
The Effects of a Campus Forest-Walking Program on Undergraduate and Graduate Students’ Physical and Psychological Health

 ,
, 
Abstract
:1. Introduction
- The experimental group participating in the program will display a higher score on health promoting behaviors than the control group will.
- The experimental group will display a lower depression score than the control group will.
- The experimental group will display more parasympathetic nerve activity than the control group will.
- The physical health (i.e., bone density, blood lipid profile, and body mass index) of the experimental group will be better than that of the control group.
2. Methods
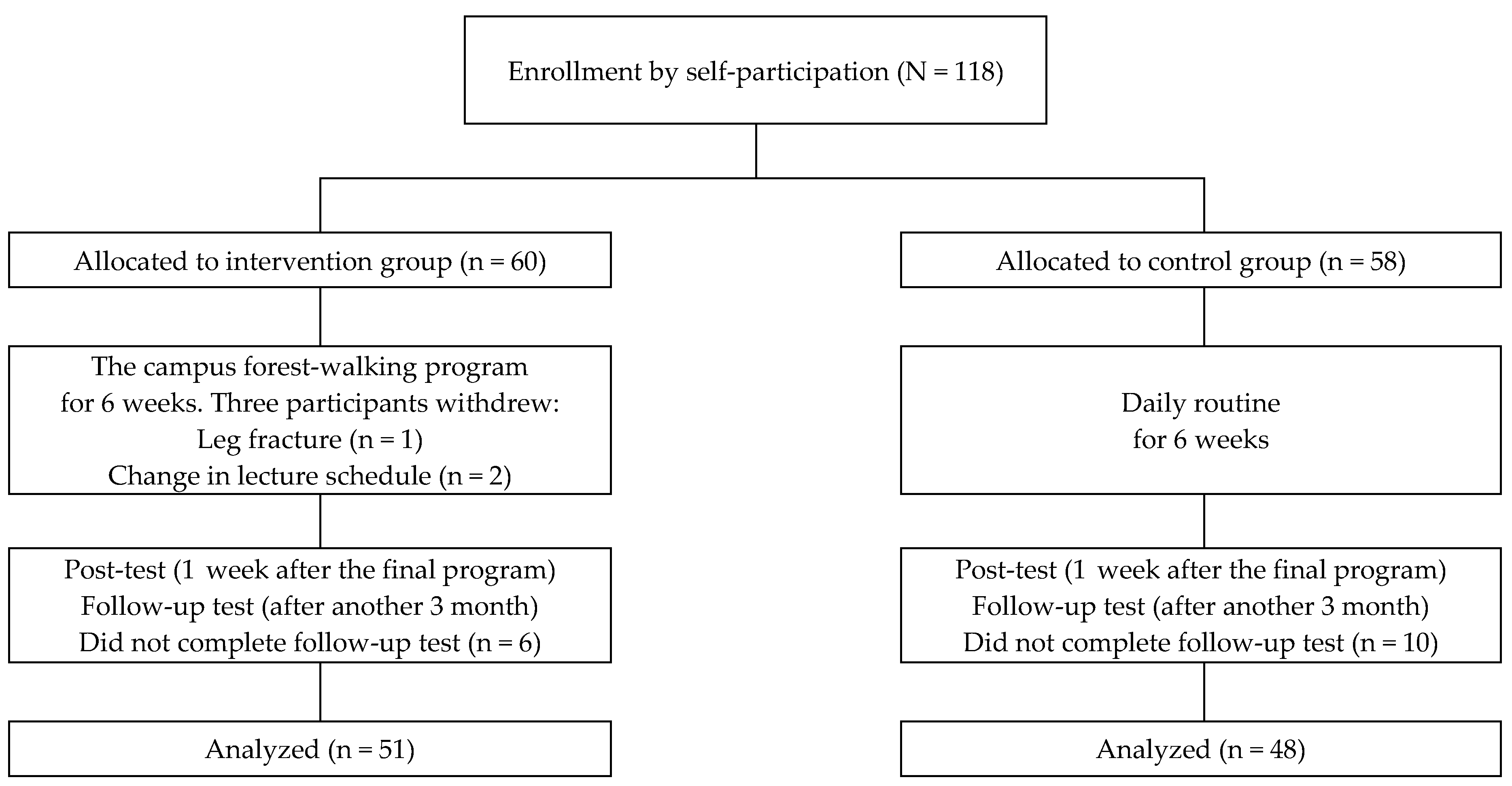
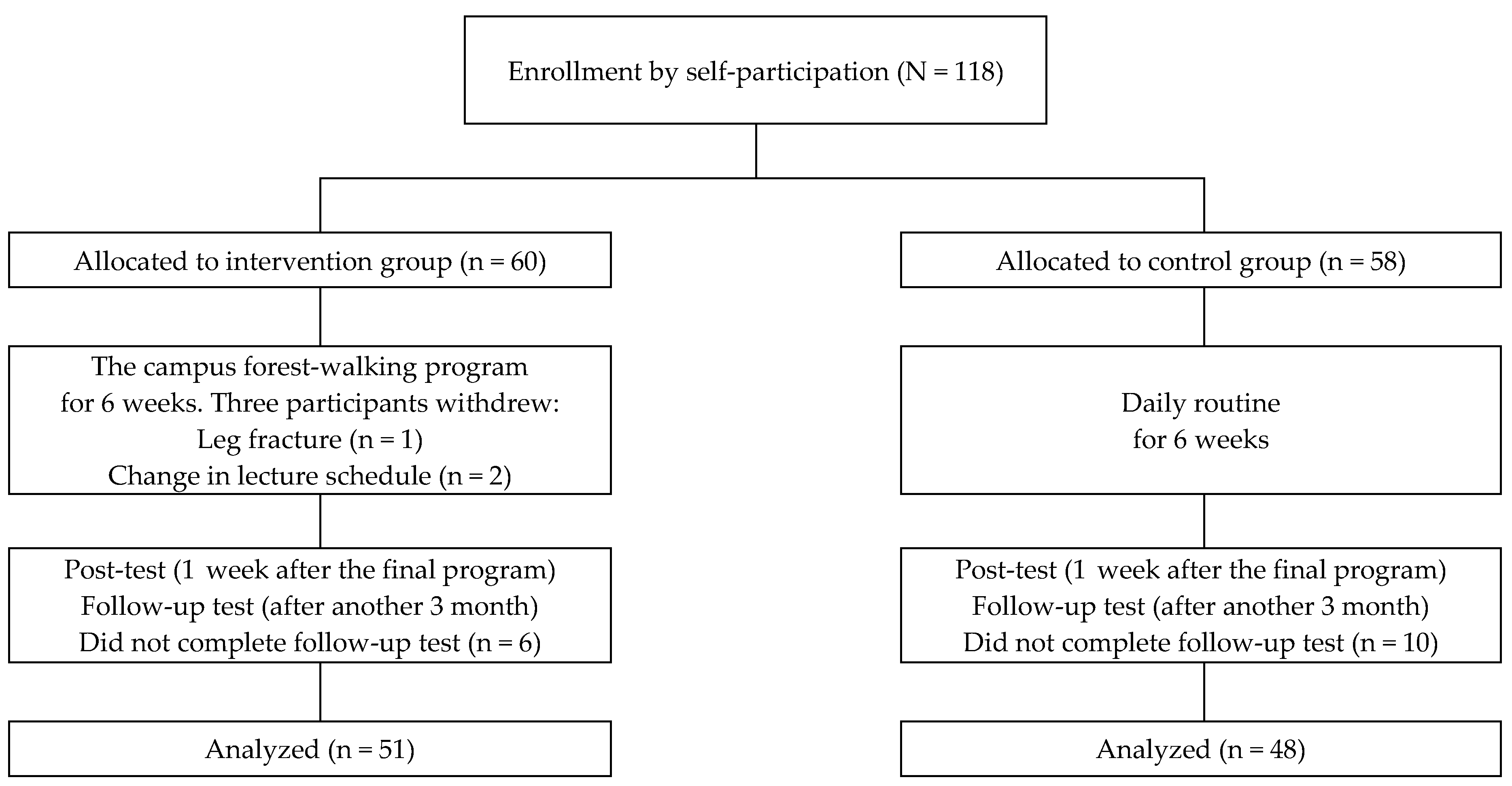
2.1. Study Design and Participants
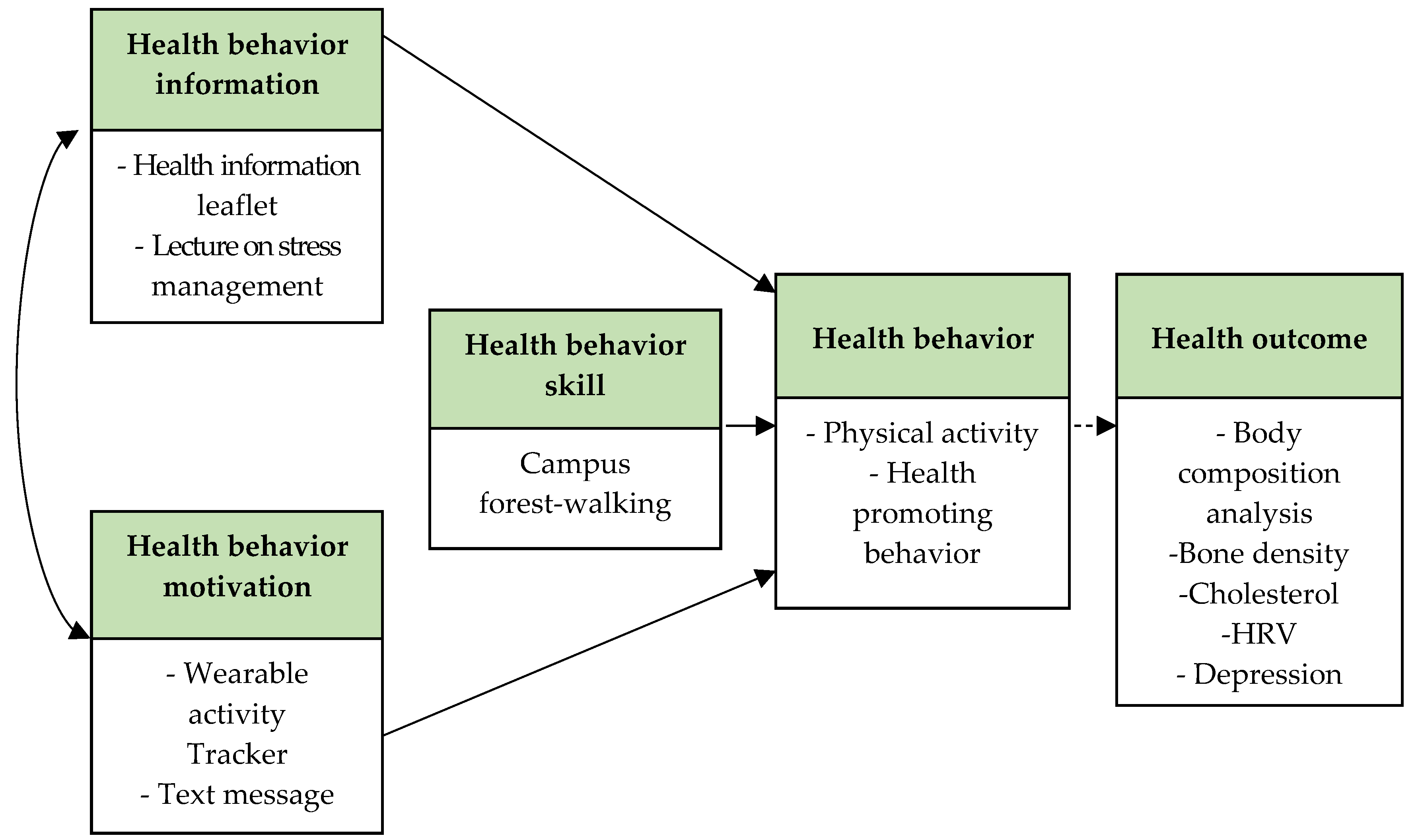
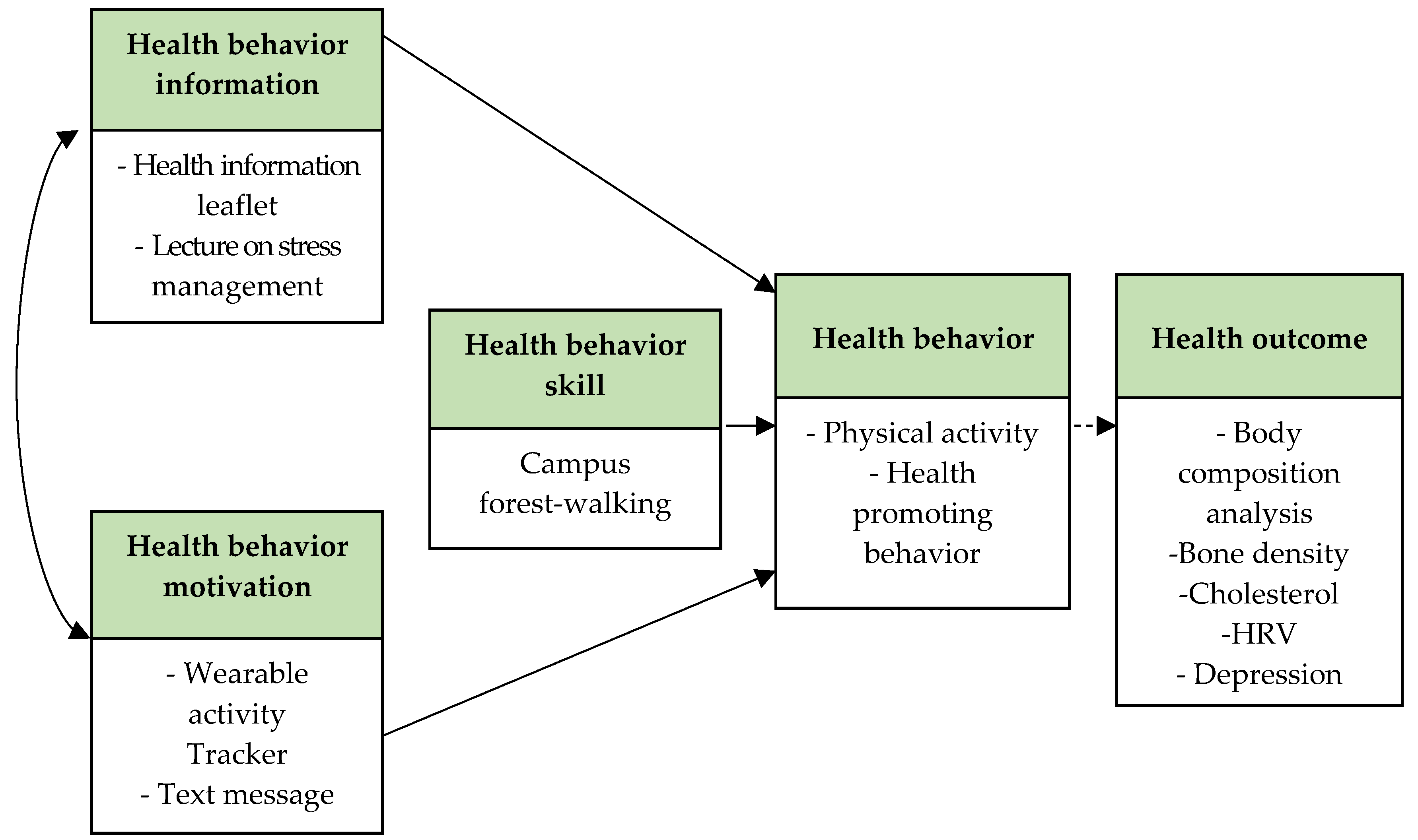
2.2. Intervention
2.3. Measurements
- Walking MET-minutes/week = 3.3 × walking minutes × walking days
- Moderate MET-minutes/week = 4.0 × moderate-intensity activity minutes × moderate days
- Vigorous MET-minutes/week = 8.0 × vigorous-intensity activity minutes × vigorous-intensity days.
2.4. Statistics
3. Results
3.1. Homogeneity Test of the Experimental and Control Group
3.2. Effects of the Intervention on Outcome Measures
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Haskell, W.L.; Blair, S.N.; Hill, J.O. Physical activity: Health outcomes and importance for public health policy. Prev. Med. 2009, 49, 280–282. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Recommendations on Physical Activity for Health; WHO Press: Geneva, Switzerland, 2010. Available online: https://www.ncbi.nlm.nih.gov/books/NBK305057 (accessed on 3 January 2017).
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Dinger, M.K.; Vesely, S.K. Relationships between physical activity and other health-related behaviors in a representative sample of U.S. college students. Am. J. Health Educ. 2001, 32, 83–88. [Google Scholar] [CrossRef]
- Nelson, M.C.; Story, M.; Larson, N.I.; Neumark-Sztainer, D.; Lytle, L.A. Emerging adulthood and college-aged youth: An overlooked age for weight-related behavior change. Obesity 2008, 16, 2205–2211. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, E.K.; Magidson, J.F.; Mayes, L.C.; Lejuez, C.W. Risk-taking behaviors across the transition from adolescence to young adulthood. In Young Adult Mental Health; Grant, J.E., Potenza, M.N., Eds.; Oxford University Press: New York, NY, USA, 2010; pp. 40–63. ISBN 978-0-19-533271-1. [Google Scholar]
- Eisenberg, D.; Gollust, S.E.; Golberstein, E.; Hefner, J.L. Prevalence and correlates of depression, anxiety, and suicidality among university students. Am. J. Orthopsychiatr. 2007, 77, 534–542. [Google Scholar] [CrossRef] [PubMed]
- The American College Health Association. American College Health Association-National College Health Assessment Spring 2007 Reference Group Data Report (abridged). J. Am. Coll. Health 2008, 56, 469–479. [Google Scholar] [CrossRef]
- Regehr, C.; Glancy, D.; Pitts, A. Interventions to reduce stress in university students: A review and meta-analysis. J. Affect. Disord. 2013, 148, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Wang, L.; Qiu, X.H.; Yang, X.X.; Qiao, Z.X.; Yang, Y.J.; Liang, Y. Depression among Chinese university students: Prevalence and socio-demographic correlates. PLoS ONE 2013, 8, e58379. [Google Scholar] [CrossRef]
- Byrd, D.R.; McKinney, K.J. Individual, interpersonal, and institutional level factors associated with the mental health of college students. J. Am. Coll. Health 2012, 60, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Keyes, C.L.; Eisenberg, D.; Perry, G.S.; Dube, S.R.; Kroenke, K.; Dhingra, S.S. The relationship of level of positive mental health with current mental disorders in predicting suicidal behavior and academic impairment in college students. J. Am. Coll. Health 2012, 60, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Wallace, L.S.; Buckworth, J.; Kirby, T.E.; Sherman, W.M. Characteristics of exercise behavior among college students: Application of social cognitive theory to predicting stage of change. Prev. Med. 2000, 31, 494–505. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.K.; Barton, J.L.; Pretty, J.; Gladwell, V.F. Walks4work: Rationale and study design to investigate walking at lunchtime in the workplace setting. BMC Public Health 2012, 12, 550. [Google Scholar] [CrossRef] [PubMed]
- Audrey, S.; Cooper, A.R.; Hollingworth, W.; Metcalfe, C.; Procter, S.; Davis, A.; Campbell, R.; Gillison, F.; Rodgers, S.E. Study protocol: The effectiveness and cost effectiveness of an employer-led intervention to increase walking during the daily commute: The travel to work randomised controlled trial. BMC Public Health 2015, 15, 154. [Google Scholar] [CrossRef] [PubMed]
- Murtagh, E.M.; Nichols, L.; Mohammed, M.A.; Holder, R.; Nevill, A.M.; Murphy, M.H. The effect of walking on risk factors for cardiovascular disease: An updated systematic review and meta-analysis of randomised control trials. Prev. Med. 2015, 72, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Takayama, N.; Korpela, K.; Lee, J.; Morikawa, T.; Tsunetsugu, Y.; Park, B.J.; Li, Q.; Tyrväinen, L.; Miyazaki, Y.; Kagawa, T. Emotional, restorative and vitalizing effects of forest and urban environments at four sites in Japan. Int. J. Environ. Res. Public Health 2014, 11, 7207–7230. [Google Scholar] [CrossRef] [PubMed]
- Mao, G.X.; Lan, X.G.; Cao, Y.B.; Chen, Z.M.; He, Z.H.; Lv, Y.D.; Wang, Y.Z.; Hu, X.L.; Wang, G.F.; Yan, J. Effects of short-term forest bathing on human health in a broad-leaved evergreen forest in Zhejiang province, China. Biomed. Environ. Sci. 2012, 25, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Berto, R. The role of nature in coping with psycho-physiological stress: A literature review on restorativeness. Behav. Sci. 2014, 4, 394–409. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, A.E.; Koole, S.L.; van der Wulp, N.Y. Environmental preference and restoration: (How) Are they related? J. Environ. Psychol. 2003, 23, 135–146. [Google Scholar] [CrossRef]
- Lee, J.; Park, B.J.; Tsunetsugu, Y.; Kagawa, T.; Miyazaki, Y. Restorative effects of viewing real forest landscapes, based on a comparison with urban landscapes. Scand. J. For. Res. 2009, 24, 227–234. [Google Scholar] [CrossRef]
- Li, Q.; Kobayashi, M.; Inagaki, H.; Hirata, Y.; Li, Y.; Hirata, K.; Shimizu, T.; Suzuki, H.; Katsumata, M.; Wakayama, Y. A day trip to a forest park increases human natural killer activity and the expression of anti-cancer proteins in male subjects. J. Biol. Regul. Homeost. Agents 2010, 24, 157–165. [Google Scholar] [PubMed]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Morikawa, T.; Kagawa, T.; Miyazaki, Y. Physiological effects of forest recreation in a young conifer forest in Hinokage town, Japan. Silva Fenn. 2009, 43, 291–301. [Google Scholar] [CrossRef]
- Tsunetsugu, Y.; Lee, J.; Park, B.J.; Tyrväinen, L.; Kagawa, T.; Miyazaki, Y. Physiological and psychological effects of viewing urban forest landscapes assessed by multiple measurements. Landsc. Urban Plan. 2013, 113, 90–93. [Google Scholar] [CrossRef]
- Morita, E.; Fukuda, S.; Nagano, J.; Hamajima, N.; Yamamoto, H.; Iwai, Y.; Nakashima, T.; Ohira, H.; Shirakawa, T. Psychological effects of forest environments on healthy adults: Shinrin-yoku (forest-air bathing, walking) as a possible method of stress reduction. Public Health 2007, 121, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Takamatsu, A.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; et al. Physiological and psychological effects of forest therapy on middle-aged males with high-normal blood pressure. Int. J. Environ. Res. Public Health 2015, 12, 2532–2542. [Google Scholar] [CrossRef] [PubMed]
- Deakin, T.; McShane, C.E.; Cade, J.E.; Williams, R. Group based training for self-management strategies in people with type 2 diabetes mellitus. Cochrane Database Syst. Rev. 2005, 2, CD003417. [Google Scholar] [CrossRef]
- Fisher, J.D.; Fisher, W.A.; Williams, S.S.; Malloy, T.E. Empirical tests of an information-motivation-behavioral skills model of AIDS-preventive behavior with gay men and heterosexual university students. Health Psychol. 1994, 13, 238–250. [Google Scholar] [CrossRef] [PubMed]
- Norton, W.E.; Amico, K.R.; Cornman, D.H.; Fisher, W.A.; Fisher, J.D. An agenda for advancing the science of implementation of evidence-based HIV prevention interventions. AIDS Behav. 2009, 13, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Saltin, B. Evidence for prescribing exercise as therapy in chronic disease. Scand. J. Med. Sci. Sports 2006, 16, 3–63. [Google Scholar] [CrossRef] [PubMed]
- Seo, H.M.; Hah, Y.S. A study of factors influencing on health promoting lifestyle in the elderly-application of Pender’s health promotion model. J. Korean Acad. Nurs. 2004, 34, 1288–1297. [Google Scholar] [CrossRef]
- IPAQ Research Committee. Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ)—Short and Long Forms. 2005. Available online: https://sites.google.com/site/theipaq/ (accessed on 6 June 2017).
- Seurer, A.; Huntington, M.K. Screening and treatment of osteoporosis. S. D. Med. 2015, 68, 497–501. [Google Scholar] [PubMed]
- Hayano, J. Heart rate variability (HRV). In Clinical Assessment of the Autonomic Nervous System; Iwase, S., Hayano, J., Orimo, S., Eds.; Springer: Tokyo, Japan, 2016; pp. 108–127. ISBN 978-4-431-56010-4. [Google Scholar]
- Song, C.; Ikei, H.; Miyazaki, Y. Physiological effects of nature therapy: A review of the research in Japan. Int. J. Environ. Res. Public Health 2016, 13, 781. [Google Scholar] [CrossRef] [PubMed]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 4th ed.; Sage Publications: London, UK, 2013. [Google Scholar]
- Baek, H.C.; Lee, S.J.; Shin, G.; Lim, E.J. Effect of resistance band exercise on body composition, physical fitness and health promoting behavior in nursing students. J. Korean Public Health Nurs. 2014, 28, 310–319. [Google Scholar] [CrossRef]
- Tucker, P.; Gilliland, J. The effect of season and weather on physical activity: A systematic review. Public Health 2007, 121, 909–922. [Google Scholar] [CrossRef] [PubMed]
- Ogilvie, D.; Foster, C.E.; Rothnie, H.; Cavill, N.; Hamilton, V.; Fitzsimons, C.F.; Mutrie, N. Interventions to promote walking: Systematic review. BMJ 2007, 334, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Park, B.; Tsunetsugu, Y.; Ishii, H.; Furuhashi, S.; Hirano, H.; Kagawa, T.; Miyazaki, Y. Physiological effects of Shinrin-yoku (taking in the atmosphere of the forest) in a mixed forest in Shinano Town, Japan. Scand. J. For. Res. 2008, 23, 278–283. [Google Scholar] [CrossRef]
- Tsunetsugu, Y.; Park, B.J.; Ishii, H.; Hirano, H.; Kagawa, T.; Miyazaki, Y. Physiological effects of Shinrin-yoku (taking in the atmosphere of the forest) in an old-growth broadleaf forest in Yamagata Prefecture, Japan. J. Physiol. Anthropol. 2007, 26, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Lim, S.K.; Chung, E.J.; Woo, J.M. The effect of cognitive behavior therapy-based psychotherapy applied in a forest environment on physiological changes and remission of major depressive disorder. Psychiatry Investig. 2009, 6, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Tsunetsugu, Y.; Takayama, N.; Park, B.J.; Li, Q.; Song, C.; Komatsu, M.; Ikei, H.; Tyrväinen, L.; Kagawa, T.; et al. Influence of forest therapy on cardiovascular relaxation in young adults. Evid. Based Complement. Alternat. Med. 2014, 2014, 834360. [Google Scholar] [CrossRef] [PubMed]
- Shin, W.S.; Shin, C.S.; Yeoun, P.S. The influence of forest therapy camp on depression in alcoholics. Environ. Health Prev. Med. 2012, 17, 73–76. [Google Scholar] [CrossRef] [PubMed]
- Richardson, C.R.; Newton, T.L.; Abraham, J.J.; Sen, A.; Jimbo, M.; Swartz, A.M. A meta-analysis of pedometer-based walking interventions and weight loss. Ann. Fam. Med. 2008, 6, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Hamer, M.; Chida, Y. Walking and primary prevention: A meta-analysis of prospective cohort studies. Br. J. Sports Med. 2008, 42, 238–243. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics/Variables | Categories | Exp. (n = 51) n (%) M ± SD | Cont. (n = 48) n (%) M ± SD | x2 or t | p |
|---|---|---|---|---|---|
| Age (years) | 24.8 ± 4.66 | 23.8 ± 3.60 | 1.29 | 0.201 | |
| Sex | Male | 26 (51.0) | 21 (43.8) | 0.518 | 0.548 |
| Female | 25 (49.0) | 27 (56.3) | |||
| College standing | Undergraduate | 23 (45.1) | 23 (47.9) | 0.079 | 0.842 |
| Graduate | 28 (54.9) | 25 (52.1) | |||
| Blood pressure (mmHg) | Systolic BP | 111.55 ± 11.45 | 107.85 ± 11.87 | 1.58 | 0.118 |
| Diastolic BP | 68.47 ± 9.64 | 67.54 ± 7.83 | 0.52 | 0.601 | |
| Blood cholesterol (mg/dL) | Cholesterol, total | 176.59 ± 31.79 | 176.25 ± 30.73 | 0.05 | 0.957 |
| HDL | 65.06 ± 15.20 | 68.58 ± 14.07 | −1.20 | 0.235 | |
| LDL | 103.49 ± 29.01 | 97.75 ± 26.91 | 1.02 | 0.311 | |
| TG | 76.92 ± 42.46 | 71.90 ± 35.53 | 0.64 | 0.526 | |
| Bone density, t-score | −0.83 ± 0.92 | −0.90 ± 1.05 | 0.33 | 0.743 | |
| BMI (kg/m2) | 21.91 ± 2.87 | 21.40 ± 2.77 | 0.89 | 0.375 | |
| Body composition | Percent of body fat (%) | 24.09 ± 6.79 | 23.47 ± 6.38 | 0.47 | 0.637 |
| Amount of muscle (kg) | 44.28 ± 9.39 | 42.33 ± 8.89 | 1.06 | 0.290 | |
| Skeletal muscle mass (kg) | 26.03 ± 6.04 | 24.74 ± 5.75 | 1.09 | 0.280 | |
| Physical activity level (MET-min/week) | 1627.87 ± 1620.76 | 1758.23 ± 1228.39 | −0.45 | 0.655 | |
| Health promoting behavior | 126.25 ± 17.80 | 126.44 ± 18.46 | −0.05 | 0.960 | |
| Heart rate variability | LF/HF ratio | 2.03 ± 1.59 | 2.21 ± 2.15 | −0.47 | 0.636 |
| Parasympathetic nerve activity (%) | 56.27 ± 9.34 | 55.88 ± 10.29 | 0.20 | 0.846 | |
| Depression | 7.86 ± 5.40 | 7.50 ± 5.34 | 0.34 | 0.738 | |
| Variables | Time | Exp. | Cont. | Source | F | p | ES | |
|---|---|---|---|---|---|---|---|---|
| M ± SD | ||||||||
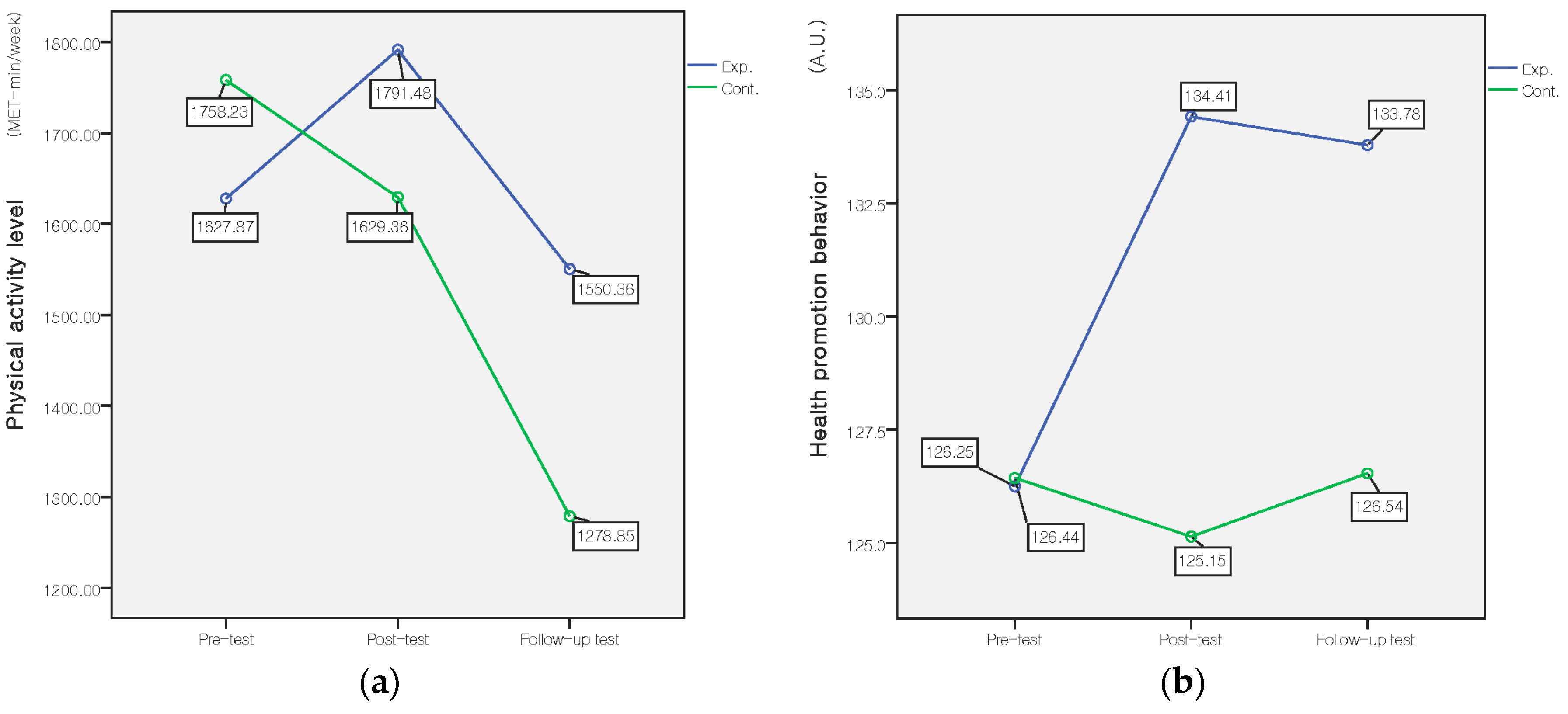
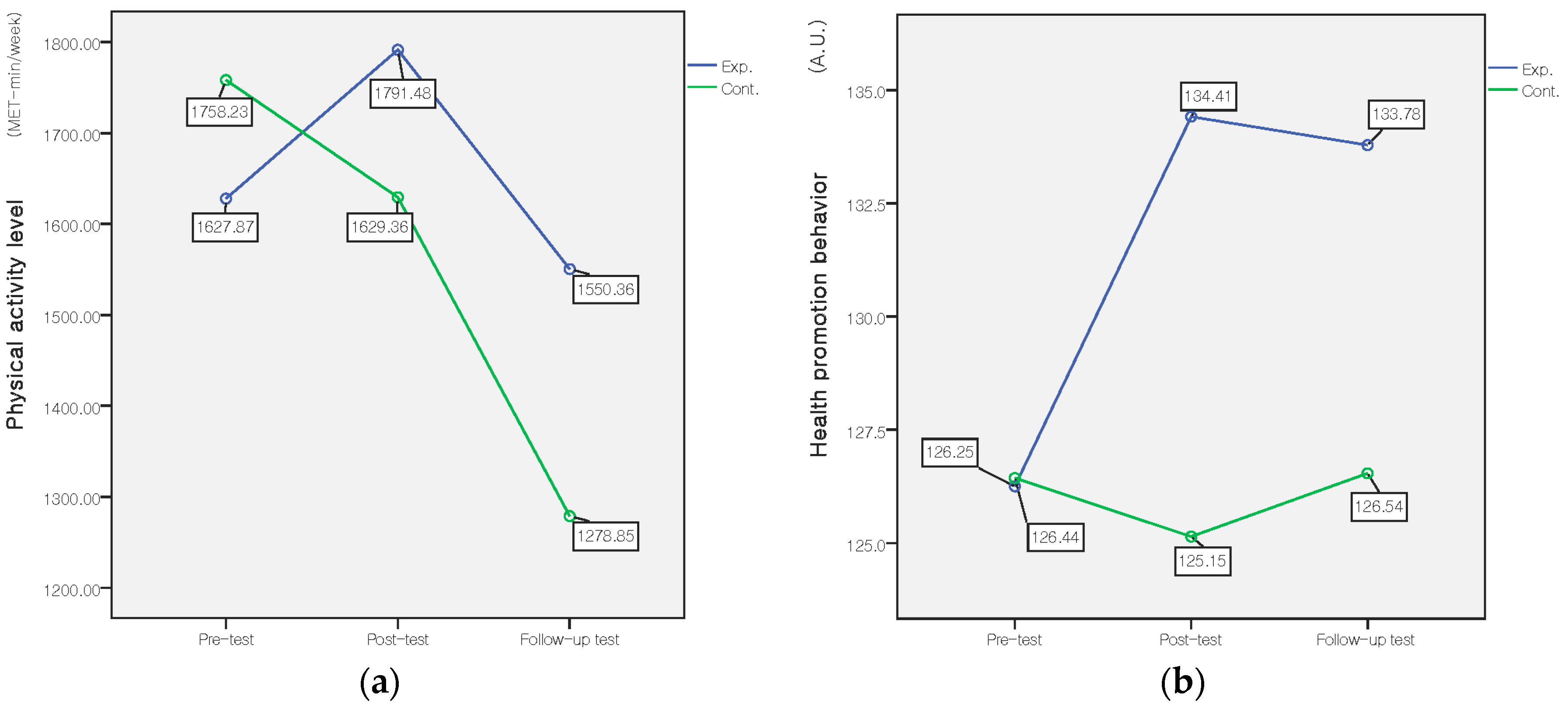
| Physical activity level (MET-min/week) | Pre-test | 1627.87 ± 1620.76 | 1758.23 ± 1228.39 | G | 0.19 | 0.661 | 0.04 | |
| Post-test | 1791.48 ± 1434.68 | 1629.36 ± 1270.70 | T | 3.01 | 0.047 | 0.18 | ||
| F/U test | 1550.36 ± 1310.35 | 1278.85 ± 1333.96 | G*T | 1.21 | 0.300 | 0.11 | ||
| Health promoting behavior | Sum | Pre-test | 126.26 ± 7.80 | 126.44 ± 18.46 | G | 2.58 | 0.112 | 0.16 |
| Post-test | 134.41 ± 15.87 | 125.15 ± 20.12 | T | 5.19 | 0.006 | 0.23 | ||
| F/U test | 133.78 ± 18.15 | 126.54 ± 20.11 | G*T | 7.27 | 0.001 | 0.27 | ||
| Responsibility for health | Pre-test | 17.61 ± 4.41 | 16.85 ± 4.18 | G | 2.32 | 0.131 | 0.15 | |
| Post-test | 18.96 ± 4.48 | 17.33 ± 4.23 | T | 6.40 | 0.002 | 0.26 | ||
| F/U test | 18.88 ± 4.57 | 17.63 ± 4.20 | G*T | 0.97 | 0.380 | 0.33 | ||
| Physical activity | Pre-test | 18.47 ± 5.54 | 19.19 ± 6.11 | G | 1.36 | 0.247 | 0.12 | |
| Post-test | 21.00 ± 4.76 | 18.94 ± 6.12 | T | 3.05 | 0.050 | 0.18 | ||
| F/U test | 20.65 ± 5.09 | 18.54 ± 5.95 | G*T | 5.91 | 0.003 | 0.25 | ||
| Healthy nutrition | Pre-test | 21.59 ± 4.75 | 21.94 ± 5.23 | G | 0.59 | 0.443 | 0.08 | |
| Post-test | 22.31 ± 4.18 | 20.96 ± 5.59 | T | 0.26 | 0.775 | 0.06 | ||
| F/U test | 22.45 ± 4.58 | 21.31 ± 5.71 | G*T | 3.64 | 0.028 | 0.19 | ||
| Social relations | Pre-test | 23.80 ± 4.54 | 24.06 ± 3.86 | G | 0.10 | 0.754 | 0.03 | |
| Post-test | 24.75 ± 4.02 | 24.02 ± 3.83 | T | 1.27 | 0.282 | 0.11 | ||
| F/U test | 24.35 ± 3.88 | 24.13 ± 3.87 | G*T | 1.46 | 0.235 | 0.12 | ||
| Stress management | Pre-test | 18.43 ± 3.89 | 18.00 ± 3.50 | G | 4.18 | 0.044 | 0.21 | |
| Post-test | 20.18 ± 2.96 | 18.13 ± 4.08 | T | 12.73 | 0.000 | 0.36 | ||
| F/U test | 20.49 ± 3.51 | 19.11 ± 3.57 | G*T | 3.32 | 0.038 | 0.18 | ||
| Spiritual growth | Pre-test | 26.35 ± 4.58 | 26.50 ± 4.89 | G | 0.72 | 0.398 | 0.08 | |
| Post-test | 27.22 ± 4.29 | 25.85 ± 4.93 | T | 0.06 | 0.941 | 0.03 | ||
| F/U test | 26.96 ± 4.49 | 25.98 ± 4.68 | G*T | 3.14 | 0.45 | 0.18 | ||
| Variables | Time | Exp. | Cont. | Source | F | p | ES | |
|---|---|---|---|---|---|---|---|---|
| M ± SD | ||||||||
| BP (mmHg) | Systolic | Pre-test | 111.55 ± 11.45 | 107.85 ± 11.87 | Group | 0.92 | 0.339 | 0.10 |
| Post-test | 112.02 ± 11.92 | 110.56 ± 11.62 | Time | 7.83 | 0.001 | 0.28 | ||
| F/U test | 114.08 ± 12.58 | 113.21 ± 11.74 | G*T | 1.11 | 0.333 | 0.11 | ||
| Diastolic | Pre-test | 68.47 ± 9.64 | 67.54 ± 7.83 | Group | 0.60 | 0.441 | 0.08 | |
| Post-test | 69.29 ± 8.98 | 66.63 ± 8.28 | Time | 0.37 | 0.694 | 0.06 | ||
| F/U test | 68.39 ± 8.01 | 68.92 ± 7.36 | G*T | 1.55 | 0.215 | 0.13 | ||
| Cholesterol (mg/dL) | Total | Pre-test | 176.59 ± 31.79 | 176.25 ± 30.73 | Group | 0.09 | 0.772 | 0.03 |
| Post-test | 175.69 ± 28.70 | 177.15 ± 27.80 | Time | 2.01 | 0.137 | 0.14 | ||
| F/U test | 177.73 ± 29.53 | 181.50 ± 29.82 | G*T | 0.63 | 0.535 | 0.08 | ||
| HDL * | Pre-test | 65.06 ± 15.20 | 68.58 ± 14.07 | Group | 0.80 | 0.375 | 0.09 | |
| Post-test | 64.22 ± 14.65 | 65.81 ± 12.42 | Time | 1.86 | 0.161 | 0.20 | ||
| F/U test | 64.82 ± 16.20 | 66.92 ± 15.63 | G*T | 0.46 | 0.635 | 0.10 | ||
| LDL * | Pre-test | 103.49 ± 29.01 | 97.75 ± 26.91 | Group | 0.19 | 0.663 | 0.04 | |
| Post-test | 100.84 ± 26.80 | 99.25 ± 22.70 | Time | 3.97 | 0.022 | 0.29 | ||
| F/U test | 103.75 ± 26.70 | 104.69 ± 24.51 | G*T | 1.51 | 0.225 | 0.18 | ||
| TG | Pre-test | 76.92 ± 42.46 | 71.90 ± 35.53 | Group | 0.07 | 0.790 | 0.03 | |
| Post-test | 80.24 ± 46.40 | 85.60 ± 55.16 | Time | 3.08 | 0.048 | 0.18 | ||
| F/U test | 73.59 ± 41.43 | 79.67 ± 45.16 | G*T | 1.53 | 0.220 | 0.13 | ||
| Bone density, T-score * | Pre-test | −0.84 ± 0.92 | −0.90 ± 1.05 | Group | 0.33 | 0.565 | 0.05 | |
| Post-test | −0.50 ± 0.96 | −0.55 ± 1.03 | Time | 27.04 | 0.000 | 0.75 | ||
| F/U test | −0.36 ± 0.94 | −0.57 ± 0.91 | G*T | 1.52 | 0.224 | 0.18 | ||
| BMI (kg/m2) * | Pre-test | 21.91 ± 2.87 | 21.40 ± 2.77 | Group | 0.69 | 0.407 | 0.08 | |
| Post-test | 22.07 ± 2.91 | 21.47 ± 2.81 | Time | 2.61 | 0.079 | 0.23 | ||
| F/U test | 21.99 ± 2.84 | 21.67 ± 3.04 | G*T | 1.94 | 0.147 | 0.20 | ||
| Percent of body fat (%) | Pre-test | 24.09 ± 6.79 | 23.47 ± 6.38 | Group | 0.41 | 0.524 | 0.06 | |
| Post-test | 24.42 ± 6.52 | 22.91 ± 6.96 | Time | 0.62 | 0.540 | 0.08 | ||
| F/U test | 23.73 ± 6.58 | 23.33 ± 6.95 | G*T | 3.41 | 0.035 | 0.19 | ||
| Variables | Time | Exp. | Cont. | Source | F | p | ES |
|---|---|---|---|---|---|---|---|
| M ± SD | |||||||
| LF/HF ratio * | Pre-test | 2.03 ± 1.59 | 2.21 ± 2.15 | Group | 0.363 | 0.548 | 0.06 |
| Post-test | 1.97 ± 1.85 | 1.85 ± 1.27 | Time | 1.139 | 0.324 | 0.15 | |
| F/U test | 1.63 ± 1.27 | 2.07 ± 1.76 | G*T | 1.867 | 0.160 | 0.20 | |
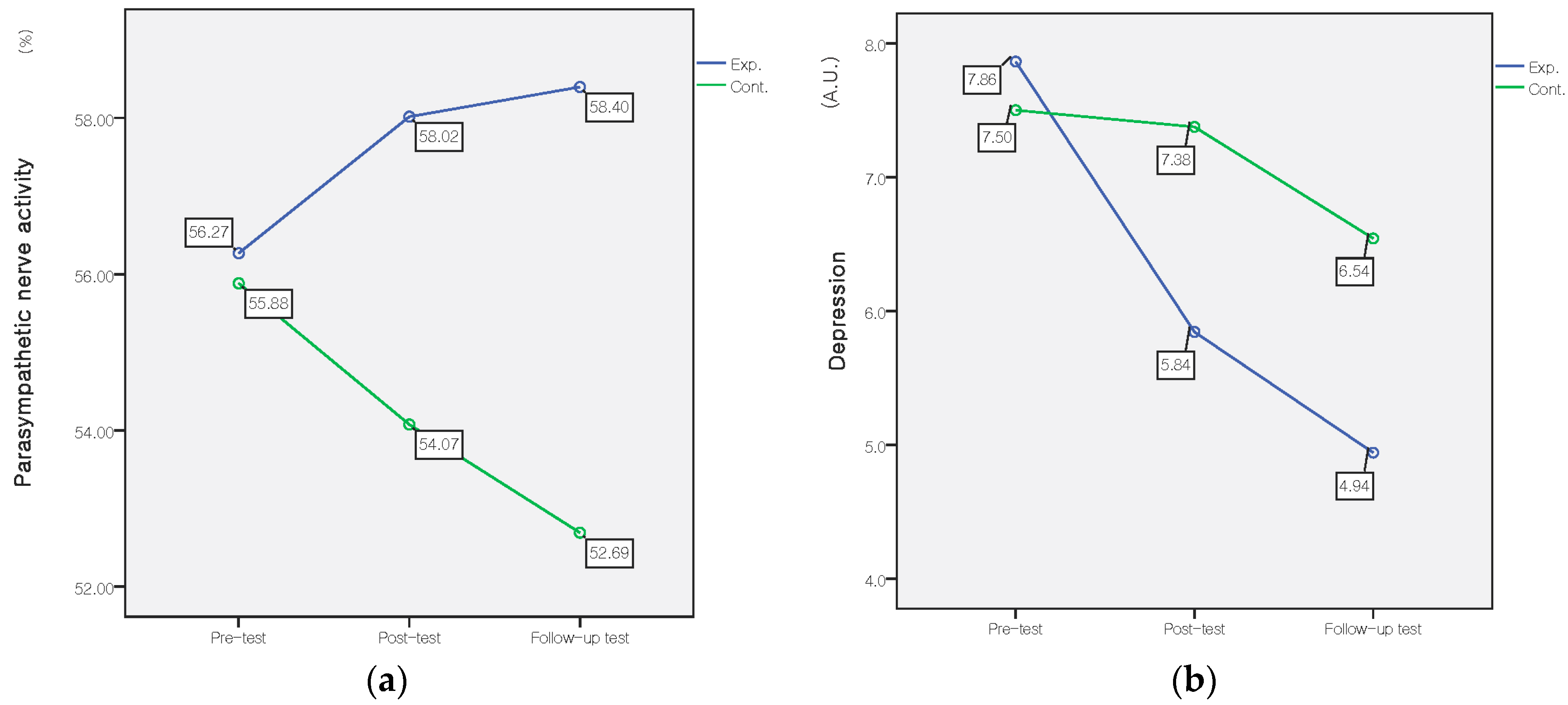
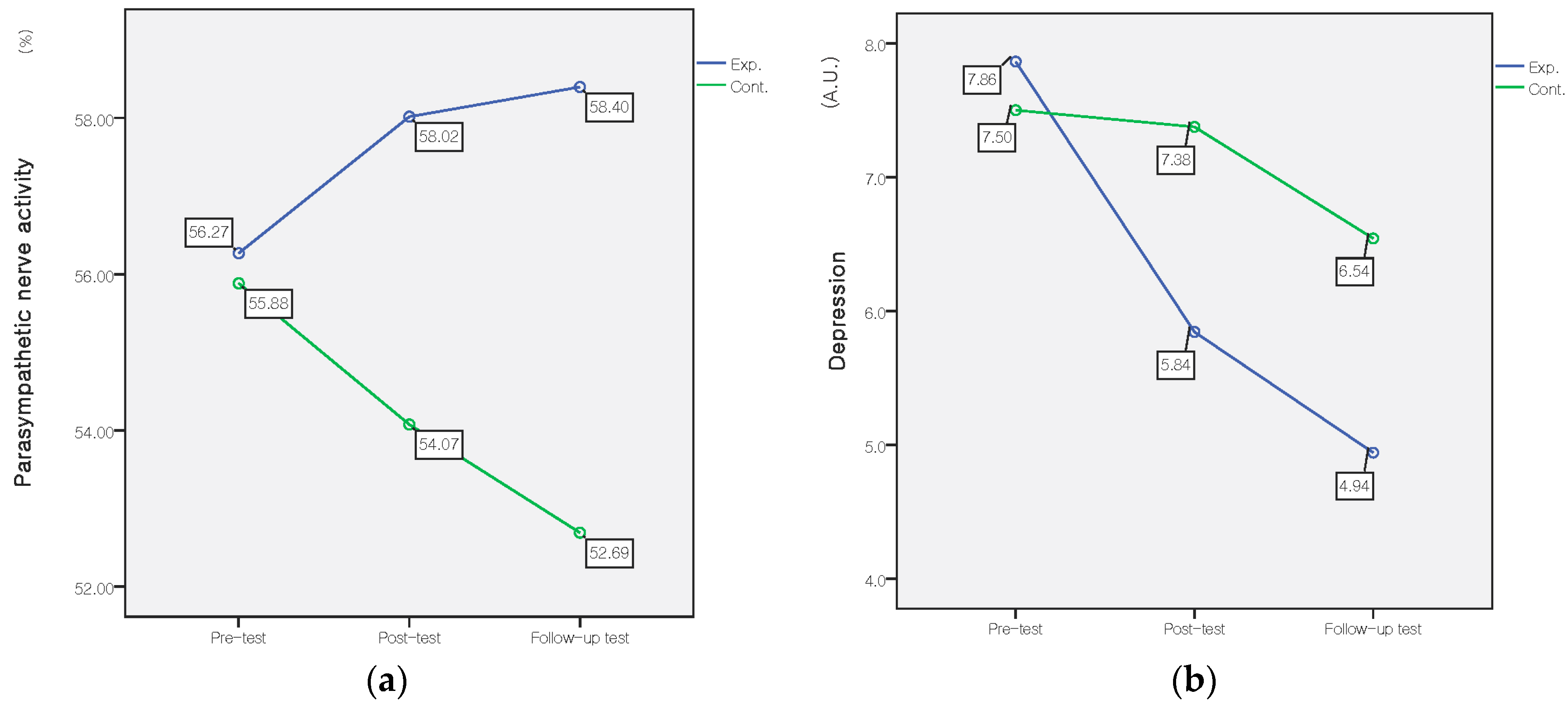
| Parasympathetic nerve activity (%) | Pre-test | 56.27 ± 9.34 | 55.88 ± 10.29 | Group | 4.11 | 0.045 | 0.21 |
| Post-test | 58.02 ± 9.20 | 54.07 ± 10.43 | Time | 0.18 | 0.836 | 0.04 | |
| F/U test | 58.40 ± 8.74 | 52.69 ± 11.90 | G*T | 3.69 | 0.027 | 0.20 | |
| Depression | Pre-test | 7.86 ± 5.40 | 7.50 ± 5.34 | Group | 0.92 | 0.340 | 0.10 |
| Post-test | 5.84 ± 5.00 | 7.38 ± 6.02 | Time | 9.59 | 0.000 | 0.31 | |
| F/U test | 4.94 ± 4.82 | 6.54 ± 5.89 | G*T | 3.15 | 0.045 | 0.18 | |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bang, K.-S.; Lee, I.; Kim, S.; Lim, C.S.; Joh, H.-K.; Park, B.-J.; Song, M.K. The Effects of a Campus Forest-Walking Program on Undergraduate and Graduate Students’ Physical and Psychological Health. Int. J. Environ. Res. Public Health 2017, 14, 728. https://doi.org/10.3390/ijerph14070728
Bang K-S, Lee I, Kim S, Lim CS, Joh H-K, Park B-J, Song MK. The Effects of a Campus Forest-Walking Program on Undergraduate and Graduate Students’ Physical and Psychological Health. International Journal of Environmental Research and Public Health. 2017; 14(7):728. https://doi.org/10.3390/ijerph14070728
Chicago/Turabian StyleBang, Kyung-Sook, Insook Lee, Sungjae Kim, Chun Soo Lim, Hee-Kyung Joh, Bum-Jin Park, and Min Kyung Song. 2017. "The Effects of a Campus Forest-Walking Program on Undergraduate and Graduate Students’ Physical and Psychological Health" International Journal of Environmental Research and Public Health 14, no. 7: 728. https://doi.org/10.3390/ijerph14070728