
Effects of Forest Therapy on Depressive Symptoms among Adults: A Systematic Review


 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. Selection Criteria
2.3. Data Extraction
2.4. Quality Assessment Tool
3. Results
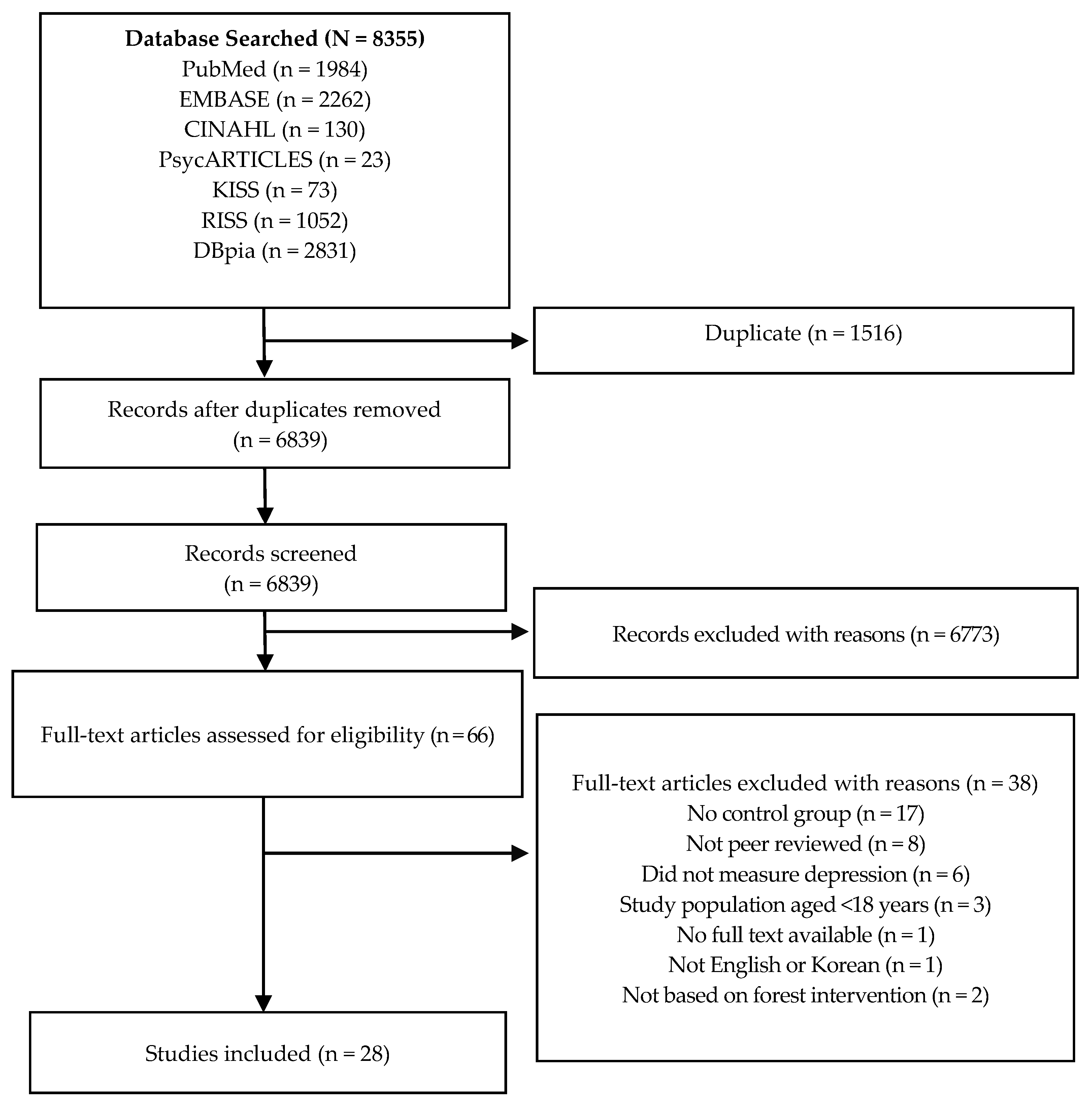
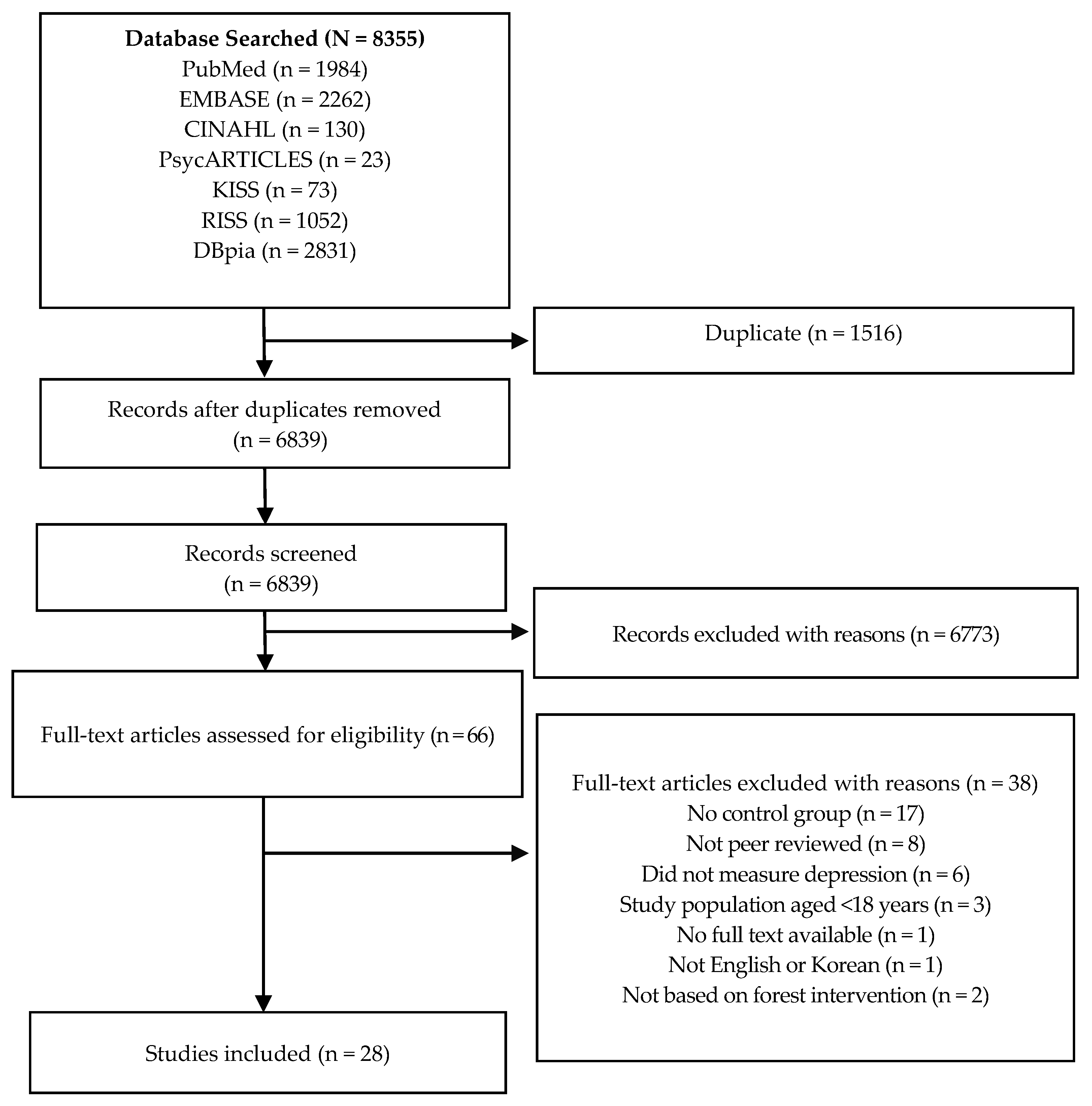
3.1. Study Identification and Selection
3.2. Study Characteristics
3.2.1. Format and Content of Forest Therapy
3.2.2. Depression Measures
3.2.3. Effects of Forest Therapy on Depression
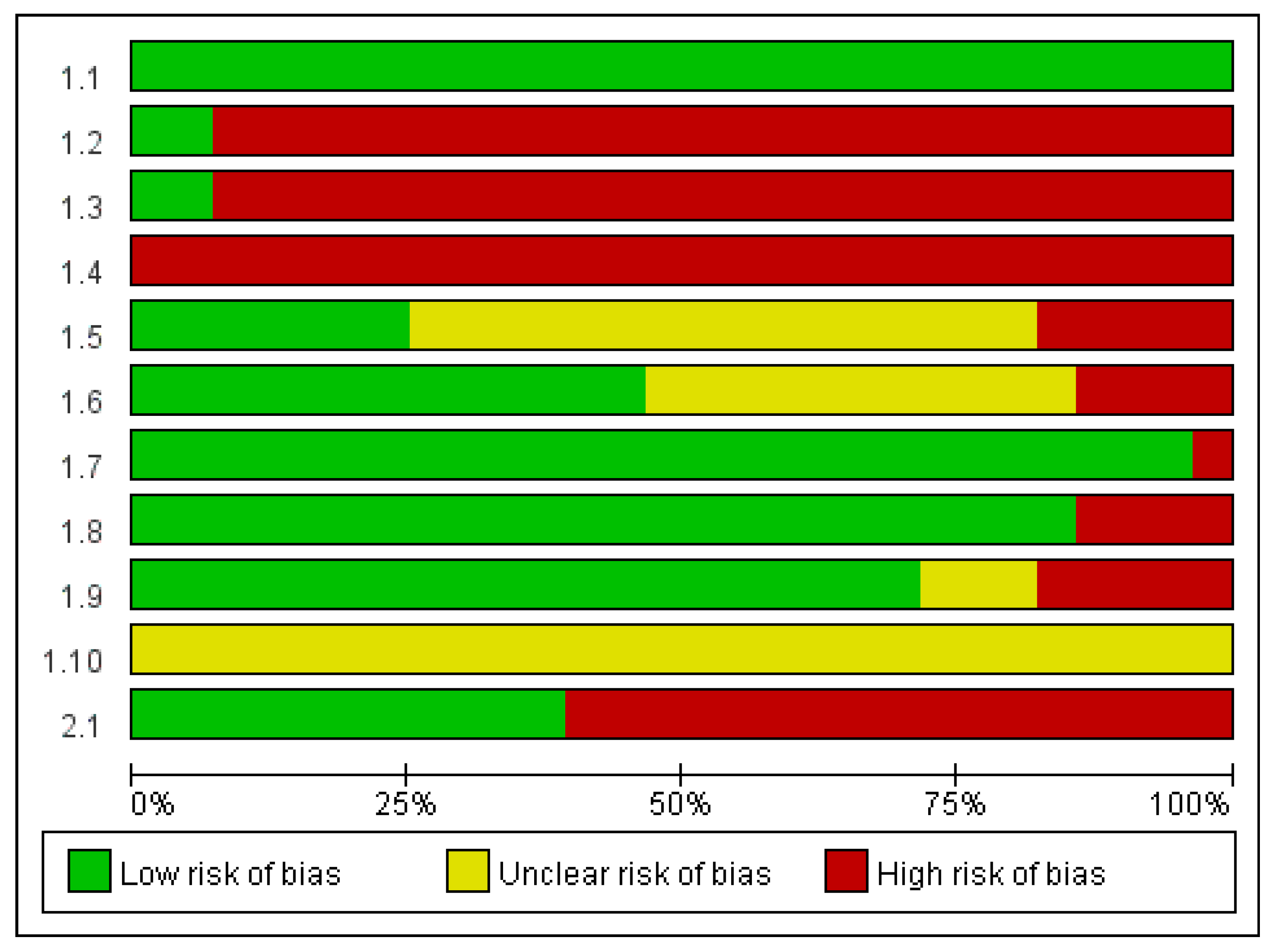
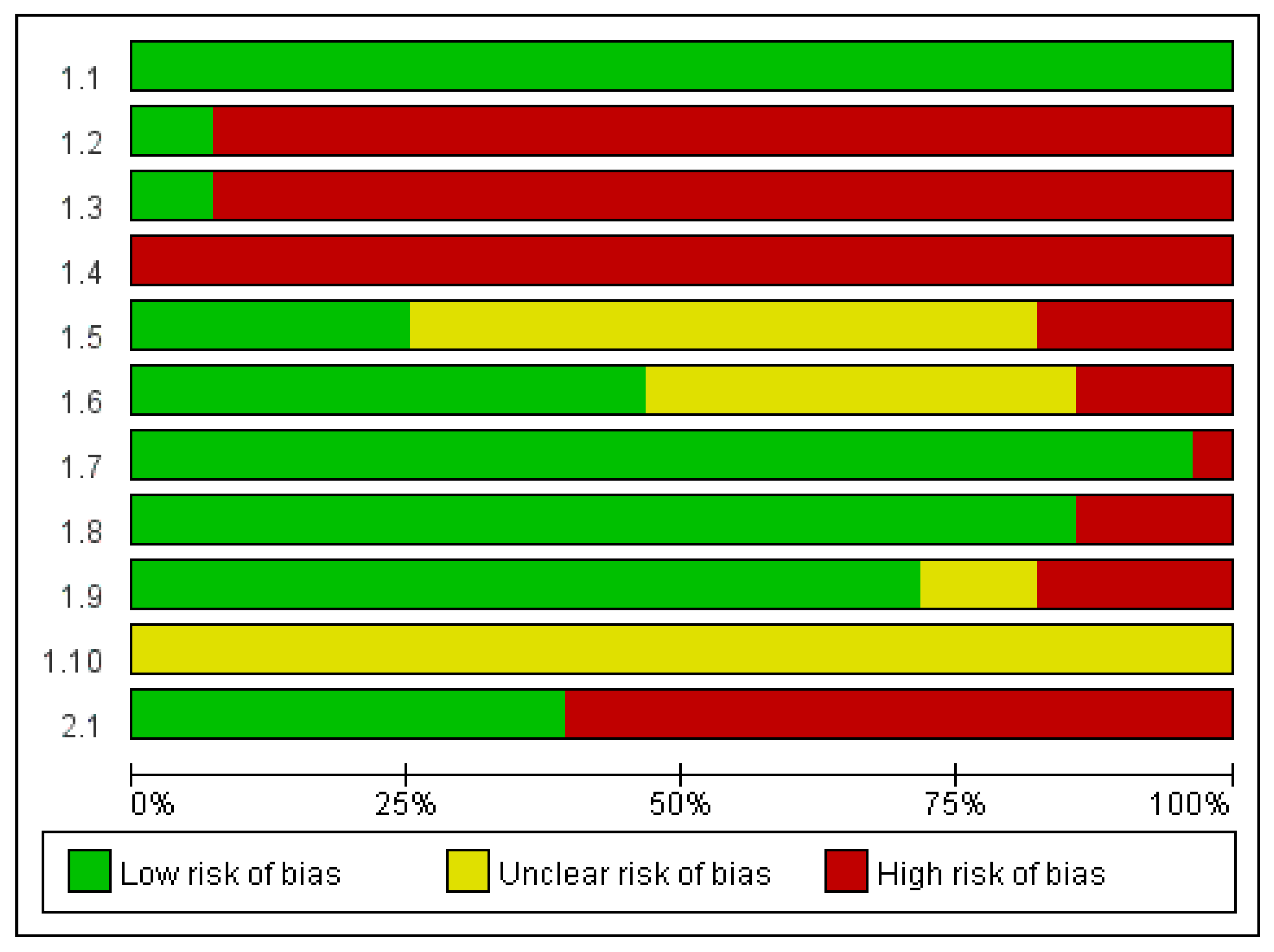
3.3. Quality Assessment
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Forest Therapy and Depression |
|---|
| Intervention |
|
| Outcome |
|
| Combined terms |
|
References
- Li, Q. What Is Forest Medicine? In Forest Medicine; Nova Science Publisher: New York, NY, USA, 2013; pp. 3–10. [Google Scholar]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Hirano, H.; Kagawa, T.; Sato, M.; Miyazaki, Y. Physiological effects of shinrin-yoku (taking in the atmosphere of the forest)—Using salivary cortisol and cerebral activity as indicators. J. Physiol. Anthropol. 2007, 26, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, U.; Fahlvik, N.; Johansson, U.; Lundström, A.; Rosvall, O. Simulation of the effect of intensive forest management on forest production in sweden. Forests 2011, 2, 373–393. [Google Scholar] [CrossRef]
- Berman, M.G.; Jonides, J.; Kaplan, S. The cognitive benefits of interacting with nature. Psychol. Sci. 2008, 19, 1207–1212. [Google Scholar] [CrossRef] [PubMed]
- Peen, J.; Schoevers, R.; Beekman, A.; Dekker, J. The current status of urban-rural differences in psychiatric disorders. Acta Psychiatr. Scand. 2010, 121, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Van Den Berg, A.E.; Maas, J.; Verheij, R.A.; Groenewegen, P.P. Green space as a buffer between stressful life events and health. Soc. Sci. Med. 2010, 70, 1203–1210. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Kobayashi, M.; Wakayama, Y. Effect of Forest Environments on Psychological Response Evaluated by the Poms Test. In Forest Medicine; Li, Q., Ed.; Nova Science Publisher: New York, NY, USA, 2013; pp. 137–146. [Google Scholar]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions the Cochrane Collaboration: 2011. Available online: www.handbook.cochrane.org (accessed on 1 December 2016).
- Crombie, I.K.; Davies, H.T. What Is Meta-Analysis. Available online: http://epu.ucc.ie/greid/PL1025-PL1011-EH1008/Lectures/Term_2/DH_small_group_sessions/Fluoride/Meta-An.pdf (accessed on 1 December 2016).
- World Health Organization. Depression Fact Sheet n 369. Available online: http://www.who.int/mediacentre/factsheets/fs369/en/# (accessed on 1 December 2016).
- Petrie, J.; Grimshaw, J.; Bryson, A. The Scottish intercollegiate guidelines network initiative: Getting validated guidelines into local practice. Health Bull. 1995, 53, 345–348. [Google Scholar]
- Barton, J.; Griffin, M.; Pretty, J. Exercise-, nature- and socially interactive-based initiatives improve mood and self-esteem in the clinical population. Perspect. Public Health 2012, 132, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.S.; Kim, H.C.; Cho, S.H. The effects of forests healing for cognitive function. J. Orient. Neuropsychiatry 2013, 24, 63–74. [Google Scholar] [CrossRef]
- Hong, S.S.; Lee, J.E.; Kim, H.C.; Cho, S.H. The effects of forests healing for hwa-byung. J. Orient. Neuropsychiatry 2012, 23, 169–182. [Google Scholar] [CrossRef]
- Kim, M.H.; Shim, B.S.; Wi, A.J.; Yoon, B.S.; Han, Y.H.; Oh, E.M.; An, K.W. The influence of forest experience program on physiological and psychological states in psychiatric inpatients. J. Korean For. Soc. 2015, 104, 133–139. [Google Scholar] [CrossRef]
- Shin, W.S.; Shin, C.S.; Yeoun, P.S. The influence of forest therapy camp on depression in alcoholics. Environ. Health Prev. Med. 2012, 17, 73–76. [Google Scholar] [CrossRef]
- Woo, J.M.; Park, S.M.; Lim, S.K.; Kim, W. Synergistic effect of forest environment and therapeutic program for the treatment of depression. J. Korean For. Soc. 2012, 101, 677–685. [Google Scholar]
- Bang, K.S.; Lee, I.S.; Kim, S.J.; Song, M.K.; Park, S.E. The effects of urban forest-walking program on health promotion behavior, physical health, depression, and quality of life: A randomized controlled trial of office-workers. J. Korean Acad. Nurs. 2016, 46, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Mao, G.X.; Lan, X.G.; Cao, Y.B.; Chen, Z.M.; He, Z.H.; Lv, Y.D.; Wang, Y.Z.; Hu, X.L.; Wang, G.F.; Yan, J. Effects of short-term forest bathing on human health in a broad-leaved evergreen forest in Zhejiang province, China. Biomed. Environ. Sci. 2012, 25, 317–324. [Google Scholar] [PubMed]
- Chun, M.H.; Chang, M.C.; Lee, S.J. The effects of forest therapy on depression and anxiety in patients with chronic stroke. Int. J. Neurosci. 2017, 127, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Jia, B.B.; Yang, Z.X.; Mao, G.X.; Lyu, Y.D.; Wen, X.L.; Xu, W.H.; Lyu, X.L.; Cao, Y.B.; Wang, G.F. Health effect of forest bathing trip on elderly patients with chronic obstructive pulmonary diseas. Biomed. Environ. Sci. 2016, 29, 212–218. [Google Scholar] [PubMed]
- Mao, G.X.; Cao, Y.B.; Lan, X.G.; He, Z.H.; Chen, Z.M.; Wang, Y.Z.; Hu, X.L.; Lv, Y.D.; Wang, G.F.; Yan, J. Therapeutic effect of forest bathing on human hypertension in the elderly. J. Cardiol. 2012, 60, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Song, C.; Lee, J.; Ikei, H.; Kagawa, T.; Miyazaki, Y.; Park, B.-J. Physiological and psychological effects of walking around and viewing a lake in a forest environment. J. Korean For. Soc. 2015, 104, 140–149. [Google Scholar] [CrossRef]
- Han, J.W.; Choi, H.; Jeon, Y.H.; Yoon, C.H.; Woo, J.M.; Kim, W. The effects of forest therapy on coping with chronic widespread pain: Physiological and psychological differences between participants in a forest therapy program and a control group. Int. J. Environ. Res. Public Health 2016, 13, 255. [Google Scholar] [CrossRef] [PubMed]
- Horiuchi, M.; Endo, J.; Takayama, N.; Murase, K.; Nishiyama, N.; Saito, H.; Fujiwara, A. Impact of viewing vs. Not viewing a real forest on physiological and psychological responses in the same setting. Int. J. Environ. Res. Public Health 2014, 11, 10883–10901. [Google Scholar] [CrossRef] [PubMed]
- Ji, G.B.; Kim, K.N.; Han, G.S. Physiological and psychological effects of viewing and walking in forest and urban area. J. Environ. Sci. Int. 2012, 21, 605–611. [Google Scholar] [CrossRef]
- Kim, K.M.; Shin, W.S.; Park, B.J.; Oh, D.K. The psychological relaxation effects on forest space type. J. KIFR 2012, 16, 87–92. [Google Scholar]
- Lee, J.; Park, B.J.; Tsunetsugu, Y.; Ohira, T.; Kagawa, T.; Miyazaki, Y. Effect of forest bathing on physiological and psychological responses in young Japanese male subjects. Public Health 2011, 125, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Tsunetsugu, Y.; Takayama, N.; Park, B.J.; Li, Q.; Song, C.; Komatsu, M.; Ikei, H.; Tyrväinen, L.; Kagawa, T.; et al. Influence of forest therapy on cardiovascular relaxation in young adults. Evid.-Based Complement. Altern. Med. 2014, 2014, 834360. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.S.; Kim, D.J.; Yeoun, P.S. Changes in depression degree and self-esteem of senior citizens in a nursing home according to forest therapy program. J. KIFR 2014, 18, 1–11. [Google Scholar]
- Shin, W.S.; Oh, H.K. The influence of the forest program on depression level. J. Korean For. Soc. 1996, 85, 586–594. [Google Scholar]
- Song, C.R.; Lee, J.Y.; Park, B.J.; Lee, M.S.; Matsuba, N.; Miyazaki, Y. Psychological effects of walking in the urban forests: Results of field tests in Shinjuku-Gyoen, Japan. J. Korean For. Soc. 2011, 100, 344–351. [Google Scholar]
- Song, J.; Cha, J.; Lee, C.; Choi, Y.; Yeoun, P. Effects of forest healing program on stress response and spirituality in female nursing college students and there experience. J. KIFR 2014, 18, 109–125. [Google Scholar]
- Takayama, N.; Korpela, K.; Lee, J.; Morikawa, T.; Tsunetsugu, Y.; Park, B.J.; Li, Q.; Tyrväinen, L.; Miyazaki, Y.; Kagawa, T. Emotional, restorative and vitalizing effects of forest and urban environments at four sites in Japan. Int. J. Environ. Res. Public Health 2014, 11, 7207–7230. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.S.; Cha, J.G.; Kim, J.A.; Hong, S.J.; Choi, Y.S. The effects of forest therapy program on spiritual health, self esteem depression and forest effectiveness in alcoholics’ families. J. Korean Alcohol. Sci. 2011, 12, 45–59. [Google Scholar]
- You, Y.S.; Lee, C.J.; Jan, N.C.; Son, B.K. A study of effects of sallimyok (forest therapy)-based mental health program on the depression the psychological stability. J. Korean Soc. Sch. Comm. Health Educ. 2014, 15, 55–65. [Google Scholar]
- Choi, Y.H.; Ha, Y.S. The effectiveness of a forest-experience-integration intervention for community dwelling cancer patients’ depression and resilience. J. Korean Acad. Community Health Nurs. 2014, 25, 109–118. [Google Scholar] [CrossRef]
- Kim, Y.G.; Lee, S.H.; Kim, Y.H.; Eum, J.O.; Yim, Y.R.; Ha, T.G.; Shin, C.S. The influence of forest activity intervention on anxiety, depression, profile of mood states (POMS) and hope of cancer patients. J. KIFR 2015, 19, 65–74. [Google Scholar]
- Song, C.; Ikei, H.; Kobayashi, M.; Miura, T.; Taue, M.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; Miyazaki, Y. Effect of forest walking on autonomic nervous system activity in middle-aged hypertensive individuals: A pilot study. Int. J. Environ. Res. Public Health 2015, 12, 2687–2699. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.; Kim, S.; Bang, K.-S.; Choi, H.; Ko, C.; Jieun, K.; Sunyoung, K. An analysis of health promotion programs utilizing forests based on Korea’s regional healthcare program plans. Perspect. Nurs. Sci. 2014, 11, 10–17. [Google Scholar] [CrossRef]
- Stigsdotter, U.K.; Palsdottir, A.M.; Burls, A.; Chermaz, A.; Ferrini, F.; Grahn, P. Nature-based therapeutic interventions. In Forests, Trees and Human Health; Nilsson, K., Sangster, M., Gallis, C., Hartig, T., Vries, S.D., Seeland, K., Schipperijn, J., Eds.; Springer: New York, NY, USA, 2011; pp. 309–342. [Google Scholar]
- Brunoni, A.R. Ceiling effects in the “effectiveness of adjunctive antidepressant treatment for bipolar depression” study: Was the sky the limit? Rev. Bras. Psiquiatr. 2011, 33, 102–103. [Google Scholar] [CrossRef] [PubMed]
- Velengtas, P.; Mohr, P.; Messner, D.A. Making Informed Decisions: Assessing the Strengths and Weaknesses of Study Designs and Analytic Methods for Comparative Effectiveness Research. National Pharmaceutical Council, 2012. Available online: http://www.ebmnow.org (accessed on 25 January 2017).
- Charness, G.; Gneezy, U.; Kuhn, M.A. Experimental methods: Between-subject and within-subject design. J. Econ. Behav. Organ. 2012, 81, 1–8. [Google Scholar] [CrossRef]
- Grove, S.K.; Burns, N.; Gray, J. The Practice of Nursing Research: Appraisal, Synthesis, and Generation of Evidence, 7th ed.; Elsevier Health Sciences: St. Louis, MO, USA, 2012. [Google Scholar]
- Polit, D.F.; Beck, C.T. Nursing Research: Generating and Assessing Evidence for Nursing Practice, 9th ed.; Wolters Kluwer Health: Philadelphia, PA, USA, 2008. [Google Scholar]
- Blackhart, G.C.; Minnix, J.A.; Kline, J.P. Can eeg asymmetry patterns predict future development of anxiety and depression? A preliminary study. Biol. Psychol. 2006, 72, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Thibodeau, R.; Jorgensen, R.S.; Kim, S. Depression, anxiety, and resting frontal eeg asymmetry: A meta-analytic review. J. Abnorm. Psychol. 2006, 115, 715–729. [Google Scholar] [CrossRef] [PubMed]
- Friedman, B.H.; Thayer, J.F. Autonomic balance revisited: Panic anxiety and heart rate variability. J. Psychosom. Res. 1998, 44, 133–151. [Google Scholar] [CrossRef]
- Kim, G.M.; Woo, J.M. Determinants for heart rate variability in a normal Korean population. J. Korean Med. Sci. 2011, 26, 1293–1298. [Google Scholar] [CrossRef] [PubMed]
- Kemp, A.H.; Quintana, D.S.; Felmingham, K.L.; Matthews, S.; Jelinek, H.F. Depression, comorbid anxiety disorders, and heart rate variability in physically healthy, unmedicated patients: Implications for cardiovascular risk. PLoS ONE 2012, 7, e30777. [Google Scholar] [CrossRef] [PubMed]
- Stein, P.K.; Carney, R.M.; Freedland, K.E.; Skala, J.A.; Jaffe, A.S.; Kleiger, R.E.; Rottman, J.N. Severe depression is associated with markedly reduced heart rate variability in patients with stable coronary heart disease. J. Psychosom. Res. 2000, 48, 493–500. [Google Scholar] [CrossRef]
- Levy, S.; Herberman, R.; Lippman, M.; D’Angelo, T. Correlation of stress factors with sustained depression of natural killer cell activity and predicted prognosis in patients with breast cancer. J. Clin. Oncol. 1987, 5, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Gleeson, M. The effect of single and repeated bouts of prolonged cycling and circadian variation on saliva flow rate, immunoglobulin a and-amylase responses. J. Sports Sci. 2004, 22, 1015–1024. [Google Scholar] [CrossRef] [PubMed]
- Skosnik, P.D.; Chatterton, R.T.; Swisher, T.; Park, S. Modulation of attentional inhibition by norepinephrine and cortisol after psychological stress. Int. J. Psychophysiol. 2000, 36, 59–68. [Google Scholar] [CrossRef]
- Park, B.J.; Tsunetsugu, Y.; Lee, J.; Ishii, H.; Kagawa, T.; Miyazaki, Y. Effect of the forest environment on physiological relaxation using the results of field tests at 35 throughout japan. In Forest Medicine; Li, Q., Ed.; Nova Science Publisher: New York, NY, USA, 2013; pp. 57–67. [Google Scholar]
- Li, Q.; Kobayashi, M.; Kawada, T. Carbamate pesticide-induced apoptosis and necrosis in human natural killer cells. J. Biol. Regul. Homeost. Agents 2013, 28, 23–32. [Google Scholar]
- Olbrich, S.; Arns, M. Eeg biomarkers in major depressive disorder: Discriminative power and prediction of treatment response. Int. Rev. Psychiatry 2013, 25, 604–6189. [Google Scholar] [CrossRef] [PubMed]
| Variables | Categories | N (%) |
|---|---|---|
| Participants | Healthy adults Adults with health problems | 16 (57.1) 12 (42.9) |
| Publication year | ≤2000 2001–2011 2012–2016 | 1 (3.6) 3 (10.7) 24 (85.7) |
| Country | Republic of Korea Japan China United Kingdom | 17 (60.7) 7 (25.0) 3 (10.7) 1 (3.6) |
| Study Design | Randomized control trial design Non-equivalent control group design Crossover trial design | 6 (21.4) 11 (39.3) 11 (39.3) |
| Sample size | ≤20 21–50 51–100 >100 | 12 (42.9) 6 (21.4) 10 (35.7) 0 (0) |
| Setting | Community Hospital University Unknown | 8 (28.6) 5 (17.9) 9 (32.1) 6 (21.4) |
| Ethical consideration | Yes No | 20 (71.4) 8 (28.6) |
| Authors (Year) | Country | Research Design | Participants (N) | Intervention(s) | Control | Measurements | Outcomes | ||
|---|---|---|---|---|---|---|---|---|---|
| Exp. | Cont. | ||||||||
| Self-Report Measures | Physiological Measures | ||||||||
| Bang (2016) [18] | Republic of Korea | RCT | Office workers (n = 45) | Urban forest-walking program—Twice a week for five weeks—Urban forest walking (40 min) and Rest (10 min) | Normal daily routines | Health-Promoting Lifestyle Profile (HPLP) II Beck Depression Inventory (BDI) General Health Questionnaire/Quality of life (GHQ/QL-12) | Blood pressure (BP) | Physical activity level * Health-Promoting behavior * Depression Quality of life * | |
| n = 18 | n = 27 | ||||||||
| BP | |||||||||
| Han (2016) [24] | Republic of Korea | Non-equivalent control group design | Full-time employees from a public organization (61) | 2-day forest therapy camp † | Normal daily routines | BDI The Euro Qol Visual Analog Scale (EQ-VAS) | Heart Rate Variability (HRV) Natural Killer Cell (NK cell) | Self-rated health condition Depression * Ani EQ-VAS * | |
| HRV NK cell * | |||||||||
| n = 33 | n = 28 | ||||||||
| Horiuchi (2014) [25] | Japan | Crossover trial | Healthy adults (n = 15) | Viewing the forest while seated on a comfortable chair for 15 min—Switched sites with 30 min interval | Conducted same activity in an enclosed condition | Profile of Mood States (POMS) | BP HRV Salivary Amylase (sAMY) | Tension-anxiety * Depression * Anger-hostility Fatigue * Confusion * Vigor | |
| n = 15 | |||||||||
| BP * HR *, HF *, LF/HF * Salivary Amylase | |||||||||
| Ji (2012) [26] | Republic of Korea | Crossover trial | Healthy male adult (n = 12) | Viewing (15 min) and walking (25 min) in the forest—Switched sites with 24 h. interval | Conducted same activities in the urban | POMS | BP HR Amylase concentration | Tension-Anxiety * Depression * Anger-hostility * Fatigue * Confusion * Vigor | |
| n = 12 | |||||||||
| BP * HR * Amylase concentration * | |||||||||
| Kim (2012) [27] | Republic of Korea | Crossover trial | Healthy students (n = 50) | Forest healing program—Viewing (15 min) and walking (15 min) in a forest park landscape—Switched sites with 24 h. interval | Conducted same activities in the urban forest | POMS Semantic Differential (SD) method | None | Tension-anxiety Depression Anger-hostility * Fatigue Confusion * Vigor * Total moods disturbance * Emotion (Pleasant *, Natural *) | |
| n = 50 | |||||||||
| Lee (2011) [28] | Japan | Crossover trial | Healthy students (n = 12) | Forest bathing—Viewing the forest (15 min)—Switched sites with 24 h. interval | Conducted same activity in the urban | POMS SD method | HRV Salivary Cortisol Pulse Rate (PR) BP | Emotion * Tension-anxiety * Depression Anger-hostility Fatigue * Confusion * Vigor * Total moods disturbance * | |
| n = 12 | |||||||||
| Parasympathetic nervous activity * Sympathetic activity * Salivary cortisol * PR * | |||||||||
| Lee (2014) [29] | Japan | Crossover trial | Healthy students (n = 48) | Forest therapy program—Forest walking (12–15 min), self-paced walking in the forest environments—Switched sites with 24 h. interval | Conducted same activities in the urban | SD method The feeling of refreshed questionnaire POMS The Spielberger State-Trait Anxiety Inventory (STAI) questionnaire | HRV BP | Emotion * Tension-anxiety * Depression Anger-hostility * Fatigue * Confusion * Vigor * State anxiety level * | |
| n = 48 | |||||||||
| ln(LF/HF) * HR * BP | |||||||||
| Lim (2014) [30] | Republic of Korea | Non-equivalent control group design | Senior citizens in a nursing home (n = 64) | Forest therapy program—Once a week (for 90 min) for 11 weeks—Meditation—Experiencing forest | Cont. 1: Indoor therapy (Conducted same activities program in the room) Cont. 2: Normal daily routines | Self-esteem Depression | None | Self-esteem * Depression * | |
| n = 22 | Cont. 1 n = 21 Cont. 2 n = 21 | ||||||||
| Mao G.X. (2012) [19] | China | RCT | Healthy students (n = 20) | Forest bathing—Twice a day for two days—Walking in the forest area (for 90 min), with a 10-min rest during the walk | Conducted same activities in the city area | POMS | BP Cytokine Enzyme-linked immunoassay | Tension-anxiety * Depression-dejection * Anger-hostility * Fatigue-inertia * Confusion-bewilderment Vigor-activity * | |
| n = 10 | n = 10 | ||||||||
| BP * Cytokine: IL-6 * Enzyme-linked immunoassay: Renin *, AGT * | |||||||||
| Shin (1996) [31] | Republic of Korea | Non-equivalent control group design | Students (BDI scores: 18–30) (n = 64) | 5-day forest program—Group presentation, team exercise, hiking, and climbing the mountain | Normal daily routines | BDI | None | Depression * | |
| n = 32 | n = 32 | ||||||||
| Song (2011) [32] | Japan | Crossover trial | Healthy male adults (n = 18) | Walking in the urban forest (20 min)—Switched sites with 24 h. interval | Conducted same activity in the urban area | POMS STAI The Symptom Checklist (SCL-90) Type A behavior | None | Tension-anxiety Depression * Anger-hostility * Fatigue * Confusion Vigor * Total mood disturbance * State-anxiety * Hostility * Anxiety * Obsessive-compulsive * Somatization * | |
| n = 18 | |||||||||
| Song (2014) [33] | Republic of Korea | Non-equivalent control groupdesign | Female nursing college students (n = 53) | Forest Healing Program—Once a week (for 3 h) for 12 weeks—Forest meditation—Natural healing play—Stress management | Normal daily routines | Stress Response The Spiritual Assessment Scale | None | Tension * Attack * Somatization Anger Depression Fatigue Frustration * Total points of stress responses * Total points of spirituality * | |
| n = 27 | n = 26 | ||||||||
| Song (2015) [23] | Japan | Crossover trial | Healthy students (n = 11) | Walking in the forest in the morning (for 15 min) Viewing the forest (for 15 min) in the afternoon—Switched sites with 24 h. interval | Conducted same activities in the urban area | SD method An inventory for the measurement of self-reported stress and arousal POMS STAI | HRV | Emotion (Comfortable, Relaxed *, Natural * Feeling refreshed *) Tension-anxiety * Depression * Anger–hostility Fatigue * Confusion Vigor * Anxiety * | |
| n = 11 | |||||||||
| Overall mean ln(HF) * Overall mean HR * | |||||||||
| Takayama (2014) [34] | Japan | Crossover trial | Healthy students (n = 45) | Forest bathing—Walking in the forest in morning (15 min)—Viewing the forest in the afternoon (15 min)—Switched sites with 24 h. interval | Conducted same activities in the urban area | POMS Positive and Negative Affect Schedule (PANAS) The Restorative Outcome Scale (ROS) The Subjective Vitality Scale | None | Tension–anxiety * Depression * Anger–hostility Fatigue Confusion * Vigor * Negative affect * Positive Affect * The ROS score * The total SVS score * | |
| n = 45 | |||||||||
| Yang (2011) [35] | Republic of Korea | Non-equivalent control groupdesign | Alcoholics’ families (n = 46) | 6-day forest program—Forest experience—Drawing a forest—Day and Night walk | Normal daily Routines | Spiritual health Inventory (SHI) BDI The Rosenberg Self-Esteem Scale | None | Spiritual health * Depression * Self-esteem * | |
| n = 24 | n = 22 | ||||||||
| You (2014) [36] | Republic of Korea | Non-equivalent control group design | Healthy females (n = 20) | Sallimyok (Forest Therapy) Meditation Walking Qi-Qong program | Normal daily routines | Zung Self-Rating Depression Scale Psychological Well-Being Scale | None | Depression * Psychological well-being * | |
| n = 10 | n = 10 | ||||||||
| Authors (Year) | Country | Research Design | Participants (N) | Intervention | Control | Measurement | Outcome | ||
|---|---|---|---|---|---|---|---|---|---|
| Exp. | Cont. | Self-Report Measures | Physiological Measures | ||||||
| Barton (2012) [12] | UK | Non-equivalent control group design | Adults with a mental health problem (n = 53) | Green exercise Walking in the green spaces (45 min) | Cont. 1: Swimming Cont. 2: Social activities | The Rosenberg Self-Esteem Scale POMS | None | Self-esteem * Overall mood | |
| n = 24 | Cont. 1 (n = 14) Cont. 2 (n = 15) | ||||||||
| Choi (2014) [37] | Republic of Korea | Non-equivalent control group design | Cancer patients (n = 53) | Forest-experience-integration intervention †—Once a week (for 120 min) for 8 weeks | Normal daily routines | Zung Self-Rating Depression Scale Self-regulation Resilience | None | Depression * Resilience * | |
| n = 26 | n = 27 | ||||||||
| Chun (2016) [20] | Republic of Korea | RCT | Chronic stroke patients (n = 59) | 4-day forest therapy program—Meditation, Experiencing the forest through all five senses—Walking in the forest | Stayed in a hotel and participated in meditation and walking activities | BDI Hamilton Depression rating scale (HAM-D17) STAI | None | Depression * Anxiety * | |
| n = 30 | n = 29 | ||||||||
| Hong (2012) [13] | Republic of Korea | Crossover trial | Psychiatric outpatients (n = 16) | 3-day forests healing program ‡for patients with Hwa-Byung—Washout period (28 days) | Conducted regular diet and exercise program (3 times a day) in the forest | The Instrument of Oriental Medical Evaluation for Hwa-Byung BDI STAI State-Trait Anger Expression Inventory (STAXI) WHO Quality of Life Scale Abbreviated Version (WHOQOL-BREF) | Heart Rate Variability | Hwa-Byung symptoms * Depression * Anxiety * State anger * Trait anger Quality of Life * | |
| n = 16 | |||||||||
| Mean HR * Heart rate variability LF/HF | |||||||||
| Hong (2013) [14] | Republic of Korea | Crossover trial | Psychiatric outpatients (n = 15) | 3-day forests healing programs ‡ for cognitive improvement—Washout period (28 days) | Conducted regular diet and exercise program (3 times a day) in the forest | BDI STAI STAXI WHOQOL-BREF | None | Depression * Anxiety Anger Quality of Life * | |
| n = 15 | |||||||||
| Jia (2016) [21] | China | RCT | COPD patient (n = 20) | One-day forest bathing trip—Forest walking in the morning (for 90 min) and in the afternoon (for 90 min) | One-day trip for urban walking | POMS | Cortisol Epinephrine | Tension-anxiety * Depression-dejection * Anger-hostility * Fatigue-inertia Confusion-bewilderment Vigor-activity | |
| n = 10 | n = 10 | ||||||||
| Cortisol * Epinephrine * | |||||||||
| Kim (2015) [15] | Republic of Korea | Non-equivalent control group design | Psychiatric inpatients (n = 20) | Forest experience program—5 times in 2 weeks (60 min each time)—Handkerchief dyeing—Decorating a frame using natural items | TAU | Korean Version of Profile of Mood State-Brief (K-POMS-B) BDI | Salivary cortisol | Tension-anxiety Depression Anger-hostility Fatigue Confusion Vigor Total moods disturbance | |
| n = 10 | n = 10 | ||||||||
| Cortisol * | |||||||||
| Kim (2015) [38] | Republic of Korea | Non-equivalentcontrol groupdesign | Cancer patients (n = 53) | Forest activity intervention—4 h. a day for 3 days—Experiencing feeling (1st day), meditation (2nd day), mindfulness (3rd day) and feedback | Normal daily routines | Hospital Anxiety and Depression Scale (HADS) Profile of Mood States-Brief (POMS-B) Dispositional Hope Scale | None | Tension * Anxiety * Depression * Anger * Fatigue * Confusion * Vigor Total mood disturbance * Hope | |
| n = 27 | n = 26 | ||||||||
| Mao (2012) [22] | China | RCT | Elderly with hypertension (n = 24) | Forest bathing—Twice a day for 7 days—Walking in the forest area for 90 min, with a 10-min rest during the walk | Conducted same activity in the city area | POMS | Serum Cortisol | Tension-anxiety Depression-dejection * Anger-hostility * Fatigue-inertia * Confusion-Bewilderment * Vigor-activity * | |
| n = 12 | n = 12 | ||||||||
| Serum Cortisol * | |||||||||
| Shin (2012)[16] | Republic of Korea | RCT | Adult alcoholics (n = 92) | 9-day forest therapy camp § | Normal daily routines | BDI | None | Depression * | |
| n = 47 | n = 45 | ||||||||
| Song (2015) [39] | Japan | Crossover trial | Middle-aged hypertensive individuals (20) | Walking in the forest area (for 17 min)—Switched sites with 24 h. interval | Conducted same activity in the urban area | SD method POMS | HRVHR | Emotion Tension–anxiety * Depression * Anger–hostility * Fatigue * Confusion * Vigor * | |
| n = 20 | |||||||||
| Ln(HF) * HR * | |||||||||
| Woo (2012) [17] | Republic of Korea | Non-equivalent control groupdesign | Patients with major depressive disorder (n = 81) | Forest therapy —Once a week for 4 weeks (for 3 h)—Cognitive behavior therapy—Forest meditation—Relaxation training—Forest explanation | Cont. 1: conducted the same intervention in a hospital Cont. 2: forest bath Cont. 3: TAU | HRSD Montgomery-Asberg Depression Rating Scale (MADRS) BDI Short Form Health Survey Questionnaire (SF-36) | HRV | Depression * Quality of life * | |
| n = 28 | Cont.1 N = 21 Cont. 2 N = 17 Cont. 3 N = 15 | HF power * LF/HF ratio | |||||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, I.; Choi, H.; Bang, K.-S.; Kim, S.; Song, M.; Lee, B. Effects of Forest Therapy on Depressive Symptoms among Adults: A Systematic Review. Int. J. Environ. Res. Public Health 2017, 14, 321. https://doi.org/10.3390/ijerph14030321
Lee I, Choi H, Bang K-S, Kim S, Song M, Lee B. Effects of Forest Therapy on Depressive Symptoms among Adults: A Systematic Review. International Journal of Environmental Research and Public Health. 2017; 14(3):321. https://doi.org/10.3390/ijerph14030321
Chicago/Turabian StyleLee, Insook, Heeseung Choi, Kyung-Sook Bang, Sungjae Kim, MinKyung Song, and Buhyun Lee. 2017. "Effects of Forest Therapy on Depressive Symptoms among Adults: A Systematic Review" International Journal of Environmental Research and Public Health 14, no. 3: 321. https://doi.org/10.3390/ijerph14030321