
The Role of Healthy Lifestyle in the Implementation of Regressing Suboptimal Health Status among College Students in China: A Nested Case-Control Study

 and
and
Abstract
:1. Background
2. Methods
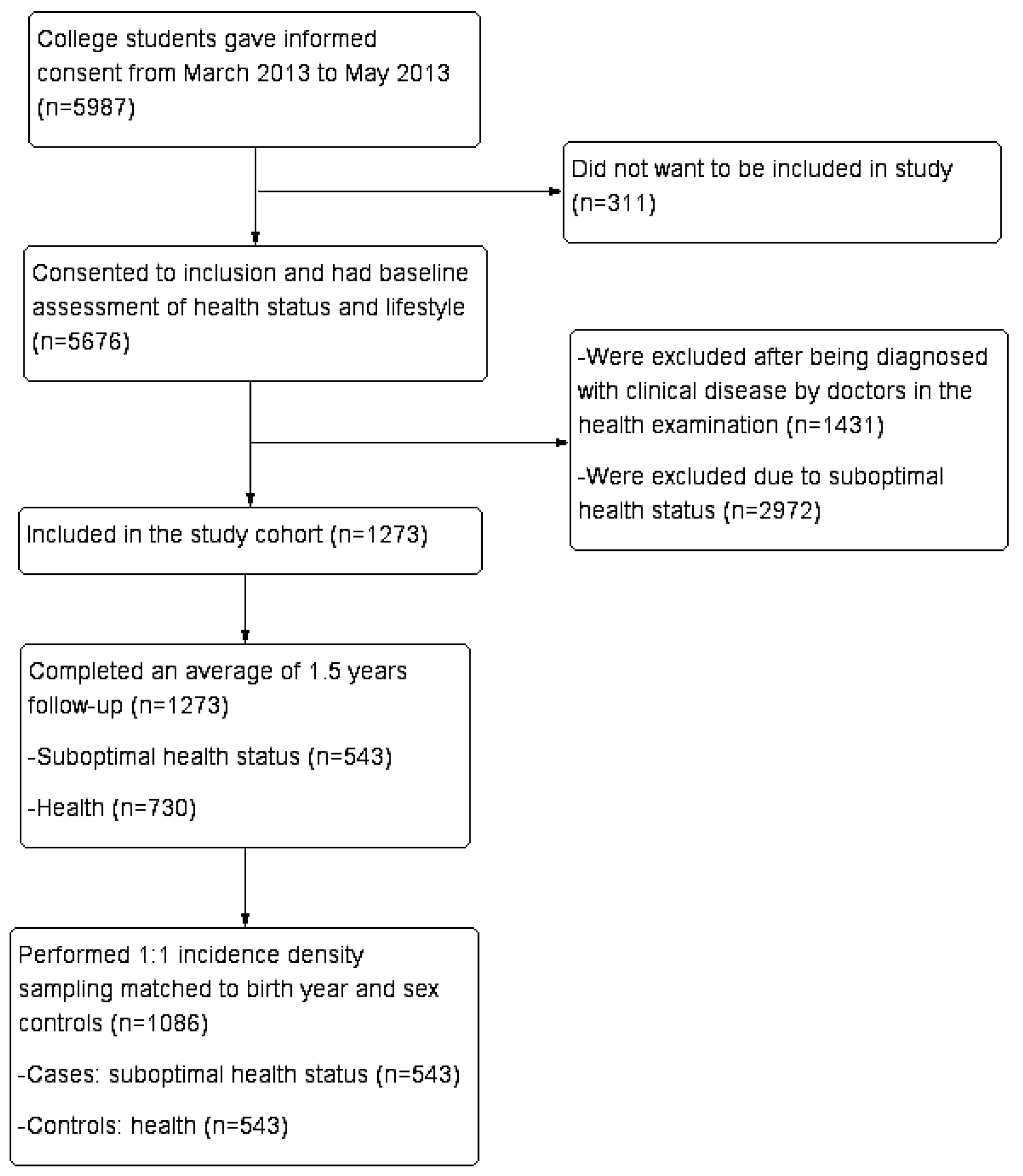
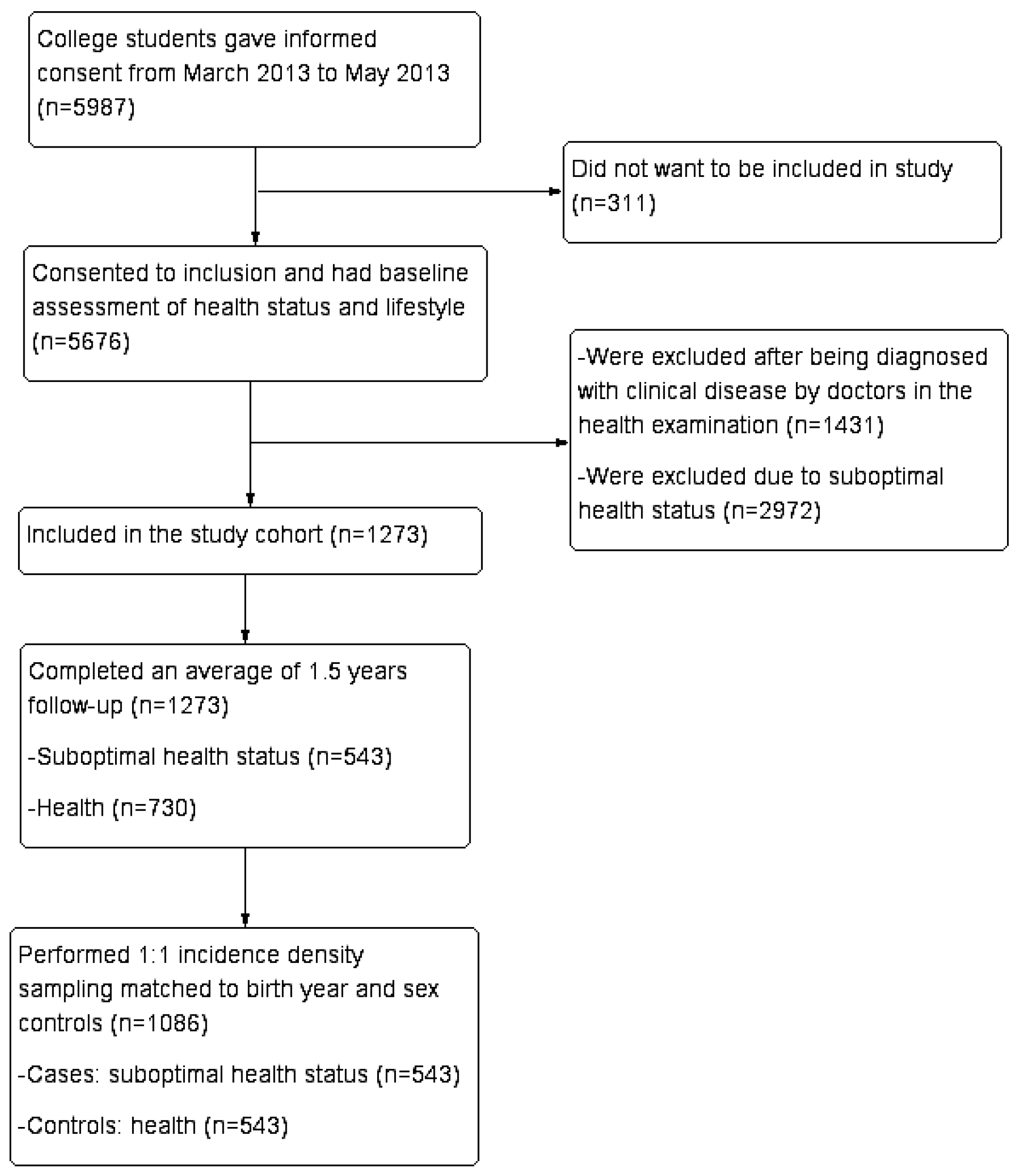
2.1. Population Cohort
2.2. Study Design
2.3. Definition and Diagnosis of Cases
2.4. Selection of Control Subjects
2.5. Exposure Assessment
2.6. Ethical Considerations
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Population Cohort and Case-Control Design
3.2. Self-Reported Discomfort Assessment by SHMS V1.0 at Baseline and at 1.5 Years Follow-Up
3.3. Health-Promoting Lifestyle Behavior Assessment by HPLP-II at Baseline and at 1.5 Years Follow-Up
3.4. Association between Unhealthy Lifestyle with SHS Risk
3.5. The Health Status Evolution among 2972 SHS Students in 1.5 Years
4. Discussion
4.1. SHS and Prevention Medicine
4.2. SHS and Unhealthy Lifestyle
4.3. Combination of Modifiable Risk Factors and the Implementation of SHS Regression
4.4. Study Strengths and Limitations
5. Conclusions
Supplementary Materials
Acknowledgements
Author Contributions
Conflicts of Interest
References
- World Health Organization. Constitution of the World Health Organization. Available online: http://www.who.int/governance/eb/who_constitution_en.pdf?ua=1 (accessed on 2 June 2015).
- Schmid, G.; Dinkel, A.; Henningsen, P.; Dieterich, M.; Hopfner, A.; Pieh, C.; Lahmann, C. Assessment of psychological aspects of somatoform disorders: A study on the German version of the Health Attitude Survey (HAS). Compr. Psychiatry 2014, 55, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Schaefert, R.; Hausteiner-Wiehle, C.; Hauser, W.; Ronel, J.; Herrmann, M.; Henningsen, P. Non-specific, functional, and somatoform bodily complaints. Dtsch. Arztebl. Int. 2012, 109, 803–813. [Google Scholar] [PubMed]
- Henningsen, P.; Zipfel, S.; Herzog, W. Management of functional somatic syndromes. Lancet 2007, 369, 946–955. [Google Scholar] [CrossRef]
- Bi, J.; Huang, Y.; Xiao, Y.; Cheng, J.; Li, F.; Wang, T.; Chen, J.; Wu, L.; Liu, Y.; Luo, R.; et al. Association of lifestyle factors and suboptimal health status: A cross-sectional study of Chinese students. BMJ Open 2014, 4, e5156. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Cheng, J.; Liu, Y.; Tang, Y.; Sun, X.; Wang, T.; Xiao, Y.; Li, F.; Xiang, L.; Jiang, P.; et al. Associations between breakfast eating habits and health-promoting lifestyle, suboptimal health status in Southern China: A population based, cross sectional study. J. Transl. Med. 2014, 12. [Google Scholar] [CrossRef] [PubMed]
- Ma, N.; Liu, M. Research progress on the epidemiology of sub-health state. China Prev. Med. 2012, 7, 556–559. [Google Scholar]
- Hilderink, P.H.; Collard, R.; Rosmalen, J.G.; Oude, V.R. Prevalence of somatoform disorders and medically unexplained symptoms in old age populations in comparison with younger age groups: A systematic review. Ageing Res. Rev. 2013, 12, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Ge, S.; Yan, Y.; Wang, A.; Zhao, Z.; Yu, X.; Qiu, J.; Alzain, M.A.; Wang, H.; Fang, H.; et al. China suboptimal health cohort study: Rationale, design and baseline characteristics. J. Transl. Med. 2016, 14, 291–302. [Google Scholar] [CrossRef] [PubMed]
- Coulter, A.; Entwistle, V.A.; Eccles, A.; Ryan, S.; Shepperd, S.; Perera, R. Personalised Care Planning for Adults with Chronic or Long-Term Health Conditions. Available online: http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD010523.pub2/pdf (accessed on 5 May 2015).
- Yan, Y.X.; Liu, Y.Q.; Li, M.; Hu, P.F.; Guo, A.M.; Yang, X.H.; Qiu, J.J.; Yang, S.S.; Shen, J.; Zhang, L.P.; et al. Development and evaluation of a questionnaire for measuring suboptimal health status in urban Chinese. J. Epidemiol. 2009, 19, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.X.; Dong, J.; Liu, Y.Q.; Yang, X.H.; Li, M.; Shia, G.; Wang, W. Association of suboptimal health status and cardiovascular risk factors in urban Chinese workers. J. Urban Health 2012, 89, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Dong, J.; Liu, Y.; Zhang, J.; Song, M.; He, Y.; Wang, W. Association of suboptimal health status with psychosocial stress, plasma cortisol and mRNA expression of glucocorticoid receptor alpha/beta in lymphocyte. Stress 2015, 18, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Kupaev, V.; Borisov, O.; Marutina, E.; Yan, Y.X.; Wang, W. Integration of suboptimal health status and endothelial dysfunction as a new aspect for risk evaluation of cardiovascular disease. EPMA J. 2016, 7, 19. [Google Scholar] [CrossRef] [PubMed]
- Medicine CAOC. The TCM Clinical Guidelines of Suboptimal Health Status; China Press of Traditional Chinese Medicine: Beijing, China, 2006. [Google Scholar]
- Xu, J.; Feng, L.Y.; Luo, R.; Qiu, J.C.; Zhang, J.H.; Zhao, X.S.; Lu, Y.; Wei, Q. Assessment of the reliability and validity of the Sub-health Measurement Scale Version1.0. J. South. Med. Univ. 2011, 31, 33–38. [Google Scholar]
- Mozaffarian, D.; Hao, T.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Changes in diet and lifestyle and long-term weight gain in women and men. N. Engl. J. Med. 2011, 364, 2392–2404. [Google Scholar] [CrossRef] [PubMed]
- Di Angelantonio, E.; Kaptoge, S.; Wormser, D.; Willeit, P.; Butterworth, A.S.; Bansal, N.; O’Keeffe, L.M.; Gao, P.; Wood, A.M.; Burgess, S.; et al. Association of Cardiometabolic Multimorbidity with Mortality. JAMA 2015, 314, 52–60. [Google Scholar] [CrossRef] [PubMed]
- O’Dowd, A. Lifestyle contributes most to distribution of cancer, report says. BMJ 2005, 331, 65. [Google Scholar] [CrossRef] [PubMed]
- Kolonel, L.N.; Altshuler, D.; Henderson, B.E. The multiethnic cohort study: Exploring genes, lifestyle and cancer risk. Nat. Rev. Cancer 2004, 4, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Reis, J.P.; Loria, C.M.; Sorlie, P.D.; Park, Y.; Hollenbeck, A.; Schatzkin, A. Lifestyle factors and risk for new-onset diabetes: A population-based cohort study. Ann. Intern. Med. 2011, 155, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Tobias, D.K.; Chavarro, J.E.; Bao, W.; Wang, D.; Ley, S.H.; Hu, F.B. Adherence to healthy lifestyle and risk of gestational diabetes mellitus: Prospective cohort study. BMJ 2014, 349, g5450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Folsom, A.R.; Yatsuya, H.; Nettleton, J.A.; Lutsey, P.L.; Cushman, M.; Rosamond, W.D. Community prevalence of ideal cardiovascular health, by the American heart association definition, and relationship with cardiovascular disease incidence. J. Am. Coll. Cardiol. 2011, 57, 1690–1696. [Google Scholar] [CrossRef] [PubMed]
- Sikorski, C.; Luppa, M.; Weyerer, S.; Konig, H.H.; Maier, W.; Schon, G.; Petersen, J.J.; Gensichen, J.; Fuchs, A.; Bickel, H.; et al. Obesity and associated lifestyle in a large sample of multi-morbid German primary care attendees. PLoS ONE 2014, 9, e102587. [Google Scholar] [CrossRef] [PubMed]
- Healy, G.N.; Wijndaele, K.; Dunstan, D.W.; Shaw, J.E.; Salmon, J.; Zimmet, P.Z.; Owen, N. Objectively measured sedentary time, physical activity, and metabolic risk: The Australian Diabetes, Obesity and Lifestyle Study (AusDiab). Diabetes Care 2008, 31, 369–371. [Google Scholar] [CrossRef] [PubMed]
- Okami, Y.; Kato, T.; Nin, G.; Harada, K.; Aoi, W.; Wada, S.; Higashi, A.; Okuyama, Y.; Takakuwa, S.; Ichikawa, H.; et al. Lifestyle and psychological factors related to irritable bowel syndrome in nursing and medical school students. J. Gastroenterol. 2011, 46, 1403–1410. [Google Scholar] [CrossRef] [PubMed]
- Sarris, J.; O’Neil, A.; Coulson, C.E.; Schweitzer, I.; Berk, M. Lifestyle medicine for depression. BMC Psychiatry 2014, 14, 107–119. [Google Scholar] [CrossRef] [PubMed]
- Peretti-Watel, P.; Legleye, S.; Baumann, M.; Choquet, M.; Falissard, B.; Chau, N. Fatigue, insomnia and nervousness: Gender disparities and roles of individual characteristics and lifestyle factors among economically active people. Soc. Psychiatry Psychiatr. Epidemiol. 2009, 44, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Moy, F.M.; Hoe, V.C.; Hairi, N.N.; Buckley, B.; Wark, P.A.; Koh, D.; Bueno-de-Mesquita, H.B.; Bulgiba, A.M. Cohort study on clustering of lifestyle risk factors and understanding its association with stress on health and wellbeing among school teachers in Malaysia (CLUSTer)––A study protocol. BMC Public Health 2014, 14, 611–619. [Google Scholar] [CrossRef] [PubMed]
- Zunhammer, M.; Eberle, H.; Eichhammer, P.; Busch, V. Somatic symptoms evoked by exam stress in university students: The role of alexithymia, neuroticism, anxiety and depression. PLoS ONE 2013, 8, e84911. [Google Scholar] [CrossRef] [PubMed]
- Van Der Windt, D.A.W.M.; Dunn, K.M.; Spies-Dorgelo, M.N.; Mallen, C.D.; Blankenstein, A.H.; Stalman, W.A.B. Impact of physical symptoms on perceived health in the community. J. Psychosom. Res. 2008, 64, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Steptoe, A.; Wardle, J.; Pollard, T.M.; Canaan, L.; Davies, G.J. Stress, social support and health-related behavior: A study of smoking, alcohol consumption and physical exercise. J. Psychosom. Res. 1996, 41, 171–180. [Google Scholar] [CrossRef]
- Arnett, J.J. Emerging adulthood: A theory of development from the late teens through the twenties. Am. Psychol. 2000, 55, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Bi, J.; Cheng, J.; Yu, B.; Xiao, Y.; Wang, T.; Li, F.; Zhao, X.; Luo, R. Formulating the assessment standard of suboptimal health measurement scale version 1.0 (SHMS V1.0) and describing the distribution of Chinese medicine constitution of suboptimal health status in Guangdong people. J. New Chin. Med. 2014, 48, 65–68. [Google Scholar]
- Mohamadian, H.; Eftekhar, H.; Rahimi, A.; Mohamad, H.T.; Shojaiezade, D.; Montazeri, A. Predicting health-related quality of life by using a health promotion model among Iranian adolescent girls: A structural equation modeling approach. Nurs. Health Sci. 2011, 13, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Pinar, R.; Celik, R.; Bahcecik, N. Reliability and construct validity of the health-promoting lifestyle profile II in an adult Turkish population. Nurs. Res. 2009, 58, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-J.; Wu, L.-J.; Xia, W.; Sun, C.; Wei, C.; Shang, T. Reliability and validity of Chinese version of the health-promoting lifestyle profile. Chin. J. Sch. Health 2007, 28, 889–891. [Google Scholar]
- Wang, W.; Russell, A.; Yan, Y. Traditional Chinese medicine and new concepts of predictive, preventive and personalized medicine in diagnosis and treatment of suboptimal health. EPMA J. 2014, 5. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Yan, Y. Suboptimal health: A new health dimension for translational medicine. Clin. Transl. Med. 2012, 1. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.M.; Zhao, X.; Wu, X.L.; Li, Y.; Yi, D.H.; Cui, H.T.; Chen, J.X. Diagnosis analysis of 4 TCM Patterns in suboptimal health status: A structural equation modelling approach. Evid. Based Complement. Alternat. Med. 2012, 2012, 970–985. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Jiang, J.; Bao, H.; Li, J.; Guo, S. Research progress in mechanism of sub-health. Chin. J. Convalesc. Med. 2010, 19, 525–526. [Google Scholar]
- Rief, W.; Broadbent, E. Explaining medically unexplained symptoms-models and mechanisms. Clin. Psychol. Rev. 2007, 27, 821–841. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, D.M. The influence of spiritual growth on adolescents’ initiative and responsibility for self-care. Pediatr. Nurs. 2005, 31, 91–95. [Google Scholar] [PubMed]
- Schmidt, H. Just health responsibility. J. Med. Ethics 2009, 35, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Feng, Q.; Zhang, Q.-L.; Du, Y.; Ye, Y.-L.; He, Q.-Q. Associations of physical activity, screen time with depression, anxiety and sleep quality among Chinese college freshmen. PLoS ONE 2014, 9, e100914. [Google Scholar] [CrossRef] [PubMed]
- Pedisic, Z.; Rakovac, M.; Titze, S.; Jurakic, D.; Oja, P. Domain-specific physical activity and health–related quality of life in university students. Eur. J. Sports Sci. 2014, 14, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Herring, M.P.; O’Connor, P.J.; Dishman, R.K. Self-esteem mediates associations of physical activity with anxiety in college women. Med. Sci. Sport Exerc. 2014, 46, 1990–1998. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, D.; Linetzky, B.; Ponce, M.; Goldberg, L.; Konfino, J.; Laspiur, S. Prevalence of overweight, obesity, physical activity and tobacco use in Argentine youth: Global school–based student health survey and global youth tobacco survey, 2007–2012. Arch. Argent Pediatr. 2014, 112, 496–503. [Google Scholar] [PubMed]
- Racette, S.B.; Deusinger, S.S.; Strube, M.J.; Highstein, G.R.; Deusinger, R.H. Changes in weight and health behaviors from freshman through senior year of college. J. Nutr. Educ. Behav. 2008, 40, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Kasparek, D.G.; Corwin, S.J.; Valois, R.F.; Sargent, R.G.; Morris, R.L. Selected health behaviors that influence college freshman weight change. J. Am. Coll. Health 2008, 56, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.S.; Kim, G.H.; Kim, J. Effectiveness of an interpersonal relationship program on interpersonal relationships, self-esteem, and depression in nursing students. J. Korean Acad. Nurs. 2011, 41, 805–813. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.; Lin, C.; Chen, C.; Chen, S.; Gwung, H. The Association between college students’ internet usage and interpersonal relationships. J. Internet Technol. 2014, 15, 671–678. [Google Scholar]
- Abdulghani, H.M.; AlKanhal, A.A.; Mahmoud, E.S.; Ponnamperuma, G.G.; Alfaris, E.A. Stress and its effects on medical students: A cross-sectional study at a college of medicine in Saudi Arabia. J. Health Popul. Nutr. 2011, 29, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Bardi, M.; Koone, T.; Mewaldt, S.; O’Connor, K. Behavioral and physiological correlates of stress related to examination performance in college chemistry students. Stress 2011, 14, 557–566. [Google Scholar] [CrossRef] [PubMed]
- Darling, C.A.; Mcwey, L.M.; Howard, S.N.; Olmstead, S.B. College student stress: The influence of interpersonal relationships on sense of coherence. Stress Health 2007, 23, 215–229. [Google Scholar] [CrossRef]
- Byrd, D.R.; McKinney, K.J. Individual, interpersonal, and institutional level factors associated with the mental health of college students. J. Am. Coll. Health 2012, 60, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Sawatzky, R.G.; Ratner, P.A.; Richardson, C.G.; Washburn, C.; Sudmant, W.; Mirwaldt, P. Stress and depression in students: The mediating role of stress management self-efficacy. Nurs. Res. 2012, 61, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Wolin, K.Y.; Yan, Y.; Colditz, G.A. Physical activity and risk of colon adenoma: A meta-analysis. Br. J. Cancer 2011, 104, 882–885. [Google Scholar] [CrossRef] [PubMed]
- Demark-Wahnefried, W.; Clipp, E.C.; Morey, M.C.; Pieper, C.F.; Sloane, R.; Snyder, D.C.; Cohen, H.J. Lifestyle intervention development study to improve physical function in older adults with cancer: Outcomes from project LEAD. J. Clin. Oncol. 2006, 24, 3465–3473. [Google Scholar] [CrossRef] [PubMed]
- De Waure, C.; Lauret, G.; Ricciardi, W.; Ferket, B.; Teijink, J.; Spronk, S.; Myriam Hunink, M.G. Lifestyle interventions in patients with coronary heart disease. Am. J. Prev. Med. 2013, 45, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Gregg, E.W.; Chen, H.; Wagenknecht, L.E.; Clark, J.M.; Delahanty, L.M.; Bantle, J.; Pownall, H.J.; Johnson, K.C.; Safford, M.M.; Kitabchi, A.E.; et al. Association of an intensive lifestyle intervention with remission of type 2 diabetes. JAMA 2012, 308, 2489–2496. [Google Scholar] [CrossRef] [PubMed]
- Wadden, T.A.; Webb, V.L.; Moran, C.H.; Bailer, B.A. Lifestyle modification for obesity: New developments in diet, physical activity, and behavior therapy. Circulation 2012, 125, 1157–1170. [Google Scholar] [CrossRef] [PubMed]
- Vinet, A.; Obert, P.; Dutheil, F.; Diagne, L.; Chapier, R.; Lesourd, B.; Courteix, D.; Walther, G. Impact of a lifestyle program on vascular insulin resistance in metabolic syndrome subjects: The resolve study. J. Clin. Endocrinol. Metab. 2015, 100, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Choi, S.W.; Lee, S.J.; Chung, W.S.; Lee, H.R.; Chung, K.Y.; Lee, E.S.; Moon, H.S.; Kim, S.H.; Sung, J.K.; et al. The effects of lifestyle modification on symptoms and quality of life in patients with irritable bowel syndrome: A prospective observational study. Gut Liver 2011, 5, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Slaman, J.; Van Den Berg-Emons, H.J.G.; Van Meeteren, J.; Twisk, J.; Van Markus, F.; Stam, H.J.; Van Der Slot, W.M.; Roebroeck, M.E. A lifestyle intervention improves fatigue, mental health and social support among adolescents and young adults with cerebral palsy: Focus on mediating effects. Clin. Rehabil. 2015, 29, 717–727. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.S.; Sze, S.L.; Woo, J.; Yu, R.H. A Chinese chan-based lifestyle intervention improves memory of older adults. Front. Aging Neurosci. 2014, 6, 50–58. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Cases (n = 543) | Controls (n = 543) | Level of Significance | |
|---|---|---|---|
| Men | 188 (34.6%) | 188 (34.6%) | - |
| Women | 355 (65.4%) | 355 (65.4%) | - |
| Mean (SD) age (years) | 18.97 (1.07) | 18.89 (1.06) | –1.28, * p = 0.200 |
| BMI | |||
| Baseline | 19.99 (2.71) | 20.21 (3.24) | 1.257, * p = 0.209 |
| Smoking status | |||
| No | 539 (99.3%) | 539 (99.3%) | 0, † p = 1.000 |
| Yes | 4 (0.7%) | 4 (0.7%) | |
| Alcohol intake | |||
| Never | 279 (51.4%) | 254 (46.8%) | 4.14, † p = 0.247 |
| Little | 220 (40.5%) | 240 (44.2%) | |
| Sometimes | 44 (8.1%) | 47 (8.7%) | |
| Often | 0 (0) | 2 (0.4%) | |
| Always | 0 (0) | 0 (0) | |
| HPLP-II | |||
| Total score (0–208) | 144.48 (18.66) | 150.22 (19.01) | 5.017, * p < 0.001 |
| Level of HPLP | Good | Good | - |
| Baseline | 1.5 Years Follow-Up | Difference | Paired t-Test | p-Value | |
|---|---|---|---|---|---|
| Cases | |||||
| SHMS V1.0 total score (0–100) | 78.60 (4.70) | 69.32 (5.45) | 9.28 (6.52) | 33.17 | <0.001 |
| Physiological dimension | 80.63 (6.51) | 74.97 (8.25) | 5.65 (8.41) | 15.68 | <0.001 |
| Physical condition | 11.56 (1.74) | 10.61 (1.94) | 0.95 (2.15) | 10.37 | <0.001 |
| Organ function | 23.82 (2.49) | 22.58 (2.94) | 1.24 (3.01) | 9.61 | <0.001 |
| Body movement function | 14.68 (0.74) | 14.25 (1.20) | 0.43 (1.25) | 7.96 | <0.001 |
| Vigour | 9.09 (0.93) | 8.55 (1.04) | 0.55 (1.21) | 10.48 | <0.001 |
| Physiological dimension | 76.15 (6.06) | 64.43 (7.92) | 11.72 (8.84) | 30.90 | <0.001 |
| Positive emotion | 17.08 (1.57) | 14.89 (2.05) | 2.19 (2.29) | 22.35 | <0.001 |
| Psychological symptoms | 23.98 (2.08) | 21.29 (2.54) | 2.68 (2.74) | 22.84 | <0.001 |
| Cognitive function | 7.49 (1.00) | 6.74 (1.05) | 0.75 (1.10) | 15.85 | <0.001 |
| Social dimension | 78.70 (6.91) | 67.05 (10.01) | 11.65 (10.83) | 25.08 | <0.001 |
| Social adjustment | 16.49 (1.40) | 14.83 (1.56) | 1.66 (1.91) | 20.26 | <0.001 |
| Social resources | 12.75 (1.52) | 10.69 (2.04) | 2.06 (2.10) | 22..87 | <0.001 |
| Social support | 8.09 (0.95) | 7.62 (1.18) | 0.48 (1.26) | 8.86 | <0.001 |
| Controls | |||||
| SHMS V1.0 total score (0–100) | 80.80 (5.40) | 80.97 (5.40) | –0.17 (6.10) | –0.67 | 0.506 |
| Physiological dimension | 82.87 (6.80) | 83.32 (6.60) | –0.45 (0.32) | –1.392 | 0.165 |
| Physical condition | 11.96 (1.79) | 11.93 (1.77) | 0.03 (1.94) | 0.35 | 0.724 |
| Organ function | 24.59 (2.42) | 24.85 (2.35) | –2.56 (2.75) | –2.17 | 0.030 |
| Body movement function | 14.68 (0.73) | 14.70 (0.69) | –0.02 (0.87) | –0.64 | 0.521 |
| Vigour | 9.18 (0.99) | 9.18 (0.99) | 0 (1.21) | –0.02 | 0.986 |
| Physiological dimension | 78.60 (6.83 ) | 78.60 (7.00) | 0 (8.09) | 0.01 | 0.996 |
| Positive emotion | 17.50 (1.62) | 17.30 (1.70) | 0.20 (2.01) | 2.28 | 0.023 |
| Psychological symptoms | 24.53 (2.27) | 24.70 (2.33) | –0.17 (2.58) | –1.54 | 0.123 |
| Cognitive function | 7.70 (1.01) | 7.73 (0.95) | –0.02 (0.99) | –0.59 | 0.557 |
| Social dimension | 80.50 (7.19) | 80.48 (7.40) | 0.02 (8.30) | 0.05 | 0.960 |
| Social adjustment | 16.77 (1.47) | 16.77 (1.47) | 0 (1.61) | 0.03 | 0.979 |
| Social resources | 12.97 (1.53) | 12.87 (1.53) | 0.10 (1.66) | 1.42 | 0.155 |
| Social support | 8.24 (0.94) | 8.34 (0.96) | –0.10 (1.12) | –2.02 | 0.044 |
| Baseline | 1.5 Years Follow-Up | Difference | Paired t-Test | p-Value | |
|---|---|---|---|---|---|
| Cases | |||||
| HPLP-II total score (0–208) | 144.48 (18.66) | 135.93 (17.65) | 8.55 (20.36) | 9.79 | <0.001 |
| Spiritual growth | 29.08 (3.92) | 26.38 (4.09) | 2.70 (4.39) | 14.32 | <0.001 |
| Health responsibility | 19.85 (4.67) | 18.16 (4.14) | 1.69 (5.01) | 7.86 | <0.001 |
| Sports and exercise | 19.46 (4.70) | 18.11 (4.67) | 1.35 (5.20) | 6.08 | <0.001 |
| Nutrition | 23.89 (4.50) | 24.56 (4.26) | −0.66 (5.10) | −3.03 | 0.003 |
| Interpersonal relationship | 28.04 (3.55) | 26.34 (3.86) | 1.69 (4.27) | 9.25 | <0.001 |
| Stress management | 24.16 (3.48) | 22.38 (3.36) | 1.78 (3.94) | 10.50 | <0.001 |
| Controls | |||||
| HPLP-II total score (0–208) | 150.22 (19.01) | 153.50 (18.42) | −3.28 (19.78) | −3.86 | <0.001 |
| Spiritual growth | 30.04 (3.85) | 30.05 (3.94) | −0.01 (4.35) | −0.06 | 0.949 |
| Health responsibility | 20.74 (5.16) | 20.39 (4.99) | 0.35 (5.48) | 1.50 | 0.136 |
| Sports and exercise | 20.25 (4.88) | 20.94 (5.04) | −0.69 (5.29) | –3.05 | <0.001 |
| Nutrition | 25.10 (4.39) | 27.13 (4.10) | −2.04 (4.82) | −9.85 | <0.001 |
| Interpersonal relationship | 28.95 (3.62) | 29.59 (3.59) | −0.64 (6.97) | −3.74 | <0.001 |
| Stress management | 25.14 (3.42) | 25.39 (3.45) | −0.25 (3.96) | −1.49 | 0.138 |
| Dependent Variables | No (%) of Controls (n = 543) | No (%) of Cases (n = 543) | OR (95% CI) | p-Value |
|---|---|---|---|---|
| Health-promoting lifestyle | ||||
| Poor | 0 | 1 | - | - |
| General | 79 | 111 | 2.333 (1.471–3.700) | <0.001 |
| Good | 378 | 377 | 1.644 (1.119–2.414) | 0.011 |
| Excellent | 86 | 54 | Reference | |
| Spiritual growth | ||||
| Poor | 0 | 1 | - | - |
| General | 14 | 15 | 1.309(0.608–2.819) | 0.491 |
| Good | 226 | 285 | 1.550(1.217–1.973) | <0.001 |
| Excellent | 303 | 242 | Reference | |
| Health responsibility | ||||
| Poor | 71 | 89 | 2.038 (1.113–3.733) | 0.021 |
| General | 303 | 335 | 1.775 (1.028–3.064) | 0.039 |
| Good | 132 | 96 | 1.148 (0.643–2.050) | 0.640 |
| Excellent | 37 | 23 | Reference | |
| Sports and exercise | ||||
| Poor | 33 | 47 | 2.337 (1.328–4.114) | 0.003 |
| General | 239 | 245 | 1.678 (1.139–2.471) | 0.009 |
| Good | 181 | 194 | 1.736 (1.168–2.579) | 0.006 |
| Excellent | 90 | 57 | Reference | |
| Nutrition | ||||
| Poor | 6 | 14 | 3.650 (1.303–10.223) | 0.014 |
| General | 146 | 197 | 2.040 (1.348–3.087) | 0.001 |
| Good | 307 | 272 | 1.289 (0.883–1.881) | 0.188 |
| Excellent | 84 | 60 | Reference | |
| Interpersonal relationship | ||||
| Poor | 0 | 1 | - | - |
| General | 18 | 27 | 2.156 (1.133–4.104) | 0.019 |
| Good | 285 | 334 | 1.599 (1.236–2.068) | <0.001 |
| Excellent | 240 | 181 | Reference | |
| Stress management | ||||
| Poor | 1 | 2 | 3.095 (0.277–34.601) | 0.359 |
| General | 22 | 37 | 2.367 (1.302–4.302) | 0.005 |
| Good | 279 | 322 | 1.547 (1.197–2.000) | 0.001 |
| Excellent | 241 | 182 | Reference | |
| Baseline | 1.5 Years Follow-Up | Difference | Paired t-Test | p-Value | |
|---|---|---|---|---|---|
| SHS→Health (n = 422) | |||||
| HPLP-II total score (0–208) | 132.72 (16.56) | 147.45 (18.76) | –14.73 (19.73) | –15.34 | <0.001 |
| Spiritual growth | 26.33 (3.99) | 28.87 (4.04) | –2.54 (4.49) | –11.631 | <0.001 |
| Health responsibility | 18.16 (3.93) | 19.71 (5.00) | –1.55 (5.39) | –5.902 | <0.001 |
| Sports and exercise | 17.42 (4.37) | 19.78 (5.14) | –2.37 (5.26) | –9.234 | <0.001 |
| Nutrition | 22.68 (4.19) | 25.94 (3.95) | –3.27 (4.68) | –14.332 | <0.001 |
| Interpersonal relationship | 25.92 (3.56) | 28.57 (3.76) | –2.66 (4.04) | –13.50 | <0.001 |
| Stress management | 22.22(3.20) | 24.57(3.28) | –2.35(3.93) | –12.282 | <0.001 |
| SHS→SHS (n = 1971) | |||||
| HPLP-II total score (0–208) | 126.00 (16.37) | 128.34 (17.52) | –2.34 (17.23) | –6.04 | <0.001 |
| Spiritual growth | 24.82 (4.36) | 24.41 (4.37) | 0.41 (4.47) | 4.07 | <0.001 |
| Health responsibility | 17.04 (3.68) | 16.80 (3.97) | 0.15 (4.19) | 1.64 | 0.101 |
| Sports and exercise | 16.52 (4.05) | 17.20 (4.53) | –0.68 (4.64) | –6.49 | <0.001 |
| Nutrition | 21.82 (4.09) | 23.72 (4.07) | –1.89 (4.60) | –18.28 | <0.001 |
| Interpersonal relationship | 24.69 (3.74) | 24.81 (3.90) | –0.11 (4.01) | –1.24 | 0.217 |
| Stress management | 21.10 (3.25) | 21.33 (3.42) | –0.22 (3.68) | –2.71 | 0.007 |
| SHS→Disease (n = 579) | |||||
| HPLP-II total score (0–208) | 126.40 (17.79) | 129.63 (18.94) | –3.23 (18.82) | –4.13 | <0.001 |
| Spiritual growth | 24.76 (4.52) | 24.63 (4.82) | 0.13 (4.79) | 0.65 | 0.516 |
| Health responsibility | 17.31 (3.82) | 17.40 (4.22) | –0.08 (4.58) | –0.44 | 0.660 |
| Sports and exercise | 16.84 (4.23) | 17.20 (4.64) | –0.35 (5.04) | –1.69 | 0.092 |
| Nutrition | 21.77 (4.33) | 24.25 (4.26) | –2.48 (4.59) | –12.98 | <0.001 |
| Interpersonal relationship | 24.74 (3.94) | 24.99( 4.42) | –0.25 (4.30) | –1.416 | 0.157 |
| Stress management | 20.97 (3.58) | 21.17(3.66) | –0.19 (3.74) | –1.25 | 0.212 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.; Xiang, H.; Jiang, P.; Yu, L.; Jing, Y.; Li, F.; Wu, S.; Fu, X.; Liu, Y.; Kwan, H.; et al. The Role of Healthy Lifestyle in the Implementation of Regressing Suboptimal Health Status among College Students in China: A Nested Case-Control Study. Int. J. Environ. Res. Public Health 2017, 14, 240. https://doi.org/10.3390/ijerph14030240
Chen J, Xiang H, Jiang P, Yu L, Jing Y, Li F, Wu S, Fu X, Liu Y, Kwan H, et al. The Role of Healthy Lifestyle in the Implementation of Regressing Suboptimal Health Status among College Students in China: A Nested Case-Control Study. International Journal of Environmental Research and Public Health. 2017; 14(3):240. https://doi.org/10.3390/ijerph14030240
Chicago/Turabian StyleChen, Jieyu, Hongjie Xiang, Pingping Jiang, Lin Yu, Yuan Jing, Fei Li, Shengwei Wu, Xiuqiong Fu, Yanyan Liu, Hiuyee Kwan, and et al. 2017. "The Role of Healthy Lifestyle in the Implementation of Regressing Suboptimal Health Status among College Students in China: A Nested Case-Control Study" International Journal of Environmental Research and Public Health 14, no. 3: 240. https://doi.org/10.3390/ijerph14030240