
Income-Related Inequalities in Access to Dental Care Services in Japan

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Ethics Statement
2.3. Access to Dental Care Services
2.4. Equivalent Household Income
2.5. Other Categorization of the Data
2.6. Statistical Analysis
2.7. Sensitivity Analysis
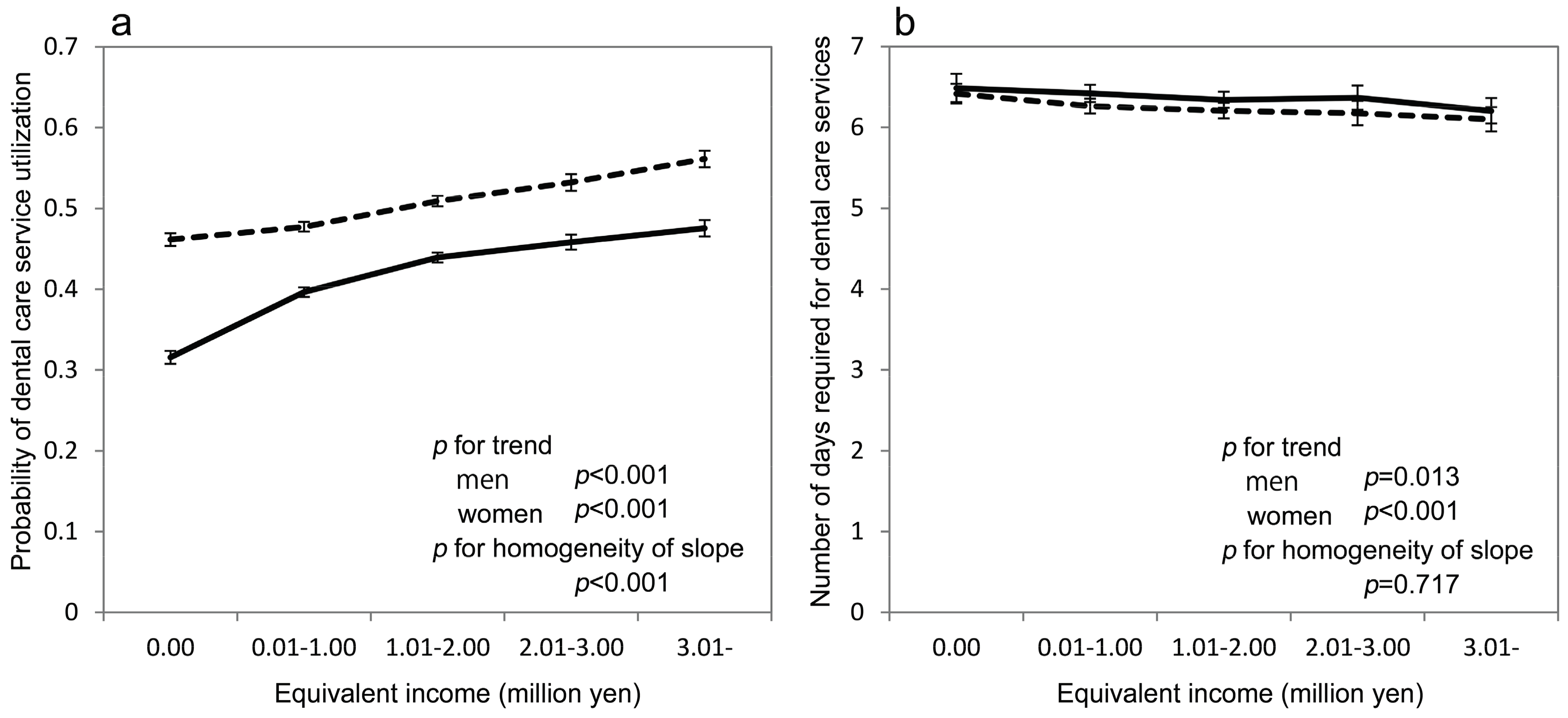
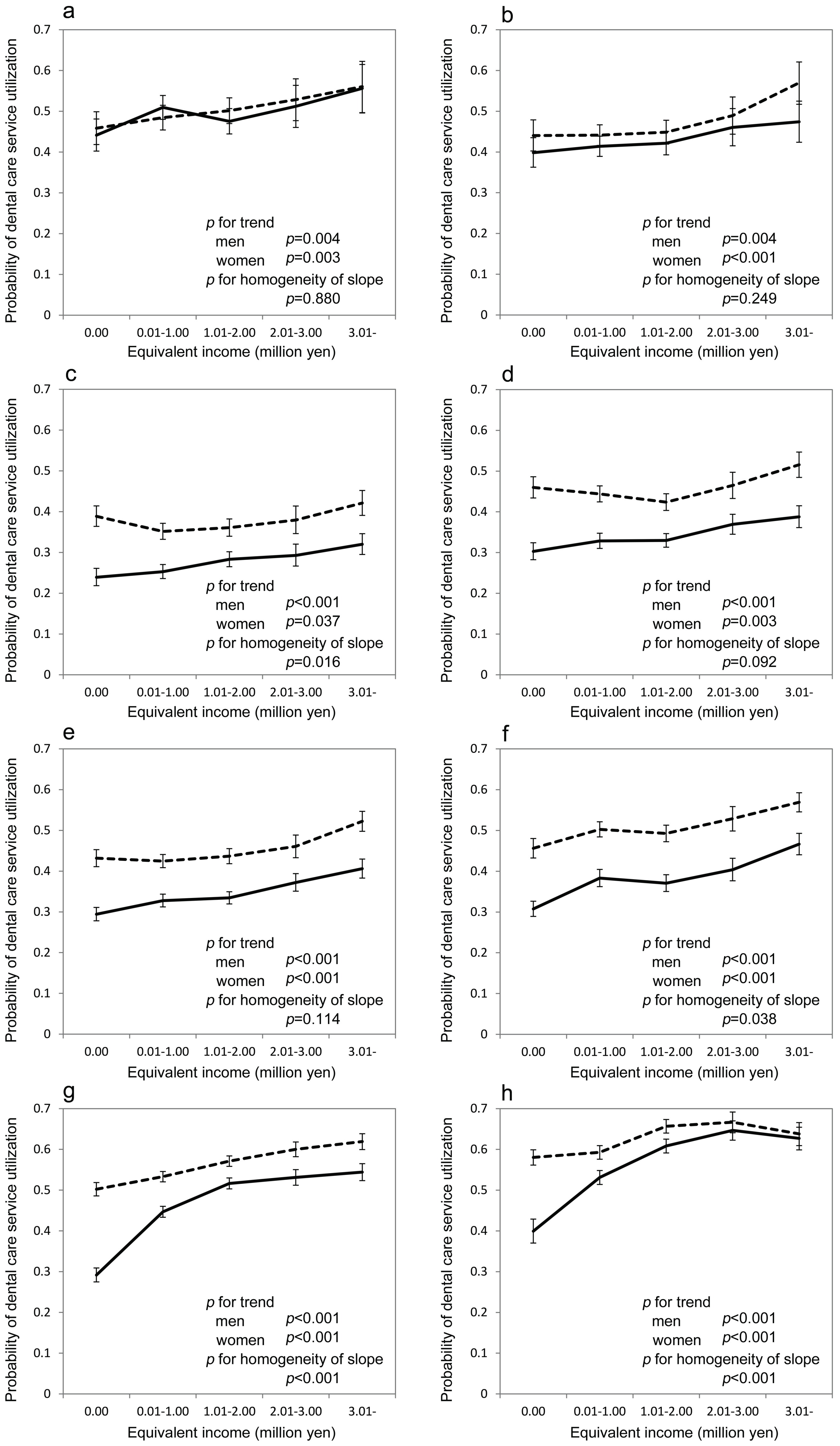
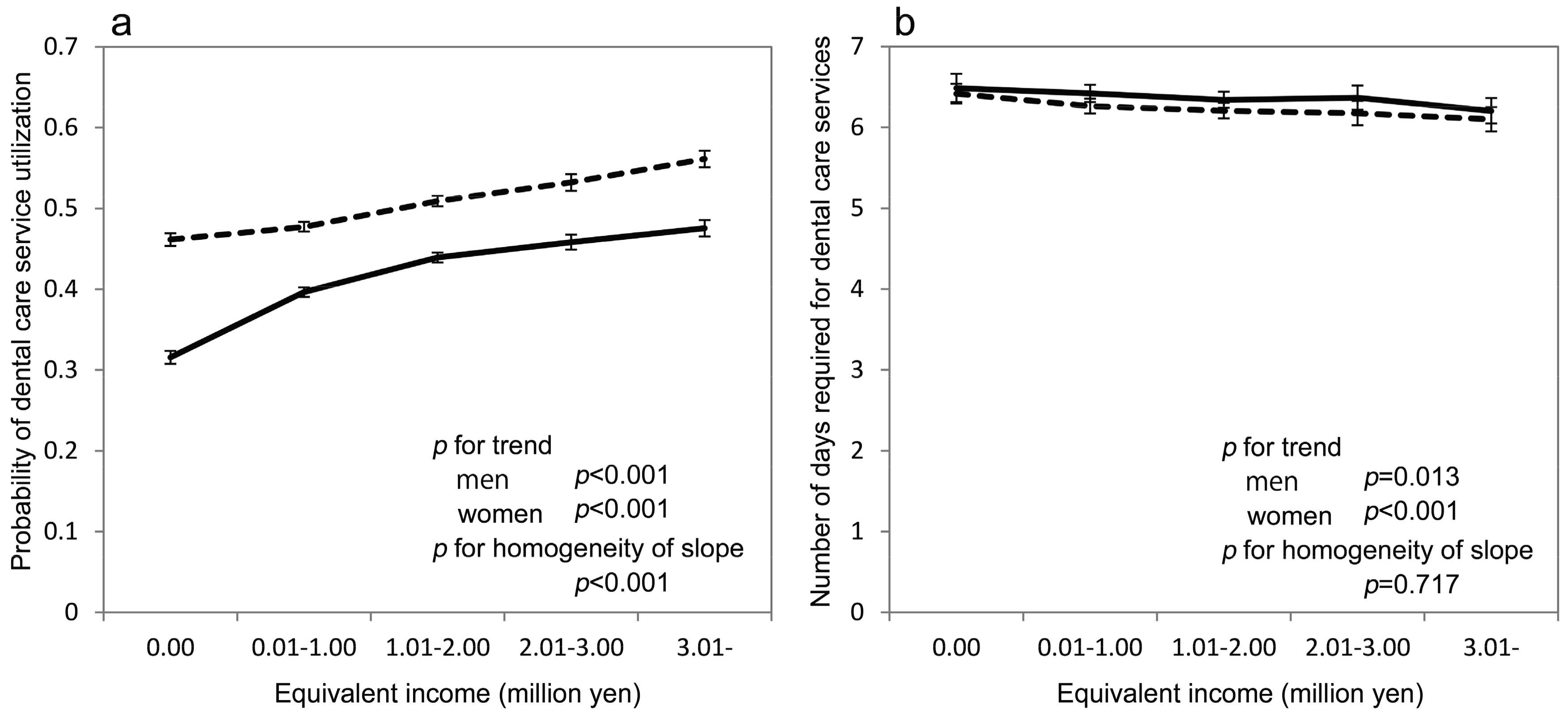
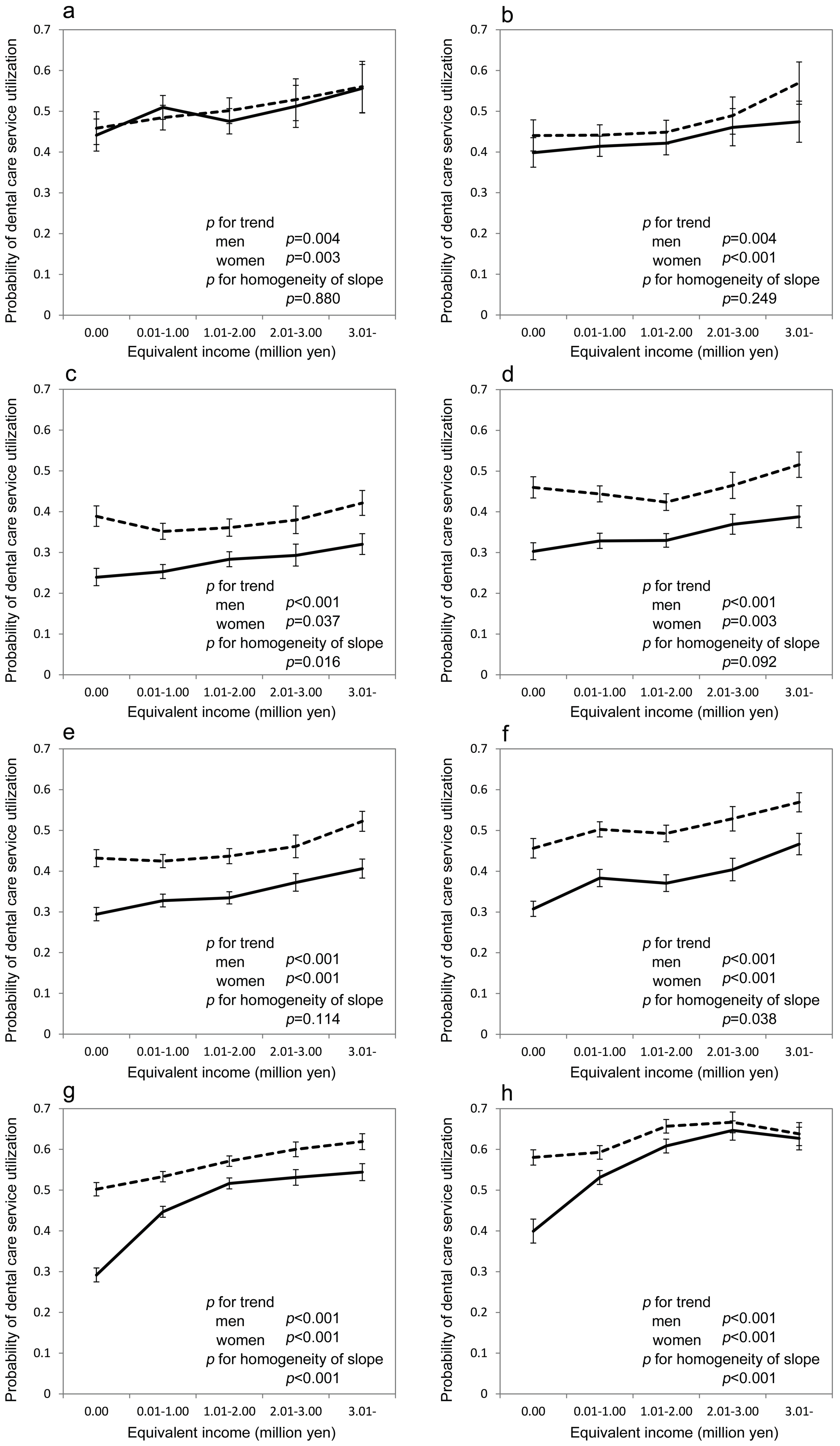
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Haugejorden, O.; Klock, K.S.; Astrom, A.N.; Skaret, E.; Trovik, T.A. Socio-economic inequality in the self-reported number of natural teeth among Norwegian adults—An analytical study. Community Dent. Oral Epidemiol. 2008, 36, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, Y.; Aida, J.; Takeuchi, K.; Tsakos, G.; Watt, R.G.; Kondo, K.; Osaka, K. Inequalities of dental prosthesis use under universal healthcare insurance. Community Dent. Oral Epidemiol. 2014, 42, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Schwendicke, F.; Dorfer, C.E.; Schlattmann, P.; Page, L.F.; Thomson, W.M.; Paris, S. Socioeconomic inequality and caries: A systematic review and meta-analysis. J. Dent. Res. 2015, 94, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Pattussi, M.P.; Peres, K.G.; Boing, A.F.; Peres, M.A.; da Costa, J.S.D. Self-rated oral health and associated factors in Brazilian elders. Community Dent. Oral Epidemiol. 2010, 38, 348–359. [Google Scholar] [CrossRef] [PubMed]
- Wamala, S.; Merlo, J.; Bostrom, G. Inequity in access to dental care services explains current socioeconomic disparities in oral health: The Swedish National surveys of Public Health 2004–2005. J. Epidemiol. Community Health 2006, 60, 1027–1033. [Google Scholar] [CrossRef] [PubMed]
- Grytten, J.; Holst, D.; Skau, I. Demand for and utilization of dental services according to household income in the adult population in Norway. Community Dent. Oral Epidemiol. 2012, 40, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Aida, J.; Ohkubo, T.; Hashimoto, H. Income-related inequalities in preventive and curative dental care use among working-age Japanese adults in urban areas: A cross-sectional study. BMC Oral Health 2014, 14, 117. [Google Scholar] [CrossRef] [PubMed]
- Listl, S. Income-related inequalities in dental service utilization by Europeans aged 50+. J. Dent. Res. 2011, 90, 717–723. [Google Scholar] [CrossRef] [PubMed]
- Hjern, A.; Grindefjord, M.; Sundberg, H.; Rosen, M. Social inequality in oral health and use of dental care in Sweden. Community Dent. Oral Epidemiol. 2001, 29, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Larson, K.; Halfon, N. Family income gradients in the health and health care access of US children. Matern. Child. Health J. 2010, 14, 332–342. [Google Scholar] [CrossRef] [PubMed]
- Tchicaya, A.; Lorentz, N. Socioeconomic inequalities in the non-use of dental care in Europe. Int. J. Equity Health 2014, 13, 7. [Google Scholar] [CrossRef] [PubMed]
- Ikegami, N.; Yoo, B.K.; Hashimoto, H.; Matsumoto, M.; Ogata, H.; Babazono, A.; Watanabe, R.; Shibuya, K.; Yang, B.M.; Reich, M.R.; et al. Japanese universal health coverage: Evolution, achievements, and challenges. Lancet 2011, 378, 1106–1115. [Google Scholar] [CrossRef]
- Fujita, M.; Sato, Y.; Nagashima, K.; Takahashi, S.; Hata, A. Income related inequality of health care access in Japan: A retrospective cohort study. PloS ONE 2016, 11, e0151690. [Google Scholar] [CrossRef] [PubMed]
- Organisation for Economic Co-Operation and Development. Terms of Reference OECD Project on the Distribution of Household Incomes 2014/15 Collection. Available online: http://www.oecd.org/statistics/data-collection/Income%20distribution_guidelines.pdf (accessed on 28 September 2016).
- Hanley, J.A.; Negassa, A.; deB Edwardes, M.D.; Forrester, J.E. Statistical analysis of correlated data using generalized estimating equations: An orientation. Am. J. Epidemiol. 2003, 157, 364–375. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, K.; Kawakami, N.; Yamaoka, K.; Ishikawa, H.; Hashimoto, H. The impact of subjective and objective social status on psychological distress among men and women in Japan. Soc. Sci. Med. 2010, 70, 1832–1839. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. Table of International Classification of Diseases for the Use of Social Insurance. Available online: http://www.mhlw.go.jp/bunya/iryouhoken/database/zenpan/shobyo_bunrui.html (accessed on 11 August 2016).
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 10th Revision-WHO Version for 2016. Available online: http://apps.who.int/classifications/icd10/browse/2016/en (accessed on 15 March 2017).
- Vikum, E.; Krokstad, S.; Holst, D.; Westin, S. Socioeconomic inequalities in dental services utilisation in a Norwegian county: The third Nord-Trondelag Health Survey. Scand. J. Public Health 2012, 40, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Somkotra, T.; Detsomboonrat, P. Is there equity in oral healthcare utilization: Experience after achieving Universal Coverage. Community Dent. Oral Epidemiol. 2009, 37, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Raittio, E.; Kiiskinen, U.; Helminen, S.; Aromaa, A.; Suominen, A.L. Income-related inequality and inequity in the use of dental services in Finland after a major subsidization reform. Community Dent. Oral Epidemiol. 2015, 43, 240–254. [Google Scholar] [CrossRef] [PubMed]
- Palència, L.; Espelt, A.; Cornejo-Ovalle, M.; Borrell, C. Socioeconomic inequalities in the use of dental care services in Europe: What is the role of public coverage? Community Dent. Oral Epidemiol. 2014, 42, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Elstad, J.I. Dental care coverage and income-related inequalities in foregone dental care in Europe during the great recession. Community Dent. Oral Epidemiol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Hirai, H.; Kondo, K.; Kawachi, I. Social Determinants of Active Aging: Differences in Mortality and the Loss of Healthy Life between Different Income Levels among Older Japanese in the AGES Cohort Study. Curr. Gerontol. Geriatr. Res. 2012, 2012, 9. [Google Scholar] [CrossRef] [PubMed]
- Macek, M.D.; Haynes, D.; Wells, W.; Bauer-Leffler, S.; Cotton, P.A.; Parker, R.M. Measuring conceptual Health knowledge in the context of oral health literacy: Preliminary results. J. Public Health Dent. 2010, 70, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Kullgren, J.T.; McLaughlin, C.G.; Mitra, N.; Armstrong, K. Nonfinancial barriers and access to care for U.S. adults. Health Serv. Res. 2012, 47, 462–485. [Google Scholar] [CrossRef] [PubMed]
- Green, C.A.; Pope, C.R. Gender, psychosocial factors and the use of medical services: A longitudinal analysis. Soc. Sci. Med. 1999, 48, 1363–1372. [Google Scholar] [CrossRef]
- Kawamura, M.; Allan, F.; Wright, C.; Sasahara, H.; Yamasaki, Y.; Suh, S.; Iwamoto, Y. An analytical study on gender differences in self-reported oral health care and problems of Japanese employees. J. Occup. Health 1999, 41, 104–111. [Google Scholar] [CrossRef]
- Widström, E.; Seppälä, T. Willingness and ability to pay for unexpected dental expenses by Finnish adults. BMC Oral Health 2012, 12, 35. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variables | Equivalent Income (Million Yen) 3 | |||||||
|---|---|---|---|---|---|---|---|---|
| All | 0.00 | 0.01–1.00 | 1.01–2.00 | 2.01–3.00 | ≥3.01 | p-Value | p-Value for Trend | |
| Number of subjects | 216,211 | 37,918 | 70,575 | 63,303 | 23,162 | 21,253 | ||
| Men (%) 1 | 105,269 (48.7) | 16,674 (44.0) | 33,083 (46.9) | 32,292 (51.0) | 12,553 (54.2) | 10,667 (50.2) | <0.001 | <0.001 |
| Age 2 | 53.0 (19.8) | 51.4 (19.3) | 54.6 (20.0) | 54.1 (19.9) | 51.3 (19.6) | 49.6 (18.7) | <0.001 | <0.001 |
| Number of Family Members 1 | ||||||||
| 1 or 2 (%) | 154,222 (71.3) | 32,494 (85.7) | 49,698 (70.4) | 43,133 (68.1) | 152,04 (65.6) | 13,693 (64.4) | <0.001 | |
| 3 (%) | 35,299 (16.3) | 3260 (8.6) | 12,547 (17.8) | 11,120 (17.6) | 4472 (19.3) | 3900 (18.4) | ||
| 4 and more | 26,690 (12.3) | 2164 (5.7) | 8330 (11.8) | 9050 (14.3) | 3486 (15.1) | 3660 (17.2) | ||
| Residual Area 1 | ||||||||
| Chuo (%) | 43,349 (20.1) | 8691 (22.9) | 13,577 (19.2) | 11,883 (18.8) | 4702 (20.3) | 4496 (21.2) | <0.001 | |
| Hanamigawa (%) | 40,345 (18.7) | 6950 (18.3) | 13,449 (19.1) | 11,801 (18.6) | 4160 (18.0) | 3985 (18.8) | ||
| Inage (%) | 34,699 (16.1) | 5854 (15.4) | 11,087 (15.7) | 10,396 (16.4) | 3697 (16.0) | 3665 (17.2) | ||
| Wakaba (%) | 40,584 (18.8) | 7669 (20.2) | 13,026 (18.5) | 11,835 (18.7) | 4449 (19.2) | 3605 (17.0) | ||
| Midori (%) | 25,645 (11.9) | 3857 (10.2) | 8497 (12.0) | 7805 (12.3) | 2852 (12.3) | 2634 (12.4) | ||
| Mihama (%) | 31,589 (14.6) | 4897 (12.9) | 10,939 (15.5) | 9583 (15.1) | 3302.(14.3) | 2868 (13.5) | ||
| Users of dental care services 1 | 108,689 (50.3) | 16,471 (43.4) | 35,304 (50.0) | 33,418 (52.8) | 12,173 (52.6) | 11,323 (53.3) | <0.001 | <0.001 |
| The number of days for dental care services 2 | 7.7 (7.1) | 7.8 (7.2) | 7.8 (7.2) | 7.7 (7.0) | 7.5 (7.0) | 7.3 (6.8) | <0.001 | <0.001 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishide, A.; Fujita, M.; Sato, Y.; Nagashima, K.; Takahashi, S.; Hata, A. Income-Related Inequalities in Access to Dental Care Services in Japan. Int. J. Environ. Res. Public Health 2017, 14, 524. https://doi.org/10.3390/ijerph14050524
Nishide A, Fujita M, Sato Y, Nagashima K, Takahashi S, Hata A. Income-Related Inequalities in Access to Dental Care Services in Japan. International Journal of Environmental Research and Public Health. 2017; 14(5):524. https://doi.org/10.3390/ijerph14050524
Chicago/Turabian StyleNishide, Akemi, Misuzu Fujita, Yasunori Sato, Kengo Nagashima, Sho Takahashi, and Akira Hata. 2017. "Income-Related Inequalities in Access to Dental Care Services in Japan" International Journal of Environmental Research and Public Health 14, no. 5: 524. https://doi.org/10.3390/ijerph14050524