Does the Short-Term Effect of Air Pollution Influence the Incidence of Spontaneous Intracerebral Hemorrhage in Different Patient Groups? Big Data Analysis in Taiwan

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
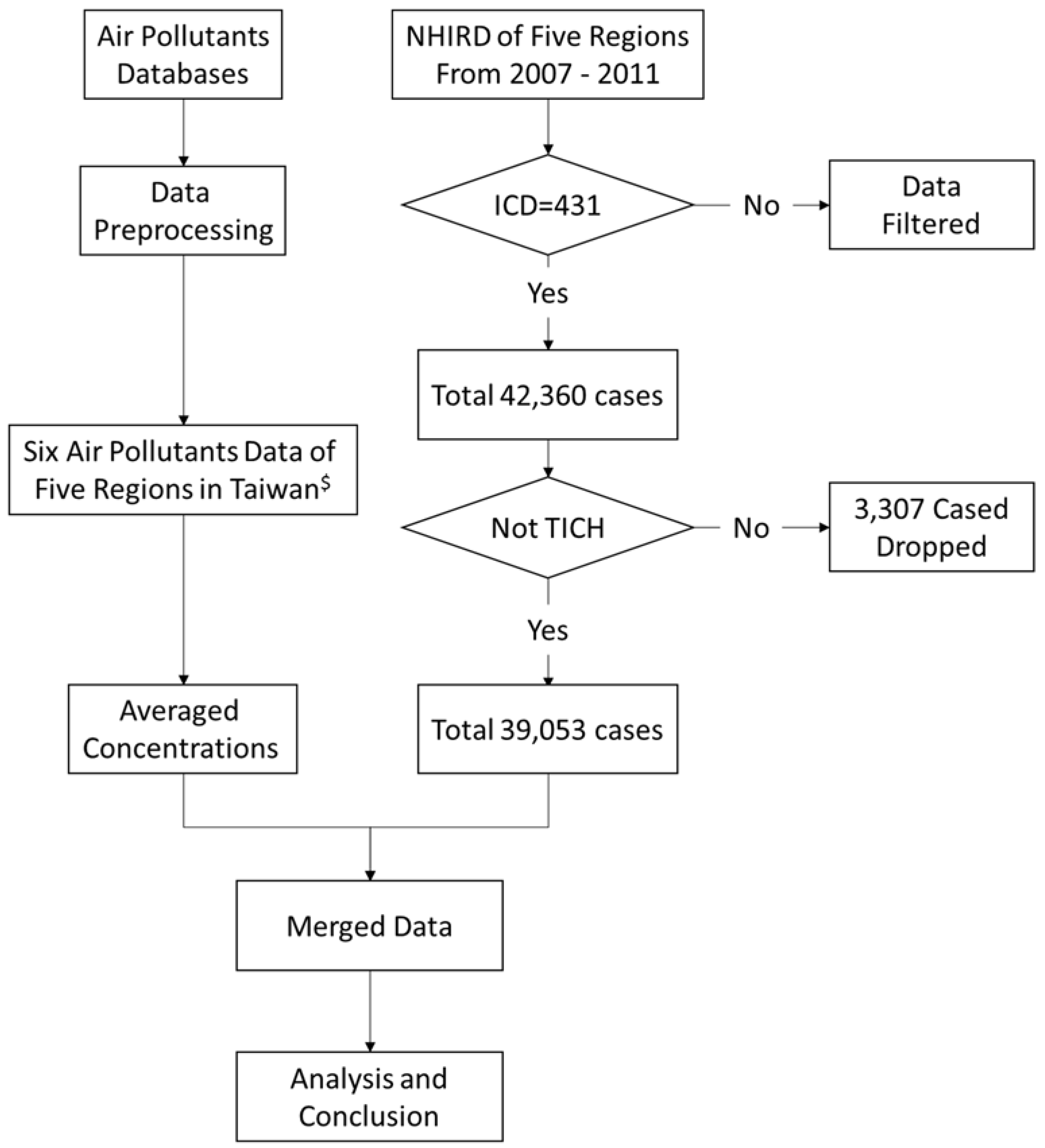
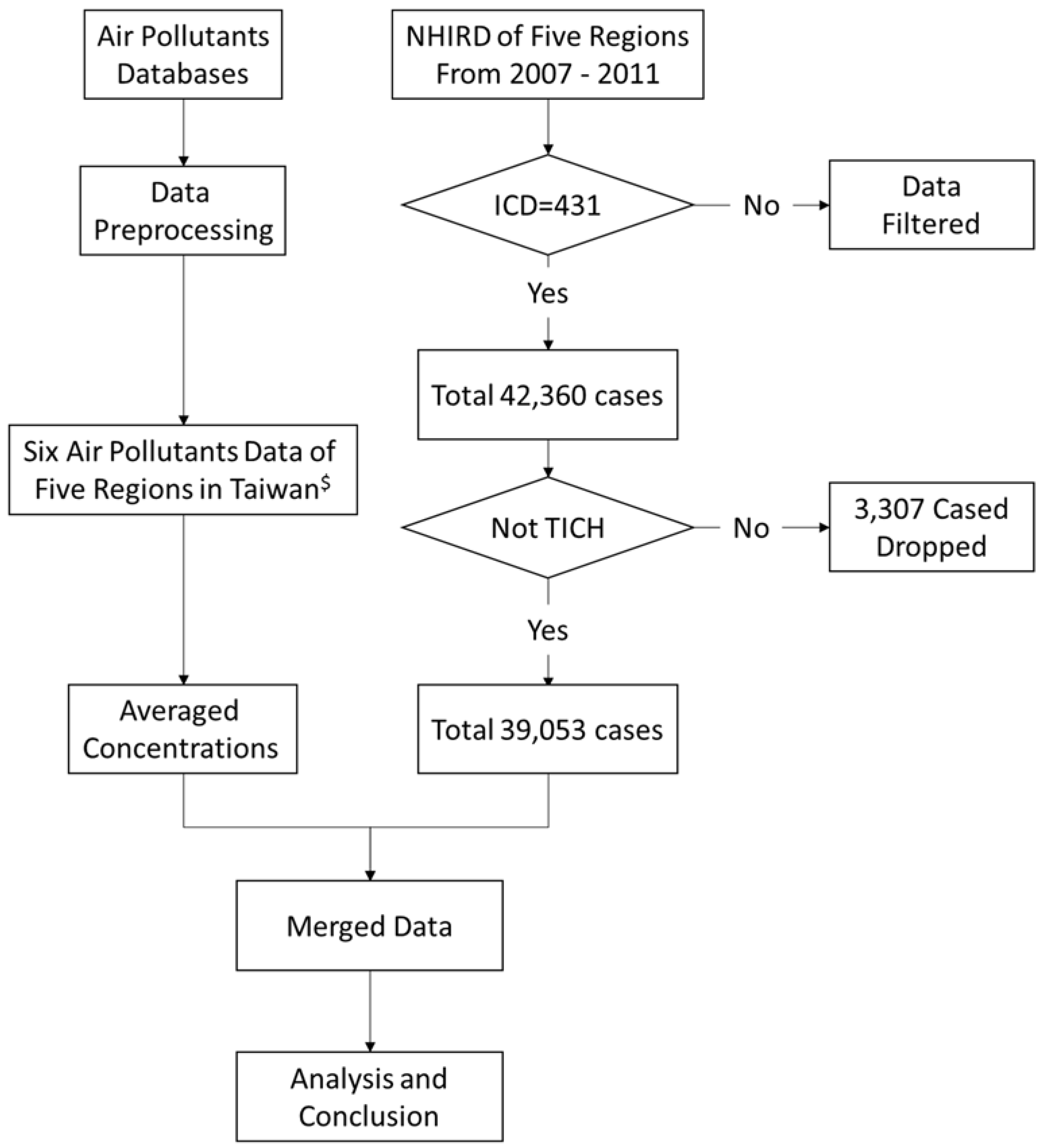
2.1. Data Sources
2.2. Data Protection and Permission
2.3. Data Management
2.4. Statistics
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ohwaki, K.; Yano, E.; Murakami, H.; Nagashima, H.; Nakagomi, T. Meteorological factors and the onset of hypertensive intracerebral hemorrhage. Int. J. Biometeorol. 2004, 49, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Goodson, J.M.; Zhang, B.; Chin, M.T. Air pollution and adverse cardiac remodeling: Clinical effects and basic mechanisms. Front. Physiol. 2015, 6, 162. [Google Scholar] [CrossRef] [PubMed]
- Vieira, S.E. The health burden of pollution: The impact of prenatal exposure to air pollutants. Int. J. Chronic Obstr. Pulm. Dis. 2015, 10, 1111–1121. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.S.; Goggins, W.B.; Chiu, H.F.; Yang, C.Y. Evidence for an association between air pollution and daily stroke admissions in Kaohsiung, Taiwan. Stroke 2003, 34, 2612–2616. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Ambient (Outdoor) Air Quality and Health. Available online: http://www.who.int/mediacentre/factsheets/fs313/en/ (accessed on 14 November 2015).
- Qureshi, A.I.; Mendelow, A.D.; Hanley, D.F. Intracerebral haemorrhage. Lancet 2009, 373, 1632–1644. [Google Scholar] [CrossRef]
- Van Asch, C.J.; Luitse, M.J.; Rinkel, G.J.; van der Tweel, I.; Algra, A.; Klijn, C.J. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: A systematic review and meta-analysis. Lancet Neurol. 2010, 9, 167–176. [Google Scholar] [CrossRef]
- Chan, C.; Ting, H.; Huang, H. The incidence, hospital expenditure, and, 30 day and 1year mortality rates of spontaneous intracerebral hemorrhage in Taiwan. J. Clin. Neurosci. 2014, 21, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Xiang, H.; Mertz, K.J.; Arena, V.C.; Brink, L.L.; Xu, X.; Bi, Y.; Talbott, E.O. Estimation of short-term effects of air pollution on stroke hospital admissions in Wuhan, China. PLoS ONE 2013, 8, e61168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, Z.J.; Kristiansen, L.C.; Andersen, K.K.; Olsen, T.S.; Hvidberg, M.; Jensen, S.S.; Ketzel, M.; Loft, S.; Sørensen, M.; Tjønneland, A.; et al. Stroke and long-term exposure to outdoor air pollution from nitrogen dioxide: A cohort study. Stroke 2012, 43, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Han, M.H.; Yi, H.J.; Kim, Y.S.; Kim, Y.S. Effect of seasonal and monthly variation in weather and air pollution factors on stroke incidence in Seoul, Korea. Stroke 2015, 46, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Turin, T.C.; Kita, Y.; Rumana, N.; Nakamura, Y.; Ueda, K.; Takashima, N.; Sugihara, H.; Morita, Y.; Ichikawa, M.; Hirose, K.; et al. Ambient air pollutants and acute case-fatality of cerebro-cardiovascular events: Takashima Stroke and AMI Registry, Japan (1988–2004). Cerebrovasc. Dis. 2012, 34, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.L.; Lin, W.; Yang, N.P.; Huang, H.T. The association between the availability of ambulatory care and non-emergency treatment in emergency medicine departments: A comprehensive and nationwide validation. Health Policy 2013, 110, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.B.; Lai, K.R.; Yang, N.P.; Wu, K.S.; Ting, H.W.; Pan, R.H.; Chan, C.L. Trends and outcomes in the utilization of laparoscopic appendectomies in a low-income population in Taiwan from 2003 to 2011. Int. J. Equity Health 2015, 14, 100. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.; Ting, H.; Huang, H. The definition of a prolonged intensive care unit stay for spontaneous intracerebral hemorrhage patients: An application with national health insurance research database. BioMed Res. Int. 2014, 2014, 891725. [Google Scholar] [CrossRef] [PubMed]
- Introduction to the National Health Insurance Research Database (NHIRD). 2003. Available online: http://w3.nhri.org.tw/nhird/ (accessed on 15 October 2016).
- Taiwan Government Open Data Platform. 2017. Available online: http://data.gov.tw/ (accessed on 30 August 2017).
- Stavem, K.; Hoel, H.; Skjaker, S.A.; Haagensen, R. Charlson comorbidity index derived from chart review or administrative data: Agreement and prediction of mortality in intensive care patients. Clin. Epidemiol. 2017, 9, 311–320. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.L.; You, H.J.; Huang, H.T.; Ting, H.W. Using an integrated COC index and multilevel measurements to verify the care outcome of patients with multiple chronic conditions. BMC Health Serv. Res. 2012, 12, 405. [Google Scholar] [CrossRef] [PubMed]
- Innovation Center for Big Data and Digital Convergence, Yuan Ze University. 2013. Available online: http://www.innobic.yzu.edu.tw/ (accessed on 1 July 2014).
- Xing, Y.F.; Xu, Y.H.; Shi, M.H.; Lian, Y.X. The impact of PM2.5 on the human respiratory system. J. Thorac. Dis. 2016, 8, E69–E74. [Google Scholar] [PubMed]
- Wang, Y.; Eliot, M.N.; Wellenius, G.A. Short-term changes in ambient particulate matter and risk of stroke: A systematic review and meta-analysis. J. Am. Heart Assoc. 2014, 3, e000983. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.C.; Chuang, K.J.; Chien, L.C.; Chen, W.J.; Chang, W.T. Urban air pollution and emergency admissions for cerebrovascular diseases in Taipei, Taiwan. Eur. Heart J. 2006, 27, 1238–1244. [Google Scholar] [CrossRef] [PubMed]
- Villeneuve, P.J.; Chen, L.; Stieb, D.; Rowe, B.H. Associations between outdoor air pollution and emergency department visits for stroke in Edmonton, Canada. Eur. J. Epidemiol. 2006, 21, 689–700. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Region | Taipei | Taoyuan | Taichung | Tainan | Kaohsiung |
|---|---|---|---|---|---|
| # Resident population | 6,709,982 | 2,190,342 | 2,731,056 | 1,840,257 | 2,777,384 |
| Male | 3,252,868 | 1,107,819 | 1,353,789 | 915,361 | 1,381,183 |
| Female | 3,457,114 | 1,052,523 | 1,377,267 | 924,896 | 1,396,201 |
| Total case number | 14,041 | 5537 | 7654 | 4739 | 7082 |
| Female ratio (%) | 38.0% | 36.4% | 36.9% | 37.3% | 37.4% |
| ¶ Incidence of sICH | 216.4 | 280.0 | 290.4 | 252.9 | 255.6 |
| Male | 272.6 | 352.5 | 367.4 | 314.0 | 318.2 |
| Female | 161.9 | 206.0 | 213.6 | 190.6 | 192.3 |
| Mean age | 61.9 (16.6) | 60.4 (16.7) | 61.6 (15.9) | 62.6 (15.4) | 61.5 (15.6) |
| Male | 60.1 (16.1) | 59.0 (16.4) | 59.7 (15.5) | 60.7 (14.8) | 59.6 (15.0) |
| Female | 64.8 (17.1) | 62.8 (17.0) | 64.7 (16.2) | 65.8 (15.8) | 64.6 (16.0) |
| Low-income cases (%) | 250 (1.8%) | 122 (2.2%) | 65 (0.8%) | 60 (1.3%) | 83 (1.2%) |
| & CCI | |||||
| 0 (%) | 6660 (47.4%) | 2690 (48.6%) | 4015 (52.5%) | 2329 (49.1) | 3476 (49.1%) |
| 1 (%) | 3834 (27.3%) | 1492 (26.9%) | 2007 (26.2%) | 1361 (28.7%) | 1829 (25.8%) |
| 2 (%) | 2356 (16.8%) | 945 (17.1%) | 1118 (14.6%) | 723 (15.3%) | 1175 (16.6%) |
| ≥3 (%) | 1191 (8.5%) | 410 (7.4%) | 514 (6.7%) | 326 (6.9%) | 602 (8.5%) |
| Total LOS | 17.3 (14.8) | 14.8 (13.4) | 15.8 (13.7) | 13.9 (11.9) | 14.0 (11.5) |
| Air Pollutant | CO | NO2 | O3 | PM10 | PM2.5 | SO2 |
|---|---|---|---|---|---|---|
| Abnormal criteria | 35 ppm | 250 ppb | 120 ppb | 125 μg/m3 | 35 μg/m3 | 100 ppb |
| (30.5 ppm) ψ | (1250 ppb) | (405 ppb) | (425 μg/m3) | (250.5 μg/m3) | (650 ppb) | |
| 8-h | 1-h | 1-h | 24-h | 24-h | 24-h | |
| Mean concentration | ||||||
| Taipei | 0.6 (0.1) | 21.1 (3.2) | 28 (5.2) | 46.8 (9.6) | 26.8 (5.3) | 3.8 (0.5) |
| Taoyuan | 0.5 (0.1) | 19.4 (2.9) | 28.5 (5.3) | 56.5 (11.1) | 28.0 (6.1) | 5.6 (0.4) |
| Taichung | 0.5 (0.1) | 18.8 (4) | 28.1 (5.4) | 58.5 (13.5) | 35.6 (8.4) | 3.5 (0.3) |
| Tainan | 0.4 (0.1) | 15.3 (4.7) | 30.9 (6.5) | 73.6 (23.7) | 39.2 (12.5) | 4.2 (0.4) |
| Kaohsiung | 0.5 (0.2) | 20.3 (6.8) | 29.9 (6.6) | 77.3 (27.5) | 44.9 (16.4) | 7.2 (1.2) |
| # Days on which normal level was exceeded | ||||||
| Taipei | 0 (0) ξ | 0 (0) | 153 (0) | 13 (1) | 428 (0) | 0 (0) |
| Taoyuan | 0 (0) | 0 (0) | 135 (0) | 31 (1) | 465 (0) | 0 (0) |
| Taichung | 0 (0) | 0 (0) | 393 (0) | 32 (1) | 818 (0) | 0 (0) |
| Tainan | 0 (0) | 0 (0) | 566 (0) | 127 (1) | 988 (0) | 0 (0) |
| Kaohsiung | 0 (0) | 0 (0) | 647 (0) | 183 (1) | 1159 (0) | 0 (0) |
| Air Pollutant | CO | NO2 | O3 | PM10 | PM2.5 | SO2 |
|---|---|---|---|---|---|---|
| Standard values | 35 ppm | 250 ppb | 120/h | 125 μg/m3 | 35 μg/m3 | 100 ppb |
| Correlation between air pollutants | ||||||
| CO | 1 | |||||
| NO2 | 0.939 ** | 1 | ||||
| O3 | 0.034 | 0.071 | 1 | |||
| PM10 | 0.399 ** | 0.610 *** | 0.372 ** | 1 | ||
| PM2.5 | 0.463 *** | 0.637 *** | 0.343 ** | 0.969 *** | 1 | |
| SO2 | 0.239 | 0.422 *** | 0.085 | 0.550 *** | 0.521 *** | 1 |
| All patients | 0.205 | 0.415 *** | 0.013 | 0.658 *** | 0.654 *** | 0.196 |
| <24 y/o ψ | −0.015 | −0.010 | −0.056 | −0.212 | −0.226 | −0.035 |
| 25–44 y/o | 0.197 | 0.341 ** | −0.163 | 0.197 | 0.180 | 0.296 * |
| 45–64 y/o | 0.124 | 0.333 ** | 0.033 | 0.629 *** | 0.625 *** | 0.245 |
| 65–79 y/o | 0.114 | 0.311 * | 0.096 | 0.689 *** | 0.695 *** | 0.110 |
| ≥80 y/o | 0.383 ** | 0.473 *** | −0.053 | 0.456 *** | 0.445 *** | −0.004 |
| Models | Constant | PM2.5 | O3 | SO2 | Adj. R2 | F for Change in R2 |
|---|---|---|---|---|---|---|
| Model 1 | X | X | 0.417 | 43.263 ** | ||
| B | 15.127 *** | 0.166 *** | ||||
| SE B | 0.654 | |||||
| Model 2 | X | 0.459 | 5.488 * | |||
| B | 18,171 *** | 0.187 *** | −0.130 * | |||
| SE B | 0.735 | −0.239 | ||||
| Model 3 | 0.490 | 4.497 * | ||||
| B | 19.745 *** | 0.219 *** | −0.143 * | −0.482 * | ||
| SE B | 0.865 | −0.263 | −0.233 |
| Factor | Constant | PM2.5 | O3 | SO2 | NO2 | Adj. R2 | F for Change in R2 |
|---|---|---|---|---|---|---|---|
| Less than 25 years of age | |||||||
| Model | X | X | X | X | X | ||
| Between 25 and 44 years | |||||||
| Model | X | X | X | 0.101 | 7.616 ** | ||
| B | 1.711 *** | 0.036 ** | |||||
| SE B | 0.341 | ||||||
| Between 45 and 64 years | |||||||
| Model | X | X | X | 0.380 | 37.195 *** | ||
| B | 6.450 *** | 0.068 *** | |||||
| SE B | 0.625 | ||||||
| Between 65 and 79 years | |||||||
| Model 1 | X | X | X | 0.474 | 54.077 *** | ||
| B | 3.805 *** | 0.071 *** | |||||
| SE B | 0.695 | ||||||
| Model 2 | X | X | 0.554 | 11.527 ** | |||
| B | 4.559 *** | 0.089 *** | −0.288 *** | ||||
| SE B | 0.875 | −0.346 | |||||
| Model 3 | X | 0.583 | 4.938 * | ||||
| B | 5.643 *** | 0.098 *** | −0.044 * | −0.310 *** | |||
| SE B | 0.957 | −0.200 | −0.372 | ||||
| Model 4 | 0.607 | 4.377 * | |||||
| B | 6.384 *** | 0.113 *** | −0.052 * | −0.290 *** | −0.059 * | ||
| SE B | 1.102 | −0.236 | −0.348 | −0.228 | |||
| Over 80 years of age | |||||||
| Model | X | X | X | 0.211 | 16.746 *** | ||
| B | 1.905 *** | 0.059 *** | |||||
| SE B | 0.473 | ||||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chien, T.-Y.; Ting, H.-W.; Chan, C.-L.; Yang, N.-P.; Pan, R.-H.; Lai, K.R.; Hung, S.-I. Does the Short-Term Effect of Air Pollution Influence the Incidence of Spontaneous Intracerebral Hemorrhage in Different Patient Groups? Big Data Analysis in Taiwan. Int. J. Environ. Res. Public Health 2017, 14, 1547. https://doi.org/10.3390/ijerph14121547
Chien T-Y, Ting H-W, Chan C-L, Yang N-P, Pan R-H, Lai KR, Hung S-I. Does the Short-Term Effect of Air Pollution Influence the Incidence of Spontaneous Intracerebral Hemorrhage in Different Patient Groups? Big Data Analysis in Taiwan. International Journal of Environmental Research and Public Health. 2017; 14(12):1547. https://doi.org/10.3390/ijerph14121547
Chicago/Turabian StyleChien, Ting-Ying, Hsien-Wei Ting, Chien-Lung Chan, Nan-Ping Yang, Ren-Hao Pan, K. Robert Lai, and Su-In Hung. 2017. "Does the Short-Term Effect of Air Pollution Influence the Incidence of Spontaneous Intracerebral Hemorrhage in Different Patient Groups? Big Data Analysis in Taiwan" International Journal of Environmental Research and Public Health 14, no. 12: 1547. https://doi.org/10.3390/ijerph14121547