
The Feasibility of Embedding Data Collection into the Routine Service Delivery of a Multi-Component Program for High-Risk Young People

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Service and Setting
2.2. Participants of the Service
2.3. Measures
2.4. Procedure to Optimise the Feasibility of Applying Best-Evidence Measures
2.5. Statistical Methods
2.6. Ethical Considerations, Ethics Approval and Consent to Participate
3. Results
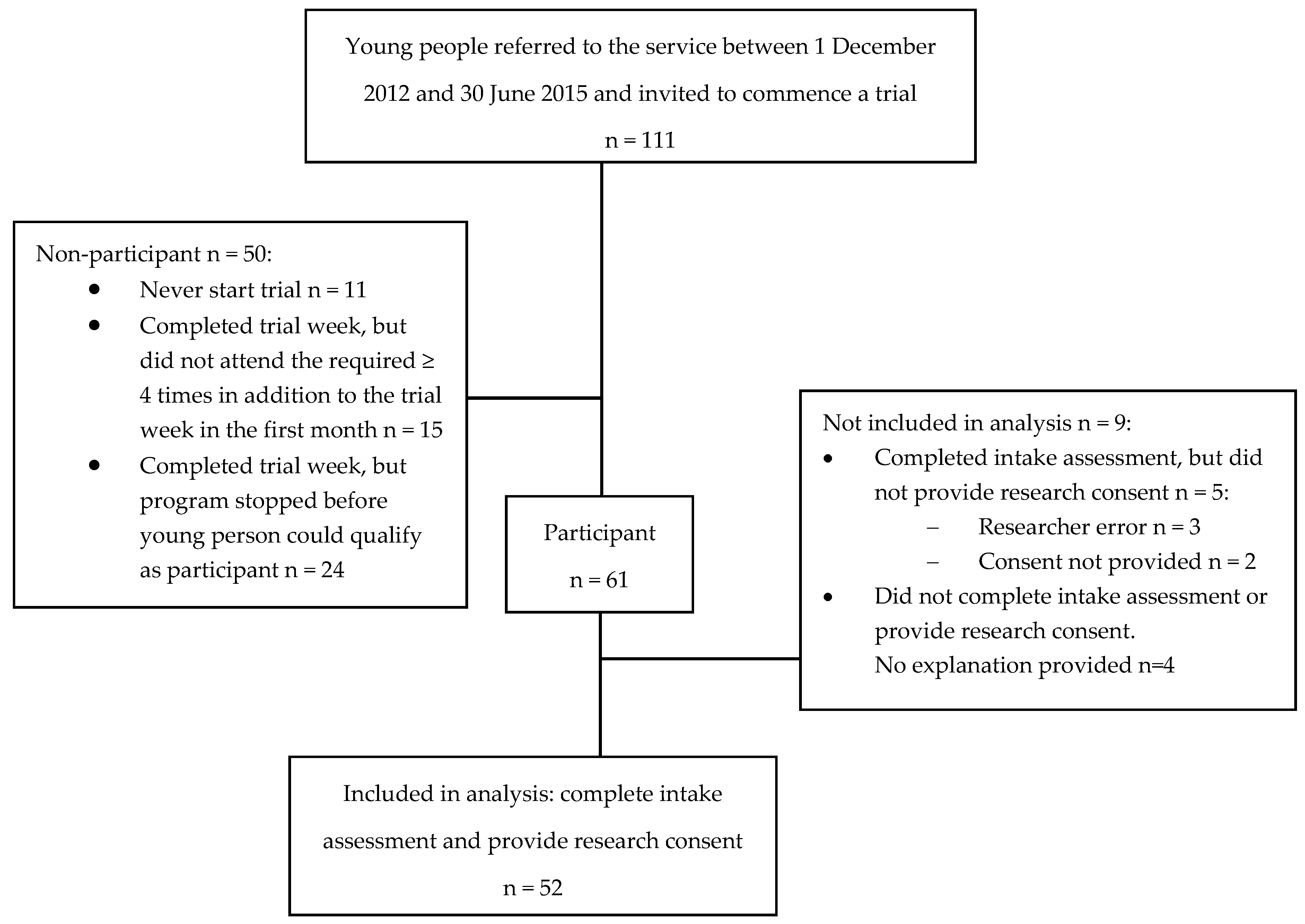
3.1. The Feasibility of Embedding Data Collection in the Routine Processes of A Service for High-Risk Young People
3.2. Demographic Characteristics and Risk Factors of Program Participants
4. Discussion
4.1. The Feasibility of Embedding Data Collection in the Routine Processes of a Service for High-Risk Young People
4.2. The Utility of Embedding Data Collection in the Routine Processes of a Service for High-Risk Young People
4.3. Other Implications of This Study
4.4. Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| ASSIST | Alcohol, Smoking and Substance Involvement Screening Test |
| AUDIT | Alcohol Use Disorders Identification Test |
| BE | Best-evidence |
| CD-RISC-10 | Connor Davidson Resilience Scale (10-item) |
| HSI | Heaviness of Smoking Index |
| K6 | Kessler Psychological Distress Scale (six-item) |
| N | New item |
| NSW | New South Wales 0 |
| SP | Similar population group |
| SAK | Suicide Assessment Kit |
References
- Hawkins, E.H. A tale of two systems: Co-occurring mental health and substance abuse disorders treatment for adolescents. Annu. Rev. Psychol. 2009, 60, 197–227. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, P.F. Evidence-based practice in real-world services for young people with complex needs: New opportunities suggested by recent implementation science. Child. Youth Serv. Rev. 2011, 33, 207–216. [Google Scholar] [CrossRef]
- Department of Economic and Social Affairs, United Nations. World Youth Report 2003: The Global Situation of Young People; Department of Economic and Social Affairs of the United Nations Secretariat, United Nations: New York, NY, USA, 2004. [Google Scholar]
- Bruun, A.; MItchell, P. A Resource for Strengthening Therapeutic Practice Frameworks in Youth AOD Services; Youth Support and Advocacy Service (YSAS): Melbourne, Australia, 2012. [Google Scholar]
- Hawkins, J.D.; Catalano, R.F.; Miller, J.Y. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: Implications for substance abuse prevention. Psychol. Bull. 1992, 112, 64. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, K.A.; Green, J.G.; Gruber, M.J.; Sampson, N.A.; Zaslavsky, A.M.; Kessler, R.C. Childhood adversities and adult psychiatric disorders in the national comorbidity survey replication II: Associations with persistence of DSM-IV disorders. Arch. Gen. Psychiatry 2010, 67, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Henry, K.L. Academic Achievement and Adolescent Drug Use: An Examination of Reciprocal Effects and Correlated Growth Trajectories. J. Sch. Health 2010, 80, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Henry, K.L.; Knight, K.E.; Thornberry, T.P. School disengagement as a predictor of dropout, delinquency, and problem substance use during adolescence and early adulthood. J. Youth Adolesc. 2012, 41, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Fergusson, D.M.; Horwood, L.; Nagin, D.S. Offending trajectories in a New Zealand birth cohort. Criminology 2000, 38, 525–552. [Google Scholar] [CrossRef]
- Vitaro, F.; Tremblay, R.E. Clarifying and Maximizing the Usefulness of Targeted Preventive Interventions, in Rutter’s Child and Adolescent Psychiatry, 5th ed.; Rutter, M.E.A., Ed.; Blackwell Publishing Ltd.: Oxford, UK, 2009; pp. 989–1008. [Google Scholar]
- Groark, C.J.; McCall, R.B. Community-Based Interventions and Services, in Rutter’s Child and Adolescent Psychiatry; Blackwell Publishing Ltd.: Oxford, UK, 2009; pp. 969–988. [Google Scholar]
- Calabria, B.; Doran, C.M.; Vos, T.; Shakeshaft, A.P.; Hall, W. Epidemiology of alcohol-related burden of disease among Indigenous Australians. Aust. N. Z. J. Public Health 2010, 34, S47–S51. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Criminology. Australian Crime. Facts and Figures 2007; Australian Institute of Criminology: Canberra, Australia, 2008.
- Australian Institute of Health and Welfare (AIHW). Rural, Regional and Remote Health: A Study on Mortality, in Rural Health; Series no. 3; AIHW: Canberra, Australia, 2007.
- Knight, A.; Shakeshaft, A.; Havard, A.; Maple, M.; Foley, C.; Shakeshaft, B. The quality and effectiveness of interventions that target multiple risk factors among young people: A Systematic Review. Aust. N. Z. J. Public Health 2016. [Google Scholar] [CrossRef] [PubMed]
- Campbell, D.; Pyett, P.; McCarthy, L.; Whiteside, M.; Tsey, K. Community development and empowerment—A review of interventions to improve aboriginal health. In Beyond Bandaids: Exploring the Underlying Social Determinants of Aboriginal Health; Anderson, I., Baum, F., Bentley, M., Eds.; Cooperative Research Centre for Aboriginal Health: Darwin, Australia, 2007; pp. 165–180. [Google Scholar]
- Campbell, M.; Ray, F.; Andrew, H.; Louise, K.A.; Peter, S.; David, S.; Peter, T. Framework for design and evaluation of complex interventions to improve health. BMJ 2000, 321, 694–696. [Google Scholar] [CrossRef] [PubMed]
- Snijder, M.; Shakeshaft, A.; Wagemakers, A.; Stephens, A.; Calabria, B. A systematic review of studies evaluating Australian indigenous community development projects: The extent of community participation, their methodological quality and their outcomes. BMC Public Health 2015, 15, 1154. [Google Scholar] [CrossRef] [PubMed]
- Jackson, C.L.; Greenhalgh, T. Co-creation: A new approach to optimising research impact? Med. J. Aust. 2015, 203, 283–284. [Google Scholar] [CrossRef] [PubMed]
- Voorberg, W.H.; Bekkers, V.J.J.M.; Tummers, L.G. A systematic review of co-creation and co-production: embarking on the social innovation journey. Public Manag. Rev. 2015, 17, 1333–1357. [Google Scholar] [CrossRef] [Green Version]
- Heath, A.C.; Lynskey, M.T.; Waldron, M. Substance Use and Substance Use Disorder. In Rutter’s Child and Adolescent Psychiatry, 5th ed.; Rutter, M., Bishop, D., Pine, D., Scott, S., Stevenson, J., Taylor, E., Thapar, A., Eds.; Blackwell Publishing: Hoboken, NJ, USA, 2008. [Google Scholar]
- Centre for Epidemiology and Evidence. New South Wales School Students Health Behaviours Survey: 2011 Report; NSW Ministry of Health: Sydney, Australia, 2013.
- Batterham, P.J.; Christensen, H.; Calear, A.L. Anxiety symptoms as precursors of major depression and suicidal ideation. Depress Anxiety 2013, 30, 908–916. [Google Scholar] [CrossRef] [PubMed]
- Lindelow, M.; Hardy, R.; Rodgers, B. Development of a scale to measure symptoms of anxiety and depression in the general UK population: The psychiatric symptom frequency scale. J. Epidemiol. Community Health 1997, 51, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Campbell-Sills, L.; Stein, M.B. Psychometric analysis and refinement of the Connor-Davidson Resilience Scale (CD-RISC): Validation of a 10-item measure of resilience. J. Trauma. Stress 2007, 20, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Hartley, M.T. Assessing and Promoting Resilience: An Additional Tool to Address the Increasing Number of College Students with Psychological Problems. J. Coll. Couns. 2012, 15, 37–51. [Google Scholar] [CrossRef]
- Campbell-Sills, L.; Forde, D.R.; Stein, M.B. Demographic and childhood environmental predictors of resilience in a community sample. J. Psychiatr. Res. 2009, 43, 1007–1012. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, T.A.; Kessler, R.C.; Slade, T.; Andrews, G. The performance of the K6 and K10 screening scales for psychological distress in the Australian National Survey of Mental Health and Well-Being. Psychol. Med. 2003, 33, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Green, J.G.; Gruber, M.J.; Sampson, N.A.; Bromet, E.; Cuitan, M.; Furukawa, T.A.; Gureje, O.; Hinkov, H.; Hu, C.-Y.; et al. Screening for serious mental illness in the general population with the K6 screening scale: Results from the WHO World Mental Health (WMH) survey initiative. Int. J. Methods Psychiatr. Res. 2010, 19, 4–22. [Google Scholar] [CrossRef] [PubMed]
- Babor, T.F.; Higgins-Biddle, J.C.; Saunders, J.B.; Monteiro, M.G. The Alcohol Use Disorders Identification Test: Guidelines for Use in Primary Care; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Reinert, D.F.; Allen, J.P. The alcohol use disorders identification test: An update of research findings. Alcohol.: Clin. Exp. Res. 2007, 31, 185–199. [Google Scholar] [CrossRef] [PubMed]
- Calabria, B.; Clifford, A.; Shakeshaft, A.P.; Conigrave, K.M.; Simpson, L.; Bliss, D.; Allan, J. Identifying Aboriginal-specific AUDIT-C and AUDIT-3 cutoff scores for at-risk, high-risk, and likely dependent drinkers using measures of agreement with the 10-item Alcohol Use Disorders Identification Test. Addict. Sci. Clin. Pract. 2014, 9, 17. [Google Scholar] [CrossRef] [PubMed]
- Conigrave, K.; Freeman, B.; Caroll, T.; Simpson, L.; Lee, K.S.K.; Wade, V.; Kiel, K.; Ella, S.; Becker, K.; Freeburn, B. The Alcohol Awareness project: Community education and brief intervention in an urban Aboriginal setting. Health Promot. J. Aust. 2012, 23, 219–225. [Google Scholar]
- National Health and Medical Research Council. Australian Guidelines to Reduce Health Risks from Drinking Alcohol; National Health and Medical Research Council: Canberra, Australia, 2009.
- Etter, J.F.; Duc, T.V.; Perneger, T.V. Validity of the Fagerstrom test for nicotine dependence and of the Heaviness of Smoking Index among relatively light smokers. Addiction 1999, 94, 269–281. [Google Scholar] [CrossRef] [PubMed]
- Ali, R.; Meena, S.; Eastwood, B.; Richards, I.; Marsden, J. Ultra-rapid screening for substance-use disorders: The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST-Lite). Drug Alcohol Depend. 2013, 132, 352–361. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.X.; Adhikari, N.K.; McDonald, H.; Rosas-Arellano, M.P.; Devereaux, P.J.; Beyene, J.; Sam, J.; Haynes, R.B. Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: A systematic review. JAMA 2005, 293, 1223–1238. [Google Scholar] [CrossRef] [PubMed]
- IBM. SPSS 22.0; SPSS Inc.: Chicago, IL, USA, 2014. [Google Scholar]
- National Regional Profile: New England and North West. 2011. Available online: http://stat.abs.gov.au/itt/r.jsp?RegionSummary®ion=110&dataset=ABS_REGIONAL_ASGS&geoconcept=REGION&datasetASGS=ABS_REGIONAL_ASGS&datasetLGA=ABS_REGIONAL_LGA®ionLGA=REGION®ionASGS=REGION (accessed on 16 January 2016).
- Clifford, A.; Shakeshaft, A.; Deans, C. Training and tailored outreach support to improve alcohol screening and brief intervention in Aboriginal Community Controlled Health Services. Drug Alcohol Rev. 2013, 32, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Calabria, B.; Clifford, A.; Rose, M.; Shakeshaft, A.P. Tailoring a family-based alcohol intervention for Aboriginal Australians, and the experiences and perceptions of health care providers trained in its delivery. BMC Public Health 2014, 14, 322. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.; Darke, S.; Kelly, E.; Hetherington, K. Suicide risk assessment practices: A national survey of generalist drug and alcohol residential rehabilitation services. Drug Alcohol Rev. 2012, 31, 790–796. [Google Scholar] [CrossRef] [PubMed]
- Havard, A.; Shakeshaft, A.P.; Conigrave, K.M. Randomized controlled trial of mailed personalized feedback for risky drinkers in the emergency department: The impact on alcohol consumption, alcohol-related injuries, and repeat emergency department presentations. Alcohol. Clin. Exp. Res. 2015, 39, 1260–1266. [Google Scholar] [CrossRef] [PubMed]
- Degenhardt, L.; Larney, S.; Chan, G.; Dobbins, T.; Weier, M.; Roxburgh, A.; Hall, W.D.; McKetin, R. Estimating the number of regular and dependent methamphetamine users in Australia, 2002–2014. Med. J. Aust. 2016, 204, 153. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.S.; Dawson, A.; Conigrave, K.M. The role of an Aboriginal women’s group in meeting the high needs of clients attending outpatient alcohol and other drug treatment. Drug Alcohol Rev. 2013, 32, 618–626. [Google Scholar] [CrossRef] [PubMed]
- Fawcett, J.S.A.; Harris, M.F.; Wodak, A.; Mattick, R.P.; Richmond, R.L. Using AUDIT to classify patients into Australian Alcohol Guideline categories. Med. J. Aust. 2004, 180, 598. [Google Scholar] [PubMed]


{kind=link}
| Adapted AUDIT-C Item | Original AUDIT-C Item | Response | Score |
|---|---|---|---|
| 1. How often do you have a drink of alcohol? | How often do you have a drink containing alcohol? | Never | 0 |
| Monthly or less | 1 | ||
| 2–4 times a month | 2 | ||
| 2–3 times a week | 3 | ||
| 4 or more times a week | 4 | ||
| 2. When you have a drink of alcohol, how many drinks do you usually have? | How many standard drinks containing alcohol do you have on a typical day when drinking? | 1 or 2 | 0 |
| 3 or 4 | 1 | ||
| 5 or 6 | 2 | ||
| 7 to 9 | 3 | ||
| 10 or more | 4 | ||
| 3. How often do you have five or more drinks all in one go? | How often do you have six or more drinks on one occasion? | Never | 0 |
| Less than monthly | 1 | ||
| Monthly | 2 | ||
| Weekly | 3 | ||
| Daily or almost daily | 4 |
| Characteristics | Participants (n = 52) | ||
|---|---|---|---|
| N | Total | % | |
| Demographics | |||
| Sex: Male | 46 | 52 | 89 |
| Age (years): | |||
| 14 | 2 | 45 | 4.5 |
| 15–18 | 41 | 45 | 91 |
| 19–21 | 2 | 45 | 4.5 |
| Median (IQR) | 17 (2) | ||
| Identify as Indigenous | 23 | 47 | 49 |
| Communities of residence clustered by the service delivery site: | |||
| Community 1 (on-site program based in shed) | 17 | 52 | 33 |
| Communities 2 and 3 (outreach program) | 13 | 52 | 25 |
| Communities 4 and 5 (on-site program based on farm) | 22 | 52 | 42 |
| Risk domain 1: Education and employment | |||
| Suspended ≥3 times in past 6 months | 39 | 48 | 81 |
| Do not usually attend school | 10 | 43 | 23 |
| Unemployed | 39 | 51 | 76 |
| Receive government financial benefit | 10 | 52 | 19 |
| Risk domain 2: Mental health and wellbeing | |||
| Experienced suicide ideation in past 4 weeks | 26 | 47 | 55 |
| Experienced moderate mental distress in past 4 weeks | 28 | 51 | 55 |
| Experienced serious mental distress in past 4 weeks | 5 | 51 | 10 |
| Resilience: Mean (Median) | 24 (24) | 48 | |
| Ate fast food ≥3 times in past week | 14 | 52 | 27 |
| Do not exercise in past week | 12 | 51 | 24 |
| Last visit to health professional ≥1 year | 38 | 48 | 79 |
| Risk domain 3: Substance use | |||
| Risky drinker | 33 | 51 | 65 |
| Current smoker | 39 | 52 | 75 |
| HSI: High tobacco dependence | 9 | 51 | 18 |
| Have tried illicit substances (including cannabis) | 38 | 50 | 76 |
| At least weekly illicit substance use in past 3 months | 15 | 40 | 38 |
| Risk domain 4: Crime | |||
| Have committed a crime | 23 | 37 | 62 |
| Have been a victim of crime | 13 | 34 | 38 |
| High risk of exposure to crime in the home | 20 | 46 | 43 |
| Have been involved with the juvenile justice system | 17 | 43 | 40 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knight, A.; Havard, A.; Shakeshaft, A.; Maple, M.; Snijder, M.; Shakeshaft, B. The Feasibility of Embedding Data Collection into the Routine Service Delivery of a Multi-Component Program for High-Risk Young People. Int. J. Environ. Res. Public Health 2017, 14, 208. https://doi.org/10.3390/ijerph14020208
Knight A, Havard A, Shakeshaft A, Maple M, Snijder M, Shakeshaft B. The Feasibility of Embedding Data Collection into the Routine Service Delivery of a Multi-Component Program for High-Risk Young People. International Journal of Environmental Research and Public Health. 2017; 14(2):208. https://doi.org/10.3390/ijerph14020208
Chicago/Turabian StyleKnight, Alice, Alys Havard, Anthony Shakeshaft, Myfanwy Maple, Mieke Snijder, and Bernie Shakeshaft. 2017. "The Feasibility of Embedding Data Collection into the Routine Service Delivery of a Multi-Component Program for High-Risk Young People" International Journal of Environmental Research and Public Health 14, no. 2: 208. https://doi.org/10.3390/ijerph14020208