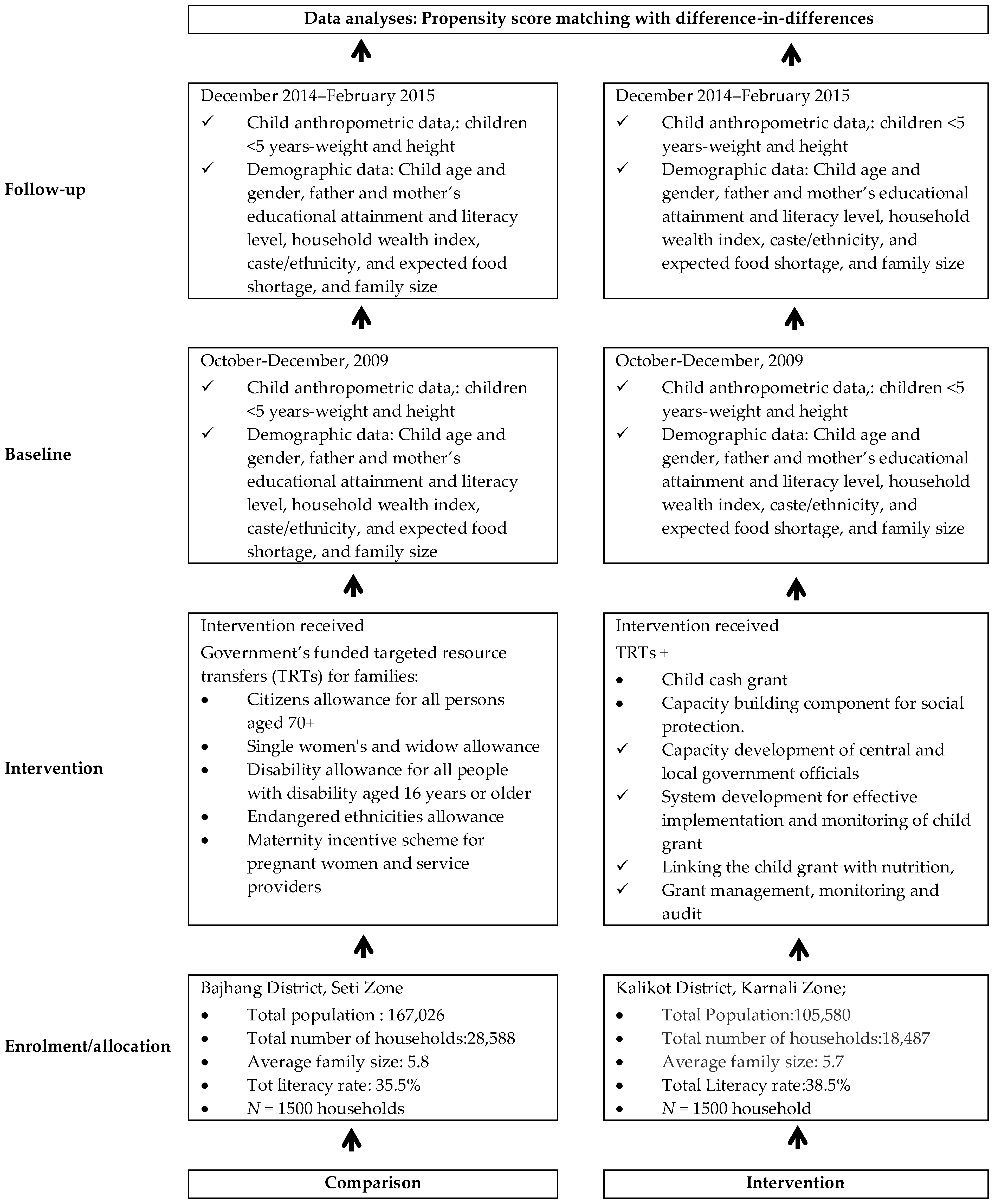
2.1. Evaluation Design and the Intervention
- (1)
- capacity building to enhance the capacity of local bodies in the project districts to deliver the child grant, through orientations for Village Development Committee (VDC) leaders, Traditional Healers and mothers/caretakers, and capacity-building for health workers and Female Community Health Volunteers (FCHVs) and VDC secretaries;
- (2)
- enhancing networking between local bodies, health facilities and communities in the project districts to improve child nutrition;
- (3)
- social behaviour change communication on child nutrition including the provision of nutrition-related counselling services;
- (4)
- awareness raising for timely birth registration to identify all eligible households and about the availability of the CCG;
- (5)
- assisting mothers and others caring for children to identify the best possible locally available food and encouraging them to use the CCG for nutritious foods and the improvement of the nutritional status of children; and
- (6)
- improving the knowledge and skills of CCG beneficiaries in the areas of infant and young child feeding (IYCF) practices, hygiene, sanitation, and other key behaviours linked to child nutrition.
2.2. Sampling Strategy
2.3. Sample Size
2.4. Evaluation Variables
2.5. Statistical Tests
3. Results
Child Malnutrition
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organisation. Children: Reducing Mortality. 2016. Available online: http://www.who.int/mediacentre/factsheets/fs178/en/ (accessed on 8 August 2017).
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; De Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- United Nations. The Millennium Development Goals Report 2015; United Nations: New York, NY, USA, 2015. [Google Scholar]
- United Nations. Resolution Adopted by the General Assembly on 25 September 2015; A/RES/70/1; United Nations: New York, NY, USA, 2015. [Google Scholar]
- World Health Organisation. Sixty-Fith World Health Assembly, Resolutions and Decisions Annexes; WHA65/2012/REC/1; WHO: Geneva, Switzerland, 21–26 May 2012. [Google Scholar]
- World Health Organisation. Global Nutrition Targets 2025: Policy Brief Series (WHO/NMH/NHD/14.2); WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Central Bureau of Statistics. Nepal Multiple Indicator Cluster Survey 2014; Final Report; Central Bureau of Statistics and UNICEF Nepal: Kathmandu, Nepal, 2015. [Google Scholar]
- Nepal MoHo; New ERA; ICF. Nepal Demographic and Health Survey 2016: Key Indicators; Ministry of Health: Kathmandu, Nepal, 2017.
- World Health Organisation. Global Database on Child Growth and Malnutrition. 2017. Available online: http://www.who.int/nutgrowthdb/about/introduction/en/index5.html (accessed on 16 August 2017).
- Prendergast, A.J.; Humphrey, J.H. The stunting syndrome in developing countries. Paediatr. Int. Child Health 2014, 34, 250–265. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Scaling Up Nutrition. SUN Movement Progress Report 2011–2012. Available online: http://scalingupnutrition.org/wp-content/uploads/2012/10/SUN-MP-REPORT_EN.pdf (accessed on 12 February 2016).
- Bhutta, Z.A.; Das, J.K.; Rizvi, A.; Gaffey, M.F.; Walker, N.; Horton, S.; Webb, P.; Lartey, A.; Black, R.E. Group TLNIR: Evidence-based interventions for improvement of maternal and child nutrition: What can be done and at what cost? Lancet 2013, 382, 452–477. [Google Scholar] [CrossRef]
- Coghlan, B.; Toole, M.J.; Chanlivong, N.; Kounnavong, S.; Vongsaiya, K.; Renzaho, A. The impact on child wasting of a capacity building project implemented by community and district health staff in rural Lao PDR. Asia Pac. J. Clin. Nutr. 2014, 23, 105–111. [Google Scholar] [PubMed]
- Devereux, S.; Sabates-Wheeler, R. Transformative Social Protection; IDS Working Paper 232; Institute of Development Studies: Brighton, UK, 2004. [Google Scholar]
- Freeland, N.; Cherrier, C. Social transfers in the fight against hunger: A resource for development practitioners, Reference document No 14. In Proceedings of Brussels EuropeAid Development and Cooperation Directorate-General European Commission; European Union: Brussels, Belgium, 2012. [Google Scholar]
- International Labour Office. Effects of Non-Contributory Social Transfers in Developing Countries: A Compendium; Social Security Department, ILO: Geneva, Switzerland, 2010. [Google Scholar]
- Samson, M.; van Niekerk, I.; Quene, K. Designing and Implementing Social Transfer Programmes; EPRI Press: Cape Town, South Africa, 2006. [Google Scholar]
- Duflo, E. Grandmothers and granddaughters: Old-age pensions and intrahousehold allocation in South Africa. World Bank Econ. Rev. 2003, 17, 1–25. [Google Scholar] [CrossRef]
- Neufeld, L.; García-Guerra, A.; Leroy, J.; Flores-López, M.; Fernández-Gaxiola, A.; Rivera-Dommarco, J. Impacto del Programa Oportunidades en nutrición y alimentación en zonas urbanas de México. In Evaluación Externa de Impacto del Programa Oportunidades; Hernández, M., Hernández, B., Urquieta, S.J., Eds.; Ediciones Instituto Nacional de Salud Pública: Cuernavaca, Mexico, 2006; pp. 47–71. [Google Scholar]
- Ponce, J.; Bedi, A.S. The impact of a cash transfer program on cognitive achievement: The Bono de Desarrollo Humano of Ecuador. Econ. Educ. Rev. 2010, 29, 116–125. [Google Scholar] [CrossRef]
- Hoddinott, J.; Bassett, L. Conditional Cash Transfer Programs and Nutrition in Latin America: Assessment of Impacts and Strategies for Improvement. 2008. Available online: http://dx.doi.org/10.2139/ssrn.1305326 (accessed on 12 May 2017).
- Paes-Sousa, R.; Santos, L.M.P.; Miazaki, É.S. Effects of a conditional cash transfer programme on child nutrition in Brazil. Bull. World Health Organ. 2011, 89, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Attanasio, O.; Gómez, L.C.; Heredia, P.; Vera-Hernandez, M. The Short-Term Impact of a Conditional Cash Subsidy on Child Health and Nutrition in Colombia; Institute for Fiscal Studies: London, UK, 2005. [Google Scholar]
- Rivera, J.A.; Sotres-Alvarez, D.; Habicht, J.-P.; Shamah, T.; Villalpando, S. Impact of the Mexican program for education, health, and nutrition (Progresa) on rates of growth and anemia in infants and young children: A randomized effectiveness study. JAMA 2004, 291, 2563–2570. [Google Scholar] [CrossRef] [PubMed]
- Maluccio, J.; Flores, R. Impact Evaluation of a Conditional Cash Transfer Program: The Nicaraguan Red de Protección Social; International Food Policy Research Institute: Columbia, DC, USA, 2005. [Google Scholar]
- Subbarao, K.; Bonnerjee, A.; Braithwaite, J.; Carvalho, S.; Ezemenari, K.; Graham, C.; Thompson, A. Safety Net Programs and Poverty Reduction. Lessons From Cross-Country Experience; World Bank: Washington, DC, USA, 1997. [Google Scholar]
- Devereux, S.; Solomon, C. Employment Creation Programmes: the International Experience; Issues in Employment and Poverty Discussion Paper No. 24; Economic and Labour Market Analysis Department, International Labour Office: Geneva, Switzerland, 2006. [Google Scholar]
- Haseen, F. Change in Food and Nutrient Consumption among the Ultra Poor: Is the CFPR/TUP Programme Making a Difference? CFPR/TUP Working Paper Series No. 11; BRAC Research and Evaluation Division: Dhaka, Bangladesh, 2006. [Google Scholar]
- Mascie-Taylor, C.; Marks, M.; Goto, R.; Islam, R. Impact of a Short-Term Cash-for-Work Programme on Nutritional Status, Food Expenditure and Consumption of Poor Rural Bangladeshi Women and Children in the Hungry Season; Chars Livelihoods Programme: Dhaka, Bangladesh, 2010. [Google Scholar]
- Fenn, B.; Colbourn, T.; Dolan, C.; Pietzsch, S.; Sangrasi, M.; Shoham, J. Impact evaluation of different cash-based intervention modalities on child and maternal nutritional status in Sindh Province, Pakistan, at 6 mo and at 1 y: A cluster randomised controlled trial. PLoS Med. 2017, 14, e1002305. [Google Scholar] [CrossRef] [PubMed]
- Gertler, P. Do conditional cash transfers improve child health? Evidence from PROGRESA’s control randomized experiment. Am. Econ. Rev. 2004, 94, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Behrman, J.R.; Hoddinott, J. Programme evaluation with unobserved heterogeneity and selective implementation: The Mexican PROGRESA impact on child nutrition. Oxf. Bull. Econ. Stat. 2005, 67, 547–569. [Google Scholar] [CrossRef]
- Bassett, L. Can Conditional Cash Transfer Programs Play a Greater Role in Reducing Child Undernutrition; World Bank: Washington, DC, USA, 2008. [Google Scholar]
- Leroy, J.L.; García-Guerra, A.; García, R.; Dominguez, C.; Rivera, J.; Neufeld, L.M. The Oportunidades program increases the linear growth of children enrolled at young ages in urban Mexico. J. Nutr. 2008, 138, 793–798. [Google Scholar] [PubMed]
- Gray, D.E. Doing Research in the Real World; SAGE: London, UK, 2014. [Google Scholar]
- World Health Organization. WHO Child Growth Standards: Length/Height for Age, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age, Methods and Development; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Rutstein, S.O. Steps to Constructing the New DHS Wealth Index. Available online: https://dhsprogram.com/programming/wealth%20index/Steps_to_constructing_the_new_DHS_Wealth_Index.pdf (accessed on 22 June 2017).
- Mayne, S.L.; Lee, B.K.; Auchincloss, A.H. Evaluating propensity score methods in a quasi-experimental study of the impact of menu-labeling. PLoS ONE 2015, 10, e0144962. [Google Scholar] [CrossRef] [PubMed]
- Baser, O. Too much ado about propensity score models? Comparing methods of propensity score matching. Value Health 2006, 9, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Caliendo, M.; Kopeinig, S. Some practical guidance for the implementation of propensity score matching. J. Econ. Surv. 2008, 22, 31–72. [Google Scholar] [CrossRef]
- Harder, V.S.; Stuart, E.A.; Anthony, J.C. Propensity score techniques and the assessment of measured covariate balance to test causal associations in psychological research. Psychol. Methods 2010, 15, 234–249. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. A critical appraisal of propensity-score matching in the medical literature between 1996 and 2003. Stat. Med. 2008, 27, 2037–2049. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, P.R.; Rubin, D.B. The central role of the propensity score in observational studies for causal effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef]
- Austin, P.C.; Small, D.S. The use of bootstrapping when using propensity-score matching without replacement: A simulation study. Stat. Med. 2014, 33, 4306–4319. [Google Scholar] [CrossRef] [PubMed]
- Pirracchio, R.; Resche-Rigon, M.; Chevret, S. Evaluation of the propensity score methods for estimating marginal odds ratios in case of small sample size. BMC Med. Res. Methodol. 2012, 12, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Groot, R.; Palermo, T.; Handa, S.; Ragno, L.P.; Peterman, A. Cash transfers and child nutrition: Pathways and impacts. Dev. Policy Rev. 2017, 35, 621–643. [Google Scholar] [CrossRef]
- Manley, J.; Gitter, S.; Slavchevska, V. How Effective Are Cash Transfer Programmes at Improving Nutritional Status? A Rapid Evidence Assessment of Programmes’ Effects on Anthropometric Outcomes; EPPI-Centre, Social Science Research Unit, Institute of Education, University of London: London, UK, 2012. [Google Scholar]
- Dehejia, R.H.; Wahba, S. Propensity score-matching methods for nonexperimental causal studies. Rev. Econ. Stat. 2002, 84, 151–161. [Google Scholar] [CrossRef]
- Lagarde, M.; Haines, A.; Palmer, N. The impact of conditional cash transfers on health outcomes and use of health services in low and middle income countries. Cochrane Database Syst. Rev. 2009. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Program Activities | Program Activities in the Intervention Area (5 Districts of the Karnali Zone) | Program Activities in the Control Area (Bajhang Distrcict) | No. of Activities per Year | Frequency of Delivery | Mode of Delivery |
|---|---|---|---|---|---|
| Advocacy and Capacity Building | |||||
| Program planning and review workshop | Yes | No | Planning undertaken Once every year, review workshop done for twice (during 2013 and 2015) | 3 times in each districts during the project period—Review twice (during mid-implementation and final review) | Planning Meeting Workshop |
| Training in Infant and Young Child Feeding (IYCF) to all health workers at district level | Yes | No | In 2011 (Starting year) and Refresher in 2015 | One IYCF ToT (Training of Trainer) and Cascading initially, review were taken annually and refresher training in 2015 | ToT jointly by Program Cooperation Agreement (PCA) partner as well as Ministry of Health (MoH), Refresher undertaken by MoH mechanisms |
| Training to all health workers at health facility (VDC) level | Yes | No | In 2011 (Starting year) and Refresher in 2015 | One IYCF TOT and Cascading initially, review were taken annually and refresher training in 2015 | ToT jointly by PCA partner as well as MoH, Refresher undertaken by MoH mechanisms |
| Training to Female Community Heath Volunteers (FCHV), Traditional Healers, teachers and community leaders | Yes | No | In 2011 (Starting year) and Refresher in 2015 | twice | training/orientation Implementation through FCHV (Government/MoH) mechanisms, facilitated by Non Government Organization (NGO) partners |
| Facilitate Mothers Group Meeting on Nutrition at community level (at least one in each ward) | Yes | No | Mothers Group meeting happens every month in each settlement through Female Community Heath Volunteers | 12 times/ year/FCHV in all districts | Through MoH mechanisms |
| Orientation to social mobilizers and community facilitators in all five districts of Karnali. | Yes | No | One a year (in 2012 and 2015) | twice | orientation through NGO partner |
| Conduct 1 day VDC level refresher training/program orientation to FCHV in each VDC in Karnali zone (Ensure IYCF-Cash Grant refresher conducted by Heath post/District Public Health Offices) | Yes | No | One training and One Refresher in 5 years | twice | Through MoH mechanisms |
| Awareness raising | |||||
| Orientation/meeting to mother/caregivers in all 5 districts (134 VDCs) of Karnali and demonstration of preparation of complementary food lito (mixtures of roasted and grinded cereals, legumes) and jaulo (cooked rice and lentils with vegetables and ghee) for children | Yes | No | twice in 5 years | 2 | Implementation through FCHVs (Government/MoH) mechanisms, facilitated by PCA partners (NGO) |
| Dissemination of Behaviour Change Communication message during orientations at 5 districts (134 VDCs) of Karnali | Yes | No | 1 | 5 | Implementation through Government/MoH (Health facilities, Health workers, FCHVs, etc.) mechanisms, facilitated by PCA partners (NGO) |
| Production of radio program on nutrition and social protection promotion. | Yes | No | 1 | 5 | Through Local Frequency Modulation (FM) Radio stations facilitated by NGO partners |
| Broadcasting the Nutrition and Social Protection related Radio Programmes through FM Radios | Yes | No | 1 | 5 | Through Local FM stations facilitated by NGO partners |
| Conduct local food preparation and demo at mother group/school and Early Childhood Development (ECD) | Yes | No | 1 | 5 (Once every year) | Through Government/MoH (Health workers, FCHVs, etc.) mechanisms at community level |
| Partnership with community Radios for producing and broadcasting the weekly magazine on child feeding, caring, nutrition, hygiene and sanitation. | Yes | No | 1 | 365 days | Through Local FM stations facilitated by NGO partners |
| Daily Airing of Jingle Message from FM radios. | Yes | No | 1 | 365 days | Through Local FM stations facilitated by NGO partners |
| Promote nutritious food (eggs, Jaulo) for underweight children and iodized salt to all children 0–23 coming to Growth Monitoring and pregnant women coming to Ante-Natal Checkups | Yes | No | 1 time in five year | 1 | Implementation through Government/MoH (Health facilities, Health workers, FCHVs, etc.) mechanisms, facilitated by NGO partners |
| Mobilization of other community structures like women’s group | |||||
| Conduct wards level discussion/meeting through community structure | Yes | No | 1 | 5 | Through Government/MoH mechanisms, facilitated by NGO partners |
| Conduct joint monitoring and Evaluation at VDC level from District Resource Group and NGO Partner | Yes | No | 1 | 2 | Through Government/MoH mechanisms, facilitated by NGO partners |
| Community Facilitator for mobilization of community groups/institutions (2 persons in each district for 5 months) | Yes | No | 1 | 3 times (2011, 2012, 2015) | Through Government/MoH mechanisms, facilitated by NGO partners |
| Community Level Dramas at cluster level in all 5 district of Karnali | Yes | No | 1 | 2 times in each clusters | Through Government/MoH mechanisms, facilitated by NGO partners |
| Distribution of Child Grant to all under 5 children (in every four months) by the Government of Nepal | Yes | Yes (only to Dalit Children—10% of total under five children) | 3 times per year | 3 times per year in all 5 districts every year | Through Local government (VDCs) |
| Birth Registration Campaign | |||||
| Conduct VDC level birth registration campaign promoting birth registration within 35 days in all 134 VDCs of Karnali | Yes | No | 1 | 2 (in 2012 and 2015) in all 5 districts | Through Local Government at district and village levels (District Development Committee (and Village Development Committees), facilitated by NGO partners |
| Provide incentive for those families who do birth registration within 35 days of child birth | Yes | No | 1 | 1 times in all 5 districts | Through Local Government at district and village levels, facilitated by NGO partners |
| Community Facilitator for mobilization of community groups/institutions(2 persons in each district for 5 months) | Yes | No | 1 | 3 times (2011, 2012, 2015) | Through Government/MoH mechanisms, facilitated by NGO partners |
| System Strengthening to Management Information System (MIS) of Social Protection Schemes (Child Grant, Old age Pension, Single Women Allowances, etc.) | |||||
| Provide technical support to DDC and KIRDARC for Information Technology support and MIS rollout in all five districts of Karnali through consultants. | Yes | No | 1 | 1 times in each districts | |
| Community Facilitator for mobilization of community groups/institutions(2 persons in each district for 5 months) | Yes | No | 1 | 3 times (2011, 2012, 2015) | Through Government/MoH mechanisms, facilitated by NGO partners |
| Supervision and Monitoring including process Monitoring | Yes | No | Ongoing | ongoing | Through Government/MoH mechanisms |
| Matching Variables | All | Intervention | Control | Logit Model | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | Baseline | Follow-Up | |||||||||||||||
| N | Mean | SD | N | Mean | SD | N | Mean | SD | N | Mean | SD | N | Mean | SD | Coefficient | SE | p-Value | |
| People per household | 3000 | 750 | 750 | 750 | 750 | |||||||||||||
| 4 people or less | 15.3% | 36.0% | 13.5% | 34.2% | 21.2% | 40.9% | 15.3% | 36.1% | 15.3% | 36.1% | 0.40 | 0.14 | 0.004 | |||||
| 5–8 people | 63.8% | 48.1% | 64.8% | 47.8% | 65.2% | 47.7% | 60.5% | 48.9% | 60.5% | 48.9% | 0.16 | 0.10 | 0.111 | |||||
| 9 people or above | 20.8% | 40.6% | 21.7% | 41.3% | 13.6% | 34.3% | 24.1% | 42.8% | 24.1% | 42.8% | Ref | |||||||
| Household wealth index | 2899 | 724 | 710 | 731 | 731 | |||||||||||||
| Poor | 60.0% | 49.0% | 89.1% | 31.2% | 54.2% | 49.9% | 10.1% | 30.2% | 10.1% | 30.2% | 2.17 | 0.13 | 0.000 | |||||
| Middle class | 20.0% | 40.0% | 9.7% | 29.6% | 35.9% | 48.0% | 23.9% | 42.7% | 23.9% | 42.7% | 2.08 | 0.15 | 0.000 | |||||
| Rich | 20.0% | 40.0% | 1.2% | 11.1% | 9.9% | 29.8% | 65.9% | 47.4% | 65.9% | 47.4% | Reference | |||||||
| Child’s age in months | 3000 | 27.98 | 15.53 | 750 | 28.66 | 15.36 | 750 | 28.4 | 15.71 | 750 | 28.08 | 15.4 | 750 | 28.08 | 15.4 | 0.01 | 0.00 | 0.045 |
| Child’s gender | 3000 | 750 | 750 | 750 | 750 | |||||||||||||
| Girl | 43.4% | 49.6% | 44.8% | 49.8% | 43.6% | 49.6% | 43.7% | 49.6% | 43.7% | 49.6% | Reference | |||||||
| Boy | 56.6% | 49.6% | 55.2% | 49.8% | 56.4% | 49.6% | 56.3% | 49.6% | 56.3% | 49.6% | −0.08 | 0.08 | 0.322 | |||||
| Ethnicity | 3000 | 750 | 750 | 750 | 750 | |||||||||||||
| Disadvantage ethnic groups | 0.4% | 6.6% | 1.5% | 12.0% | 0.1% | 3.7% | 0.0% | 0.0% | 0.0% | 0.0% | 2.04 | 1.04 | 0.050 | |||||
| Dalit Hill/Terai | 21.1% | 40.8% | 21.3% | 41.0% | 25.5% | 43.6% | 16.8% | 37.4% | 16.8% | 37.4% | 0.01 | 0.10 | 0.911 | |||||
| Upper caste Group | 78.5% | 41.1% | 77.2% | 42.0% | 74.4% | 43.7% | 83.2% | 37.4% | 83.2% | 37.4% | Reference | |||||||
| Father’s education | 3000 | 750 | 750 | 750 | 750 | |||||||||||||
| Intermediate or higher | 12.6% | 33.2% | 2.1% | 14.5% | 16.8% | 37.4% | 5.6% | 23.1% | 25.9% | 43.8% | Reference | |||||||
| Secondary level | 30.0% | 45.8% | 33.1% | 47.1% | 22.3% | 41.6% | 38.3% | 48.6% | 26.4% | 44.1% | −0.05 | 0.14 | 0.744 | |||||
| Primary or less | 57.4% | 49.5% | 64.8% | 47.8% | 60.9% | 48.8% | 56.1% | 49.7% | 47.7% | 50.0% | 0.27 | 0.14 | 0.052 | |||||
| Intervention | Comparison | %Bias | |||
|---|---|---|---|---|---|
| Unmatched | Matched | Unmatched | Matched | ||
| No. of people per household | |||||
| 4 people or less | 0.159 | 0.082 | 0.128 | 0.118 | −10.30 |
| 5–8 people | 0.657 | 0.664 | 0.629 | 0.659 | 1.20 |
| 9 people or more | 0.184 | 0.254 | 0.243 | 0.223 | 7.40 |
| Household wealth index | |||||
| Poor | 0.717 | 0.648 | 0.484 | 0.683 | −7.40 |
| Middle class | 0.227 | 0.275 | 0.174 | 0.240 | 8.80 |
| Rich | 0.056 | 0.077 | 0.342 | 0.077 | 0.00 |
| Child’s age in months | 28.341 | 25.429 | 27.476 | 27.602 | −14.00 |
| Child’s gender | |||||
| Girl | 0.438 | 0.395 | 0.429 | 0.421 | 5.30 |
| Boy | 0.562 | 0.605 | 0.571 | 0.579 | −5.30 |
| Ethnicity | |||||
| Disadvantage ethnic groups | 0.008 | 0.001 | 0.001 | 0.001 | 0.00 |
| Dalit Hill/ Terai | 0.224 | 0.208 | 0.179 | 0.212 | −1.00 |
| Upper caste Group | 0.768 | 0.791 | 0.820 | 0.787 | 1.00 |
| Father’s education | |||||
| Primary or less | 0.630 | 0.496 | 0.519 | 0.540 | −8.90 |
| Secondary level | 0.277 | 0.378 | 0.323 | 0.338 | 8.70 |
| Intermediate or higher | 0.093 | 0.127 | 0.158 | 0.122 | −1.20 |
| Original Dataset | Matched Dataset: Matching Algorithms | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Comparison | Intervention | Comparison | Intervention | Kernel ! | Nearest Neighbour ! | Radius !# | ||||||||||
| N = 748 | N = 743 | N = 749 | N = 750 | ADID | 95% CI | ADID | 95% CI | ADID | 95% CI | ADID | 95% CI | |||||
| Girls a | ||||||||||||||||
| Height | 77.2 (10.3) | 77.8 (10.9) | 78.7 (11.1) | 78.8 (11.7) | 0.17 | −0.05 | 0.40 | 0.65 | −0.87 | 2.18 | 0.01 | −1.43 | 1.45 | 0.69 | −0.99 | 2.36 |
| Weight | 9.3 (2.4) | 9.3 (2.5) | 9.7 (2.6) | 9.8 (2.9) | 0.31 *** | 0.22 | 0.40 | 0.32 | −0.06 | 0.71 | 0.13 | −0.25 | 0.51 | 0.33 * | 0.06 | 0.6 |
| HAZ | −2.3 (1.3) | −2.6 (1.4) | −2.1 (1.3) | −2.2 (1.3) | 0.21 | −0.01 | 0.44 | 0.11 | −0.06 | 0.27 | 0.07 | −0.18 | 0.32 | 0.15 | −0.06 | 0.36 |
| WAZ | −1.7 (1.0) | −2.1 (1.1) | −1.5 (1.1) | −1.6 (1.1) | 0.33 *** | 0.23 | 0.44 | 0.17 * | 0.06 | 0.28 | 0.13 | −0.1 | 0.37 | 0.19 * | 0.09 | 0.29 |
| WHZ | −0.5 (0.9) | −0.8 (1.1) | −0.5 (1.0) | −0.4 (1.0) | 0.31 *** | 0.15 | 0.46 | 0.17 * | 0.05 | 0.3 | 0.13 | −0.06 | 0.33 | 0.18 | −0.01 | 0.36 |
| Stunting | 61.9 | 68 | 55.5 | 61 | −3.98 | −15.44 | 7.48 | −2.65 | −9.15 | 3.85 | −5.07 | −11.78 | 1.63 | −4.24 | −10.4 | 1.93 |
| Underweight | 37.1 | 53.1 | 30.8 | 34.9 | −16.25 *** | −24.12 | −8.38 | −7.83 *** | −14.39 | −1.26 | −8.89 | −18.96 | 1.17 | −9.02 *** | −15.1 | −2.94 |
| Wasting | 4.5 | 9.3 | 7 | 4.9 | −9.29 *** | −15.86 | −2.72 | −2.62 | −6.33 | 1.09 | −3.31 | −8.2 | 1.58 | −2.47 | −5.9 | 0.95 |
| Boys a | ||||||||||||||||
| Height | 80.2 (11.2) | 80.6 (11.2) | 82.4 (11.2) | 81.6 (11.8) | −0.05 | −1.17 | 1.06 | 0.21 | −1.31 | 1.74 | 0.13 | −1.13 | 1.39 | 0.22 | −0.9 | 1.35 |
| Weight | 10.2 (2.6) | 10.2 (2.7) | 10.9 (2.8) | 10.7 (3.0) | 0.17 | −0.17 | 0.52 | 0.23 | −0.11 | 0.57 | 0.21 | −0.23 | 0.66 | 0.25 | −0.09 | 0.6 |
| HAZ | −2.4 (1.3) | −2.6 (1.5) | −2.0 (1.3) | −2.2 (1.4) | 0.14 | −0.14 | 0.43 | 0.16 * | 0 | 0.31 | 0.08 | −0.17 | 0.33 | 0.22 * | 0.08 | 0.35 |
| WAZ | −1.7 (1.0) | −2.1 (1.1) | −1.4 (1.1) | −1.6 (1.1) | 0.26 | 0.01 | 0.51 | 0.19 ** | 0.1 | 0.29 | 0.17 * | 0.01 | 0.32 | 0.25 * | 0.08 | 0.42 |
| WHZ | −0.6 (0.9) | −0.9 (1.2) | −0.3 (1.1) | −0.4 (1.0) | 0.27 *** | 0.08 | 0.47 | 0.21 * | 0.06 | 0.36 | 0.20 * | 0.02 | 0.38 | 0.21 * | 0.07 | 0.36 |
| Stunting | 63.7 | 65.7 | 50.8 | 58.8 | 0.69 | −14.00 | 15.37 | −4.14 | −10.48 | 2.19 | −1.27 | −10.49 | 7.95 | −6.15 * | −11.76 | −0.53 |
| Underweight | 37.4 | 48.8 | 27.5 | 34.8 | −9.74 | −23.38 | 3.90 | −5.03 | −11.19 | 1.13 | −3.39 | −13.45 | 6.67 | −6.49 | −13.15 | 0.16 |
| Wasting | 6.6 | 15.3 *** | 5.9 | 6.4 | −9.55 *** | −14.46 | −4.64 | −3.11 | −6.4 | 0.19 | −3.54 | −8.31 | 1.23 | −3.33 * | −6.16 | −0.49 |
| <2 years b | ||||||||||||||||
| Height | 70.0 (6.5) | 69.6 (6.7) | 70.8 (7.4) | 69.2 (7.4) | −0.28 | −1.16 | 0.60 | −0.85 * | −1.67 | −0.02 | −0.91 | −2.45 | 0.63 | −0.81 * | −1.6 | −0.02 |
| Weight | 7.8 (1.5) | 7.5 (1.6) | 8.1 (1.8) | 7.6 (1.8) | 0.03 | −0.30 | 0.37 | −0.15 | −0.38 | 0.08 | −0.17 | −0.45 | 0.11 | −0.14 | −0.36 | 0.08 |
| HAZ | −2.0 (1.4) | −2.2 (1.5) | −1.6 (1.4) | −1.9 (1.5) | 0.03 | −0.21 | 0.28 | 0.12 | −0.09 | 0.33 | −0.1 | −0.37 | 0.18 | 0.13 | −0.08 | 0.33 |
| WAZ | −1.5 (1.1) | −2.0 (1.2) | −1.2 (1.2) | −1.6 (1.2) | 0.18 | −0.04 | 0.41 | 0.08 | −0.06 | 0.22 | −0.01 | −0.24 | 0.23 | 0.09 | −0.08 | 0.27 |
| WHZ | −0.6 (0.9) | −1.1 (1.3) | −0.5 (1.1) | −0.7 (1.1) | 0.18 | −0.04 | 0.41 | 0.05 | −0.09 | 0.2 | 0.1 | −0.15 | 0.34 | 0.07 | −0.08 | 0.21 |
| Stunting | 52 | 58.2 | 39.8 | 50.8 | 2.76 | −5.16 | 10.68 | −2.48 | −8.1 | 3.14 | 1.61 | −6.44 | 9.66 | −3.57 | −10.37 | 3.23 |
| Underweight | 32.6 | 47.1 | 23.8 | 37.1 | −5.39 | −18.43 | 7.66 | −0.46 | −7.8 | 6.89 | 1.86 | −8.42 | 12.15 | −1.24 | −8.08 | 5.6 |
| Wasting | 6.7 | 18.8 | 6.8 | 10.3 | −9.19 *** | −15.81 | −2.57 | −1.2 | −5.16 | 2.76 | −1.91 | −6.88 | 3.05 | −1.03 | −4.2 | 2.13 |
| ≥2 years b | ||||||||||||||||
| Height | 87.1 (7.1) | 86.4 (7.9) | 88.3 (7.1) | 87.9 (7.6) | 0.53 | −0.12 | 1.18 | 0.41 | −0.18 | 1.01 | 0.59 | −0.45 | 1.63 | 0.74 | −0.16 | 1.64 |
| Weight | 11.7 (1.9) | 11.4 (2.0) | 12.1 (2.0) | 12.1 (2.1) | 0.39 *** | 0.12 | 0.66 | 0.36 *** | 0.12 | 0.6 | 0.44 ** | 0.18 | 0.69 | 0.44 *** | 0.25 | 0.63 |
| HAZ | −2.6 (1.1) | −2.8 (1.2) | −2.4 (1.1) | −2.4 (1.3) | 0.15 | −0.02 | 0.31 | 0.17 * | 0.06 | 0.28 | 0.12 | −0.03 | 0.28 | 0.21 * | 0.06 | 0.35 |
| WAZ | −1.9 (1.0) | −2.1 (1.1) | −1.6 (1.0) | −1.6 (1.0) | 0.28 *** | 0.12 | 0.44 | 0.28 *** | 0.18 | 0.37 | 0.27 ** | 0.13 | 0.41 | 0.30 *** | 0.19 | 0.41 |
| WHZ | −0.5 (0.9) | −0.6 (1.0) | −0.3 (1.0) | −0.2 (0.9) | 0.29 *** | 0.11 | 0.47 | 0.26 *** | 0.17 | 0.35 | 0.29 ** | 0.12 | 0.46 | 0.27 *** | 0.14 | 0.4 |
| Stunting | 73 | 73.1 | 62.8 | 65.8 | 0.05 | −6.01 | 6.11 | −4.82 | −10.23 | 0.6 | −4.05 | −12.54 | 4.44 | −6.66 ** | −12.13 | −1.18 |
| Underweight | 41.5 | 53.3 | 32.8 | 33.3 | −14.87 *** | −23.27 | −6.46 | −10.45 *** | −16.02 | −4.88 | −9.2 | −18.52 | 0.11 | −11.40 *** | −16.66 | −6.13 |
| Wasting | 4.9 | 8.2 | 6.1 | 2.7 | −8.51 *** | −13.91 | −3.11 | −3.86 ** | −5.98 | −1.74 | −6.22 ** | −9.22 | −3.22 | −4.10 ** | −6.43 | −1.78 |
| All c | ||||||||||||||||
| Height | 78.9 (10.9) | 79.3 (11.1) | 80.8 (11.3) | 80.3 (11.9) | 0.11 | −0.51 | 0.72 | 0.42 | −0.68 | 1.52 | −0.11 | −1.08 | 0.86 | 0.48 | −0.33 | 1.28 |
| Weight | 9.8 (2.6) | 9.8 (2.7) | 10.4 (2.8) | 10.3 (3.0) | 0.26 ** | 0.05 | 0.47 | 0.27 * | 0 | 0.55 | 0.17 | −0.12 | 0.47 | 0.29 | −0.01 | 0.6 |
| HAZ | −2.3 (1.3) | −2.6 (1.4) | −2.1 (1.3) | −2.2 (1.4) | 0.17 * | 0.03 | 0.31 | 0.14 * | 0.03 | 0.25 | 0.05 | −0.12 | 0.23 | 0.18 * | 0.09 | 0.27 |
| WAZ | −1.7 (1.0) | −2.1 (1.1) | −1.4 (1.1) | −1.6 (1.1) | 0.29 *** | 0.15 | 0.44 | 0.19 ** | 0.11 | 0.28 | 0.18 * | 0.07 | 0.29 | 0.22 ** | 0.15 | 0.29 |
| WHZ | −0.5 (0.9) | −0.8 (1.1) | −0.4 (1.1) | −0.4 (1.0) | 0.29 *** | 0.15 | 0.42 | 0.18 * | 0.09 | 0.28 | 0.24 * | 0.08 | 0.4 | 0.19 * | 0.09 | 0.3 |
| Stunting | 63 | 66.7 | 52.9 | 59.8 | −1.34 | −7.12 | 4.44 | −3.51 | −7.83 | 0.82 | −2.18 | −10.22 | 5.87 | −5.16 * | −9.55 | −0.77 |
| Underweight | 37.3 | 50.7 | 28.9 | 34.8 | −12.54 *** | −19.82 | −5.25 | −6.29 *** | −10.96 | −1.62 | −5.19 | −10.75 | 0.37 | −7.35 *** | −11.62 | −3.08 |
| Wasting | 5.8 | 12.7 | 6.4 | 5.7 | −9.32 *** | −14.86 | −3.79 | −2.86 * | −4.91 | −0.8 | −4.84 *** | −8.62 | −1.06 | −2.84 ** | −5.58 | −0.1 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Renzaho, A.M.N.; Chitekwe, S.; Chen, W.; Rijal, S.; Dhakal, T.; Dahal, P. The Synergetic Effect of Cash Transfers for Families, Child Sensitive Social Protection Programs, and Capacity Building for Effective Social Protection on Children’s Nutritional Status in Nepal. Int. J. Environ. Res. Public Health 2017, 14, 1502. https://doi.org/10.3390/ijerph14121502
Renzaho AMN, Chitekwe S, Chen W, Rijal S, Dhakal T, Dahal P. The Synergetic Effect of Cash Transfers for Families, Child Sensitive Social Protection Programs, and Capacity Building for Effective Social Protection on Children’s Nutritional Status in Nepal. International Journal of Environmental Research and Public Health. 2017; 14(12):1502. https://doi.org/10.3390/ijerph14121502
Chicago/Turabian StyleRenzaho, Andre M. N., Stanley Chitekwe, Wen Chen, Sanjay Rijal, Thakur Dhakal, and Pradiumna Dahal. 2017. "The Synergetic Effect of Cash Transfers for Families, Child Sensitive Social Protection Programs, and Capacity Building for Effective Social Protection on Children’s Nutritional Status in Nepal" International Journal of Environmental Research and Public Health 14, no. 12: 1502. https://doi.org/10.3390/ijerph14121502