
Environmental Barriers to Participation of Preschool Children with and without Physical Disabilities


Abstract
:1. Introduction
- What environmental factors were perceived by parents as barriers to participation of children with and without physical disabilities?
- Does the impact of environmental barriers on participation differ between children with and without physical disabilities?
2. Methods
2.1. Participants
2.2. Measure and Procedures
2.3. Data Analysis
3. Results
3.1. The Identification of Environmental Barriers in Two Groups
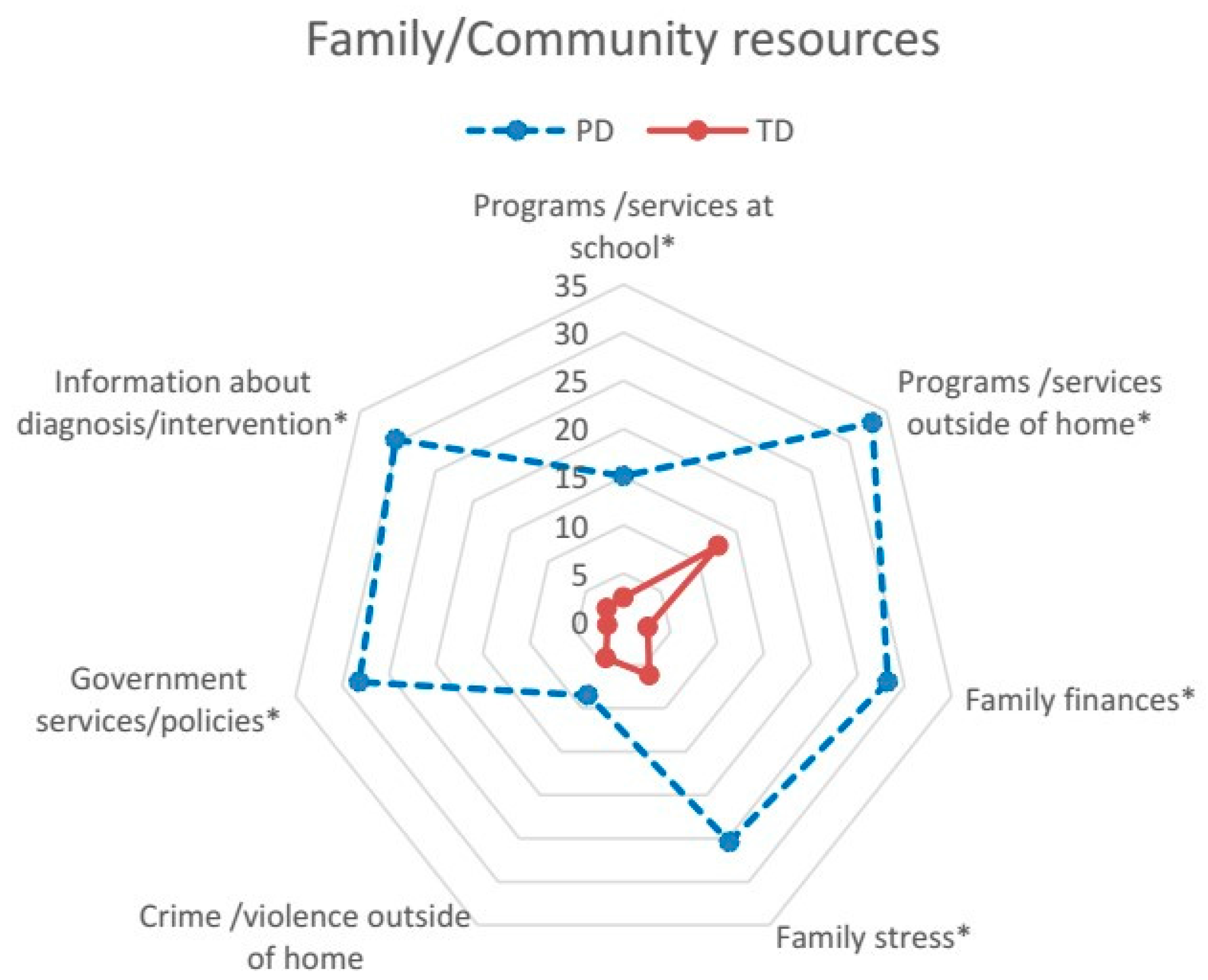
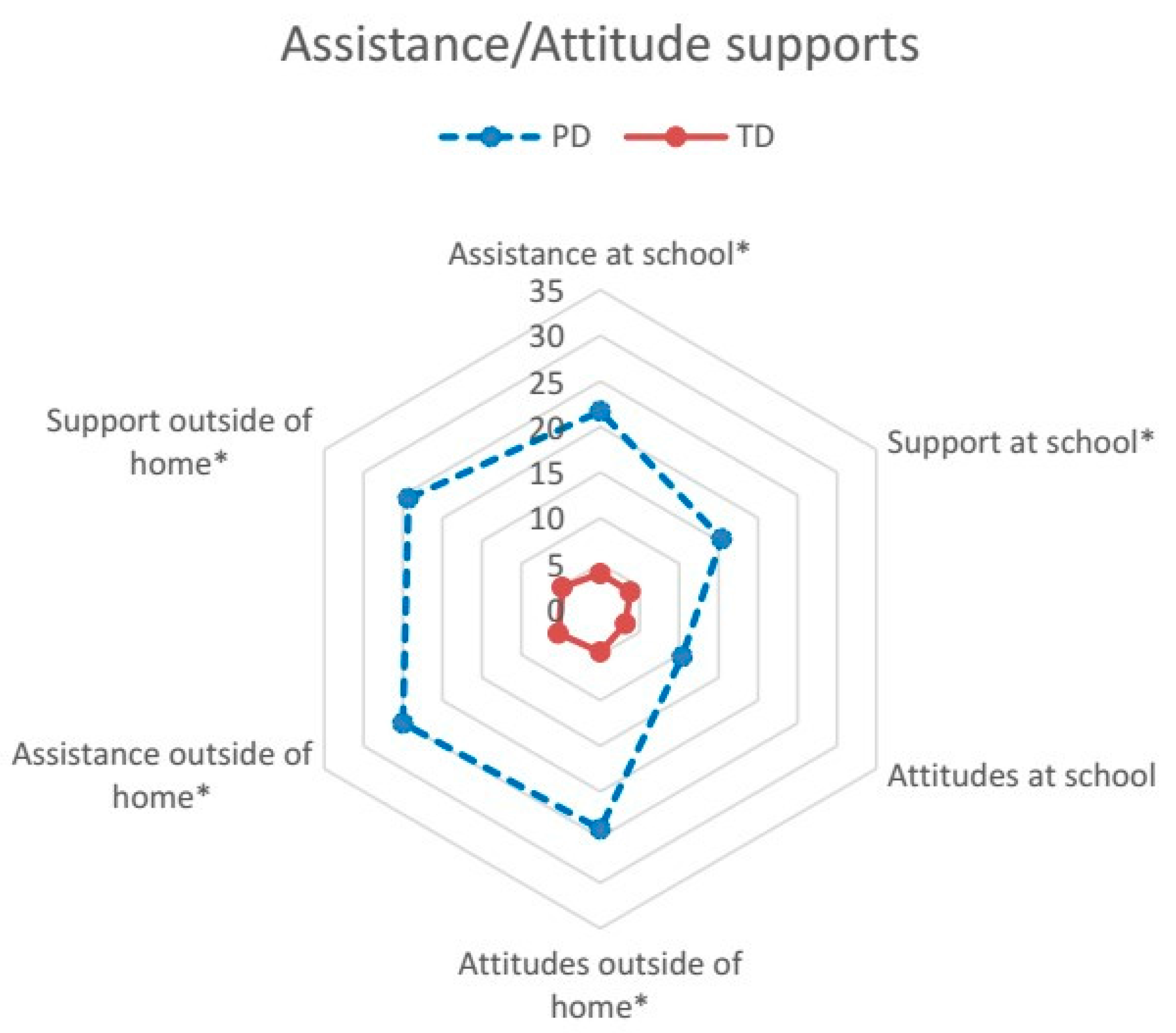
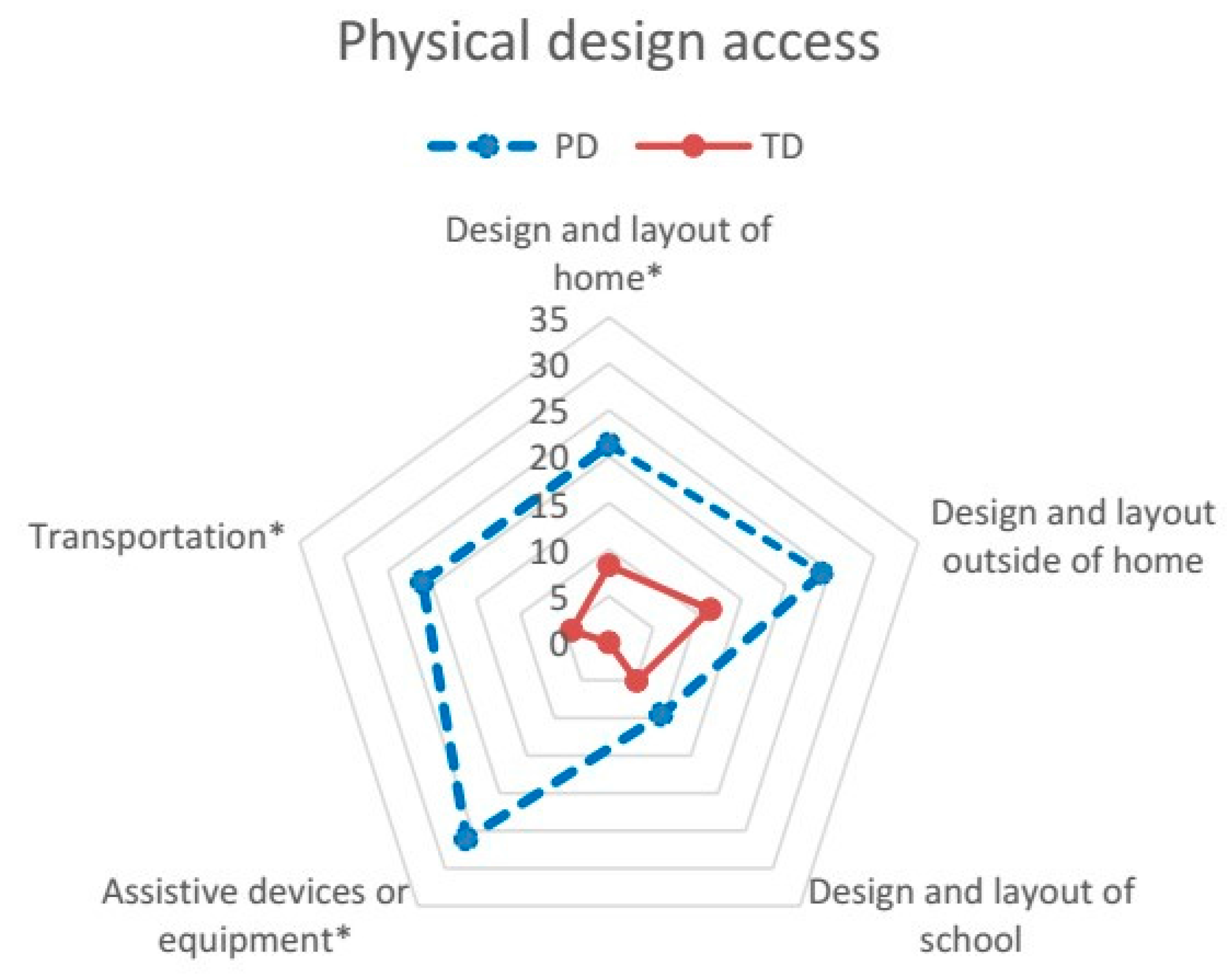
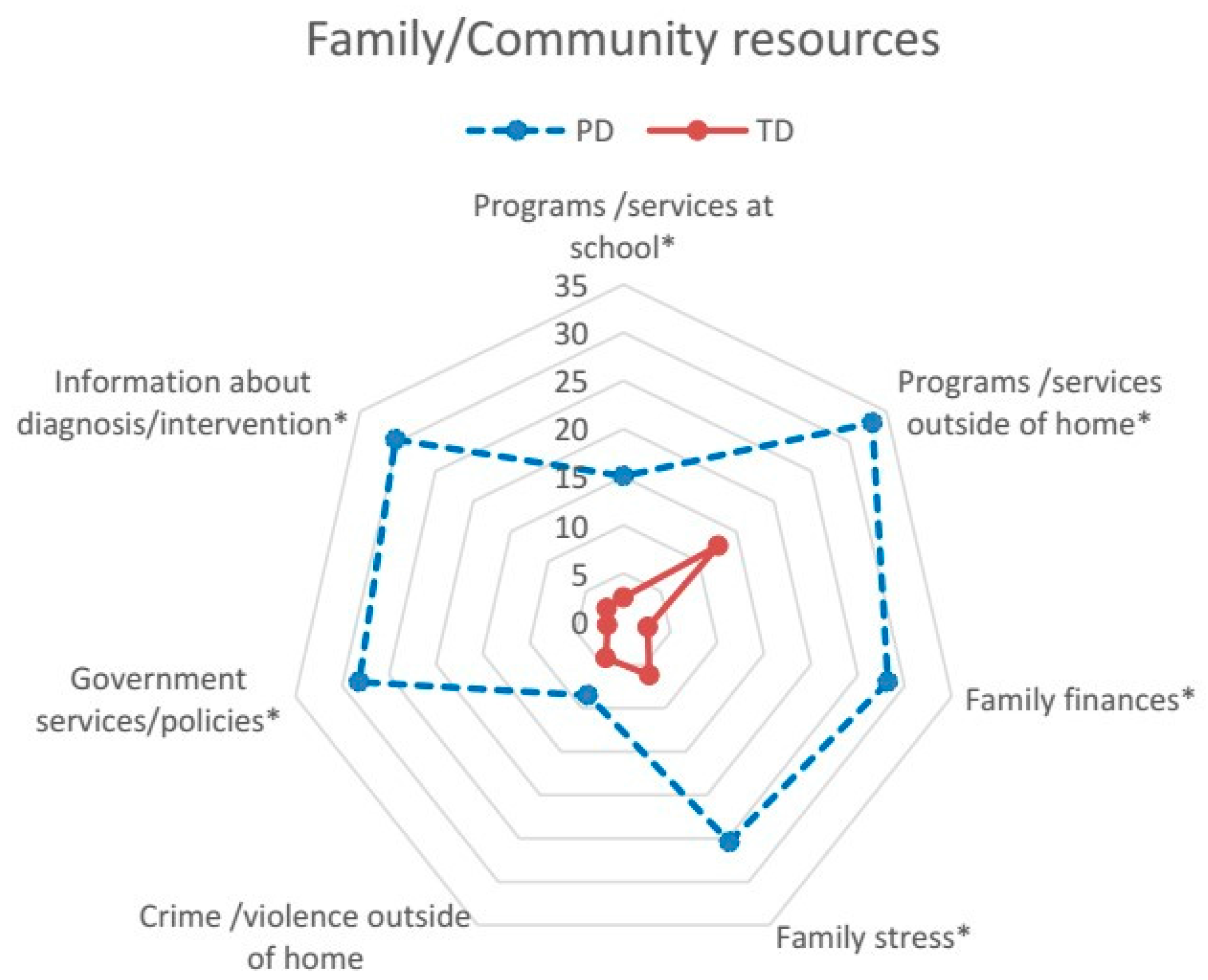
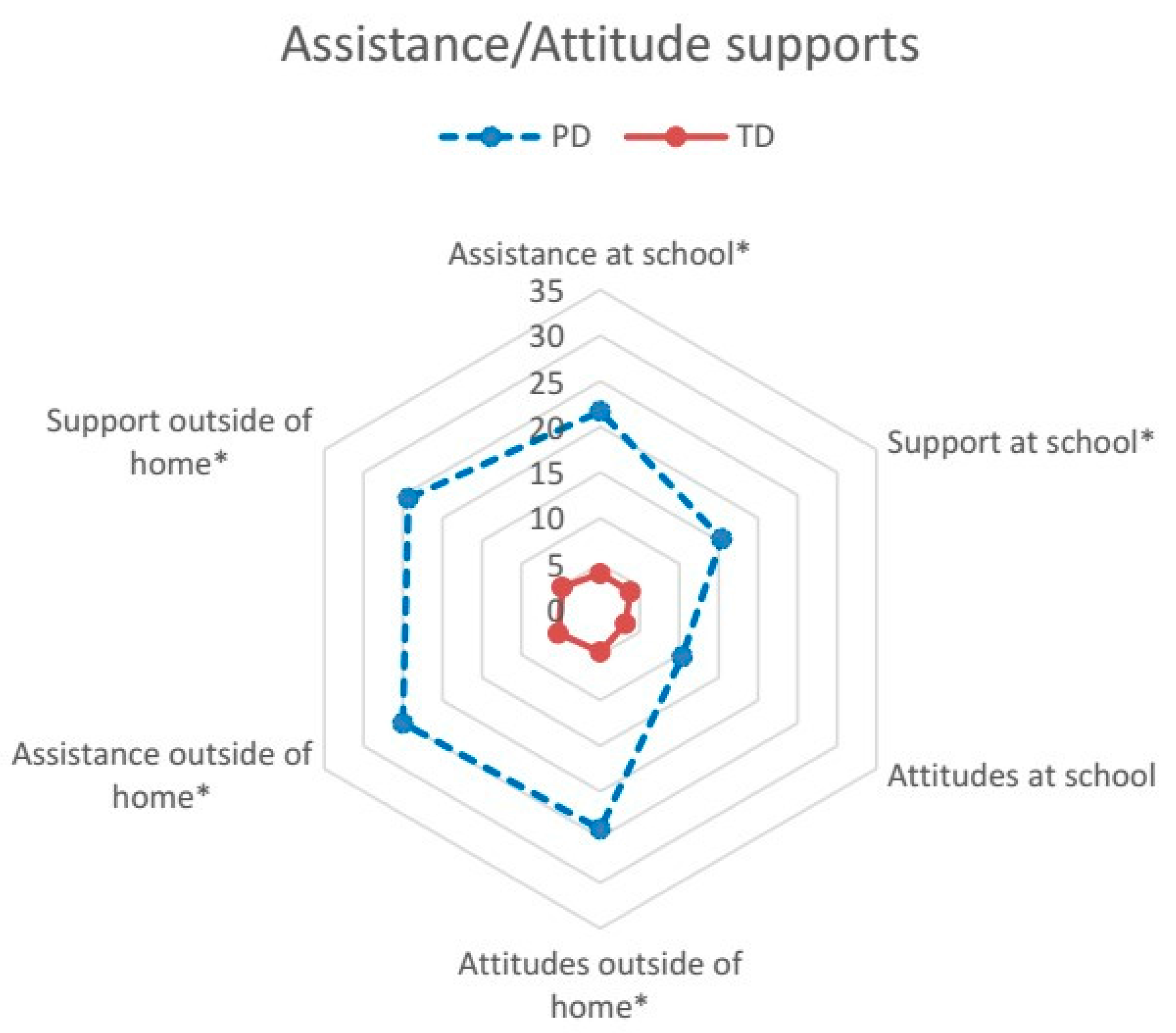
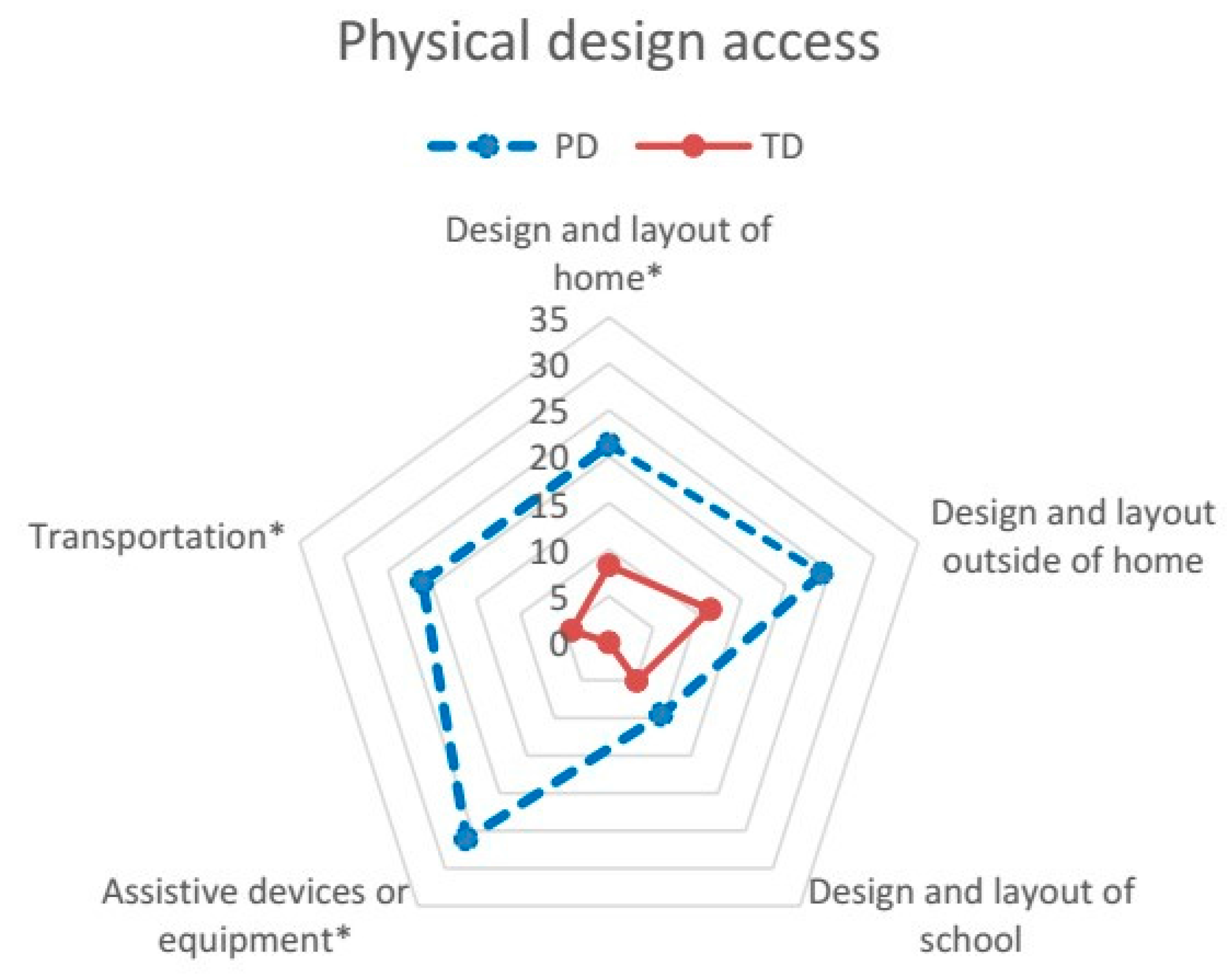
3.2. Comparison of Environmental Barriers between Two Groups
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| PD | Physical disabilities |
| TD | Typical development |
| CASE-C | Chinese version of the Child and Adolescent Scale of Environment |
| ICF | International Classification of Functioning, Health, and Disability |
| DEC | Division for Early Childhood |
| ANCOVA | Analysis of covariance |
| SD | Standard deviation |
References
- Lim, C.Y.; Law, M.; Khetani, M.; Pollock, N.; Rosenbaum, P. Participation in out-of-home environments for young children with and without developmental disabilities. OTJR Occup. Particip. Health 2016, 36, 112–125. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, E.C.; Khetani, M.A. Environmental impact on young children’s participation in home-based activities. Dev. Med. Child. Neurol. 2016, 54, 388–394. [Google Scholar] [CrossRef]
- Benjamin, T.E.; Lucas-Thompson, R.G.; Little, L.M.; Davies, P.L.; Khetani, M.A. Participation in early childhood educational environments for young children with and without developmental disabilities and delays: A mixed methods study. Phys. Occup. Ther. Pediatr. 2017, 37, 87–107. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Division for Early Childhood. DEC Recommended Practices in Early Intervention/Early Childhood Special Education. Available online: http://www.dec-sped.org/recommendedpractices (accessed on 10 February 2017).
- Anaby, D.; Law, M.; Coster, W.; Bedell, G.; Khetani, M.; Avery, L.; Teplicky, R. The mediating role of the environment in explaining participation of children and youth with and without disabilities across home, school, and community. Arch. Phys. Med. Rehabil. 2014, 95, 908–917. [Google Scholar] [CrossRef] [PubMed]
- Majnemer, A.; Shevell, M.; Law, M.; Birnbaum, R.; Chilingaryan, G.; Rosenbaum, P.; Poulin, C. Participation and enjoyment of leisure activities in school-aged children with cerebral palsy. Dev. Med. Child Neurol. 2008, 50, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Kang, L.J.; Palisano, R.J.; Orlin, M.N.; Chiarello, L.A.; King, G.A.; Polansky, M. Determinants of social participation—With friends and others who are not family members—For youths with cerebral palsy. Phys. Ther. 2010, 90, 1743–1757. [Google Scholar] [CrossRef] [PubMed]
- Imms, C. Children with cerebral palsy participate: A review of the literature. Disabil. Rehabil. 2008, 30, 1867–1884. [Google Scholar] [CrossRef] [PubMed]
- Shikako-Thomas, K.; Majnemer, A.; Law, M.; Lach, L. Determinants of participation in leisure activities in children and youth with cerebral palsy: Systematic review. Phys. Occup. Ther. Pediatr. 2008, 28, 155–169. [Google Scholar] [CrossRef] [PubMed]
- Mihaylov, S.I.; Jarvis, S.N.; Colver, A.F.; Beresford, B. Identification and description of environmental factors that influence participation of children with cerebral palsy. Dev. Med. Child. Neurol. 2004, 46, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Bedell, G.; Dumas, H. Social participation of children and youth with acquired brain injuries discharged from inpatient rehabilitation: A follow-up study. Brain Inj. 2004, 18, 65–82. [Google Scholar] [CrossRef] [PubMed]
- Khetani, M.; Graham, J.E.; Alvord, C. Community participation patterns among preschool-aged children who have received part c early intervention services. Child Care Health Dev. 2013, 39, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Darrah, J.; Pollock, N.; Wilson, B.; Russell, D.J.; Walter, S.D.; Rosenbaum, P.; Galuppi, B. Focus on function: A cluster, randomized controlled trial comparing child-versus context-focused intervention for young children with cerebral palsy. Dev. Med. Child Neurol. 2011, 53, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Hwang, A.W.; Liao, H.F.; Granlund, M.; Simeonsson, R.J.; Kang, L.J.; Pan, Y.L. Linkage of icf-cy codes with environmental factors in studies of developmental outcomes of infants and toddlers with or at risk for motor delays. Disabil. Rehabil. 2014, 36, 89–104. [Google Scholar] [CrossRef] [PubMed]
- Khetani, M.A. Validation of environmental content in the young children’s participation and environment measure. Arch. Phys. Med. Rehabil. 2015, 96, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.S.; Hwang, A.W.; Liao, H.F.; Chen, P.C.; Hsieh, W.S.; Chu, P.Y. Psychometric properties of a Chinese version of the home environment measure for motor development. Disabil. Rehabil. 2011, 33, 2454–2463. [Google Scholar] [CrossRef] [PubMed]
- Clawson, C.; Luze, G. Individual experiences of children with and without disabilities in early childhood settings. Top. Early Child. Spec. Educ. 2008, 28, 132–147. [Google Scholar] [CrossRef]
- Law, M.; Anaby, D.; Teplicky, R.; Khetani, M.A.; Coster, W.; Bedell, G. Participation in the home environment among children and youth with and without disabilities. Br. J. Occup. Ther. 2013, 76, 58–66. [Google Scholar] [CrossRef]
- Coster, W.; Law, M.; Bedell, G.; Liljenquist, K.; Kao, Y.C.; Khetani, M.; Teplicky, R. School participation, supports and barriers of students with and without disabilities. Child Care Health Dev. 2013, 39, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Bedell, G.; Coster, W.; Law, M.; Liljenquist, K.; Kao, Y.C.; Teplicky, R.; Anaby, D.; Khetani, M.A. Community participation, supports, and barriers of school-age children with and without disabilities. Arch. Phys. Med. Rehabil. 2013, 94, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Bedell, G. Developing a follow-up survey focused on participation of children and youth with acquired brain injuries after discharge from inpatient rehabilitation. Neurorehabilitation 2004, 19, 191–205. [Google Scholar] [PubMed]
- Kang, L.J.; Yen, C.F.; Bedell, G.; Simeonsson, R.J.; Liou, T.H.; Chi, W.C.; Liu, S.W.; Liao, H.F.; Hwang, A.W. The Chinese version of the child and adolescent scale of environment (case-c): Validity and reliability for children with disabilities in Taiwan. Res. Dev. Disabil. 2015, 38, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Kang, L.J.; Hwang, A.W.; King, G.A.; Hsieh, M.C. Determinants of participation for preschool children with physical disabilities and children with typical development. In Proceedings of the P3M 2017: A Research Symposium for Childhood-Onset Disability, Melbourne, Australia, 14–16 March 2017. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 5th ed.; Allyn & Bacon: Boston, MA, USA, 2007. [Google Scholar]
- Bedell, G. The Child and Adolescent Scale of Environment (CASE): Administration and Scoring Guidelines. Unpublished Work. 2011. [Google Scholar]
- Mallinson, T.; Hammel, J. Measurement of participation: Intersecting person, task, and environment. Arch. Phys. Med. Rehabil. 2010, 91, S29–S33. [Google Scholar] [CrossRef] [PubMed]
- Kirk, R.E. Experimental Design: Procedures for the Behavioral Sciences, 4th ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- Simeonsson, R.J.; Sauer-Lee, A.; Granlund, M.; Bjorck-Akesson, E. Developmental and health assessment in rehabilitation with the ICF for children and youth. In Rehabilitation and Health Assessment: Applying ICF Guidelines; Mpofu, E., Oakland, T., Eds.; Springer Publishing Company: New York, NY, USA, 2010; pp. 27–46. [Google Scholar]
- Teng, S.W.; Yen, C.F.; Liao, H.F.; Chang, K.H.; Chi, W.C.; Wang, T.H.; Liou, T.H.; Team, T.I. Evolution of system for disability assessment based on the international classification of functioning, disability, and health: A Taiwanese study. J. Formos. Med. Assoc. 2013, 112, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Chiu, W.T.; Yen, C.F.; Teng, S.W.; Liao, H.F.; Chang, K.H.; Chi, W.C.; Wang, Y.H.; Liou, T.H. Implementing disability evaluation and welfare services based on the framework of the international classification of functioning, disability and health: Experiences in Taiwan. BMC Health Serv. Res. 2013, 13, 416. [Google Scholar] [CrossRef] [PubMed]
- Hwang, A.W.; Yen, C.F.; Liou, T.H.; Bedell, G.; Granlund, M.; Teng, S.W.; Chang, K.H.; Chi, W.C.; Liao, H.F. Development and validation of the icf-cy-based functioning scale of the disability evaluation system—Child version in Taiwan. J. Formos. Med. Assoc. 2015, 114, 1170–1180. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.C.; Hsieh, M.C.; Kang, L.J. Environmental Barriers in Daily Life of Children with Special Needs and Their Family. In Proceedings of the Seoul International Conference on Social Sciences and Management, Seoul, Korea, 7–9 February 2017. [Google Scholar]
- Anaby, D.; Hand, C.; Bradley, L.; Direzze, B.; Forhan, M.; Digiacomo, A.; Law, M. The effect of the environment on participation of children and youth with disabilities: A scoping review. Disabil. Rehabil. 2013, 35, 1589–1598. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Haight, M.; Milroy, B.; Willms, D.; Stewart, D.; Rosenbaum, P. Environmental factors affecting the occupations of children with physical disabilities. J. Occup. Sci. 1999, 6, 102–110. [Google Scholar] [CrossRef]
- Buell, M.J.; Hallam, R.; Gamel-Mccormick, M.; Scheer, S. A survey of general and special education teachers’ perceptions and inservice needs concerning inclusion. Int. J. Disabil. Dev. Educ. 1999, 46, 143–156. [Google Scholar] [CrossRef]
- Gan, S.M.; Lin, H.Y. Effectiveness and barriers of preschool inclusive program for children with special needs. J. Disabil. Res. 2006, 4, 32–45. [Google Scholar]
- McWilliam, R.A.; Casey, A.M. Engagement of Every Child in the Preschool Classroom; Paul H. Brookes Publishing Co.: Baltimore, MD, USA, 2008. [Google Scholar]
- Colver, A.F.; Dickinson, H.O.; Parkinson, K.; Arnaud, C.; Beckung, E.; Fauconnier, J.; Marcelli, M.; McManus, V.; Michelsen, S.I.; Parkes, J.; et al. Access of children with cerebral palsy to the physical, social and attitudinal environment they need: A cross-sectional European study. Disabil. Rehabil. 2011, 33, 28–35. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Convention on the Right of the Child; United Nations: New York, NY, USA, 1989. [Google Scholar]
- Dinnebeil, L.; Boat, M.; Bae, Y. Integrating principles of universal design into the early childhood curriculum. Dimens. Early Child. 2013, 41, 3–14. [Google Scholar]
- Copple, C.; Bredekamp, S. Developmentally Appropriate Practice in Early Childhood Programs Serving Children from Birth through Age 8; National Association for the Education of Young Children: Washington, DC, USA, 2009. [Google Scholar]
- Ministry of Health and Welfare. The People with Disabilities Rights Protection Act. Available online: http://law.moj.gov.tw/Eng/LawClass/LawAll.aspx?PCode=D0050046 (accessed on 10 February 2017).

{kind=link}
{kind=link}
{kind=link}
| Variables | PD (n = 142) | TD (n = 192) | χ2 | p-Value |
|---|---|---|---|---|
| Child’s age | 3.48 | 0.062 | ||
| < 4 years | 72 (50.7%) | 117 (60.9%) | ||
| ≥ 4 years | 70 (49.3%) | 75 (39.1%) | ||
| Child’s sex | 2.03 | 0.154 | ||
| Boys | 92 (64.8%) | 109 (57.1%) | ||
| Girls | 50 (35.2%) | 82 (42.9%) | ||
| Child schooling | 0.11 | 0.743 | ||
| School | 105 (73.9%) | 145 (75.5%) | ||
| At home | 37 (26.1%) | 47 (24.5%) | ||
| Parent respondents, n (%) | 1.93 | 0.381 | ||
| Mother | 120 (84.5%) | 171 (89.1%) | ||
| Father | 21 (14.8%) | 19 (9.9%) | ||
| Grandparent | 1 (0.7%) | 2 (1.0%) | ||
| Parental education | 43.47 | <0.001 | ||
| Junior high school and under | 9 (6.3%) | 0 | ||
| High school graduate | 47 (33.1%) | 26 (13.5%) | ||
| College/university graduate | 71 (50.0%) | 107 (55.7%) | ||
| Graduate degree | 13 (9.2%) | 57 (29.7%) | ||
| Unanswered | 2 (1.4%) | 2 (1.0%) | ||
| Parental employment status | 19.64 | <0.001 | ||
| Employed | 65 (45.8%) | 134 (69.8%) | ||
| Unemployed | 75 (52.8%) | 56 (29.2%) | ||
| Unanswered | 2 (1.4%) | 2 (1.0%) | ||
| Household income a | 38.14 | <0.001 | ||
| <$800,000 | 89 (62.7%) | 73 (38.0%) | ||
| $800,000–$1,800,000 | 44 (31.0%) | 95 (49.5%) | ||
| >$1,800,000 | 4 (2.8%) | 23 (12.0%) | ||
| Unanswered | 5 (3.5%) | 1 (0.5%) |
| Variables | n (%) |
|---|---|
| Primary conditions | |
| Cerebral palsy | 53 (37.3%) |
| Developmental delay | 53 (37.3%) |
| Chromosomal disorder | 20 (14.1%) |
| Acquired brain injury a | 13 (9.2%) |
| Spina bifida | 1 (0.7%) |
| Congenital anomalies | 2 (1.4%) |
| Primary methods of mobility | |
| Walking | 86 (60.6%) |
| Walking with assistive device | 22 (15.5%) |
| Crawling | 6 (4.2%) |
| Carried by others | 28 (19.7%) |
| PD | TD | ANCOVA | ||
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | F(df) | ηp2 | |
| Total | 42.00 (8.65) | 35.17 (3.19) | 95.35(1,329) * | 0.23 |
| Family/Community resources | 43.47 (11.14) | 35.22 (4.26) | 81.83(1,329) * | 0.20 |
| Assistance/Attitude supports | 40.77 (11.28) | 34.72 (3.86) | 42.24(1,329) * | 0.11 |
| Physical design access | 41.24 (9.32) | 35.50 (4.66) | 57.12(1,329) * | 0.15 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, L.-J.; Hsieh, M.-C.; Liao, H.-F.; Hwang, A.-W. Environmental Barriers to Participation of Preschool Children with and without Physical Disabilities. Int. J. Environ. Res. Public Health 2017, 14, 518. https://doi.org/10.3390/ijerph14050518
Kang L-J, Hsieh M-C, Liao H-F, Hwang A-W. Environmental Barriers to Participation of Preschool Children with and without Physical Disabilities. International Journal of Environmental Research and Public Health. 2017; 14(5):518. https://doi.org/10.3390/ijerph14050518
Chicago/Turabian StyleKang, Lin-Ju, Ming-Chieh Hsieh, Hua-Fang Liao, and Ai-Wen Hwang. 2017. "Environmental Barriers to Participation of Preschool Children with and without Physical Disabilities" International Journal of Environmental Research and Public Health 14, no. 5: 518. https://doi.org/10.3390/ijerph14050518