
Nocturnal Road Traffic Noise Exposure and Children’s Sleep Duration and Sleep Problems

Abstract
:1. Introduction
2. Materials and Methods
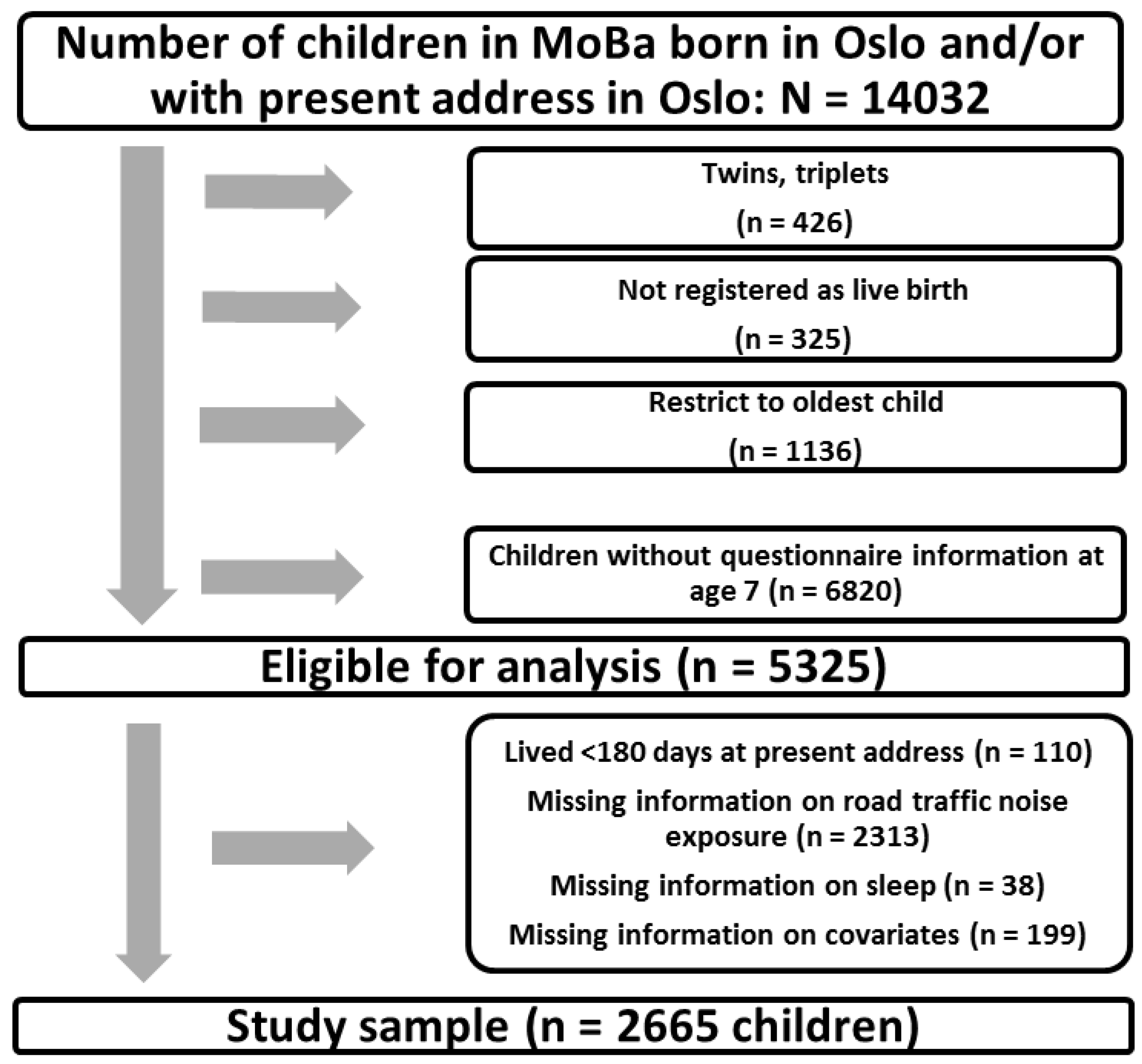
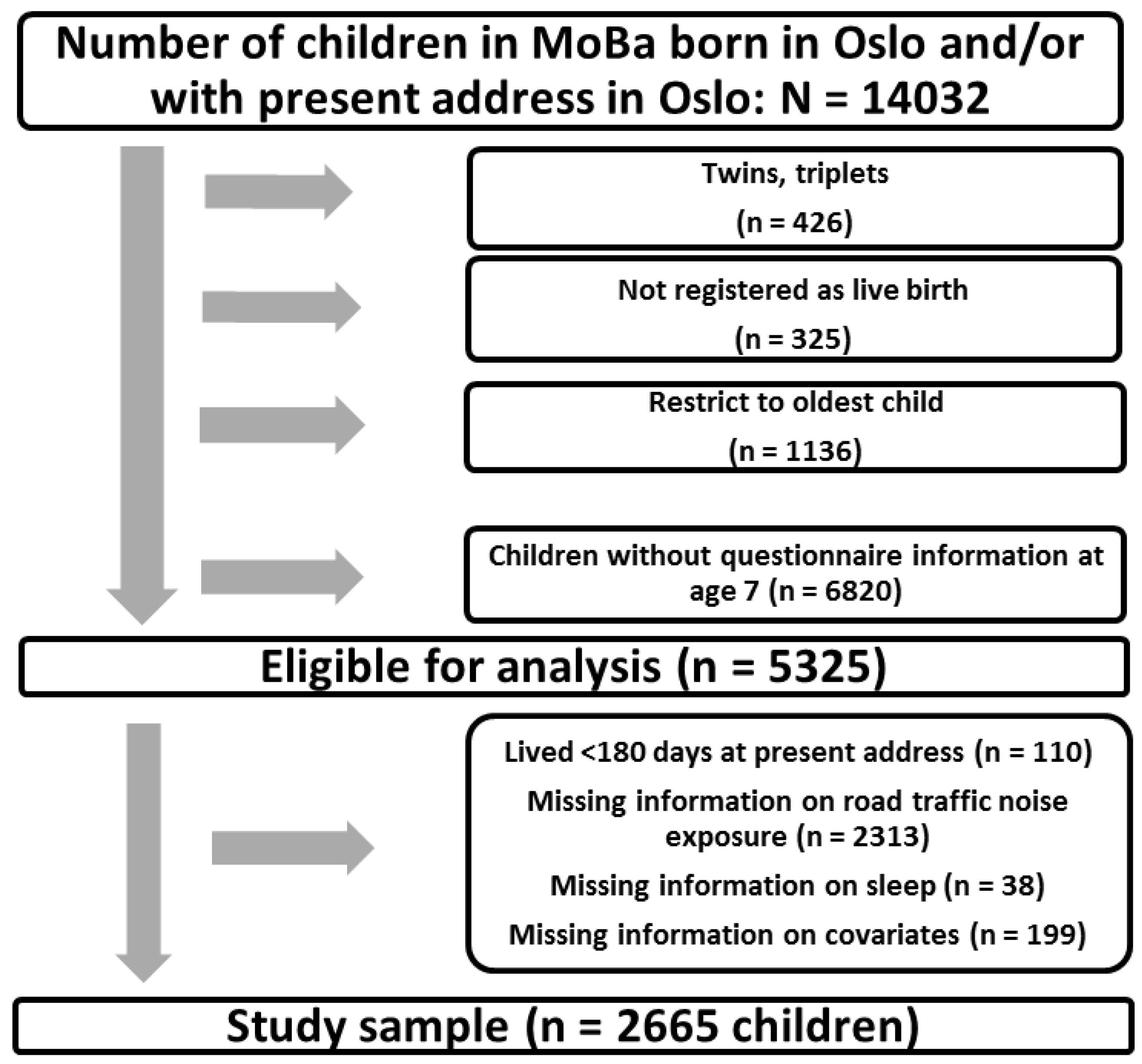
2.1. Study Population
2.2. Noise Exposure Assessment
2.3. Sleep Outcomes
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Descriptives
3.2. Study Sample versus Non-Participants
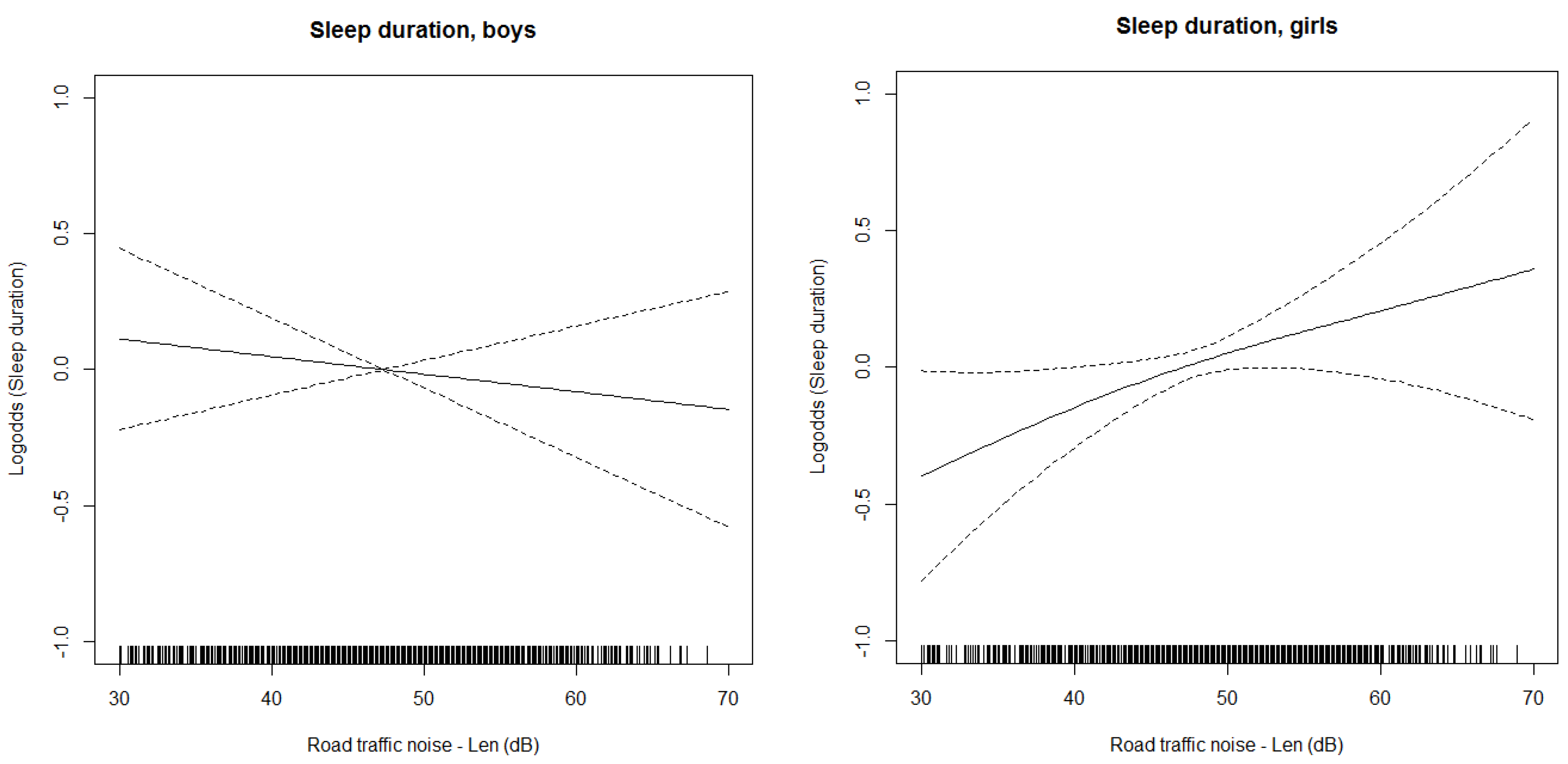
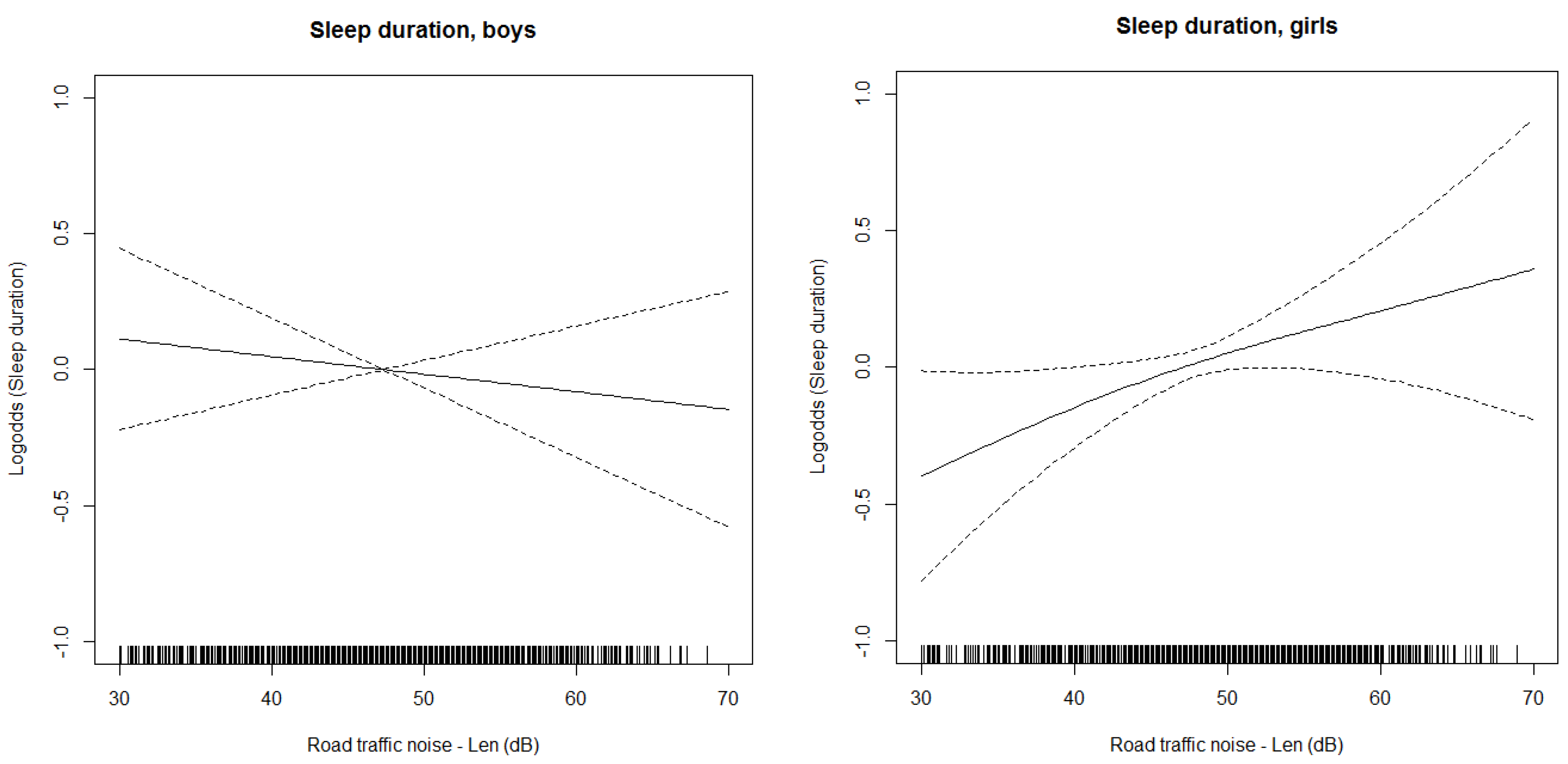
3.3. Main Results
4. Discussion
4.1. Summary of Findings and Comparison with Existing Literature
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- WHO. Burden of Disease from Environmental Noise: Quantification of Healthy Years Life Lost in Europe; World Health Organisation. Regional Office for Europe: Copenhagen, Denmark, 2011. [Google Scholar]
- EEA. Noise in Europe 2014; European Environment Agency: Luxembourg, 2014. [Google Scholar]
- EEA. Good Practice Guide on Noise Exposure and Potential Health Effects; European Environment Agency: Luxembourg, 2010. [Google Scholar]
- Statistics Norway. Barn og Unges Miljø og Helse 2011. Utvalgte Indikatorer om Barn og Unges Fysiske og Sosiale Miljøfaktorer. Available online: http://www.ssb.no/a/publikasjoner/pdf/rapp_201212/rapp_201212.pdf (accessed on 22 February 2015).
- Basner, M.; Babisch, W.; Davis, A.; Brink, M.; Clark, C.; Janssen, S.; Stansfeld, S. Auditory and non-auditory effects of noise on health. Lancet 2014, 383, 1325–1332. [Google Scholar] [CrossRef]
- Hjortebjerg, D.; Andersen, A.M.N.; Christensen, J.S.; Ketzel, M.; Raaschou-Nielsen, O.; Sunyer, J.; Julvez, J.; Forns, J.; Sørensen, M. Exposure to road traffic noise and behavioral problems in 7-year-old children: A cohort study. Environ. Health Perspect. 2015. [CrossRef]
- Orban, E.; McDonald, K.; Sutcliffe, R.; Hoffmann, B.; Fuks, K.B.; Dragano, N.; Viehmann, A.; Erbel, R.; Jockel, K.H.; Pundt, N.; et al. Residential road traffic noise and high depressive symptoms after five years of follow-up: Results from the heinz nixdorf recall study. Environ. Health Perspect. 2016, 124, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Basner, M.; Glatz, C.; Griefahn, B.; Penzel, T.; Samel, A. Aircraft noise: Effects on macro- and microstructure of sleep. Sleep Med. 2008, 9, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Evandt, J.; Oftedal, B.; Krog, N.H.; Nafstad, P.; Schwarze, P.; Aasvang, G.M. A population-based study on nighttime road traffic noise and insomnia. Sleep 2017, 40, zsw055. [Google Scholar] [CrossRef] [PubMed]
- Frei, P.; Mohler, E.; Roosli, M. Effect of nocturnal road traffic noise exposure and annoyance on objective and subjective sleep quality. Int. J. Hyg. Environ. Health 2014, 217, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Griefahn, B.; Bröde, P.; Marks, A.; Basner, M. Autonomic arousals related to traffic noise during sleep. Sleep 2008, 34, 569–577. [Google Scholar] [CrossRef]
- Pirrera, S.; De Valck, E.; Cluydts, R. Field study on the impact of nocturnal road traffic noise on sleep: The importance of in- and outdoor noise assessment, the bedroom location and nighttime noise disturbances. Sci. Total Environ. 2014, 500–501, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Öhrström, E.; Hadzibajramovic, E.; Holmes, M.; Svensson, H. Effects of road traffic noise on sleep: Studies on children and adults. J. Environ. Psychol. 2006, 26, 116–126. [Google Scholar] [CrossRef]
- Van Kamp, I.; Persson Waye, K.; Gidlöf-Gunnarsson, A. The effects of noise disturbed sleep in children on cognitive development and long term health. J. Child. Adolescent Behav. 2015, 3. [Google Scholar] [CrossRef]
- Skinner, C.J.; Grimwood, C.J. The UK national noise incidence study 2000/2001. In Proceedings of the Noise Forum Conference, London, UK, 20 May 2002. [Google Scholar]
- Babisch, W.; Schulz, C.; Seiwert, M.; Conrad, A. Noise annoyance as reported by 8- to 14-year-old children. Environ. Behav. 2010, 44, 68–86. [Google Scholar] [CrossRef]
- Stansfeld, S.; Clark, C. Health effects of noise exposure in children. Curr. Environ. Health Rep. 2015, 2, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Kurth, S.; Ringli, M.; Lebourgeois, M.K.; Geiger, A.; Buchmann, A.; Jenni, O.G.; Huber, R. Mapping the electrophysiological marker of sleep depth reveals skill maturation in children and adolescents. NeuroImage 2012, 63, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Moroni, F.; Nobili, L.; Curcio, G.; De Carli, F.; Tempesta, D.; Marzano, C.; De Gennaro, L.; Mai, R.; Francione, S.; Lo Russo, G.; et al. Procedural learning and sleep hippocampal low frequencies in humans. NeuroImage 2008, 42, 911–918. [Google Scholar] [CrossRef] [PubMed]
- Urbain, C.; Galer, S.; Van Bogaert, P.; Peigneux, P. Pathophysiology of sleep-dependent memory consolidation processes in children. Int. J. Psychophysiol. 2013, 89, 273–283. [Google Scholar] [CrossRef] [PubMed]
- Beebe, D.W. Cognitive, behavioral, and functional consequences of inadequate sleep in children and adolescents. Pediatr. Clin. N. Am. 2011, 58, 649–665. [Google Scholar] [CrossRef] [PubMed]
- Iglowstein, I.; Jenni, O.G.; Molinari, L.; Largo, L.H. Sleep duration from infancy to adolescence: Reference values and generational trends. Pediatrics 2003, 111, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Matricciani, L.; Olds, T.; Petkov, J. In search of lost sleep: Secular trends in the sleep time of school-aged children and adolescents. Sleep Med. Rev. 2012, 16, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Tiesler, C.M.; Birk, M.; Thiering, E.; Kohlbock, G.; Koletzko, S.; Bauer, C.P.; Berdel, D.; von Berg, A.; Babisch, W.; Heinrich, J.; et al. Exposure to road traffic noise and children’s behavioural problems and sleep disturbance: Results from the giniplus and lisaplus studies. Environ. Res. 2013, 123, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ising, H.; Ising, M. Chronic cortisol increases in the first half of the night caused by road traffic noise. Noise Health 2002, 4, 13–21. [Google Scholar] [PubMed]
- Eberhardt, J.L. The influence of road traffic noise on sleep. J. Sound Vibr. 1988, 127, 449–455. [Google Scholar] [CrossRef]
- Bagley, E.J.; Kelly, R.J.; Buckhalt, J.A.; El-Sheikh, M. What keeps low-ses children from sleeping well: The role of presleep worries and sleep environment. Sleep Med. 2015, 16, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, L.; Fabbri, M.; Natale, V. Sex difference in sleep-time preference and sleep need: A cross-sectional survey among italian pre-adolescents, adolescents, and adults. Chronobiol. Int. 2008, 25, 745–759. [Google Scholar] [CrossRef] [PubMed]
- Hysing, M.; Pallesen, S.; Stormark, K.M.; Lundervold, A.J.; Sivertsen, B. Sleep patterns and insomnia among adolescents: A population-based study. J. Sleep Res. 2013, 22, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Halonen, J.I.; Vahtera, J.; Stansfeld, S.; Yli-Tuomi, T.; Salo, P.; Pentti, J.; Kivimaki, M.; Lanki, T. Associations between nighttime traffic noise and sleep: The finnish public sector study. Environ. Health Perspect. 2012, 120, 1391–1396. [Google Scholar] [CrossRef] [PubMed]
- Nissenbaum, N.A.; Aramini, J.J.; Hanning, C.D. Effects of industrial wind turbine noise on sleep and health. Noise Health 2012, 14, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Röösli, M.; Mohler, E.; Frei, P.; Vienneau, D. Noise-related sleep disturbances: Does gender matter? Noise Health 2014, 16, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Biggs, S.N.; Lushington, K.; James Martin, A.; van den Heuvel, C.; Declan Kennedy, J. Gender, socioeconomic, and ethnic differences in sleep patterns in school-aged children. Sleep Med. 2013, 14, 1304–1309. [Google Scholar] [CrossRef] [PubMed]
- Bøe, T.; Hysing, M.; Stormark, K.M.; Lundervold, A.J.; Sivertsen, B. Sleep problems as a mediator of the association between parental education levels, perceived family economy and poor mental health in children. J. Psychosom. Res. 2012, 73, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Magnus, P.; Birke, C.; Vejrup, K.; Haugan, A.; Alsaker, E.; Daltveit, A.K.; Handal, M.; Haugen, M.; Hoiseth, G.; Knudsen, G.P.; et al. Cohort profile update: The norwegian mother and child cohort study [2]. Int. J. Epidemiol. 2016, 45, 382–388. [Google Scholar] [CrossRef] [PubMed]
- EU. Directive 2002/49/ec of the european parliament and of the councilof 25 june 2002 relating to the assessment and management of environmental noise. Off. J. Eur. Communities 2002, 189, 12–25. [Google Scholar]
- Jonasson, H.; Nielsen, H.L. Road Traffic Noise-Nordic Prediction Method; Nordic Council of Ministers: Copenhagen, Denmark, 1996. [Google Scholar]
- Bendtsen, H. The nordic prediction method for road traffic noise. Sci. Total Environ. 1999, 235, 331–338. [Google Scholar] [CrossRef]
- DataKustik. Cadnaa Version 4.3; DataKustik GmbH: Bayern, Germany, 2017. [Google Scholar]
- Shrier, I.; Platt, R.W. Reducing bias through directed acyclic graphs. BMC Med. Res. Methodol. 2008, 8, 70. [Google Scholar] [CrossRef] [PubMed]
- Greenland, S.; Pearl, J.; Robins, J.M. Causal diagrams for epidemiologic research. Epidemiology 1999, 10, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Pearl, J. Causality: Models, Reasoning and Inference; Cambridge University Press: New York, NY, USA, 2000. [Google Scholar]
- Textor, J.; Hardt, J.; Knüppel, S. Dagitty: A graphical tool for analyzing causal diagrams. Epidemiology 2011, 22, 745. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, R.; Gould, W. An approximate likelihood-ratio test for ordinal response models. Stata Tech. Bull. 1998, 42, 24–27. [Google Scholar]
- Williams, R. Fitting heterogeneous choice models with oglm. Stata J. 2010, 10, 540–567. [Google Scholar]
- Aasvang, G.M.; Moum, T.; Engdahl, B. Self-reported sleep disturbances due to railway noise: Exposure-response relationships for nighttime equivalent and maximum noise levels. J. Acoust. Soc. Am. 2008, 124, 257–268. [Google Scholar] [CrossRef] [PubMed]
- StataCorp. Stata Version 14.0; StataCorp LLC: College Station, TX, USA, 2015. [Google Scholar]
- WHO. Night Noise Guidelines for Europe; World Health Organization: Copenhagen, Denmark, 2009. [Google Scholar]
- Høydal, E. Innvandrerbegreper i statistikken: Vestlig og ikke-vestlig-ord som ble for store og gikk ut på dato. Samfunnsspeilet 2008, 4, 66–69. [Google Scholar]
- Oginska, H.; Pokorski, J. Fatigue and mood correlates of sleep length in three age-social groups: School children, students, and employees. Chronobiol. Int. 2009, 23, 1317–1328. [Google Scholar] [CrossRef] [PubMed]
- Haines, M.M.; Brentnall, S.L.; Stansfeld, S.A.; Klineberg, E. Qualitative responses of children to environmental noise. Noise Health 2003, 5, 19–30. [Google Scholar] [PubMed]
- Basner, M.; Müller, U.; Elmenhorst, E.-M. Single and combined effects of air, road, and rail traffic noise on sleep and recuperation. Sleep 2011, 34, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Holley, S.; Hill, C.M.; Stevenson, J. A comparison of actigraphy and parental report of sleep habits in typically developing children aged 6 to 11 years. Behav. Sleep Med. 2010, 8, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Pirrera, S.; De Valck, E.; Cluydts, R. Nocturnal road traffic noise assessment and sleep research: The usefulness of different timeframes and in- and outdoor noise measurements. Appl. Acoust. 2011, 72, 677–683. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Covariate | Total Study Sample (n = 2665) | |||
|---|---|---|---|---|
| <40 dB | 40–50 dB | >50 dB | Total | |
| n (%) | 455 (17.1) | 1321(49.6) | 889 (33.4) | 2665 |
| % male | 54.3 | 50.3 | 47.6 | 50.1 |
| Sleep duration (%) | ||||
| >10 h | 19.0 | 49.0 | 32.0 | 27.5 |
| 10 h | 16.6 | 50.3 | 33.1 | 57.5 |
| <10 h | 15.5 | 47.8 | 36.8 | 15.0 |
| Sleep problems (% yes) | 2.6 | 2.4 | 3.6 | 2.9 |
| Gross annual household income a (NOK), mean (SD) | 1,057,762 (686,380) | 1,070,305 (923,924) | 893,990 (598,621) | 100,9347 (793,343) |
| Season, questionnaire completion (%) | ||||
| Winter | 19.5 | 46.8 | 33.7 | 23.6 |
| Spring | 16.2 | 48.5 | 35.3 | 23.9 |
| Summer | 15.6 | 51.9 | 32.6 | 20.8 |
| Fall | 16.9 | 50.9 | 32.2 | 31.7 |
| Urbanity b (%) | ||||
| Outskirts | 20.2 | 53.3 | 26.5 | 71.8 |
| Semi-central | 11.1 | 48.6 | 40.2 | 20.5 |
| Center | 3.4 | 17.1 | 79.5 | 7.7 |
| Age (months), mean (SD) | 85.5 (1.5) | 85.4 (1.6) | 85.4 (1.6) | 85.4 (1.6) |
| Mother’s education (%) | ||||
| >4 years university/college | 17.2 | 52.1 | 30.7 | 41.6 |
| ≤4 years university/college | 17.8 | 48.4 | 33.7 | 44.2 |
| High school | 14.2 | 45.8 | 40.0 | 14.3 |
| Ethnicity c (%) | ||||
| Non-Western | 15.1 | 39.6 | 45.3 | 10.4 |
| Western | 17.3 | 50.7 | 32.0 | 89.6 |
| Siblings < age 4 (%) | ||||
| Yes | 18.1 | 49.8 | 32.2 | 37.0 |
| No | 16.5 | 49.4 | 34.1 | 63.0 |
| Type of building (%) | ||||
| Detached house | 19.5 | 57.7 | 22.8 | 22.4 |
| Semi-detached | 19.4 | 54.0 | 26.6 | 46.3 |
| Apartment | 12.0 | 37.2 | 50.8 | 31.3 |
| Rail traffic noise (Len) | ||||
| 0 dB | 59.6 | 48.4 | 40.7 | 47.7 |
| ≤30 dB | 20.2 | 24.8 | 17.3 | 21.5 |
| >30 dB | 20.2 | 26.9 | 42.0 | 30.8 |
| Analysis | Total | Girls | Boys |
|---|---|---|---|
| Crude a (n = 2665) | 1.08 (0.98, 1.19) | 1.19 (1.03, 1.37) | 0.99, (0.86, 1.14) |
| Min. adj. set b (n = 2665) | 1.07 (0.96, 1.18) | 1.17 (1.01, 1.36) | 0.98 (0.85, 1.13) |
| Full c (n = 2665) | 1.05 (0.94, 1.17) | 1.21 (1.04, 1.41) | 0.91 (0.78, 1.06) |
| Live with both parents (n = 2371) | 1.03 (0.92, 1.15) | 1.21 (1.03, 1.42) | 0.87 (0.74, 1.02) |
| Full with rail traffic noise d (n = 2665) | 1.04 (0.94, 1.16) | 1.18 (1.01, 1.38) | 0.93 (0.80, 1.08) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weyde, K.V.; Krog, N.H.; Oftedal, B.; Evandt, J.; Magnus, P.; Øverland, S.; Clark, C.; Stansfeld, S.; Aasvang, G.M. Nocturnal Road Traffic Noise Exposure and Children’s Sleep Duration and Sleep Problems. Int. J. Environ. Res. Public Health 2017, 14, 491. https://doi.org/10.3390/ijerph14050491
Weyde KV, Krog NH, Oftedal B, Evandt J, Magnus P, Øverland S, Clark C, Stansfeld S, Aasvang GM. Nocturnal Road Traffic Noise Exposure and Children’s Sleep Duration and Sleep Problems. International Journal of Environmental Research and Public Health. 2017; 14(5):491. https://doi.org/10.3390/ijerph14050491
Chicago/Turabian StyleWeyde, Kjell Vegard, Norun Hjertager Krog, Bente Oftedal, Jorunn Evandt, Per Magnus, Simon Øverland, Charlotte Clark, Stephen Stansfeld, and Gunn Marit Aasvang. 2017. "Nocturnal Road Traffic Noise Exposure and Children’s Sleep Duration and Sleep Problems" International Journal of Environmental Research and Public Health 14, no. 5: 491. https://doi.org/10.3390/ijerph14050491