
Life after Stroke in an Urban Minority Population: A Photovoice Project

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Photovoice Sessions
2.3. Data Analysis
3. Results
3.1. Demographics
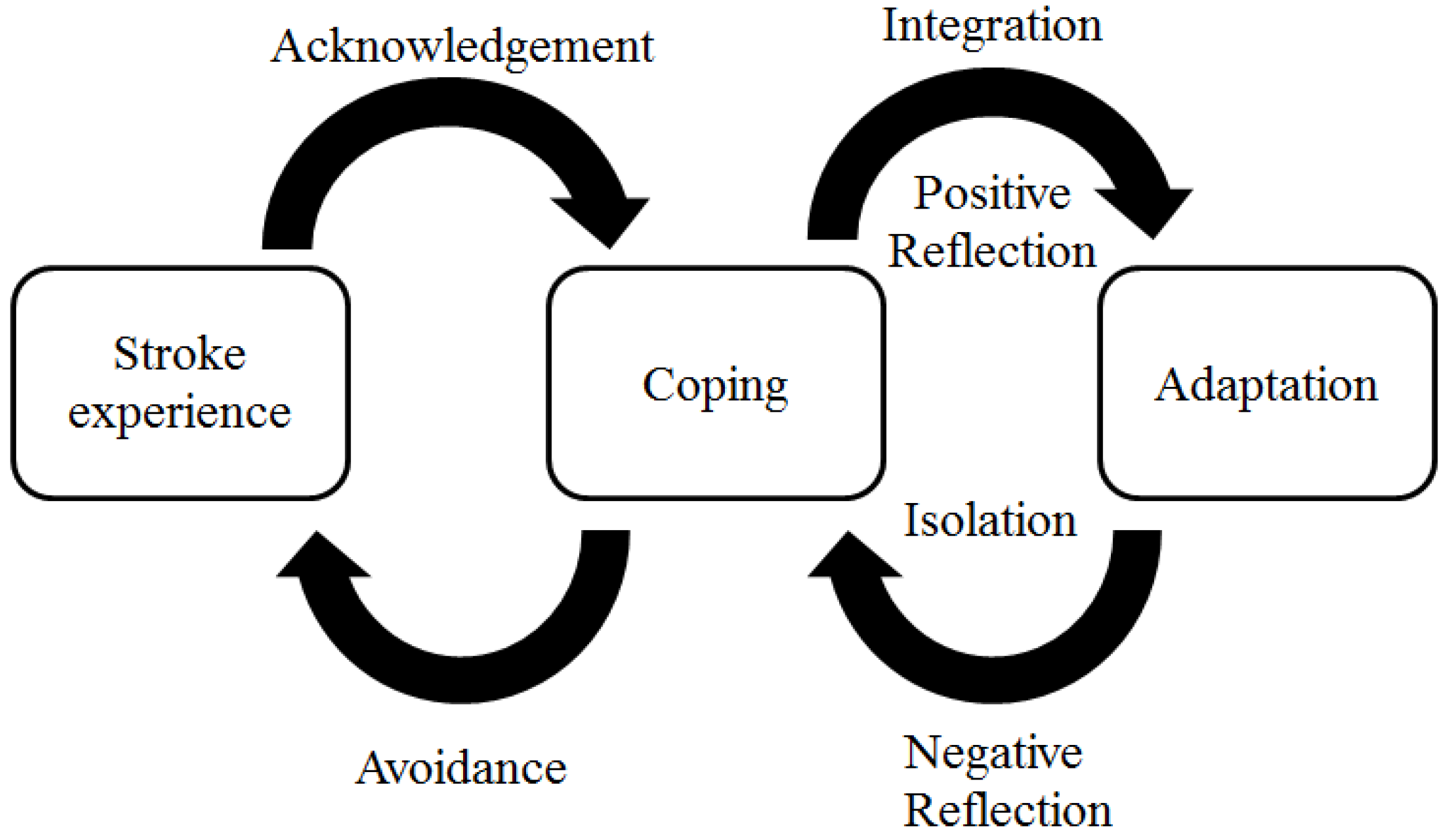
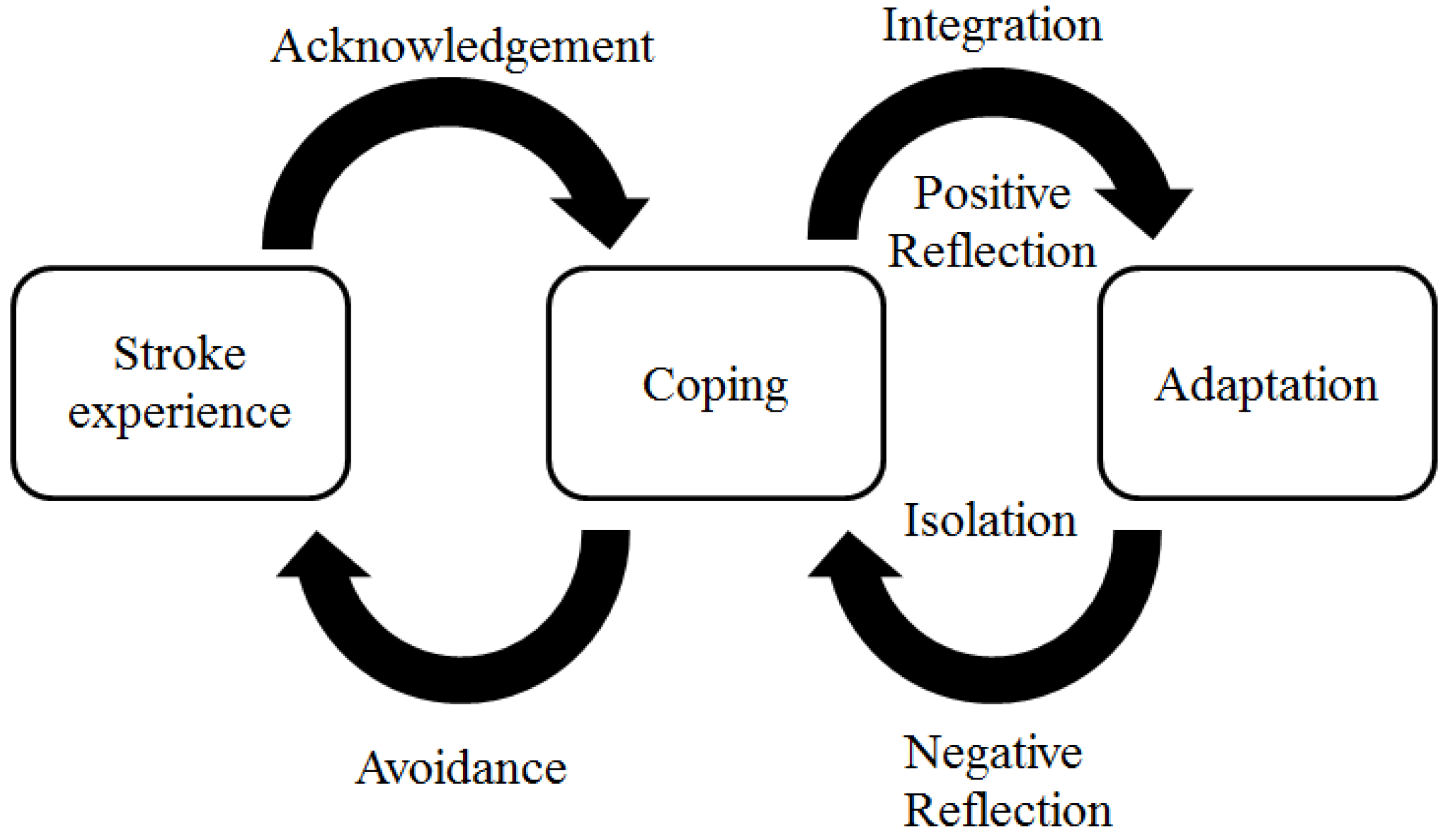
3.2. Conceptual Model of Recovery
3.2.1. Stroke Experience
“The day I came home it took me almost half an hour to get to the front door to the lobby. I was crushed. I wanted to just cry, crawl under a rock or just be somewhere there was no one... It wasn’t until then that I realized my life was over…”
3.2.2. Coping: Acknowledgement versus Avoidance
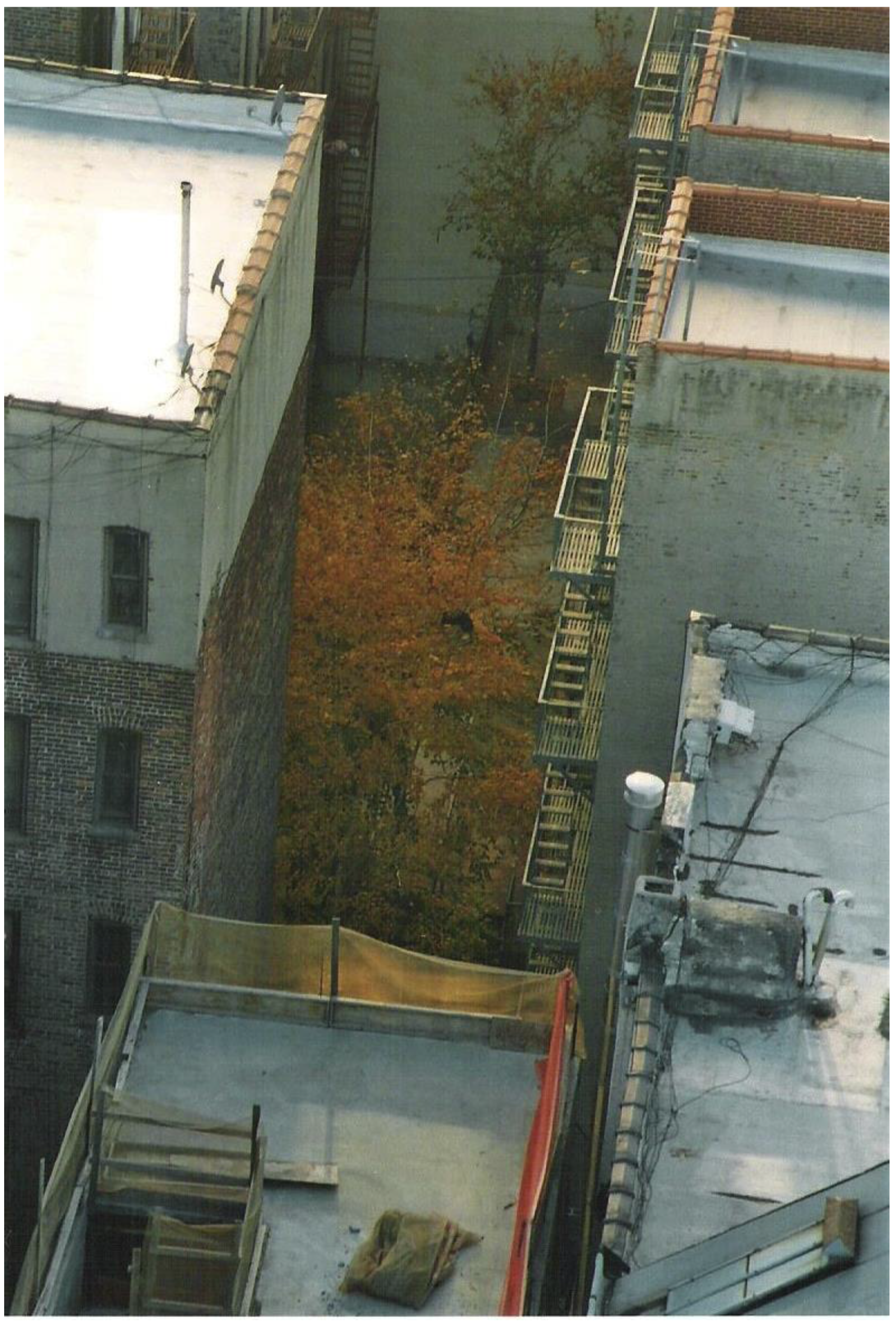
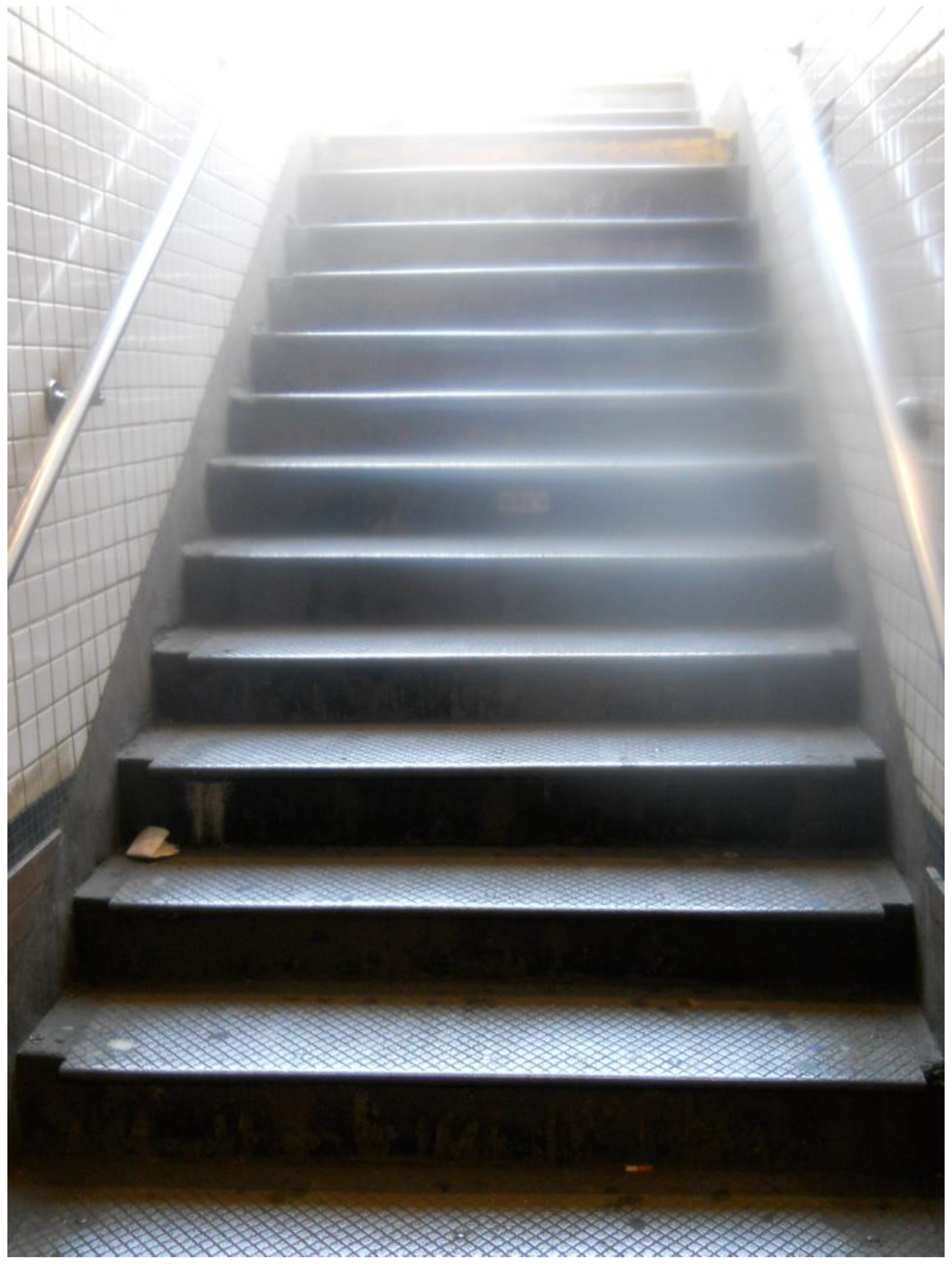
“This is an obstacle course... I found out you have to be twice as cautious and more tentative walking…and I didn’t want people to help me, I was sweatin’ bullets, but I had to take that challenge.”
“… I was helping a lot of people…because of their personality I didn’t want them to know I was sick. So I refused talking to them at all, because in my mind I felt that it was better that they be angry with me than to feel that I was sick.”
3.2.3. Reflection: Integration versus Isolation
“You know, I’m not going to be the same person and I don’t really care… I’m still who I am, I’m just a little bit awkward now… Sometimes you got to go through bad…in order [to] really appreciate who you are.”
3.2.4. Adaptation: Long-Term Changes
“[The] negative is that, that’s it for life…we got to take that forever now; we don’t give it up just cause we feel better…the pills are our life… It is a positive that you’re still alive…you are living.” (Figure 5)
“If you had issues with yourself or with not accomplishing, you can get into gardening and forget all the negativity… When I garden I talk to myself…it’s almost like you can look at yourself and see that you’re coming along, like each day you get better.”
3.2.5. Follow-Up
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Dhamoon, M.S.; Moon, Y.P.; Paik, M.C.; Boden-Albala, B.; Rundek, T.; Sacco, R.L.; Elkind, M.S. Quality of life declines after first ischemic stroke: The Northern Manhattan Study. Neurology 2010, 75, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Lynch, E.B.; Butt, Z.; Heinemann, A.; Victorson, D.; Nowinski, C.J.; Perez, L.; Cella, D. A qualitative study of quality of life after stroke: The importance of social relationships. J. Rehabil. Med. 2008, 40, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Turner, M.B. Heart disease and stroke statistics—2012 update: A report from the American Heart Association. Circulation 2012, 125, e2–e220. [Google Scholar] [PubMed]
- Wang, C.; Burris, M.A. Photovoice: Concept, methodology, and use for participatory needs assessment. Health Educ. Behav. 1997, 24, 369–387. [Google Scholar] [CrossRef] [PubMed]
- Killion, C.M.; Wang, C.C. Linking African American mothers across life stage and station through photovoice. J. Health Care Poor Underserved 2000, 11, 310–325. [Google Scholar] [CrossRef] [PubMed]
- Khanare, F. Schoolchildren affected by HIV in rural South Africa: Schools as environments that enable or limit coping. Afr. J. AIDS Res. 2012, 11, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Goldfinger, J.Z.; Kronish, I.M.; Fei, K.; Graciani, A.; Rosenfeld, P.; Lorig, K.; Horowitz, C.R. Peer education for secondary stroke prevention in inner-city minorities: Design and methods of the prevent recurrence of all inner-city strokes through education randomized controlled trial. Contemp. Clin. Trials 2012, 33, 1065–1073. [Google Scholar] [CrossRef] [PubMed]
- Kronish, I.M.; Goldfinger, J.Z.; Negron, R.; Fei, K.; Tuhrim, S.; Arniella, G.; Horowitz, C.R. Effect of peer education on stroke prevention: The prevent recurrence of all inner-city strokes through education randomized controlled trial. Stroke 2014, 45, 3330–3336. [Google Scholar] [CrossRef] [PubMed]
- Wallerstein, N.; Bernstein, E. Empowerment education: Freire’s ideas adapted to health education. Health Educ. Behav. 1988, 15, 379–394. [Google Scholar] [CrossRef]
- Strauss, A.L.; Corbin, J.M. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory; Sage Publications: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Graneheim, U.H.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.T.; Hareendran, A.; Grant, M.; Baird, T.; Schulz, U.G.R.; Muir, K.W.; Bone, I. Improving the assessment of outcomes in stroke: Use of a structured interview to assign grades on the modified Rankin scale. Stroke 2002, 33, 2243–2246. [Google Scholar] [CrossRef] [PubMed]
- Easton, K.L. The poststroke journey: From agonizing to owning. Geriatr. Nurs. 1999, 20, 70–76. [Google Scholar]
- King, R.B. Quality of life after stroke. Stroke 1996, 27, 1467–1472. [Google Scholar] [CrossRef] [PubMed]
- Salter, K.; Hellings, C.; Foley, N.; Teasell, R. The experience of living with stroke: A qualitative meta-synthesis. J. Rehabil. Med. 2008, 40, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Hammel, J.; Jones, R.; Gossett, A.; Morgan, E. Examining barriers and supports to community living and participation after a stroke from a participatory action research approach. Top. Stroke Rehabil. 2006, 13, 43–58. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, E.; Wallerstein, N.; Braithwaite, R.; Gutierrez, L.; Labonte, R.; Zimmerman, M. Empowerment forum: A dialogue between guest editorial board members. Health Educ. Q. 1994, 21, 281–294. [Google Scholar] [CrossRef] [PubMed]
- Goodsmith, L. Beyond where it started: A look at the “Healing Images” experience. Torture 2007, 17, 222–232. [Google Scholar] [PubMed]
- Hines-Martin, V.P.; Usui, W.; Kim, S.; Furr, A. A comparison of influences on attitudes towards mental health service use in an African-American and White community. J. Natl. Black Nurses Assoc. 2004, 15, 17–22. [Google Scholar] [PubMed]
- Laub, D.; Podell, D. Art and trauma. Int. J. Psychoanal. 1995, 76, 991–1005. [Google Scholar] [PubMed]
- Levin, T.; Scott, B.M.; Borders, B.; Hart, K.; Lee, J.; Decanini, A. Aphasia Talks: Photography as a means of communication, self-expression, and empowerment in persons with aphasia. Top. Stroke Rehabil. 2007, 14, 72–84. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Burris, M.A. Empowerment through photo novella: Portraits of participation. Health Educ. Q. 1994, 21, 171–186. [Google Scholar] [CrossRef] [PubMed]
- Lykes, M.B.; Blanche, M.T.; Hamber, B. Narrating survival and change in Guatemala and South Africa: The politics of representation and a liberatory community psychology. Am. J. Commun. Psychol. 2003, 31, 79–90. [Google Scholar] [CrossRef]
- Goldfinger, J.Z.; Edmondson, D.; Kronish, I.M.; Fei, K.; Balakrishnan, R.; Tuhrim, S.; Horowitz, C.R. Correlates of post-traumatic stress disorder in stroke survivors. J. Stroke Cerebrovasc. Dis. 2014, 23, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- Kronish, I.M.; Edmondson, D.; Goldfinger, J.Z.; Fei, K.; Horowitz, C.R. Posttraumatic stress disorder and adherence to medications in survivors of strokes and transient ischemic attacks. Stroke 2012, 43, 2192–2197. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean (SD) | |
| Age, years | 64 (10) |
| Time since last stroke or TIA, years | 2.0 (1.5) |
| Number (%) | |
| Female | 11 (65) |
| Race/Ethnicity | |
| Black/African American | 11 (65) |
| Hispanic/Latino | 2 (12) |
| White or Other | 4 (23) |
| Income (≤15,000) | 7 (41) |
| Modified Rankin Score | |
| 0–2 | 10 (59) |
| 3–4 | 7 (41) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balakrishnan, R.; Kaplan, B.; Negron, R.; Fei, K.; Goldfinger, J.Z.; Horowitz, C.R. Life after Stroke in an Urban Minority Population: A Photovoice Project. Int. J. Environ. Res. Public Health 2017, 14, 293. https://doi.org/10.3390/ijerph14030293
Balakrishnan R, Kaplan B, Negron R, Fei K, Goldfinger JZ, Horowitz CR. Life after Stroke in an Urban Minority Population: A Photovoice Project. International Journal of Environmental Research and Public Health. 2017; 14(3):293. https://doi.org/10.3390/ijerph14030293
Chicago/Turabian StyleBalakrishnan, Revathi, Benjamin Kaplan, Rennie Negron, Kezhen Fei, Judith Z. Goldfinger, and Carol R. Horowitz. 2017. "Life after Stroke in an Urban Minority Population: A Photovoice Project" International Journal of Environmental Research and Public Health 14, no. 3: 293. https://doi.org/10.3390/ijerph14030293