Antibiotic Resistance and Antibiotic Resistance Genes in Escherichia coli Isolates from Hospital Wastewater in Vietnam

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Collection of Water Samples
2.2. Antibacterial Susceptibility Testing and Detection of ARGs
2.3. Data Analysis
3. Results
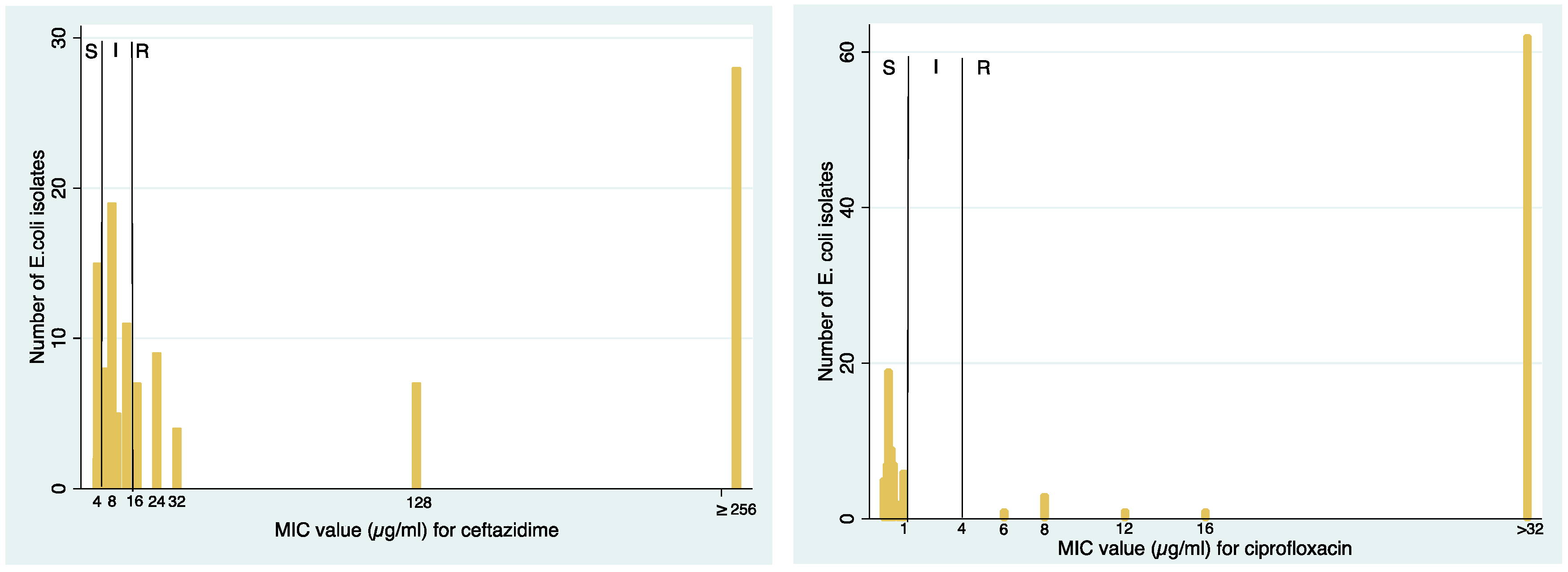
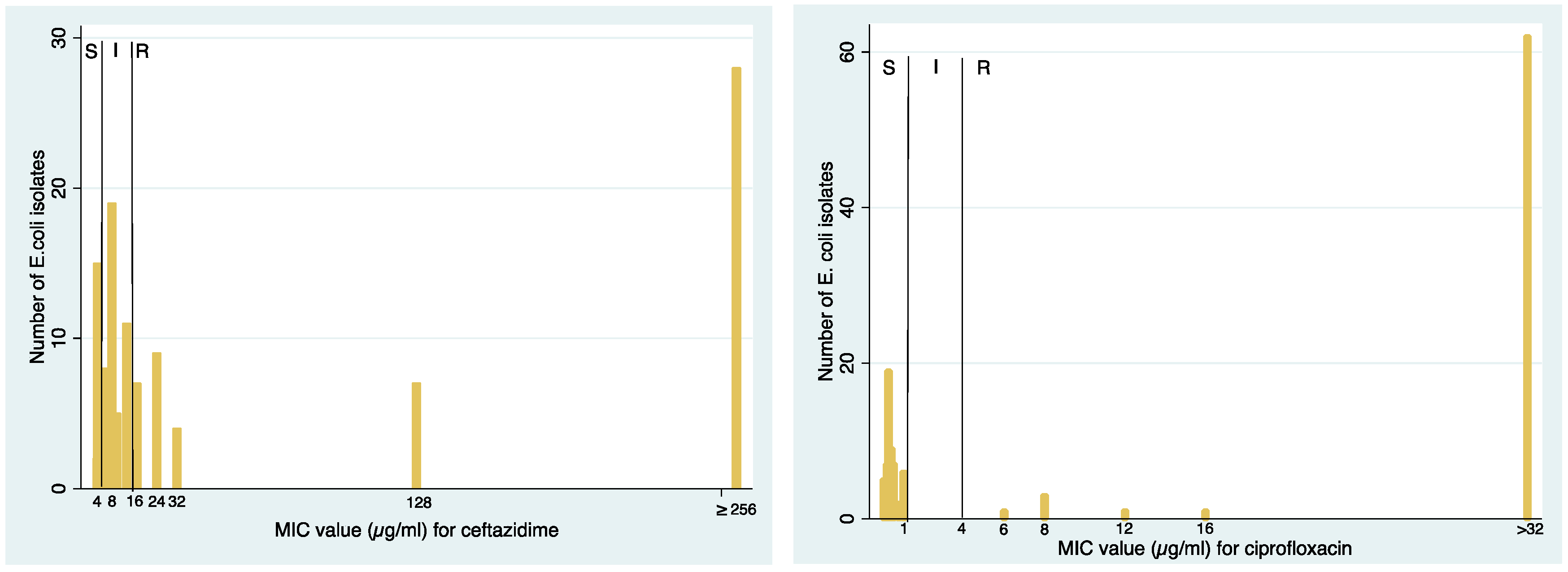
3.1. Resistance to Studied Antibiotics
3.2. ESBL-Producing E. coli, ESBL, and Quinolone Resistance Genes
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Williams, M.R.; Stedtfeld, R.D.; Guo, X.; Hashsham, S.A. Antimicrobial resistance in the environment. Water Environ. Res. 2016, 88, 1951–1967. [Google Scholar] [CrossRef] [PubMed]
- Berendonk, T.U.; Manaia, C.M.; Merlin, C.; Fatta-Kassinos, D.; Cytryn, E.; Walsh, F.; Burgmann, H.; Sorum, H.; Norstrom, M.; Pons, M.N.; et al. Tackling antibiotic resistance: The environmental framework. Nat. Rev. Microbiol. 2015, 13, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Verlicchi, P.; Al Aukidy, M.; Galletti, A.; Petrovic, M.; Barceló, D. Hospital effluent: Investigation of the concentrations and distribution of pharmaceuticals and environmental risk assessment. Sci. Total Environ. 2012, 430, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Lien, L.T.; Hoa, N.Q.; Chuc, N.T.; Thoa, N.T.; Phuc, H.D.; Diwan, V.; Dat, N.T.; Tamhankar, A.J.; Lundborg, C.S. Antibiotics in Wastewater of a Rural and an Urban Hospital before and after Wastewater Treatment, and the Relationship with Antibiotic Use-A One Year Study from Vietnam. Int. J. Environ. Res. Public Health 2016, 13, 558. [Google Scholar] [CrossRef] [PubMed]
- Guenther, S.; Ewers, C.; Wieler, L.H. Extended-Spectrum Beta-Lactamases Producing E. coli in Wildlife, yet Another Form of Environmental Pollution? Front. Microbiol. 2011, 2, 246. [Google Scholar] [CrossRef] [PubMed]
- Drieux, L.; Haenn, S.; Moulin, L.; Jarlier, V. Quantitative evaluation of extended-spectrum beta-lactamase-producing Escherichia coli strains in the wastewater of a French teaching hospital and relation to patient strain. Antimicrob. Resist. Infect. Control 2016, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Antibiotic Resistance: Global Report on Surveillance 2014; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Chandy, S.J.; Naik, G.S.; Balaji, V.; Jeyaseelan, V.; Thomas, K.; Lundborg, C.S. High cost burden and health consequences of antibiotic resistance: The price to pay. J. Infect. Dev. Ctries. 2014, 8, 1096–1102. [Google Scholar] [CrossRef] [PubMed]
- Alsan, M.; Schoemaker, L.; Eggleston, K.; Kammili, N.; Kolli, P.; Bhattacharya, J. Out-of-pocket health expenditures and antimicrobial resistance in low-income and middle-income countries: An economic analysis. Lancet Infect. Dis. 2015, 15, 1203–1210. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Global Action Plan on Antimicrobial Resistance; WHO: Geneva, Switzeland, 2015. [Google Scholar]
- World Health Organization (WHO). Worldwide Country Situation Analysis: Response to Antimicrobial Resistance; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Velez, R.; Sloand, E. Combating antibiotic resistance, mitigating future threats and ongoing initiatives. J. Clin. Nurs. 2016, 25, 1886–1889. [Google Scholar] [CrossRef] [PubMed]
- Roca, I.; Akova, M.; Baquero, F.; Carlet, J.; Cavaleri, M.; Coenen, S.; Cohen, J.; Findlay, D.; Gyssens, I.; Heuer, O.E.; et al. The global threat of antimicrobial resistance: Science for intervention. New Microbes New Infect. 2015, 6, 22–29. [Google Scholar] [CrossRef] [PubMed]
- General Assembly of the United Nations. PRESS RELEASE: High-Level Meeting on Antimicrobial Resistance. Available online: http://www.un.org/pga/71/2016/09/21/press-release-hl-meeting-on-antimicrobial-resistance/ (accessed on 7 November 2016).
- Hocquet, D.; Muller, A.; Bertrand, X. What happens in hospitals does not stay in hospitals: Antibiotic-resistant bacteria in hospital wastewater systems. J. Hosp. Infect. 2016, 93, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Talaro, K.P.; Talaro, A. Foundations in Microbiology, 4th ed.; The McGraw−Hill Companies: Boston, MA, USA, 2002; pp. 799–813. [Google Scholar]
- Cinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Disk Susceptibility Tests. Approved Standard-Eleventh Edition; CLSI: Wayne, PA, USA, 2012. [Google Scholar]
- EUCAST Antimicrobial Wild Type Distributions of Microorganisms. Available online: http://mic.eucast.org/Eucast2/SearchController/search.jsp?action=performSearch&BeginIndex=0&Micdif=dif&NumberIndex50&Antib=−1&Specium=162 (accessed on 2 December 2016).
- Dallenne, C.; Da Costa, A.; Decre, D.; Favier, C.; Arlet, G. Development of a set of multiplex PCR assays for the detection of genes encoding important beta-lactamases in Enterobacteriaceae. J. Antimicrob. Chemother. 2010, 65, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Le, T.M.; Baker, S.; Le, T.P.; Cao, T.T.; Tran, T.T.; Nguyen, V.M.; Campbell, J.I.; Lam, M.Y.; Nguyen, T.H.; et al. High prevalence of plasmid-mediated quinolone resistance determinants in commensal members of the Enterobacteriaceae in Ho Chi Minh City, Vietnam. J. Méd. Microbiol. 2009, 58, 1585–1592. [Google Scholar] [PubMed]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed]
- Duong, H.A.; Pham, N.H.; Nguyen, H.T.; Hoang, T.T.; Pham, H.V.; Pham, V.C.; Berg, M.; Giger, W.; Alder, A.C. Occurrence, fate and antibiotic resistance of fluoroquinolone antibacterials in hospital wastewaters in Hanoi, Vietnam. Chemosphere 2008, 72, 968–973. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.Z.; Aqil, F.; Ahmad, I.; Ahmad, S. Incidence and transferability of antibiotic resistance in the enteric bacteria isolated from hospital wastewater. Braz. J. Microbiol. 2013, 44, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Korzeniewska, E.; Korzeniewska, A.; Harnisz, M. Antibiotic resistant Escherichia coli in hospital and municipal sewage and their emission to the environment. Ecotoxicol. Environ. Saf. 2013, 91, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Huovinen, P. Resistance to trimethoprim-sulfamethoxazole. Clin. Infect. Dis. 2001, 32, 1608–1614. [Google Scholar] [PubMed]
- Chagas, T.P.; Seki, L.M.; Cury, J.C.; Oliveira, J.A.; Davila, A.M.; Silva, D.M.; Asensi, M.D. Multiresistance, beta-lactamase-encoding genes and bacterial diversity in hospital wastewater in Rio de Janeiro, Brazil. J. Appl. Microbiol. 2011, 111, 572–581. [Google Scholar] [CrossRef] [PubMed]
- Rawat, D.; Nair, D. Extended-spectrum β-lactamases in Gram Negative Bacteria. J. Glob. Infect. Dis. 2010, 2, 263–274. [Google Scholar] [CrossRef] [PubMed]
- Bush, K. Characterization of beta-lactamases. Antimicrob. Agents Chemother. 1989, 33, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.; Castillo, G.; Callejas, L.; Lopez, H.; Olmos, J. Frequency of transferable multiple antibiotic resistance amongst coliform bacteria isolated from a treated sewage effluent in Antofagasta, Chile. Electron. J. Biotechnol. 2006, 5, 533–540. [Google Scholar] [CrossRef]
- Brun-Buisson, C.; Legrand, P.; Philippon, A.; Montravers, F.; Ansquer, M.; Duval, J. Transferable enzymatic resistance to third-generation cephalosporins during nosocomial outbreak of multiresistant Klebsiella pneumoniae. Lancet 1987, 2, 302–306. [Google Scholar] [CrossRef]
- Chandran, S.P.; Diwan, V.; Tamhankar, A.J.; Joseph, B.V.; Rosales-Klintz, S.; Mundayoor, S.; Lundborg, C.S.; Macaden, R. Detection of carbapenem resistance genes and cephalosporin, and quinolone resistance genes along with oqxAB gene in Escherichia coli in hospital wastewater: A matter of concern. J. Appl. Microbiol. 2014, 117, 984–995. [Google Scholar] [CrossRef] [PubMed]
- Diwan, V.; Chandran, S.P.; Tamhankar, A.J.; Lundborg, C.S.; Macaden, R. Identification of extended-spectrum -lactamase and quinolone resistance genes in Escherichia coli isolated from hospital wastewater from central India. J. Antimicrob. Chemother. 2012, 67, 857–859. [Google Scholar] [CrossRef] [PubMed]
- Abdulhaq, A.; Basode, V.K. Prevalence of extended-spectrum beta-lactamase-producing bacteria in hospital and community sewage in Saudi Arabia. Am. J. Infect. Control 2015, 43, 1139–1141. [Google Scholar] [CrossRef] [PubMed]
- Bush, K.; Jacoby, G.A. Updated functional classification of beta-lactamases. Antimicrob. Agents Chemother. 2010, 54, 969–976. [Google Scholar] [CrossRef] [PubMed]
- Varela, A.R.; Macedo, G.N.; Nunes, O.C.; Manaia, C.M. Genetic characterization of fluoroquinolone resistant Escherichia coli from urban streams and municipal and hospital effluents. FEMS Microbiol. Ecol. 2015, 91. [Google Scholar] [CrossRef] [PubMed]
- Yamane, K.; Wachino, J.; Suzuki, S.; Arakawa, Y. Plasmid-mediated qepA gene among Escherichia coli clinical isolates from Japan. Antimicrob. Agents Chemother. 2008, 52, 1564–1566. [Google Scholar] [CrossRef] [PubMed]
- Alrowais, H.; McElheny, C.L.; Spychala, C.N.; Sastry, S.; Guo, Q.; Butt, A.A.; Doi, Y. Fosfomycin Resistance in Escherichia coli, Pennsylvania, USA. Emerg. Infect. Dis. 2015, 21, 2045–2047. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J.R.; Betts, M.J. Carbapenems: The pinnacle of the β-lactam antibiotics or room for improvement? J. Antimicrob. Chemother. 2000, 45, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Le, N.K.; Wertheim, H.F.; Vu, P.D.; Khu, D.T.; Le, H.T.; Hoang, B.T.; Vo, V.T.; Lam, Y.M.; Vu, D.T.; Nguyen, T.H.; et al. High prevalence of hospital-acquired infections caused by gram-negative carbapenem resistant strains in Vietnamese pediatric ICUs: A multi-centre point prevalence survey. Medicine 2016, 95, e4099. [Google Scholar] [CrossRef] [PubMed]
- Laffite, A.; Kilunga, P.I.; Kayembe, J.M.; Devarajan, N.; Mulaji, C.K.; Giuliani, G.; Slaveykova, V.I.; Pote, J. Hospital Effluents Are One of Several Sources of Metal, Antibiotic Resistance Genes, and Bacterial Markers Disseminated in Sub-Saharan Urban Rivers. Front. Microbiol. 2016, 7, 1128. [Google Scholar] [CrossRef] [PubMed]
- Mandal, S.M.; Ghosh, A.K.; Pati, B.R. Dissemination of antibiotic resistance in methicillin-resistant Staphylococcus aureus and vancomycin-resistant S. aureus strains isolated from hospital effluents. Am. J. Infect. Control 2015, 43, e87–e88. [Google Scholar] [CrossRef] [PubMed]
- Ory, J.; Bricheux, G.; Togola, A.; Bonnet, J.L.; Donnadieu-Bernard, F.; Nakusi, L.; Forestier, C.; Traore, O. Ciprofloxacin residue and antibiotic-resistant biofilm bacteria in hospital effluent. Environ. Pollut. 2016, 214, 635–645. [Google Scholar] [CrossRef] [PubMed]
- Roderova, M.; Sedlakova, M.H.; Pudova, V.; Hricova, K.; Silova, R.; Imwensi, P.E.; Bardon, J.; Kolar, M. Occurrence of bacteria producing broad-spectrum beta-lactamases and qnr genes in hospital and urban wastewater samples. New Microbiol. 2016, 39, 124–133. [Google Scholar] [PubMed]
- Santoro, D.O.; Cardoso, A.M.; Coutinho, F.H.; Pinto, L.H.; Vieira, R.P.; Albano, R.M.; Clementino, M.M. Diversity and antibiotic resistance profiles of Pseudomonads from a hospital wastewater treatment plant. J. Appl. Microbiol. 2015, 119, 1527–1540. [Google Scholar] [CrossRef] [PubMed]
- Varela, A.R.; Nunes, O.C.; Manaia, C.M. Quinolone resistant Aeromonas spp. as carriers and potential tracers of acquired antibiotic resistance in hospital and municipal wastewater. Sci. Total Environ. 2016, 542, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Vaz-Moreira, I.; Varela, A.R.; Pereira, T.V.; Fochat, R.C.; Manaia, C.M. Multidrug Resistance in Quinolone-Resistant Gram-Negative Bacteria Isolated from Hospital Effluent and the Municipal Wastewater Treatment Plant. Microb. Drug Resist. 2016, 22, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Anssour, L.; Messai, Y.; Estepa, V.; Torres, C.; Bakour, R. Characteristics of ciprofloxacin-resistant Enterobacteriaceae isolates recovered from wastewater of an Algerian hospital. J. Infect. Dev. Ctries. 2016, 10, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Lu, J.; Liu, J.; Zhang, G.; Tong, Y.; Ma, N. Exploring the correlations between antibiotics and antibiotic resistance genes in the wastewater treatment plants of hospitals in Xinjiang, China. Environ. Sci. Pollut. Res. Int. 2016, 23, 15111–15121. [Google Scholar] [CrossRef] [PubMed]
- Harris, S.; Morris, C.; Morris, D.; Cormican, M.; Cummins, E. Antimicrobial resistant Escherichia coli in the municipal wastewater system: Effect of hospital effluent and environmental fate. Sci. Total Environ. 2014, 468–469, 1078–1085. [Google Scholar] [CrossRef] [PubMed]
- Iweriebor, B.C.; Gaqavu, S.; Obi, L.C.; Nwodo, U.U.; Okoh, A.I. Antibiotic susceptibilities of enterococcus species isolated from hospital and domestic wastewater effluents in alice, eastern cape province of South Africa. Int. J. Environ. Res. Public Health 2015, 12, 4231–4246. [Google Scholar] [CrossRef] [PubMed]
- Galvin, S.; Boyle, F.; Hickey, P.; Vellinga, A.; Morris, D.; Cormican, M. Enumeration and Characterization of Antimicrobial-Resistant Escherichia coli Bacteria in Effluent from Municipal, Hospital, and Secondary Treatment Facility Sources. Appl. Environ. Microbiol. 2010, 76, 4772–4779. [Google Scholar] [CrossRef] [PubMed]
- Ferreira da Silva, M.; Vaz-Moreira, I.; Gonzalez-Pajuelo, M.; Nunes, O.C.; Manaia, C.M. Antimicrobial resistance patterns in Enterobacteriaceae isolated from an urban wastewater treatment plant. FEMS Microbiol. Ecol. 2007, 60, 166–176. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, L.; Manaia, C.; Merlin, C.; Schwartz, T.; Dagot, C.; Ploy, M.C.; Michael, I.; Fatta-Kassinos, D. Urban wastewater treatment plants as hotspots for antibiotic resistant bacteria and genes spread into the environment: A review. Sci. Total Environ. 2013, 447, 345–360. [Google Scholar] [CrossRef] [PubMed]
- Nagulapally, S.R.; Ahmad, A.; Henry, A.; Marchin, G.L.; Zurek, L.; Bhandari, A. Occurrence of ciprofloxacin-, trimethoprim-sulfamethoxazole-, and vancomycin-resistant bacteria in a municipal wastewater treatment plant. Water Environ. Res. 2009, 81, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg Goldstein, R.E.; Micallef, S.A.; Gibbs, S.G.; George, A.; Claye, E.; Sapkota, A.; Joseph, S.W.; Sapkota, A.R. Detection of vancomycin-resistant enterococci (VRE) at four U.S. wastewater treatment plants that provide effluent for reuse. Sci. Total Environ. 2014, 466–467, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Maheshwari, M.; Yaser, N.H.; Naz, S.; Fatima, M.; Ahmad, I. Emergence of ciprofloxacin-resistant extended-spectrum beta-lactamase-producing enteric bacteria in hospital wastewater and clinical sources. J. Glob. Antimicrob. Resist. 2016, 5, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Huijbers, P.M.; Blaak, H.; de Jong, M.C.; Graat, E.A.; Vandenbroucke-Grauls, C.M.; de Roda Husman, A.M. Role of the Environment in the Transmission of Antimicrobial Resistance to Humans: A Review. Environ. Sci. Technol. 2015, 49, 11993–12004. [Google Scholar] [CrossRef] [PubMed]
- Hower, S.; Phillips, M.C.; Brodsky, M.; Dameron, A.; Tamargo, M.A.; Salazar, N.C.; Jackson, C.R.; Barrett, J.B.; Davidson, M.; Davis, J.; et al. Clonally related methicillin-resistant Staphylococcus aureus isolated from short-finned pilot whales (Globicephala macrorhynchus), human volunteers, and a bayfront cetacean rehabilitation facility. Microb. Ecol. 2013, 65, 1024–1038. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Studied Antibiotics | Rural Hospital (n = 158) | Urban Hospital (n = 107) | Both Hospitals (n = 265) Overall (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| WBT (%) n = 84 | WAT (%) n = 74 | p-Value | Overall (%) | WBT (%) n = 60 | WAT (%) n = 47 | p-Value | Overall (%) | ||
| Amoxicillin/clavulanic acid | 51 | 24 | 0.001 * | 39 | 28 | 19 | 0.36 | 24 | 33 |
| Ceftazidime | 42 | 36 | 0.52 | 39 | 32 | 23 | 0.40 | 28 | 35 |
| Ceftriaxone | 55 | 42 | 0.11 | 49 | 45 | 32 | 0.23 | 39 | 45 |
| Ciprofloxacin | 25 | 35 | 0.22 | 30 | 23 | 17 | 0.50 | 21 | 26 |
| Co-trimoxazole | 86 | 53 | <0.001 * | 70 | 80 | 60 | 0.03 * | 71 | 70 |
| Fosfomycin | 1 | 3 | 0.60 | 2 | 15 | 0 | 0.005 * | 8 | 4 |
| Gentamycin | 51 | 31 | 0.02 * | 42 | 33 | 23 | 0.30 | 29 | 37 |
| Imipenem | 1 | 0 | 1.00 | 1 | 0 | 0 | N/A | 0 | 1 |
| At least one antibiotic | 94 | 74 | 0.001 * | 85 | 88 | 68 | 0.02 * | 79 | 83 |
| MDR | 44 | 26 | 0.02 * | 35 | 32 | 21 | 0.30 | 27 | 32 |
| MDR Pattern | Rural Hospital (n = 158) | Urban Hospital (n = 107) | ||
|---|---|---|---|---|
| WBT | WAT | WBT | WAT | |
| CTX + CIP + SXT | 0 | 0 | 0 | 2 |
| CTX + GEN + SXT | 7 | 0 | 3 | 0 |
| AMC + GEN + SXT | 0 | 0 | 1 | 0 |
| GEN + CIP + SXT | 0 | 4 | 7 | 1 |
| CAZ + CTX + AMC + CIP | 2 | 0 | 0 | 0 |
| CAZ + CTX + AMC + SXT | 2 | 0 | 0 | 2 |
| CAZ + CTX + GEN + SXT | 6 | 0 | 1 | 0 |
| CAZ + CTX + CIP + SXT | 0 | 0 | 0 | 1 |
| CAZ + CTX + SXT + FOM | 1 | 0 | 0 | 0 |
| CTX + GEN + CIP + SXT | 4 | 1 | 2 | 0 |
| AMC + GEN + CIP + SXT | 0 | 1 | 0 | 1 |
| CAZ + CTX + GEN + CIP + SXT | 2 | 2 | 3 | 0 |
| CAZ + CTX + AMC + CIP + SXT | 0 | 1 | 0 | 0 |
| CTX + GEN + CIP + SXT + FOM | 0 | 1 | 0 | 0 |
| CTX + AMC + GEN + CIP + SXT | 1 | 0 | 0 | 0 |
| IMP + CAZ + CTX + AMC + SXT | 1 | 0 | 0 | 0 |
| CAZ + CTX + AMC + GEN + CIP + SXT | 11 | 9 | 1 | 3 |
| CAZ + CTX + AMC + GEN + CIP + FOM | 0 | 0 | 1 | 0 |
| Total (%) | 37 (44%) | 19 (26%) | 19 (32%) | 10 (21%) |
| 56 (35%) | 29 (27%) | |||
| Genetic Analysis | Rural Hospital | Urban Hospital | Both Hospitals | ||||
|---|---|---|---|---|---|---|---|
| WBT n (%) | WAT n (%) | Overall n (%) | WBT n (%) | WAT n (%) | Overall n (%) | Overall n (%) | |
| ESBL-producing | 45 (54) | 31 (42) | 76 (48) | 27 (45) | 12 (26) | 39 (36) | 115 (43) |
| blaCTX-M | 29 (64) | 29 (94) | 58 (76) | 14 (52) | 2 (17) | 16 (41) | 74 (64) |
| blaTEM | 44 (98) | 30 (97) | 74 (97) | 27 (100) | 10 (83) | 37 (95) | 111 (97) |
| blaCTX-M + blaTEM | 29 (64) | 28 (90) | 57 (75) | 14 (52) | 2 (17) | 16 (41) | 73 (63) |
| Ciprofloxacin resistance | 21 (25) | 26 (35) | 47 (30) | 14 (23) | 8 (17) | 22 (21) | 69 (26) |
| qepA | 14 (67) | 20 (77) | 34 (72) | 12 (86) | 7 (88) | 19 (86) | 53 (77) |
| qepA + blaCTX-M + blaTEM | 13 (62) | 11 (42) | 24 (51) | 6 (43) | 2 (25) | 8 (36) | 32 (46) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lien, L.T.Q.; Lan, P.T.; Chuc, N.T.K.; Hoa, N.Q.; Nhung, P.H.; Thoa, N.T.M.; Diwan, V.; Tamhankar, A.J.; Stålsby Lundborg, C. Antibiotic Resistance and Antibiotic Resistance Genes in Escherichia coli Isolates from Hospital Wastewater in Vietnam. Int. J. Environ. Res. Public Health 2017, 14, 699. https://doi.org/10.3390/ijerph14070699
Lien LTQ, Lan PT, Chuc NTK, Hoa NQ, Nhung PH, Thoa NTM, Diwan V, Tamhankar AJ, Stålsby Lundborg C. Antibiotic Resistance and Antibiotic Resistance Genes in Escherichia coli Isolates from Hospital Wastewater in Vietnam. International Journal of Environmental Research and Public Health. 2017; 14(7):699. https://doi.org/10.3390/ijerph14070699
Chicago/Turabian StyleLien, La Thi Quynh, Pham Thi Lan, Nguyen Thi Kim Chuc, Nguyen Quynh Hoa, Pham Hong Nhung, Nguyen Thi Minh Thoa, Vishal Diwan, Ashok J. Tamhankar, and Cecilia Stålsby Lundborg. 2017. "Antibiotic Resistance and Antibiotic Resistance Genes in Escherichia coli Isolates from Hospital Wastewater in Vietnam" International Journal of Environmental Research and Public Health 14, no. 7: 699. https://doi.org/10.3390/ijerph14070699