Differences in Spontaneous Intracerebral Hemorrhage Cases between Urban and Rural Regions of Taiwan: Big Data Analytics of Government Open Data

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
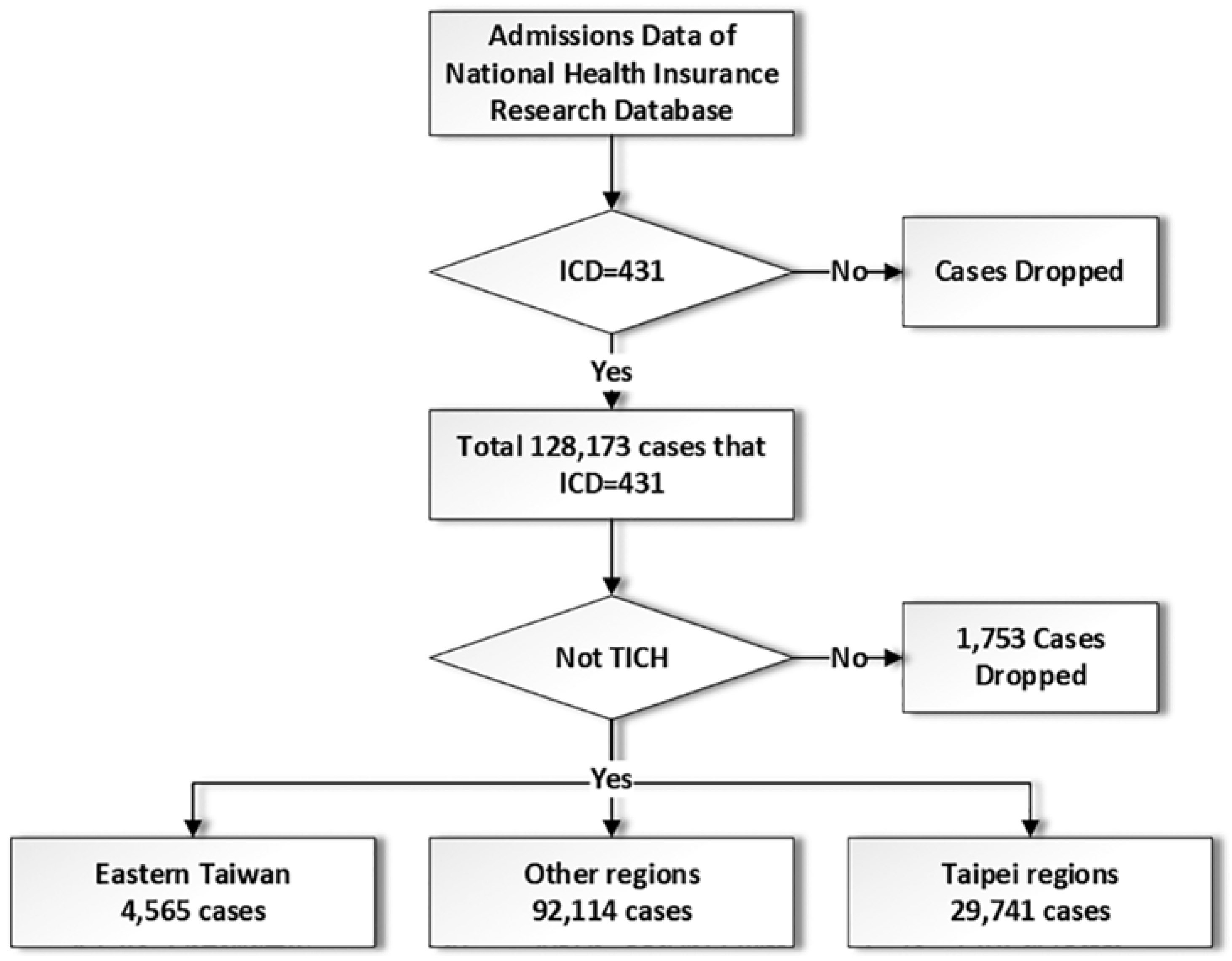
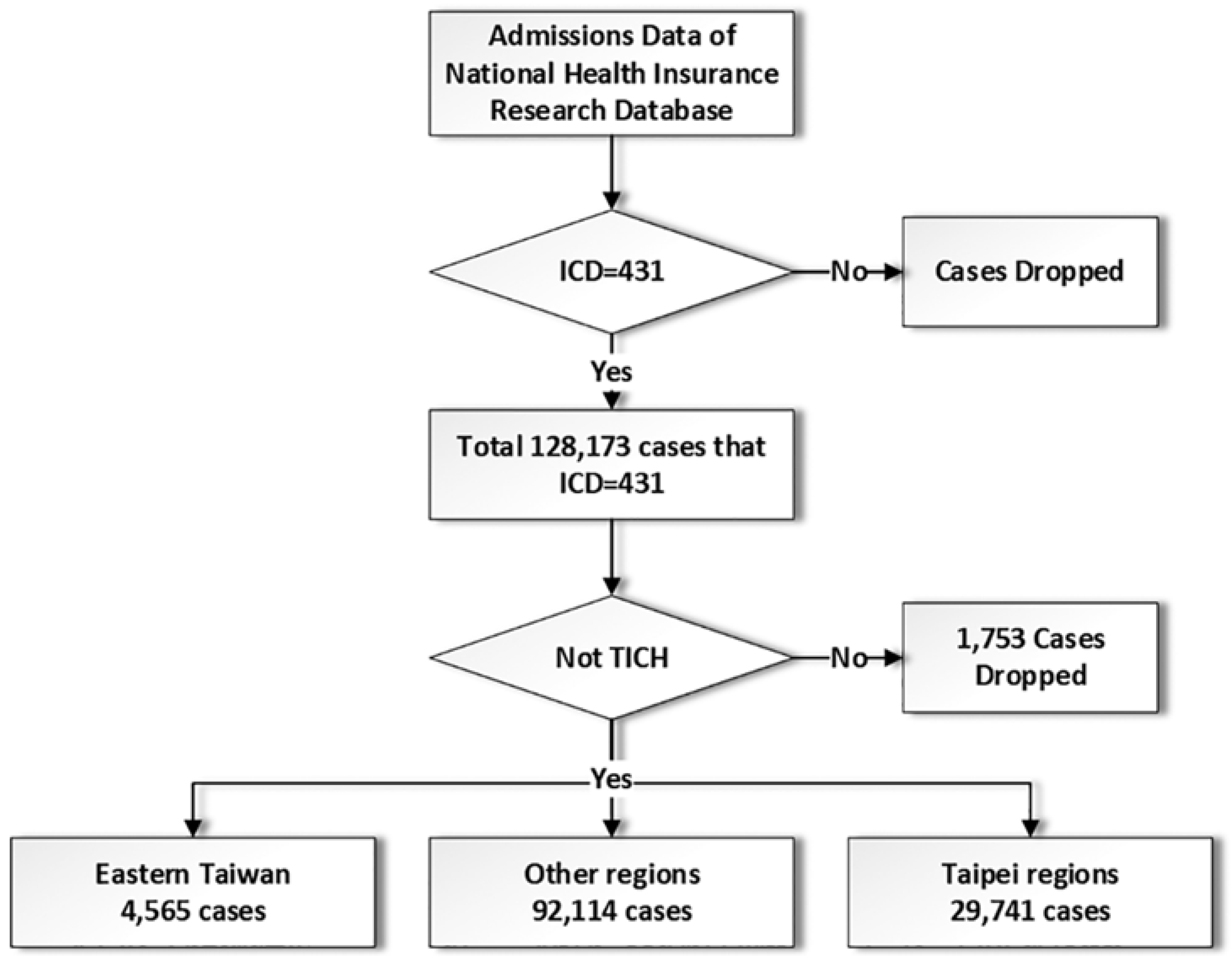
2.1. Data Source
2.2. Data Protection and Permission
2.3. Data Management
2.4. Statistics and Data Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Chan, C.; Ting, H.; Huang, H. The definition of a prolonged intensive care unit stay for spontaneous intracerebral hemorrhage patients: An application with national health insurance research database. Biomed. Res. Int. 2014, 2014, 891725. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.; Ting, H.; Huang, H. The incidence, hospital expenditure, and, 30 day and 1 year mortality rates of spontaneous intracerebral hemorrhage in Taiwan. J. Clin. Neurosci. 2013, 21, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Thanvi, B.R.; Sprigg, N.; Munshi, S.K. Advances in spontaneous intracerebral haemorrhage. Int. J. Clin. Pract. 2012, 66, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Mensah, N.; Sukums, F.; Awine, T.; Meid, A.; Williams, J.; Akweongo, P.; Kaltschmidt, J.; Haefeli, W.E.; Blank, A. Impact of an electronic clinical decision support system on workflow in antenatal care: The QUALMAT eCDSS in rural health care facilities in Ghana and Tanzania. Glob. Health Action 2015, 8, 25756. [Google Scholar] [CrossRef] [PubMed]
- Barakat-Haddad, C.; Siddiqua, A. Primary health care use and health care accessibility among adolescents in the united arab emirates. East Mediterr. Health J. 2015, 21, 171–184. [Google Scholar] [CrossRef] [PubMed]
- Sobolewski, P.; Szczuchniak, W.; Sobota, A.; Grzesik, M. Are there differences between rural and urban populations in long-term outcome after systemic cerebral thrombolysis in a hospital located in an agricultural region? Rural Remote Health 2014, 14, 2867. [Google Scholar] [PubMed]
- Chen, R.; Hu, Z.; Chen, R.-L.; Zhang, D.; Xu, L.; Wang, J.; Wei, L. Socioeconomic deprivation and survival after stroke in china: A systematic literature review and a new population-based cohort study. BMJ Open 2015, 5, e005688. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.N.; McCulloch, B.J. ‘Heart attack’ symptoms and decision-making: The case of older rural women. Rural Remote Health 2014, 14, 2560. [Google Scholar] [PubMed]
- Guo, H.; Wang, L.; Chen, F.; Liang, D. Scientific big data and digital earth. Chin. Sci. Bull. 2014, 59, 5066–5073. [Google Scholar]
- Chen, Y.-C.; Yeh, H.-Y.; Wu, J.-C.; Haschler, I.; Chen, T.-J.; Wetter, T. Taiwan’s National Health Insurance Research Database: Administrative health care database as study object in bibliometrics. Scientometrics 2011, 86, 365–380. [Google Scholar] [CrossRef]
- Cheng, C.L.; Kao, Y.H.; Lin, S.J.; Lee, C.H.; Lai, M.L. Validation of the National Health Insurance Research Database with ischemic stroke cases in Taiwan. Pharmacoepidemiol. Drug Saf. 2011, 20, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Introduction to the National Health Insurance Research Database (NHIRD). Available online: http://w3.nhri.org.tw/nhird/ (accessed on 15 October 2016).
- Department of Household Registration, M.O.I., 2016. Available online: http://www.ris.gov.tw/zh_TW/346 (accessed on 15 October 2016).
- 2010 Population and Housing Census. 2011. Available online: http://ebas1.ebas.gov.tw/phc2010/chinese/rchome.htm (accessed on 12 November 2016).
- Taiwan Government Open Data Platform. 2017. Available online: http://data.gov.tw/ (accessed on 30 November 2017).
- Chan, C.-L.; You, H.-J.; Huang, H.-T.; Ting, H.-W. Using an integrated coc index and multilevel measurements to verify the care outcome of patients with multiple chronic conditions. BMC Health Serv. Res. 2012, 12, 405. [Google Scholar] [CrossRef] [PubMed]
- Stavem, K.; Hoel, H.; Skjaker, S.A.; Haagensen, R. Charlson comorbidity index derived from chart review or administrative data: Agreement and prediction of mortality in intensive care patients. Clin. Epidemiol. 2017, 9, 311–320. [Google Scholar] [CrossRef] [PubMed]
- Schadt, E.E. The changing privacy landscape in the era of big data. Mol. Syst. Biol. 2012, 8, 612. [Google Scholar] [CrossRef] [PubMed]
- Wood, D.; King, M.; Landis, D.; Courtney, W.; Wang, R.; Kelly, R.; Turner, J.A.; Calhoun, V.D. Harnessing modern web application technology to create intuitive and efficient data visualization and sharing tools. Front. Neuroinform. 2014, 8, 71. [Google Scholar] [CrossRef] [PubMed]
- Schoeps, A.; Gabrysch, S.; Niamba, L.; Sie, A.; Becher, H. The effect of distance to health-care facilities on childhood mortality in rural burkina faso. Am. J. Epidemiol. 2011, 173, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.C.; Chou, C.L.; Chiang, S.C.; Chen, T.J.; Chou, L.F.; Chou, Y.C. Urban-rural disparity of generics prescription in Taiwan: The example of dihydropyridine derivatives. Sci. World J. 2014, 2014, 905213. [Google Scholar] [CrossRef] [PubMed]
- Celikbilek, A.; Goksel, B.K.; Zararsiz, G.; Benli, S. Spontaneous intra-cerebral hemorrhage: A retrospective study of risk factors and outcome in a Turkish population. J. Neurosci. Rural Pract. 2013, 4, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Vang, S. Barriers to cancer screening in Hmong Americans: The influence of health care accessibility, culture, and cancer literacy. J. Community Health 2010, 35, 302–314. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Regions | Taipei Region (Urban Area) | Eastern Taiwan (Rural Area) |
|---|---|---|
| Region Demographic Data | ||
| Resident population (average 2001 ~ 2011) | 6,396,597 | 582,108 |
| Male | 3,167,119 (49.51%) | 305,268 (52.44%) |
| Female | 3,229,478 (50.49%) | 276,840 (47.56%) |
| <24 y/o | 2,030,830 (31.75%) | 186,927 (32.11%) |
| 25~44 y/o | 2,152,713 (33.65%) | 184,737 (31.74%) |
| 45~64 y/o | 1,631,497 (25.51%) | 140,433 (24.12%) |
| 65~79 y/o | 448,614 (7.01%) | 54,396 (9.34%) |
| ≥80 y/o | 132,943 (2.08%) | 15,615 (2.68%) |
| Permanent resident population (2010) | 6,709,982 | 510,980 |
| Area (km2) | 2324.4 | 8143.9 |
| Resident population density *** | 2751.93 | 71.48 |
| Permanent resident population density *** | 2861.42 | 62.38 |
| Average income per year (US$) *** | 10,112 | 4200 |
| Total low-income residents (2010) (%) *** | 1.3% | 3.1% |
| Smoker (average 2006~2010) (%) | 20.84% | 23.51% |
| Educational Status of Residents *** | ||
| Elementary school | 12.1% | 25.0% |
| Junior high school | 12.3% | 16.7% |
| Senior high school | 28.9% | 32.7% |
| University/college | 46.7% | 25.5% |
| Regions | Taipei Region (Urban Area) | Eastern Taiwan (Rural Area) |
|---|---|---|
| Hospital Facilities | ||
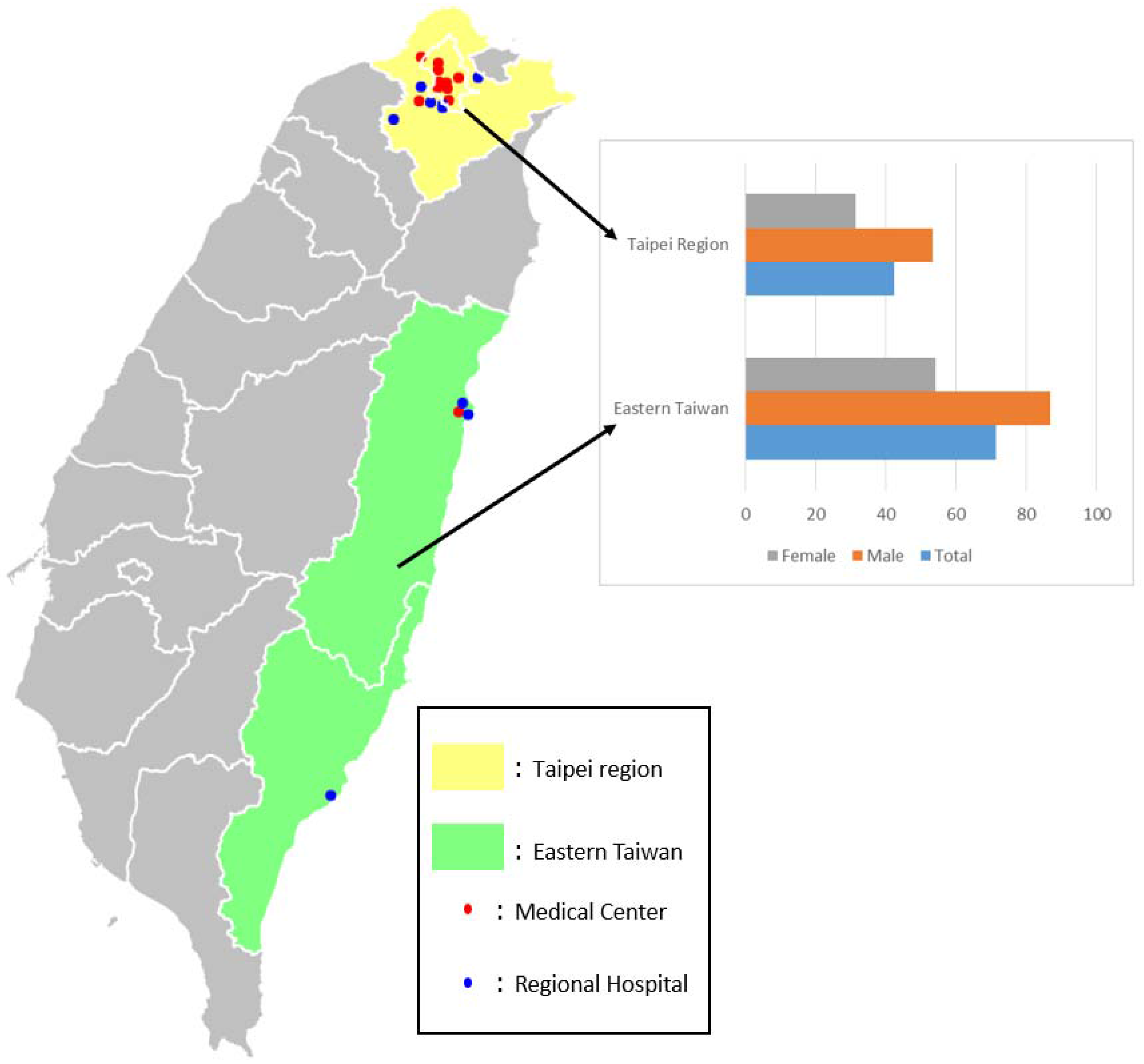
| Hospital numbers | 97 | 18 |
| Medical centres | 12 | 1 |
| Regional hospitals | 15 | 3 |
| Mean coverage area per hospital (km2) | 24 | 452.4 |
| Total hospital beds | 33,570 | 5588 |
| Total ICU beds | 1861 | 238 |
| Hospital beds per 10,000 population | 52.6 | 96 |
| ICU beds per 10,000 population | 2.9 | 4.1 |
| Hospital beds per 10,000 population (permanent) | 50 | 109.4 |
| ICU beds per 10,000 population (permanent) | 2.8 | 4.7 |
| Medical Staff | ||
| Medical staff | 44,556 | 4555 |
| Physicians | 8529 | 733 |
| Medical staff per 10,000 population *** | 69.7 | 78.3 |
| Physicians per 10,000 population * | 13.3 | 12.6 |
| Medical staff per 10,000 population (permanent) *** | 66.4 | 89.1 |
| Physicians per 10,000 population (permanent) ** | 12.7 | |
| Regions | Taipei Region (Urban Area) | Eastern Taiwan (Rural Area) |
|---|---|---|
| Total case number (2001–2011) | 29,741 | 4565 |
| Male | 18,597 (62.5%) | 2910 (63.5%) |
| Female | 11,144 (37.5%) | 1655 (36.3%) |
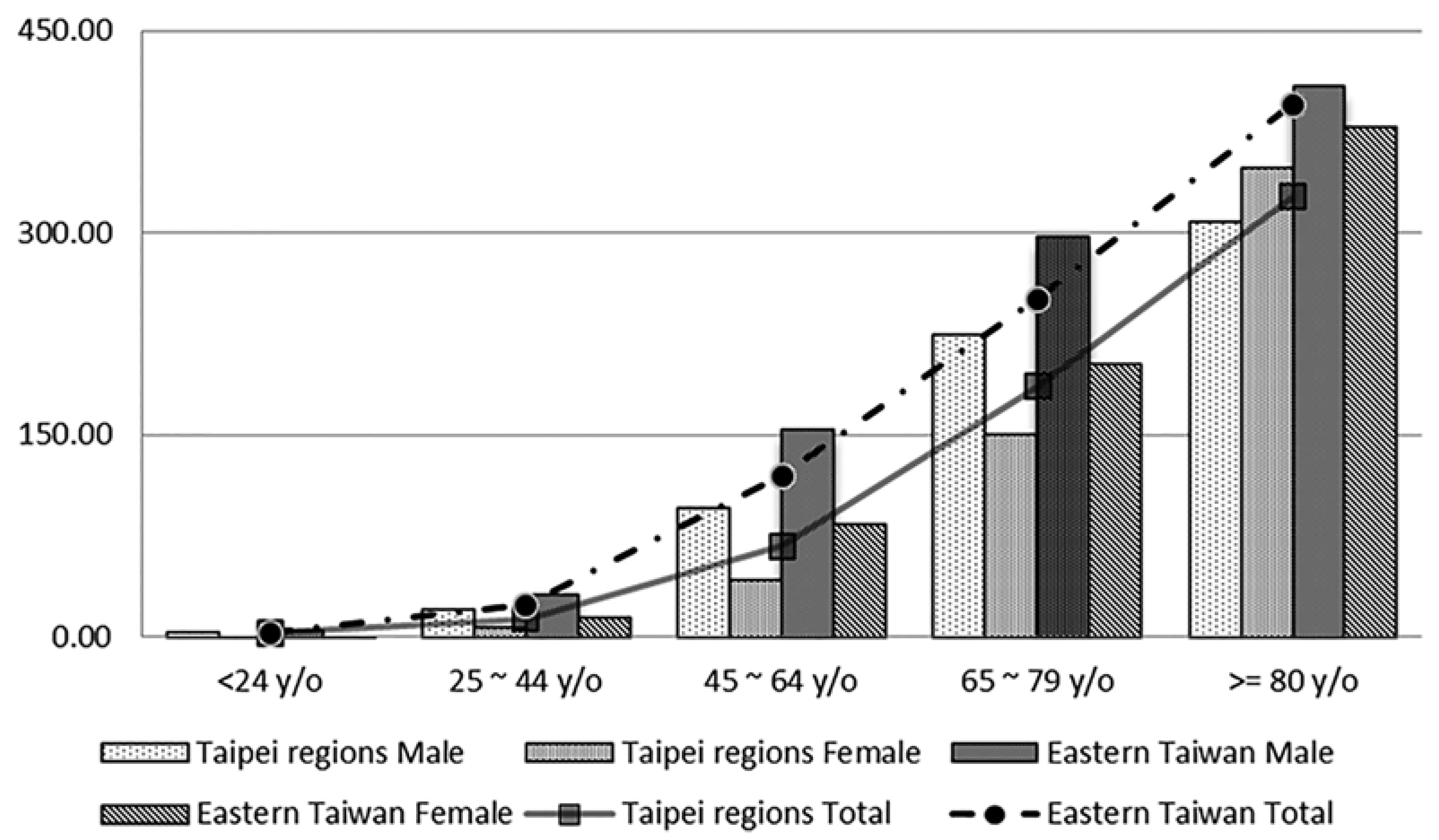
| Incidence per 100,000 population per year *** | 42.3 | 71.3 |
| Male | 53.4 | 86.7 |
| Female | 31.4 | 54.3 |
| Mean age | 62.4 (16.34) | 62.7 (15.58) |
| Male | 60.7 (15.95) | 61.6 (15.78) |
| Female | 65.2 (16.59) | 64.6 (15.03) |
| Low-income and veteran patients (%) | 2525 (8.5%) | 483 (10.6%) |
| Charlson Comorbidity Index (CCI) | ||
| 0 (%) | 14,569 (49.0%) | 2271 (49.8%) |
| 1 (%) | 7678 (25.8%) | 1283 (28.1%) |
| 2 (%) | 4918 (16.5%) | 732 (16.0%) |
| 3 (%) | 1512 (5.1%) | 162 (3.5%) |
| ≥4 (%) | 1064 (3.6%) | 117 (2.6%) |
| Mean hospital length of stay (SD) *** | 17.9 (15.13) | 16.3 (13.82) |
| Mean ICU length of stay | 10.2 (17.13) | 8.4 (10.60) |
| Prolonged ICU stay | 35.4% | 26.9% |
| Surgical intervention rate | 24.9% | 29.3% |
| §Total hospital expenditure (SD) | 4674 (5977.8) | 4873 (5433.8) |
| Doctor fees (SD) *** | 253 (212,4) | 235 (202.2) |
| Room fees (SD) * | 1442 (1658.6) | 1404 (1579.7) |
| Examination fees (SD) * | 277 (380.3) | 225 (313.0) |
| Surgical fees if received surgery (SD) | 1333 (1071.1) | 1310 (1014.1) |
| Medications fees (SD) *** | 740 (2536.7) | 723 (1358.1) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ting, H.-W.; Chien, T.-Y.; Lai, K.R.; Pan, R.-H.; Wu, K.-H.; Chen, J.-M.; Chan, C.-L. Differences in Spontaneous Intracerebral Hemorrhage Cases between Urban and Rural Regions of Taiwan: Big Data Analytics of Government Open Data. Int. J. Environ. Res. Public Health 2017, 14, 1548. https://doi.org/10.3390/ijerph14121548
Ting H-W, Chien T-Y, Lai KR, Pan R-H, Wu K-H, Chen J-M, Chan C-L. Differences in Spontaneous Intracerebral Hemorrhage Cases between Urban and Rural Regions of Taiwan: Big Data Analytics of Government Open Data. International Journal of Environmental Research and Public Health. 2017; 14(12):1548. https://doi.org/10.3390/ijerph14121548
Chicago/Turabian StyleTing, Hsien-Wei, Ting-Ying Chien, K. Robert Lai, Ren-Hao Pan, Kuan-Hsien Wu, Jun-Min Chen, and Chien-Lung Chan. 2017. "Differences in Spontaneous Intracerebral Hemorrhage Cases between Urban and Rural Regions of Taiwan: Big Data Analytics of Government Open Data" International Journal of Environmental Research and Public Health 14, no. 12: 1548. https://doi.org/10.3390/ijerph14121548