
A Youth-Led, Social Marketing Intervention Run by Adolescents to Encourage Healthy Lifestyles among Younger School Peers (EYTO-Kids Project): A Protocol for Pilot Cluster Randomized Controlled Trial (Spain)

 , , and
, , and
Abstract
:1. Background
2. Methods/Design
2.1. Study Aims
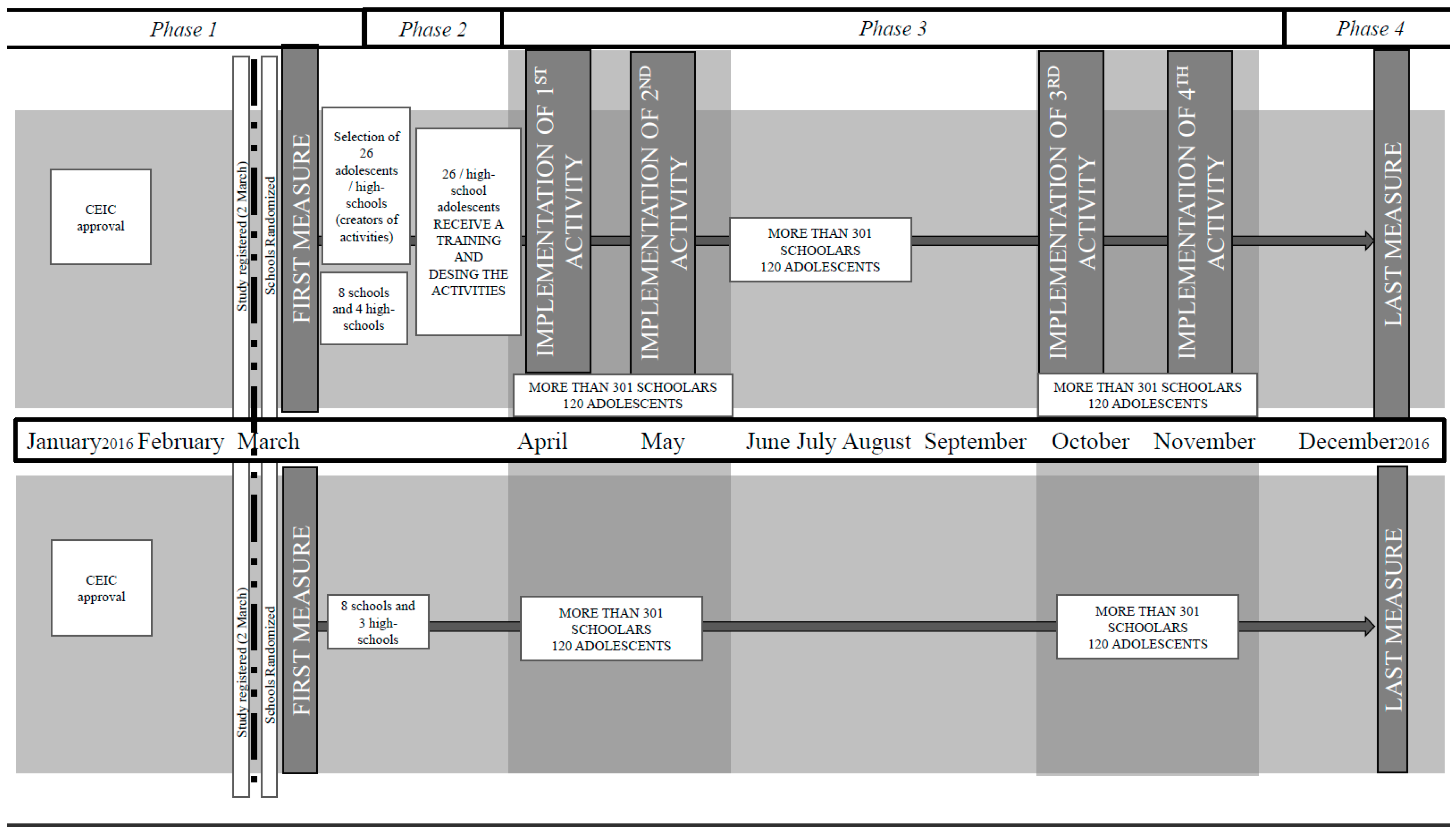
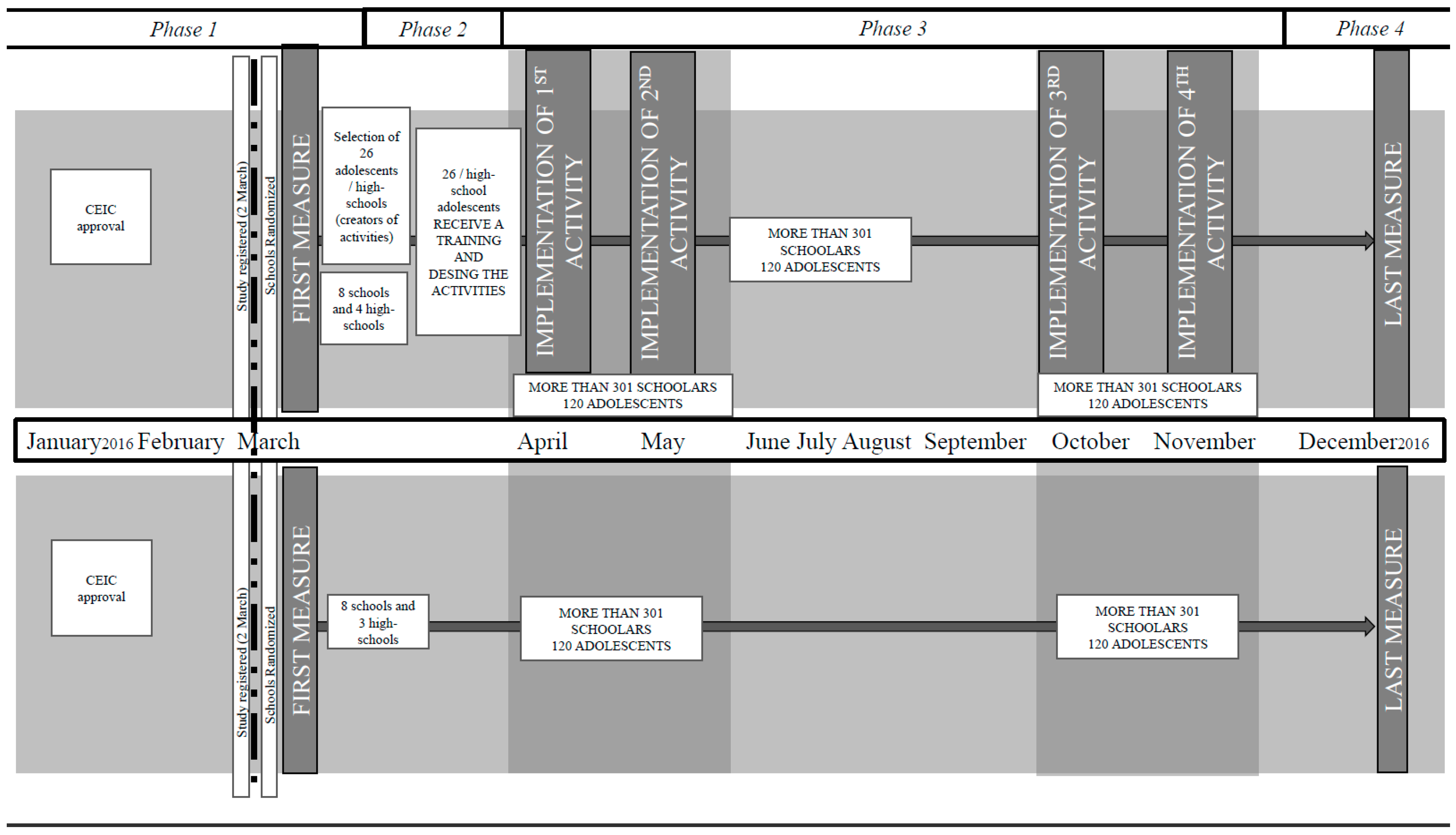
2.2. Study Design and Setting
2.3. Youth Participants and Professional Experts
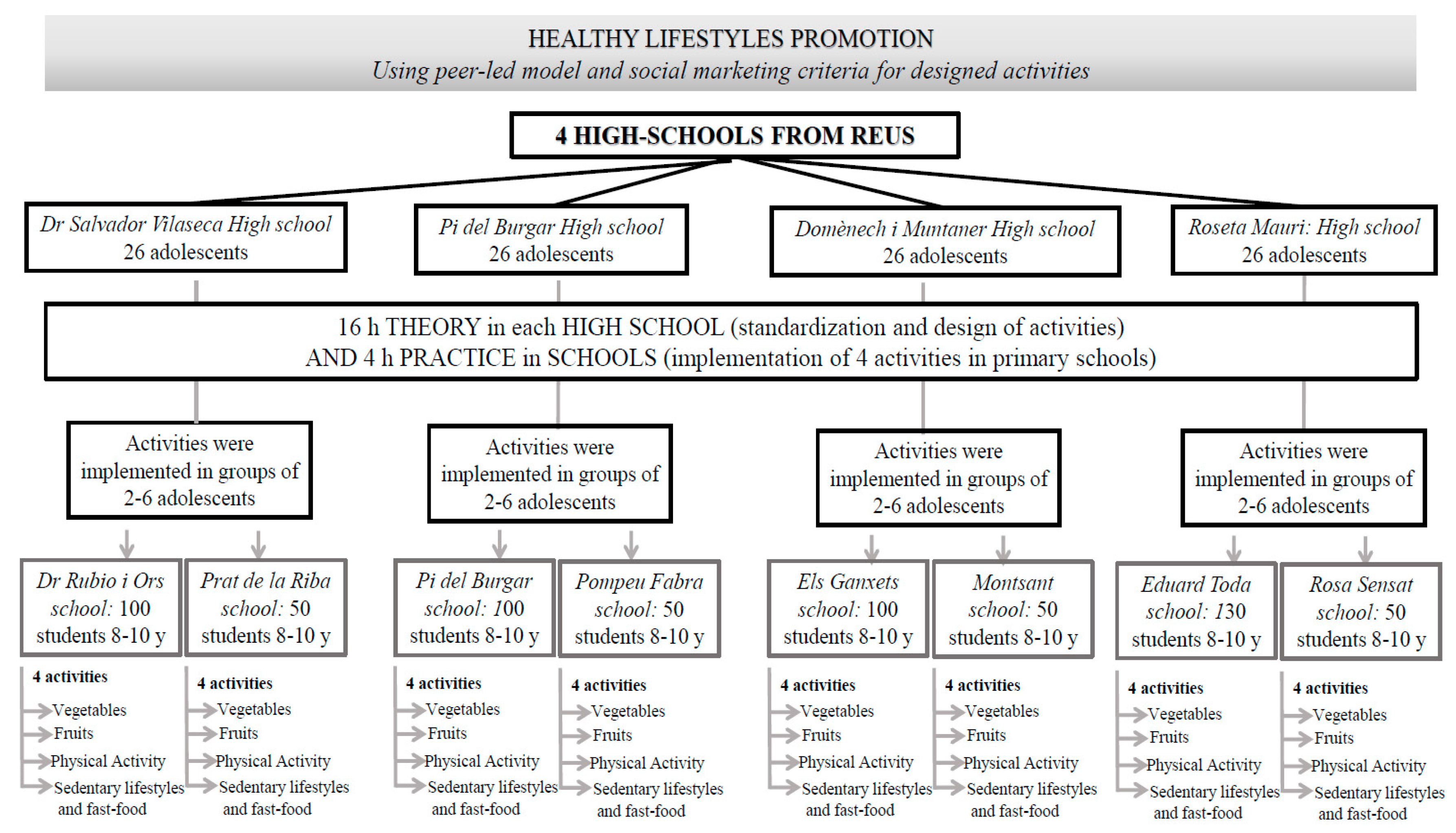
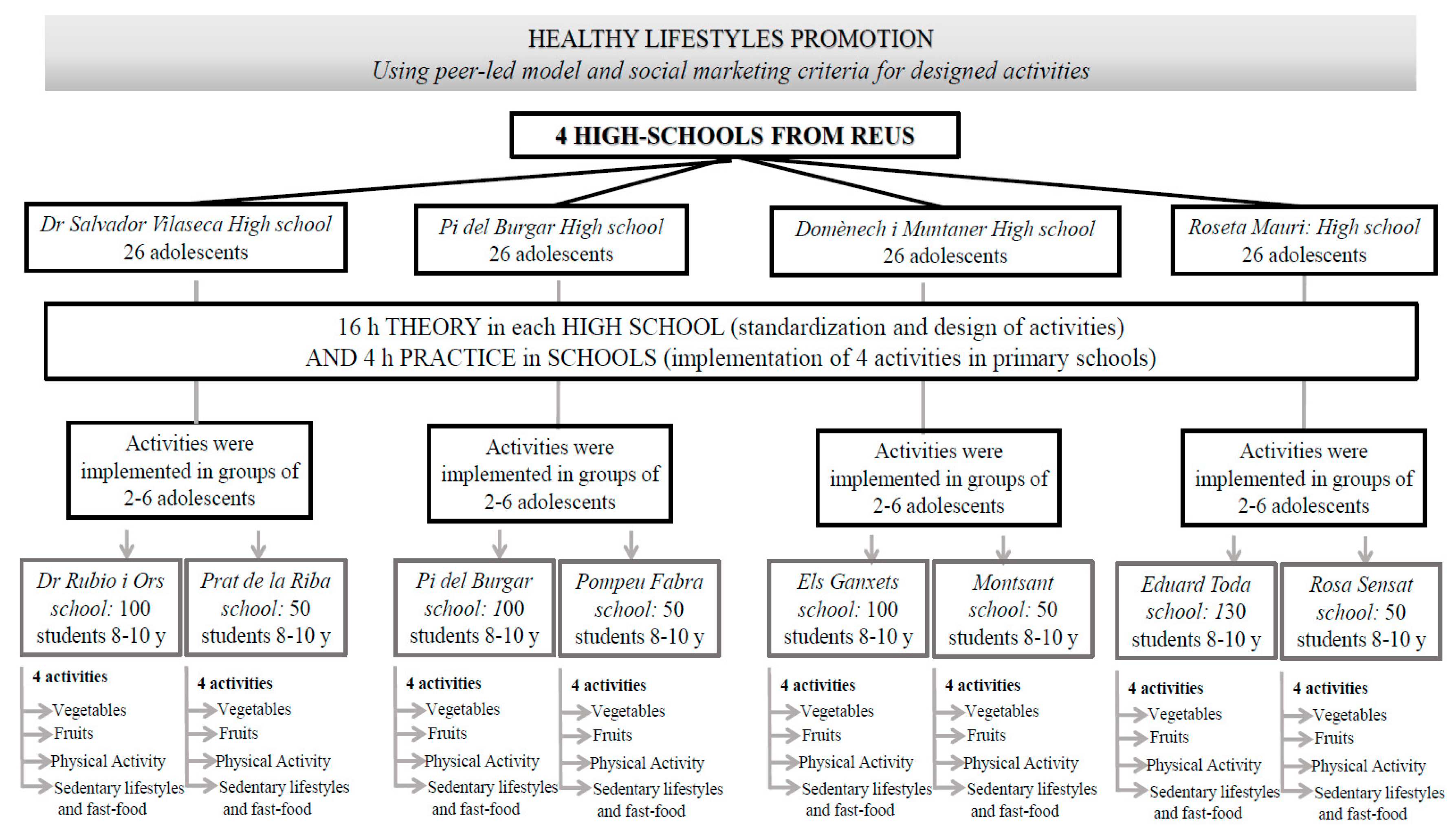
2.3.1. ACs in High Schools
2.3.2. Younger School Peers in Primary Schools
2.3.3. Professionals Experts
2.4. Intervention
2.4.1. Selection of Adolescents and Process of Contact in High Schools
2.4.2. Training of Adolescents in High Schools and Implementation of Activities in Primary Schools
- Customer orientation: To gear the intervention towards younger school peers in primary schools.
- Behavior: To change behaviors by encouraging healthy lifestyles using knowledge-based theories.
- Theory: To use behavioral theories on behavioral change: involvement of adolescents in projects focused on youth populations.
- Insight: To motivate adolescents and younger school peers: adolescents are closer in age to their younger school peers and therefore understand the interests of this younger population.
- Exchange: To evaluate the costs of healthy lifestyle changes.
- Competition: To identify the difficulties faced by younger school peers in following a healthy lifestyle, and to involve stakeholders in the intervention: high schools, primary schools, parents, the local community and local food markets.
- Segmentation: To select a specific population: adolescents in the first and second years of high school and younger school peers in the third and fourth grades of primary schools in Reus.
- Methods mix: To use different methods to transmit the healthy lifestyle messages (activities implemented in the school, visual material, and products tasting).
- -
- The ACs will design 4 activities based on the 8 SMBC and will be supervised by the physicians and nutritionists specializing in health education and promotion (6 h). The 26 ACs for each of the 4 intervention high schools will lead 4 activities involving healthy lifestyles, with a total of 104 ACs.
- -
- Exhibition of activities designed by the ACs for the ACs of the other high schools (2 h).
- -
- Standardization and training in each high school regarding the 4 activities designed by the ACs (6 h). The AC activities will be standardized with those of other high school ACs to accurately implement each activity in all of the primary school interventions. To achieve standardization, the activities will be written as theatre scripts, and the ACs will repeat the activities until all of the ACs transmit the same health message.
- -
- In groups of 2–6 ACs from the same high schools, the ACs will implement the activities designed for primary schools (4 h) according to Table 1.
2.5. Primary and Secondary Outcomes
2.6. Sample Size
2.7. Statistical Analysis Plan
3. Discussion
4. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lobstein, T.; Jackson-Leach, R.; Moodie, M.L.; Hall, K.D.; Gortmaker, S.L.; Swinburn, B.A.; James, W.P.T.; Wang, Y.; McPherson, K. Child and adolescent obesity: Part of a bigger picture. Lancet 2015, 385, 2510–2520. [Google Scholar] [CrossRef]
- McLaren, L. Socioeconomic status and obesity. Epidemiol. Rev. 2007, 29, 29–48. [Google Scholar] [CrossRef] [PubMed]
- Story, M.; Lytle, L.A.; Birnbaum, A.S.; Perry, C.L. Preadolescent and adolescent influences and health. In Promoting Health: Intervention Strategies from Social and Behavioral Research; National Academy Press: Washington, DC, USA, 2000; pp. 217–253. [Google Scholar]
- Organización Mundial de la Salud. Estrategia Mundial Sobre el Régimen Alimentario, Actividad Física y Salud. Available online: http://www.who.int (accessed on 2 August 2017).
- Katzmarzyk, P.T.; Dentro, K.; Beals, K.; Crouter, S.; Eisenmann, J.C.; McKenzie, T.L.; Spruijt, D. The 2014 United States Report Card on Physical Activity for Children & Youth. National Physical Activity Plan, 2014. Available online: http://www.physicalactivityplan.org/reportcard/NationalReportCard_longform_final%20for%20web.pdf (accessed on 5 August 2017).
- Palenzuela Paniagua, S.M.; Pérez Milena, A.; Pérula de Torres, L.A.; Fernández García, J.A.; Maldonado Alconada, J. Food consumption patterns among adolescents. An. Sist. Sanit. Navar. 2014, 37, 47–58. [Google Scholar] [CrossRef] [PubMed]
- Valverde, P.R.; Rodríguez, M. Desarrollo Adolescente y Salud en España: Resumen del Estudio Health Behaviour in School Aged Children 2011, (HBSC-2006). Available online: https://www.msssi.gob.es/profesionales/saludPublica/prevPromocion/promocion/saludJovenes/docs/Divulgativo_completo_HBSC2006.pdf (accessed on 5 August 2017).
- Gracia-Marco, L.; Vicente-Rodríguez, G.; Borys, J.M.; Le Bodo, Y.; Pettigrew, S.; Moreno, L.A. Contribution of social marketing strategies to community-based obesity prevention programmes in children. Int. J. Obes. 2011, 35, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, A.R. Social marketing: Its definition and domain. J. Public Policy Mark. 1994, 13, 108–114. [Google Scholar] [CrossRef]
- French, J.; Blair-Stevens, C. Social Marketing: National Benchmark Criteria; National Social Marketing Centre: London, UK, 2006. [Google Scholar]
- Evans, W.D.; Christoffel, K.K.; Necheles, J.W.; Becker, A.B. Social marketing as a childhood obesity prevention strategy. Obesity 2010, 18, S23–S26. [Google Scholar] [CrossRef] [PubMed]
- Aceves-Martins, M.; Llauradó, E.; Tarro, L.; Moreno-García, C.F.; Trujillo Escobar, T.G.T.; Solà, R.; Giralt, M. Effectiveness of social marketing strategies to reduce youth obesity in European school-based interventions: A systematic review and meta-analysis. Nutr. Rev. 2016, 74, 337–351. [Google Scholar] [CrossRef] [PubMed]
- Georgie, J.M.; Sean, H.; Deborah, M.C.; Matthew, H.; Rona, C. Peer-led interventions to prevent tobacco, alcohol and/or drug use among young people aged 11–21 years: A systematic review and meta-analysis. Addiction 2016, 111, 391–407. [Google Scholar] [CrossRef] [PubMed]
- Story, M.; Lytle, L.A.; Birnbaum, A.S.; Perry, C.L. Peer-led, school-based nutrition education for young adolescents: Feasibility and process evaluation of the TEENS study. J. Sch. Health 2002, 72, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.L.; Audrey, S.; Cooper, A.R.; Noble, S.; Campbell, R. Lessons from a peer-led obesity prevention programme in English schools. Health Promot. Int. 2017, 32, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Santos, R.G.; Durksen, A.; Rabbanni, R.; Chanoine, J.P.; Lamboo Miln, A.; Mayer, T.; McGavock, J.M. Effectiveness of peer-based healthy living lesson plans on anthropometric measures and physical activity in elementary school students: A cluster randomized trial. JAMA Pediatr. 2014, 168, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Stock, S.; Miranda, C.; Evans, S.; Plessis, S.; Ridley, J.; Yeh, S.; Chanoine, J.P. Healthy Buddies: A novel, peer-led health promotion program for the prevention of obesity and eating disorders in children in elementary school. Pediatrics 2007, 120, e1059–e1068. [Google Scholar] [CrossRef] [PubMed]
- Llauradó, E.; Aceves-Martins, M.; Tarro, L.; Papell-Garcia, I.; Puiggròs, F.; Arola, L.; Prades-Tena, J.; Montagut, M.; Moragas-Fernández, C.M.; Solà, R.; et al. A youth-led social marketing intervention to encourage healthy lifestyles, the EYTO (European Youth Tackling Obesity) project: A cluster randomised controlled trial in Catalonia, Spain. BMC Public Health 2015, 15, 607. [Google Scholar] [CrossRef] [PubMed]
- Aceves-Martins, M.; Llauradó, E.; Tarro, L.; Moriña, D.; Papell-Garcia, I.; Prades-Tena, J.; Kettner-Hoeberg, H.; Puiggròs, F.; Arola, L.; Davies, A.; et al. A school-based, peer-led, social marketing intervention to engage Spanish adolescents in a healthy lifestyle (“We are cool”-Som la Pera Study): A parallel-cluster randomized controlled study. Child Obes. 2017, 13, 300–313. [Google Scholar] [CrossRef] [PubMed]
- Urbaniak, G.C.; Scott, P. Research Randomizer. Available online: https://www.randomizer.org (accessed on 9 January 2016).
- Serra Majem, L.; Ribas Barba, L.; Aranceta Bartrina, J.; Pérez Rodrigo, C.; Saavedra Santana, P.; Peña Quintana, L. Obesidad infantily juvenil en España. Resultados del Estudio enKid (1998–2000). Med. Clin. 2003, 121, 725–732. [Google Scholar] [CrossRef]
- Llargués, E.; Franco, R.; Recasens, A.; Nadal, A.; Vila, M.; José Pérez, M.; Martínez-Mateo, F.; Recasens, I.; Salvador, G.; Serra, J.; et al. Weight, dietary patterns and exercise habits in first-year primary school children: The AVall study. Endocrinol. Nutr. 2009, 56, 287–292. [Google Scholar] [CrossRef]
- Currie, C.; Griebler, R.; Inchley, J.; Theunissen, A.; Molcho, M.; Samdal, O.; Dür, W. Health Behaviour in School-Aged Children (HBSC) Study Protocol: Background, Methodology and Mandatory Items for the 2009/10 Survey; CAHRU & Vienna: Edinburgh, UK, 2010. [Google Scholar]
- Wright, N.D.; Groisman-Perelstein, A.E.; Wylie-Rosett, J.; Vernon, N.; Diamantis, P.M.; Isasi, C.R. A lifestyle assessment and intervention tool for pediatric weight management: The HABITS questionnaire. J. Hum. Nutr. Diet. 2011, 24, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.B. Basic ideas of multiple imputation for nonresponse. Surv. Methodol. 1986, 12, 37–47. [Google Scholar]
- Stef, V.B.; Karin, G.O. Mice: Multivariate imputation by chained equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar]
- R Core Team R. A Language and Environment for Statistical Computing; The R Foundation for Statistical Computing: Vienna, Austria, 2016. [Google Scholar]
- De Bourdeaudhuij, I.; Verbestel, V.; De Henauw, S.; Maes, L.; Huybrechts, I.; Mårild, S.; Eiben, G.; Moreno, L.A.; Barba, G.; Kovács, É.; et al. Behavioural effects of a community based intervention for prevention of childhood obesity in eight European countries. Main results from the IDEFICS study. Obes. Rev. 2015, 16, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Sisson, S.B.; Broyles, S.T.; Baker, B.L.; Katzmarzyk, P.T. Television, reading, and computer time: Correlates of school-day leisure-time sedentary behavior and relationship with overweight in children in the U.S. J. Phys. Act. Health 2011, 8, S188–S197. [Google Scholar] [CrossRef] [PubMed]
- Currie, C.; Zanotti, C.; Morgan, A.; Currie, D.; de Looze, M.; Roberts, C.; Samdal, O.; Smith, O.R.F.; Barnekow, V. Social Determinants of Health and Well-Being Among Young People. Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2009/2010 Survey; World Health Organization: Copenhagen, Denmark, 2012. [Google Scholar]
- Roberts, C.; Freeman, J.; Samdal, O.; Schnohr, C.W.; de Looze, M.E.; Nic Gabhainn, S.; Iannotti, R.; Rasmussen, M.; International HBSC Study Group. The Health Behaviour in School-Aged Children (HBSC) study: Methodological developments and current tensions. Int. J. Public Health 2009, 54, 140–150. [Google Scholar] [CrossRef] [PubMed]
- Gortmaker, S.L.; Wang, Y.C.; Long, M.W.; Giles, C.M.; Ward, Z.J.; Barrett, J.L.; Kenney, E.L.; Sonneville, K.R.; Afzal, A.S.; Resch, S.C.; et al. Three interventions that reduce childhood obesity are projected to save more than they cost to implement. Health Aff. 2015, 34, 1932–1939. [Google Scholar] [CrossRef] [PubMed]
- Kotler, P.; Roberto, E.L. Social Marketing Strategies for Changing Public Behavior; Free Press: New York, NY, USA, 2002. [Google Scholar]
- Storey, J.D.; Saffitz, G.B.; Rimón, J.G. Social marketing. In Health Behavior and Health Education: Theory, Research and Practice; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 435–464. [Google Scholar]
- Bammann, K.; Peplies, J.; Henauw, D.S.; Hunsberger, M.; Molnar, D.; Moreno, L.A.; Tornaritis, M.; Veidebaum, T.; Ahrens, W.; Siani, A.; et al. Early life course risk factors for childhood obesity: The IDEFICS case-control study. PLoS ONE 2014, 9, e86914. [Google Scholar] [CrossRef] [PubMed]
- Langley-Evans, S.C.; Moran, V.H. Childhood obesity: Risk factors, prevention and management. Matern. Child Nutr. 2014, 10, 453–455. [Google Scholar] [CrossRef] [PubMed]
- Telama, R.; Yang, X.; Leskinen, E.; Kankaanpää, A.; Hirvensalo, M.; Tammelin, T.; Viikari, J.S.A.; Raitakari, O.T. Tracking of physical activity from early childhood through youth into adulthood. Med. Sci. Sports Exerc. 2014, 46, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Enquesta de Salut de Catalunya 2014. Principals Resultats, 2015. Departament de Salut, Catalunya, Spain. Available online: http://salutweb.gencat.cat/ca/el_departament/estadistiques_sanitaries/enquestes/esca/resultats_enquesta_salut_catalunya/ (accessed on 2 August 2017).

{kind=link}
{kind=link}
| Hours | Subject Matter | Adolescents |
|---|---|---|
| 2 h | Nutrition, healthy lifestyles, social marketing topics and tools to transmit healthy messages in each high school, taught by health professionals from Faculty of Medicine and Health Sciences from Rovira i Virgili University. | |
| 6 h | Design of 4 healthy lifestyle promotion activities: the adolescents (in groups composed of 2–6 members) had 6 h to design an activity geared towards third and fourth grade students (8–9 years old) with the following aims:
| Twenty-six adolescents per high school designed an activity related to each aim. In total, 4 activities of 1 h each were related to the project aims. |
| 2 h | Combined session in FMCS. | The 4 activities were designed by 4 high schools (1 activity per high school) during a combined session with 104 adolescents (26 adolescents per high school) with a common understanding of the 4 activities. Each high school had 30 minutes to present the activity in front of the other adolescents. |
| 6 h | To standardize the activities, after designing the entire session, 26 adolescents per high school (104 adolescents) had to learn the 4 activities and reproduce them in the same form to implement the activities in all schools and transmit the same health message in the same manner. | During the 15 days prior to implementation of each activity, a professional from FMCS helped standardize the activities in each high school. |
| 4 h | Finally, the adolescents visited schools to implement the activities among third and fourth grade students. | In each high school, the 26 adolescents were in groups composed of 2–6 members and implemented the activities (1 h/activity) in the classrooms of each school near the high school. Activity 1: April 2016 Activity 2: May 2016 Activity 3: October 2016 Activity 4: November 2016 |
| 20 h total | ||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarro, L.; Aceves-Martins, M.; Papell-Garcia, I.; Arola, L.; Giralt, M.; Llauradó, E.; Solà, R. A Youth-Led, Social Marketing Intervention Run by Adolescents to Encourage Healthy Lifestyles among Younger School Peers (EYTO-Kids Project): A Protocol for Pilot Cluster Randomized Controlled Trial (Spain). Int. J. Environ. Res. Public Health 2017, 14, 923. https://doi.org/10.3390/ijerph14080923
Tarro L, Aceves-Martins M, Papell-Garcia I, Arola L, Giralt M, Llauradó E, Solà R. A Youth-Led, Social Marketing Intervention Run by Adolescents to Encourage Healthy Lifestyles among Younger School Peers (EYTO-Kids Project): A Protocol for Pilot Cluster Randomized Controlled Trial (Spain). International Journal of Environmental Research and Public Health. 2017; 14(8):923. https://doi.org/10.3390/ijerph14080923
Chicago/Turabian StyleTarro, Lucia, Magaly Aceves-Martins, Ignasi Papell-Garcia, Lluís Arola, Montse Giralt, Elisabet Llauradó, and Rosa Solà. 2017. "A Youth-Led, Social Marketing Intervention Run by Adolescents to Encourage Healthy Lifestyles among Younger School Peers (EYTO-Kids Project): A Protocol for Pilot Cluster Randomized Controlled Trial (Spain)" International Journal of Environmental Research and Public Health 14, no. 8: 923. https://doi.org/10.3390/ijerph14080923