Horizontal Inequity in Health Care Utilization among the Middle-Aged and Elderly in China

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Descriptive Results
3.2. Indices for Total Inequality and Horizontal Inequity
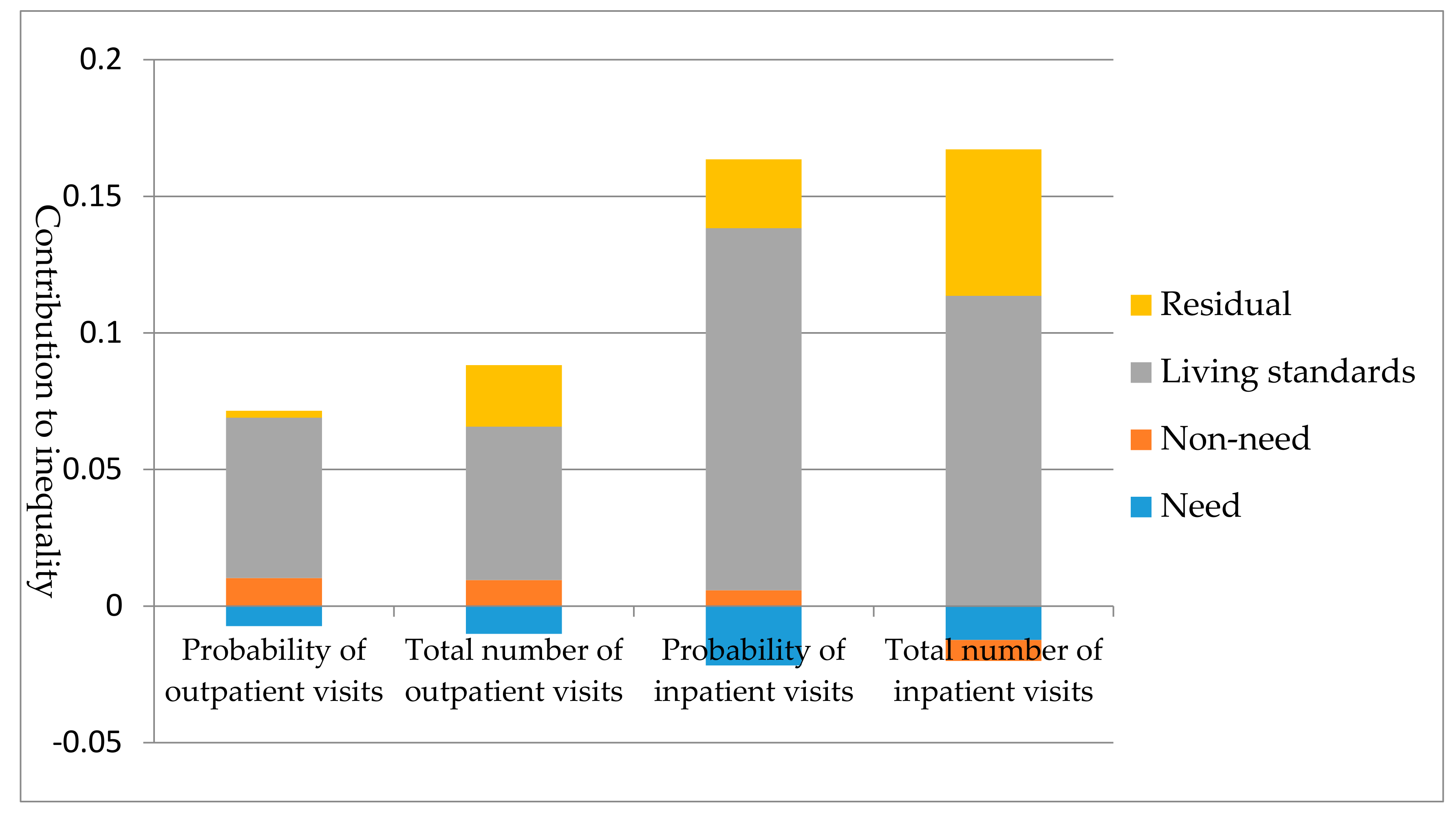
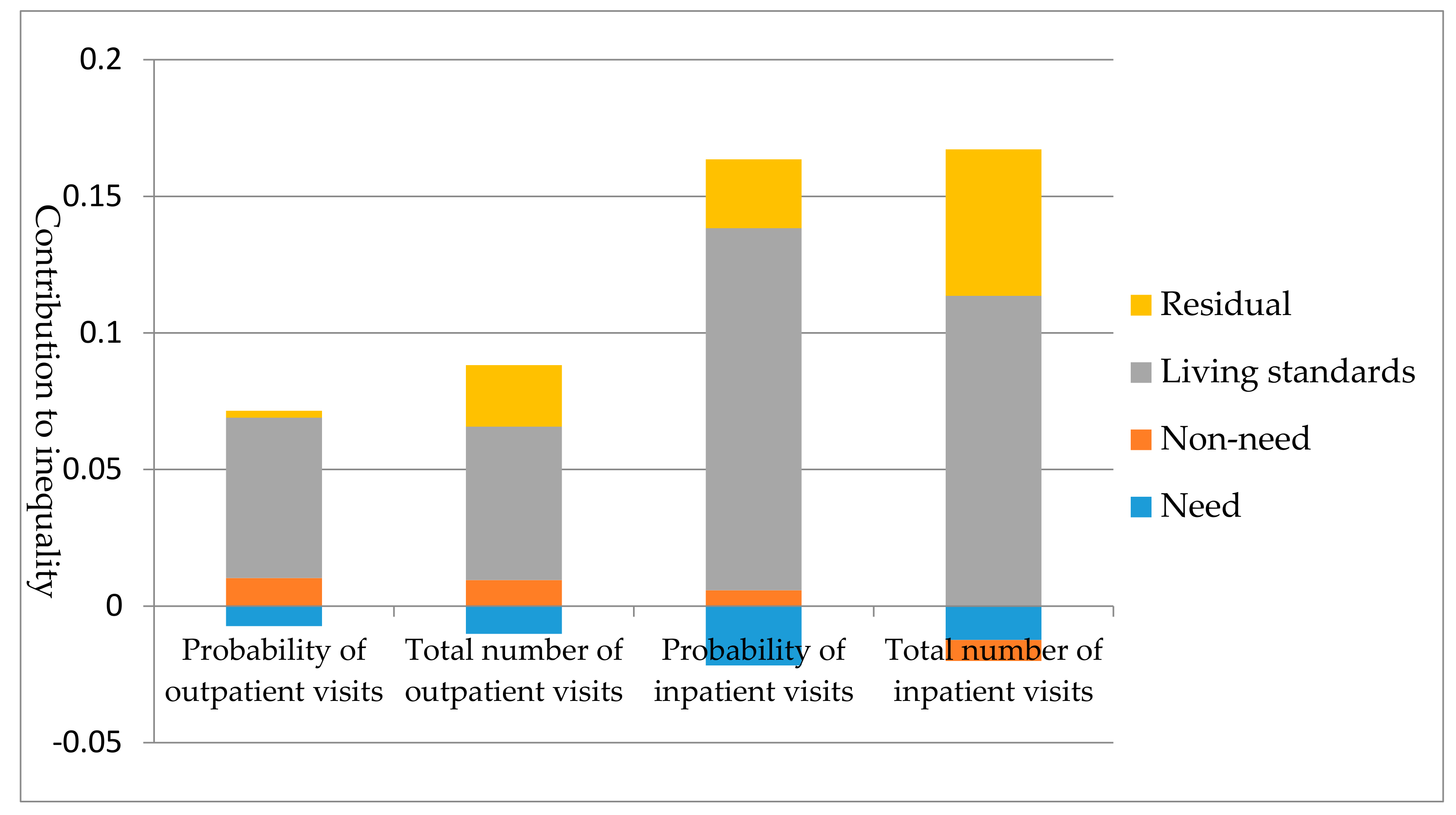
3.3. Decomposition of Inequality in Outpatient Visits
3.4. Decomposition of Inequality in Inpatient Visits
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Penning, M.J.; Zheng, C. Income inequities in health care utilization among adults aged 50 and older. Can. J. Aging 2016, 35, 55–69. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Wu, Q.; Shao, Y.; Fu, W.; Liu, G.; Coyte, P.C. Socioeconomic inequities in health care utilization in China. Asia Pac. J. Public Health 2015, 27, 429–438. [Google Scholar] [CrossRef]
- Braveman, P. Health disparities and health equity: Concepts and measurement. Annu. Rev Public Health 2006, 27, 167–194. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.; Meng, Q.; Chen, L.; Bekedam, H.; Evans, T.; Whitehead, M. Tackling the challenges to health equity in China. Lancet 2008, 372, 1493–1501. [Google Scholar] [CrossRef]
- Van Doorslaer, E.; Koolman, X.; Jones, A.M. Explaining income-related inequalities in doctor utilisation in Europe. Health Econ. 2004, 13, 629–647. [Google Scholar] [CrossRef]
- Macinko, J.; Lima-Costa, M.F. Horizontal equity in health care utilization in Brazil, 1998–2008. Int. J. Equity Health 2012, 11, 33. [Google Scholar] [CrossRef]
- Vikum, E.; Krokstad, S.; Westin, S. Socioeconomic inequalities in health care utilisation in Norway: The population-based HUNT3 survey. Int. J. Equity Health 2012, 11, 48. [Google Scholar] [CrossRef]
- Barraza-Llorens, M.; Panopoulou, G.; Diaz, B.Y. Income-related inequalities and inequities in health and health care utilization in Mexico, 2000–2006. Rev. Panam Salud Publica 2013, 33, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Nunez, A.; Chi, C. Equity in health care utilization in Chile. Int. J. Equity Health 2013, 12, 58. [Google Scholar] [CrossRef] [PubMed]
- Duy Kien, V.; Van Minh, H.; Bao Giang, K.; Weinehall, L.; Ng, N. Horizontal inequity in public health care service utilization for non-communicable diseases in urban Vietnam. Glob. Health Action 2014, 7, 24919. [Google Scholar] [CrossRef]
- Devaux, M. Income-related inequalities and inequities in health care services utilisation in 18 selected OECD countries. Eur. J. Health Econ. 2015, 16, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Dorjdagva, J.; Batbaatar, E.; Dorjsuren, B.; Kauhanen, J. Income-related inequalities in health care utilization in Mongolia, 2007/2008–2012. Int. J. Equity Health 2015, 14, 57. [Google Scholar] [CrossRef] [PubMed]
- Park, J.M. Equity in the utilization of physician and inpatient hospital services: Evidence from Korean health panel survey. Int. J. Equity Health 2016, 15, 159. [Google Scholar] [CrossRef] [PubMed]
- Flato, H.; Zhang, H. Inequity in level of healthcare utilization before and after universal health coverage reforms in China: Evidence from household surveys in Sichuan province. Int. J. Equity Health 2016, 15, 96. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Zhang, Q.; Lu, M.; Kwon, C.S.; Quan, H. Rural and urban disparity in health services utilization in China. Med. Care 2007, 45, 767–774. [Google Scholar] [CrossRef]
- Li, Y. Research of Prediction and Equity of Utilization of Health Services of Residents in China. Master’s Thesis, Shandong University, Jinan, China, 2016. [Google Scholar]
- Zhou, Z.; Gao, J.; Fox, A.; Rao, K.; Xu, K.; Xu, L.; Zhang, Y. Measuring the equity of inpatient utilization in Chinese rural areas. BMC Health Serv. Res. 2011, 11, 201. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Su, Y.; Gao, J.; Campbell, B.; Zhu, Z.; Xu, L.; Zhang, Y. Assessing equity of healthcare utilization in rural China: Results from nationally representative surveys from 1993 to 2008. Int. J. Equity Health 2013, 12, 34. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Rechel, B.; Grundy, E.; Robine, J.M.; Cylus, J.; Mackenbach, J.P.; Knai, C.; McKee, M. Ageing in the European Union. Lancet 2013, 381, 1312–1322. [Google Scholar] [CrossRef]
- The Office of China National Committee on Aging. The general research report of Chinese strategic for dealing with population aging. Sci. Res. Aging 2015, 3, 34–38. [Google Scholar]
- Crespo-Cebada, E.; Urbanos-Garrido, R.M. Equity and equality in the use of GP services for elderly people: The Spanish case. Health Policy 2012, 104, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Joe, W.; Rudra, S.; Subramanian, S.V. Horizontal inequity in elderly health care utilization: Evidence from India. J. Korean Med. Sci. 2015, 30, S155–S166. [Google Scholar] [CrossRef] [PubMed]
- Terraneo, M. Inequities in health care utilization by people aged 50+: Evidence from 12 European countries. Soc. Sci. Med. 2015, 126, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, J.; Maitland, E.; Zhao, Y.H.; Nicholas, S.; Lu, M.S. Growing old before growing rich: Inequality in health service utilization among the mid-aged and elderly in Gansu and Zhejiang provinces, China. BMC Health Serv. Res. 2012, 12, 302. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G. Explaining Economic Status Related Inequity of Health Care Utilization among the Mid-Aged and Elderly in China. Master’s Thesis, Shandong University, Jinan, China, 2013. [Google Scholar]
- The China Health and Retirement Longitudinal Study (CHARLS). Available online: http://charls.pku.edu.cn/zh-CN (accessed on 15 April 2016).
- Zhao, Y.; Hu, Y.; Smith, J.P.; Strauss, J.; Yang, G. Cohort profile: The China health and retirement longitudinal study (CHARLS). Int. J. Epidemiol. 2014, 43, 61–68. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, O.; Doorslaer, E.V.; Wagstaff, A.; Lindelow, M. Analyzing Health Equit Using Household Survey Data: A Guide to Techniques and Their Implementation; World Bank: Washington, DC, USA, 2008; p. 178. [Google Scholar]
- Wagstaff, A.; Paci, P.; van Doorslaer, E. On the measurement of inequalities in health. Soc. Sci. Med. 1991, 33, 545–557. [Google Scholar] [CrossRef]
- Wagstaff, A.; van Doorslaer, E. Measuring and testing for inequity in the delivery of health care. J. Hum. Resour. 2000, 35, 716–733. [Google Scholar] [CrossRef]
- Wagstaff, A.; van Doorslaer, E.; Watanabe, N. On decomposing the causes of health sector inequalities with an application to malnutrition inequalities in Vietnam. J. Econ. 2003, 112, 207–223. [Google Scholar] [CrossRef]
- Van Doorslaer, E.; Masseria, C. Income-Related Inequality in the Use of Medical Care in 21 OECD Countries; OECD, Health Project: Paris, France, 2004; No. 14. [Google Scholar]
- Lu, J.F.; Leung, G.M.; Kwon, S.; Tin, K.Y.; Van Doorslaer, E.; O’Donnell, O. Horizontal equity in health care utilization evidence from three high-income Asian economies. Soc. Sci. Med. 2007, 64, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Yang, W. China’s new cooperative medical scheme and equity in access to health care: Evidence from a longitudinal household survey. Int. J. Equity Health 2013, 12, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Z.; Zhu, L.; Zhou, Z.; Li, Z.; Gao, J.; Chen, G. The effects of China’s urban basic medical insurance schemes on the equity of health service utilisation: Evidence from Shaanxi province. Int. J. Equity Health 2014, 13, 23. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.Y.; Hashimoto, H. How do patients and providers react to different incentives in the Chinese multiple health security systems? Chin. Med. J. 2015, 128, 632–637. [Google Scholar] [PubMed]
- Devaux, M.; De Looper, M. Income-Related Inequalities in Health Service Utilisation in 19 OECD Countries; OECD Publishing: Paris, France, 2012; No. 58. [Google Scholar]
- Kim, S.; Kwon, S. The effect of extension of benefit coverage for cancer patients on health care utilization across different income groups in South Korea. Int. J. Health Care Financ. Econ. 2014, 14, 161–177. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Category | All (n = 13,302) |
|---|---|---|
| Dependent variables | At least one outpatient visit in the last month, n (%) | 2826 (21.24) |
| Total number of outpatient visits, mean (SD) | 0.49 ± 1.57 | |
| At least one inpatient visit in the last year, n (%) | 1654 (12.43) | |
| Total number of inpatient visits, mean (SD) | 0.18 ± 0.64 | |
| Need variables | ||
| Gender | Female 1, n (%) | 6814 (51.23) |
| Male, n (%) | 6488 (48.77) | |
| Age | 45−59.1, n (%) | 7019 (52.77) |
| 60−74, n (%) | 5285 (39.73) | |
| 75+, n (%) | 998 (7.50) | |
| Self-reported health status | Very good 1, n (%) | 651 (4.89) |
| Good, n (%) | 1547 (11.63) | |
| Fair, n (%) | 4382 (32.94) | |
| Poor, n (%) | 4790 (36.01) | |
| Very poor, n (%) | 1932 (14.52) | |
| Chronic disease | Yes, n (%) | 9642 (72.49) |
| No 1, n (%) | 3660 (27.51) | |
| Disability | Yes, n (%) | 3050 (22.93) |
| No 1, n (%) | 10,252 (77.07) | |
| Non-need variables | ||
| Health insurance schemes | UEBMI 1, n (%) | 1416 (10.65) |
| URBMI, n (%) | 860 (6.47) | |
| NRCMS, n (%) | 9100 (68.41) | |
| Other health insurance, n (%) | 450 (3.38) | |
| No health insurance, n (%) | 424 (3.19) | |
| Two kinds of health insurance, n (%) | 1052 (7.91) | |
| Education level | Illiterate 1, n (%) | 3187 (23.96) |
| Primary school, n (%) | 5406 (40.64) | |
| Middle school, n (%) | 2929 (22.02) | |
| High school, n (%) | 1471 (11.06) | |
| College and above, n (%) | 309 (2.32) | |
| Region | East 1, n (%) | 4575 (34.39) |
| Central, n (%) | 4391 (33.01) | |
| West, n (%) | 4336 (32.60) | |
| Marital status | Married 1, n (%) | 11,854 (89.11) |
| Divorced, n (%) | 149 (1.12) | |
| Unmarried, n (%) | 1299 (9.77) | |
| Occupation status | Agricultural work 1, n (%) | 6104 (45.89) |
| Employed, n (%) | 2055 (15.45) | |
| Self-employed, n (%) | 963 (7.24) | |
| Not working, n (%) | 4180 (31.42) | |
| Area | Urban, n (%) | 5140 (38.64) |
| Rural 1, n (%) | 8162 (61.36) | |
| Living standards | Pce, mean (SD) | 11,177.52 ± 18,359.71 |
| Quintiles | Probability of Outpatient Visits | Total Number of Outpatient Visits | Probability of Inpatient Visits | Total Number of Inpatient Visits |
|---|---|---|---|---|
| Poorest | 0.1819 | 0.4055 | 0.0888 | 0.1261 |
| 2 | 0.2119 | 0.4386 | 0.1023 | 0.1379 |
| 3 | 0.2173 | 0.5323 | 0.1246 | 0.1888 |
| 4 | 0.2201 | 0.5574 | 0.1511 | 0.2202 |
| Richest | 0.2650 | 0.6372 | 0.1725 | 0.2483 |
| CI | 0.0642 * | 0.0780 * | 0.1418 * | 0.1471 * |
| HI | 0.0714 * | 0.0882 * | 0.1636 * | 0.1596 * |
| Variable | Probability | Total Number | ||||
|---|---|---|---|---|---|---|
| Coeff 1 | Cont 2 | Percent | Coeff 1 | Cont 2 | Percent | |
| Need variables | −0.0073 | −11.37 | −0.0102 | −13.08 | ||
| Male | −0.1143 * | −0.0009 | −1.46 | −0.3151 ** | −0.0016 | −2.04 |
| 60−74 | −0.0652 | 0.0016 | 2.55 | 0.0412 | −0.0006 | −0.82 |
| 75+ | −0.1274 | 0.0014 | 2.13 | −0.0343 | 0.0002 | 0.31 |
| Health good | 0.3307 ** | 0.0013 | 2.09 | 0.2196 | 0.0005 | 0.64 |
| Health fair | 0.5247 ** | 0.0044 | 6.85 | 0.7493 ** | 0.0036 | 4.67 |
| Health poor | 0.7359 ** | −0.0008 | −1.17 | 1.2220 ** | −0.0007 | −0.92 |
| Health very poor | 0.9655 ** | −0.0165 | −25.71 | 1.5888 ** | −0.0136 | −17.50 |
| Chronic disease | 0.4883 ** | 0.0033 | 5.16 | 0.8124 ** | 0.0037 | 4.79 |
| Disability | 0.0483 | −0.0011 | −1.71 | 0.1226 | −0.0017 | −2.18 |
| Non-need variables | 0.0103 | 16.04 | 0.0095 | 12.18 | ||
| URBMI | −0.1762 | −0.0028 | −4.29 | −0.3123 | −0.0032 | −4.12 |
| NRCMS | −0.1221 | 0.0126 | 19.71 | −0.1020 | 0.0064 | 8.26 |
| Other health insurance | −0.1191 | −0.0022 | −3.37 | −0.3513 | −0.0041 | −5.29 |
| No health insurance | −0.2597 * | 0.0005 | 0.81 | −0.0700 | 0.0001 | 0.12 |
| Two kinds of health insurance | −0.0772 | −0.0009 | −1.44 | −0.0068 | −0.0001 | −0.07 |
| Primary school | 0.0194 | −0.0006 | −0.97 | 0.0307 | −0.0006 | −0.78 |
| Middle school | 0.0189 | 0.0005 | 0.77 | 0.0792 | 0.0013 | 1.63 |
| High school | 0.0218 | 0.0009 | 1.39 | 0.1361 | 0.0034 | 4.36 |
| College and above | −0.0184 | −0.0004 | −0.57 | 0.1967 | 0.0024 | 3.10 |
| Central | −0.1047 * | 0.0015 | 2.32 | −0.1583 | 0.0014 | 1.81 |
| West | −0.0083 | 0.0001 | 0.17 | 0.0180 | −0.0001 | −0.18 |
| Divorced | 0.3568 | 0.0020 | 3.10 | 0.7201 * | 0.0022 | 2.79 |
| Unmarried | 0.1476 | −0.0017 | −2.62 | 0.2010 * | −0.0013 | −1.73 |
| Employed | −0.1204 | −0.0023 | −3.62 | −0.2008 | −0.0025 | −3.17 |
| Self-employed | −0.0787 | −0.0009 | −1.35 | 0.0608 | 0.0004 | 0.55 |
| Not working | 0.0398 | 0.0020 | 3.15 | 0.0400 | 0.0012 | 1.60 |
| Urban | 0.0205 | 0.0020 | 3.11 | 0.0428 | 0.0026 | 3.30 |
| Living standards | ||||||
| Ln pce 3 | 0.0846 ** | 0.0587 | 91.39 | 0.1313 ** | 0.0562 | 72.04 |
| Variable | Probability | Total Number | ||||
|---|---|---|---|---|---|---|
| Coeff 1 | Cont 2 | Percent | Coeff 1 | Cont 2 | Percent | |
| Need variables | −0.0217 | −15.30 | −0.0124 | −8.43 | ||
| Male | 0.0999 | 0.0009 | 0.64 | 0.1860 * | 0.0008 | 0.56 |
| 60−74 | 0.0933 * | 0.0004 | 0.28 | 0.1028 * | 0.0002 | 0.14 |
| 75+ | 0.1065 | −0.0030 | −2.14 | 0.1695 * | −0.0023 | −1.56 |
| Health good | 0.1628 | −0.0022 | −1.56 | 0.3166 | −0.0019 | −1.30 |
| Health fair | 0.2360 * | 0.0022 | 1.53 | 0.4290 * | 0.0018 | 1.23 |
| Health poor | 0.5043 ** | −0.0006 | −0.41 | 0.8393 ** | −0.0004 | −0.29 |
| Health very poor | 0.8589 ** | −0.0187 | −13.21 | 1.4619 ** | −0.0109 | −7.44 |
| Chronic disease | 0.3160 ** | 0.0024 | 1.70 | 0.7588 ** | 0.0030 | 2.07 |
| Disability | 0.1179 ** | −0.0031 | −2.17 | 0.2256 ** | −0.0027 | −1.85 |
| Non-need variables | 0.0058 | 4.09 | −0.0077 | −5.24 | ||
| URBMI | −0.0946 | −0.0017 | −1.18 | −0.1318 | −0.0012 | −0.80 |
| NRCMS | −0.0038 | 0.0004 | 0.31 | −0.0396 | 0.0022 | 1.48 |
| Other health insurance | −0.2430 * | −0.0045 | −3.15 | −0.4807 * | −0.0049 | −3.34 |
| No health insurance | 0.0907 | −0.0002 | −0.17 | 0.0503 | −0.0001 | −0.04 |
| Two kinds of health insurance | 0.0605 | 0.0009 | 0.60 | 0.1157 | 0.0008 | 0.52 |
| Primary school | 0.0678 | −0.0024 | −1.72 | 0.0638 | −0.0011 | −0.75 |
| Middle school | 0.0625 | 0.0018 | 1.30 | −0.0370 | −0.0005 | −0.35 |
| High school | −0.0268 | −0.0012 | −0.84 | −0.2242 | −0.0049 | −3.32 |
| College and above | −0.0018 | 0 | −0.03 | −0.1769 | −0.0019 | −1.29 |
| Central | 0.0305 | −0.0005 | −0.35 | 0.2350 ** | −0.0018 | −1.24 |
| West | 0.1572 ** | −0.0023 | −1.65 | 0.4117 ** | −0.0028 | −1.93 |
| Divorced | −0.0220 | −0.0001 | −0.08 | −0.0166 | 0 | −0.03 |
| Unmarried | 0.0385 | −0.0005 | −0.33 | 0.0626 | −0.0004 | −0.25 |
| Employed | −0.2095 ** | −0.0043 | −3.01 | −0.3614 ** | −0.0039 | −2.63 |
| Self-employed | 0.0636 | 0.0008 | 0.59 | 0.1327 | 0.0008 | 0.55 |
| Not working | 0.2576 ** | 0.0152 | 10.69 | 0.5015 ** | 0.0136 | 9.26 |
| Urban | 0.0403 | 0.0044 | 3.09 | −0.0310 | −0.0016 | −1.10 |
| Living standards | ||||||
| Ln pce 3 | 0.1717 ** | 0.1325 | 93.45 | 0.3046 ** | 0.1136 | 77.19 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, C.; Dou, L.; Wang, H.; Jing, S.; Yin, A. Horizontal Inequity in Health Care Utilization among the Middle-Aged and Elderly in China. Int. J. Environ. Res. Public Health 2017, 14, 842. https://doi.org/10.3390/ijerph14080842
Li C, Dou L, Wang H, Jing S, Yin A. Horizontal Inequity in Health Care Utilization among the Middle-Aged and Elderly in China. International Journal of Environmental Research and Public Health. 2017; 14(8):842. https://doi.org/10.3390/ijerph14080842
Chicago/Turabian StyleLi, Chaofan, Lei Dou, Haipeng Wang, Shanshan Jing, and Aitian Yin. 2017. "Horizontal Inequity in Health Care Utilization among the Middle-Aged and Elderly in China" International Journal of Environmental Research and Public Health 14, no. 8: 842. https://doi.org/10.3390/ijerph14080842