
Association between Functional Movements Skills and Health Indicators in Children Aged between 9 and 12 Years Old


Abstract
:1. Introduction
2. Methods
2.1. Study Design and Population
2.2. PLAYbasic
2.3. Passport for Life
2.4. Primary Outcomes
2.5. Statistical Analysis
3. Results
3.1. General Characteristics of the Sample
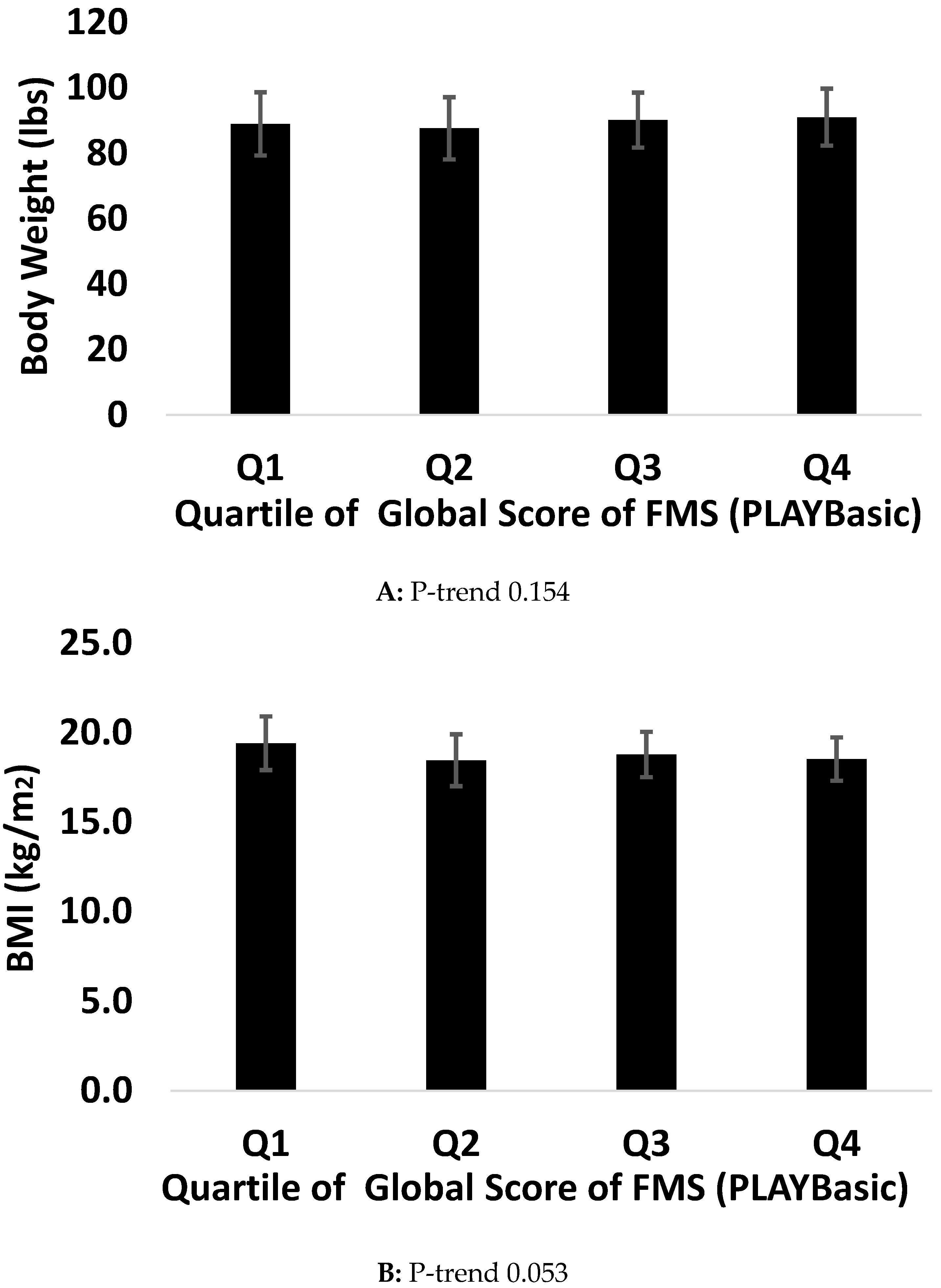
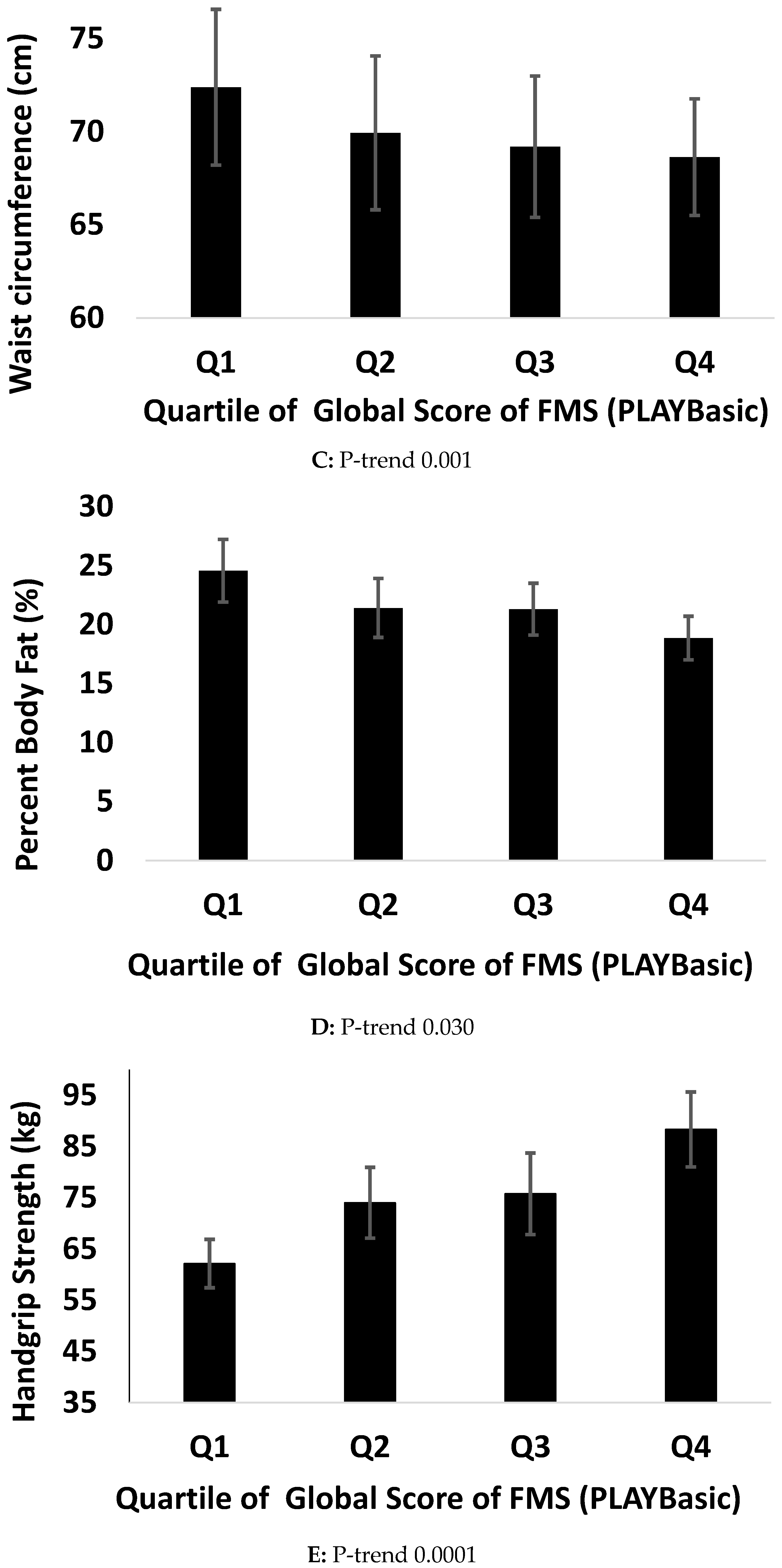
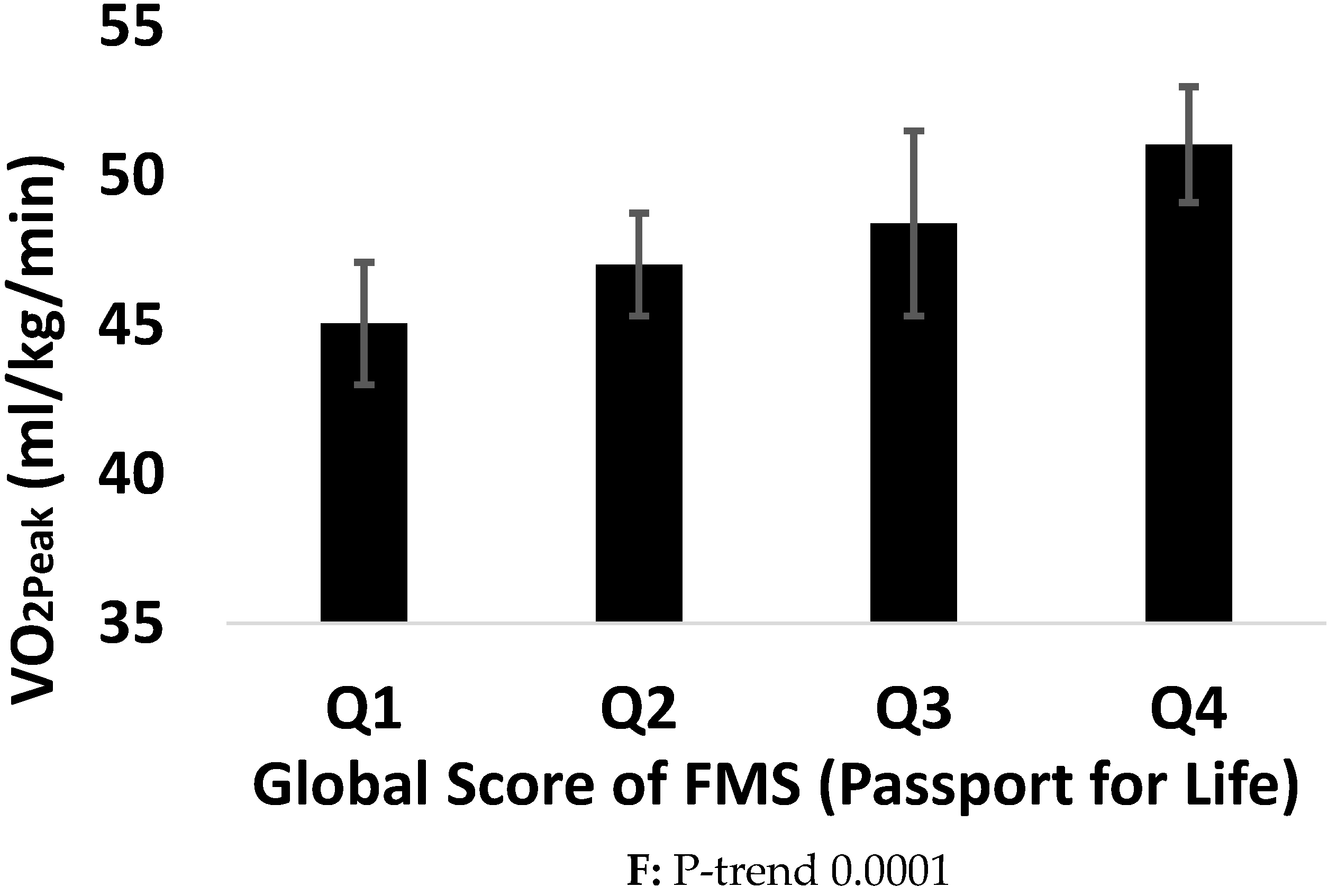
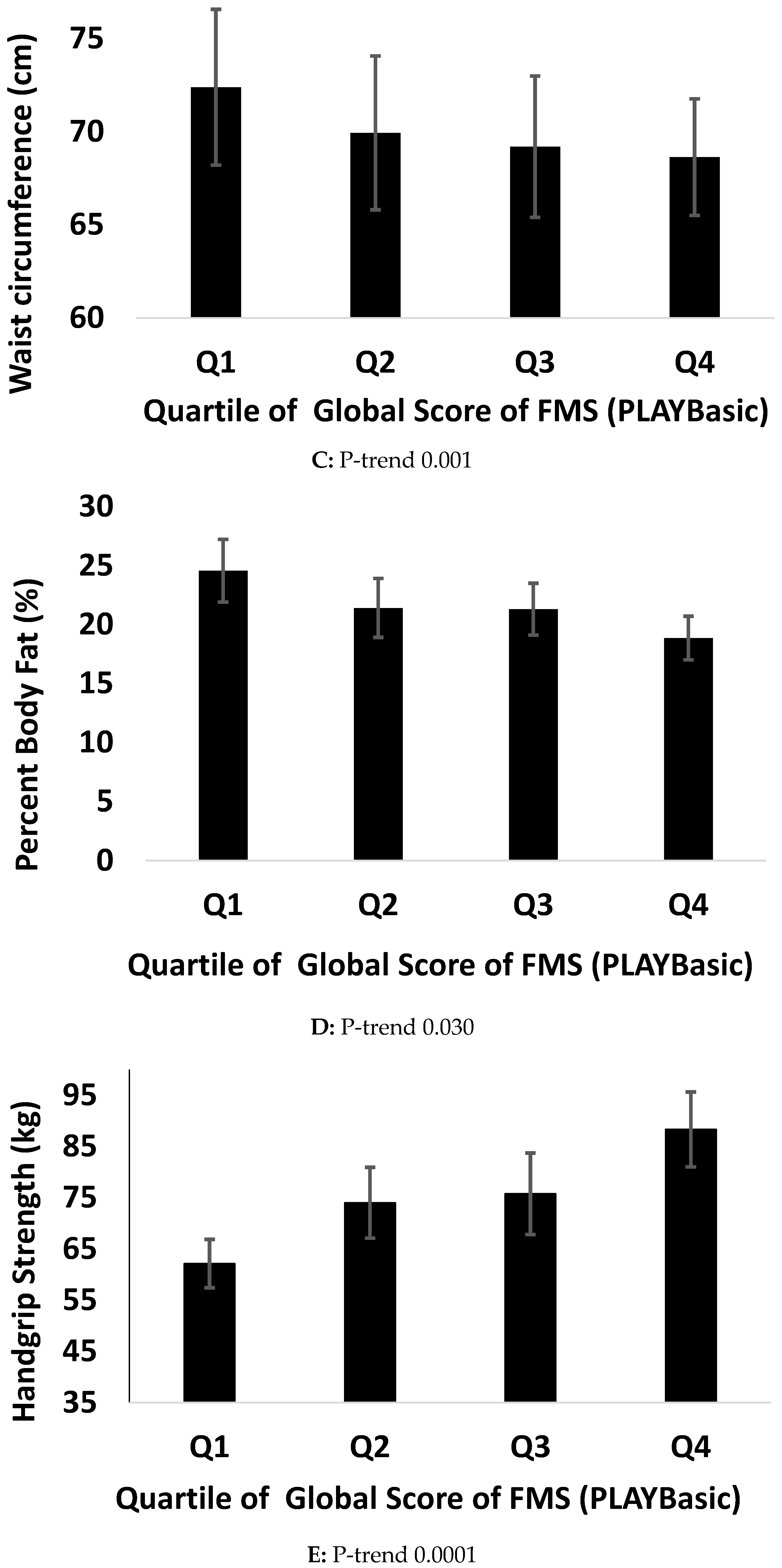
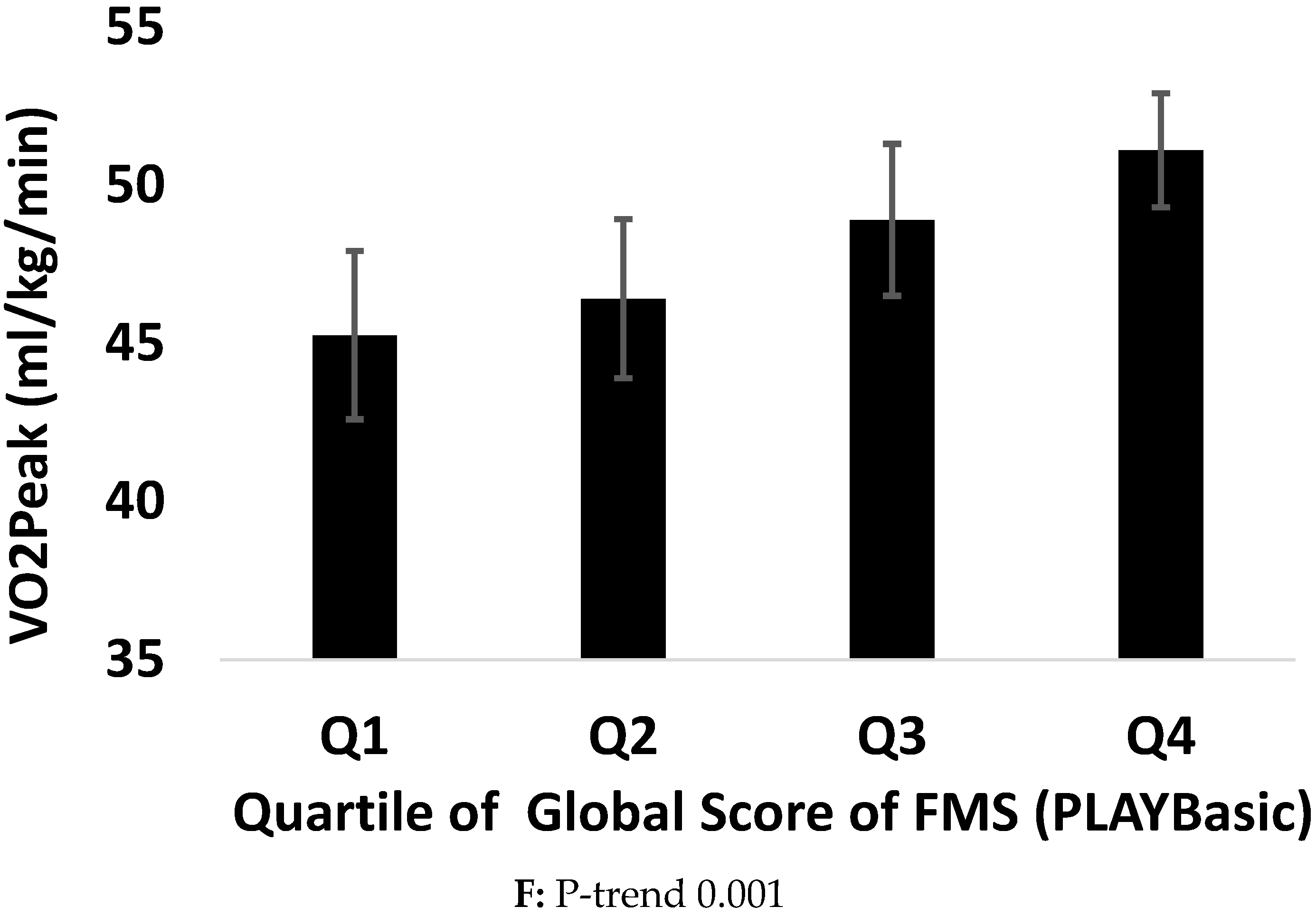
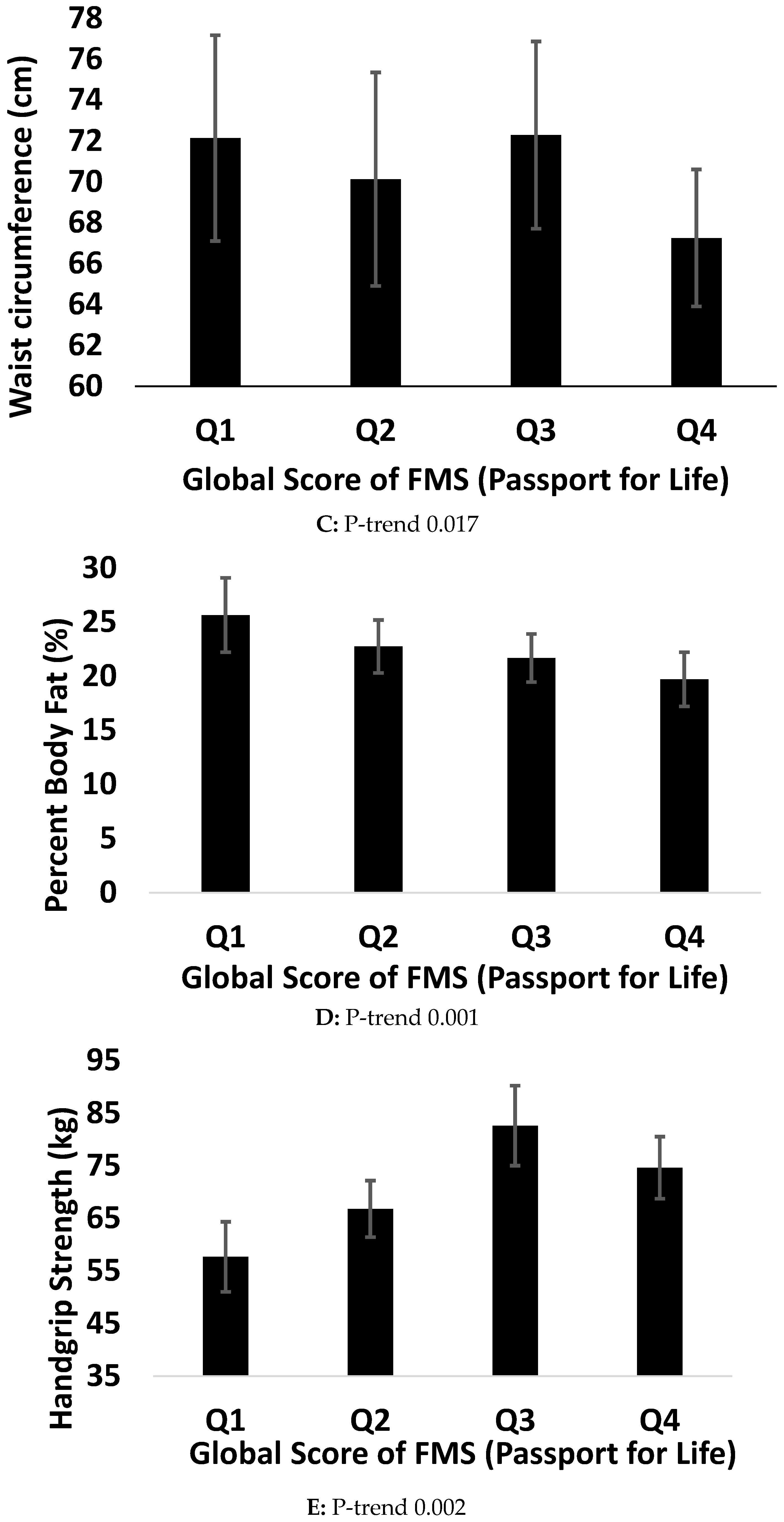
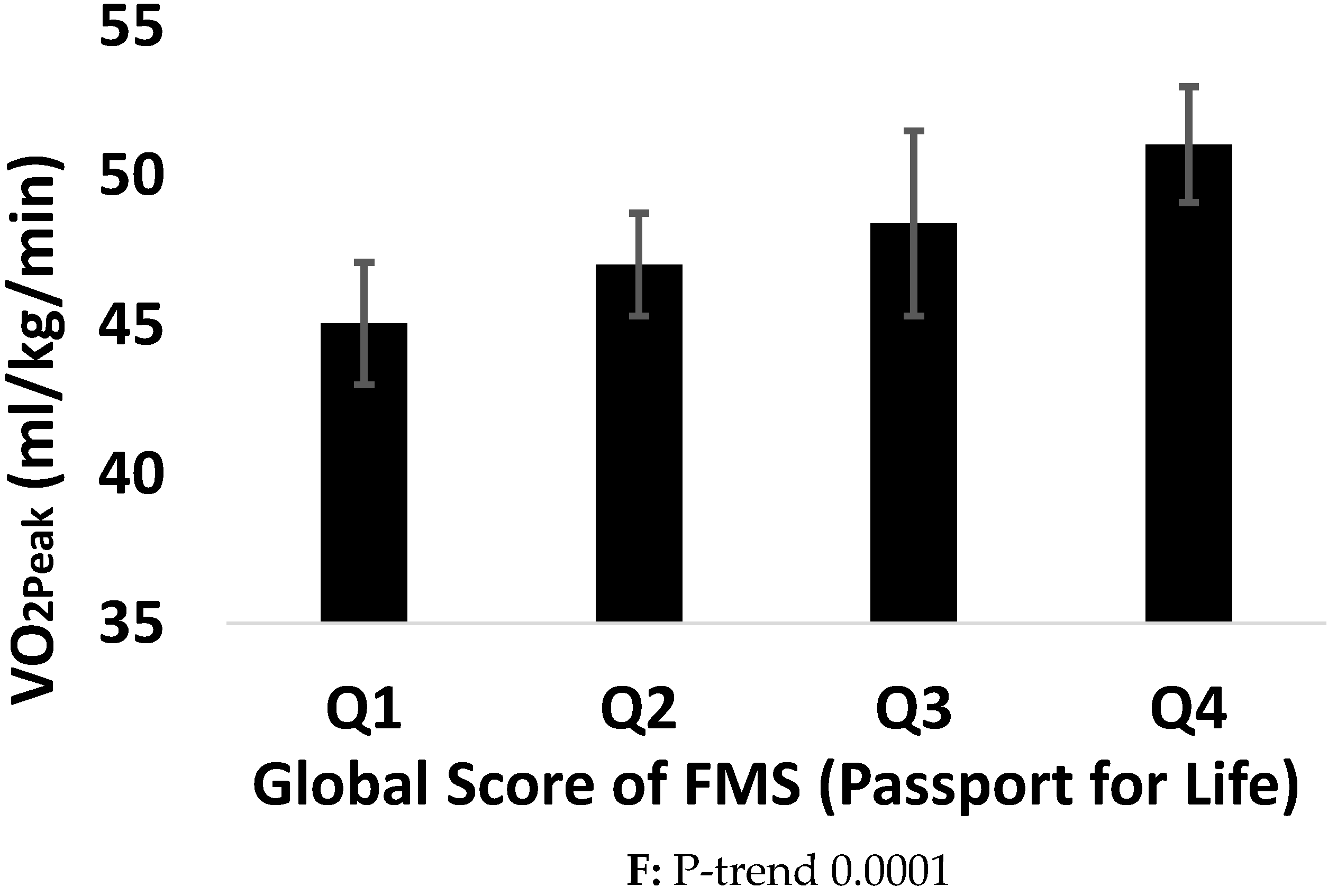
3.2. Association Between Health Indicators and FMS
3.3. Comparing Associations between Tools and Health Indicators
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Tremblay, M.S.; Shields, M.; Laviolette, M.; Craig, C.L.; Janssen, I.; Connor Gorber, S. Fitness of Canadian Children and Youth: Results from the 2007–2009 Canadian Health Measures Survey. Health Rep. 2010, 21, 7–20. [Google Scholar] [PubMed]
- Williams, H.G.; Pfeiffer, K.A.; O’Neill, J.R.; Dowda, M.; McIver, K.L.; Brown, W.H.; Pate, R.R. Motor skill performance and physical activity in preschool children. Obesity (Silver Spring) 2008, 16, 1421–1426. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, M.; Saunders, T.J.; Bremer, E.; Tremblay, M.S. Long-term importance of fundamental motor skills: A 20-year follow-up study. Adapt. Phys. Act. Quart. 2014, 31, 67–78. [Google Scholar] [CrossRef] [PubMed]
- Henrique, R.S.; Re, A.H.; Stodden, D.F.; Fransen, J.; Campos, C.M.; Queiroz, D.R.; Cattuzzo, M.T. Association between sports participation, motor competence and weight status: A longitudinal study. J. Sci. Med. Sport 2016, 19, 825–829. [Google Scholar] [CrossRef] [PubMed]
- Jaakkola, T.; Yli-Piipari, S.; Huotari, P.; Watt, A.; Liukkonen, J. Fundamental movement skills and physical fitness as predictors of physical activity: A 6-year follow-up study. Scand. J. Med. Sci. Sports 2016, 26, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Canadian Health Report Card. 2016. Available online: https://www.participaction.com/sites/default/files/downloads/2016%20ParticipACTION%20Report%20Card%20-%20Presentation.pdf (accessed on 1 September 2017).
- Vameghi, R.; Shams, A.; Shamsipour Dehkordi, P. The effect of age, sex and obesity on fundamental motor skills among 4 to 6 years-old children. Pakistan J. Med. Sci. 2013, 29, 586–589. [Google Scholar] [CrossRef]
- Duncan, M.J.; Bryant, E.; Stodden, D. Low fundamental movement skill proficiency is associated with high BMI and body fatness in girls but not boys aged 6–11 years old. J. Sports Sci. 2016, 35, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lubans, D.R.; Morgan, P.J.; Cliff, D.P.; Barnett, L.M.; Okely, A.D. Fundamental movement skills in children and adolescents: Review of associated health benefits. Sports Med. 2010, 40, 1019–1035. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, W.; Belton, S.; Issartel, J. The relationship between adolescents’ physical activity, fundamental movement skills and weight status. J. Sports Sci. 2016, 34, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- Castetbon, K.; Andreyeva, T. Obesity and motor skills among 4 to 6-year-old children in the United States: Nationally-Representative surveys. BMC Pediatr. 2012, 12, 28. [Google Scholar] [CrossRef] [PubMed]
- Robinson, L.E.; Stodden, D.F.; Barnett, L.M.; Lopes, V.P.; Logan, S.W.; Rodrigues, L.P.; D’Hondt, E. Motor Competence and its Effect on Positive Developmental Trajectories of Health. Sports Med. 2015, 45, 1273–1284. [Google Scholar] [CrossRef] [PubMed]
- Bonvin, A.; Barral, J.; Kakebeeke, T.H.; Kriemler, S.; Longchamp, A.; Marques-Vidal, P.; Puder, J.J. Weight status and gender-related differences in motor skills and in child care-based physical activity in young children. BMC Pediatr. 2012, 12, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kriellaars, D. PLAY Basic. Available online: http://www.physicalliteracy.ca/PLAY/basic (accessed on 5 February 2017).
- Physical & Health Education Canada. Passport for Life. Available online: http://passportforlife.ca/ (accessed on 1 September 2017).
- Logan, S.W.; Robinson, L.E.; Getchell, N. The comparison of performances of preschool children on two motor assessments. Percept. Mot. Skills 2011, 113, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Kriellaars, D. Physical Literacy Assessment for Youth. 2014. Available online: http://physicalliteracy.ca/wp-content/uploads/2016/08/PLAYself_Workbook.pdf (accessed on 1 September 2017).
- CSEP. CSEP-Physical Activity Training for Health (CSEP-PATH). Available online: http://store.csep.ca/CSEP-PATH-Physical-Activity-Training-for-Health_p_52.html (accessed on 1 September 2017).
- Leger, L.; Lambert, J.; Goulet, A.; Rowan, C.; Dinelle, Y. Aerobic capacity of 6 to 17-year-old Quebecois—20 meter shuttle run test with 1 minute stages. Can. J. Appl. Sport. Sci. 1984, 9, 64–69. [Google Scholar] [PubMed]
- Luque, V.; Closa-Monasterolo, R.; Rubio-Torrents, C.; Zaragoza-Jordana, M.; Ferre, N.; Gispert-Llaurado, M.; Escribano, J. Bioimpedance in 7-year-old children: Validation by dual X-ray absorptiometry-part 1: Assessment of whole body composition. Ann. Nutr. Metab. 2014, 64, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.D.; Davis, R.E.; Fu, Y.C. Early motor skill competence as a mediator of child and adult physical activity. Prev. Med. Rep. 2015, 2, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Holfelder, B.; Nadja, S. Relationship of fundamental movement skills and physical activity in children and adolescents: A systematic review. Psychol. Sport. Exerc. 2014, 15, 382–391. [Google Scholar] [CrossRef]
- D’Hondt, E.; Gentier, I.; Deforche, B.; Tanghe, A.; De Bourdeaudhuij, I.; Lenoir, M. Weight loss and improved gross motor coordination in children as a result of multidisciplinary residential obesity treatment. Obesity (Silver Spring) 2011, 19, 1999–2005. [Google Scholar] [CrossRef] [PubMed]
- Bryant, E.S.; Duncan, M.J.; Birch, S.L. Fundamental movement skills and weight status in British primary school children. Eur. J. Sports Sci. 2014, 14, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Lee, K. The relationship between fundamental movement skills and body mass index in Korean preschool children. Eur. Early Child. Educ. Res. J. 2016, 24, 928–935. [Google Scholar] [CrossRef]
- Wind, A.E.; Takken, T.; Helders, P.J.; Engelbert, R.H. Is grip strength a predictor for total muscle strength in healthy children, adolescents, and young adults? Eur. J. Pediat. 2010, 169, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Rioux, B.V.; Kuwornu, P.; Sharma, A.; Tremblay, M.S.; Mcgavock, J.M.; Sénéchal, M. Association Between Handgrip Muscle Strength and Cardio-Metabolic Z-Score in Children 6 to 19 Years of Age: Results from the Canadian Health Measures Survey. Metab. Syndr. Relat. Disord. 2017, 15, 379–384. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | n = 145 |
|---|---|
| Age (years) | 10.4 ± 1.2 |
| Boys n (%) | 78 (54.2) |
| Body weight (kg) | 39.8 ± 9.2 |
| Body Mass Index (kg/m2) | 18.5 ± 2.9 |
| Body Mass Index z-score | 0.37 ± 1.0 |
| Waist Circumference (cm) | 69.0 ± 8.7 |
| Handgrip Strength (lb) | 74.8 ± 21.9 |
| VO2peak (mL/kg/min) # | 48.1 ± 3.9 |
| Percent Body Fat (%) | 21.5 ± 6.2 |
| PLAYbasic (0–100) | |
| Run There and Back | 62.9 ± 20.6 |
| Hop | 61.6 ± 21.6 |
| Overhead Throw | 70.2 ± 19.6 |
| Kick Ball | 62.3 ± 24.6 |
| Balance Walk Backward | 63.0 ± 19.0 |
| Average Score | 64.0 ± 15.8 |
| Passport for Life (0–4) | |
| Lateral Bound | 3.4 ± 0.7 |
| Plank | 2.6 ± 1.1 |
| Circuit | 1.8 ± 1.2 |
| Run, Stop, Return | 3.0 ± 0.8 |
| Throw and Catch | 3.1 ± 1.1 |
| Kicks | 2.7 ± 1.0 |
| Average Score | 2.8 ± 0.7 |
| Body Weight | BMI | Waist Circumference | Percent Body Fat | Handgrip Strength | VO2peak # | |
|---|---|---|---|---|---|---|
| PLAYbasic | ||||||
| Run There and Back | −0.18 (0.03) | −0.29 (0.001) | −0.35 (0.001) | −0.45 (0.001) | 0.29 (0.001) | 0.47 (0.002) |
| Hop | −0.19 (0.26) | −0.30 (0.001) | −0.32 (0.001) | −0.38 (0.001) | 0.24 (0.004) | 0.48 (0.001) |
| Overhand Throw | 0.17 (0.044) | 0.06 (0.445) | 0.021 (0.798) | −0.17 (0.051) | 0.33 (0.001) | 0.41 (0.008) |
| Kick Ball | 0.21 (0.011) | 0.16 (0.054) | 0.11 (0.186) | −0.15 (0.071) | 0.39 (0.001) | 0.49 (0.001) |
| Balance Walk Backwards | 0.01 (0.907) | −0.13 (0.121) | −0.09 (0.295) | −0.26 (0.002) | 0.28 (0.001) | 0.34 (0.026) |
| Average Score | −0.002 (0.977) | −0.11 (0.171) | −0.17 (0.037) | −0.33 (0.001) | 0.41 (0.001) | 0.60 (0.001) |
| Passport for Life | ||||||
| Lateral Bound | −0.16 (0.063) | −0.17 (0.042) | −0.21 (0.014) | −0.19 (0.028) | 0.15 (0.076) | 0.22 (0.164) |
| Plank | −0.17 (0.43) | −0.24 (0.004) | −0.27 (0.001) | −0.33 (0.001) | 0.27 (0.001) | 0.44 (0.003) |
| Circuit | −0.23 (0.007) | −0.29 (0.001) | −0.31 (0.001) | −0.37 (0.001) | 0.27 (0.001) | 0.54 (0.001) |
| Run, Stop, Return | −0.17 (0.042) | −0.32 (0.001) | −0.33 (0.001) | −0.47 (0.001) | 0.37 (0.001) | 0.55 (0.001) |
| Throw and Catch | 0.22 (0.020) | 0.043 (0.654) | 0.20 (0.036) | −0.15 (0.126) | 0.38 (0.001) | 0.20 (0.203) |
| Kicks | 0.20 (0.015) | 0.12 (0.150) | 0.083 (0.322) | −0.19 (0.025) | 0.39 (0.001) | 0.57 (0.001) |
| Average Score | −0.09 (0.323) | −0.22 (0.023) | −0.18 (0.520) | −0.37 (0.001) | 0.38 (0.001) | 0.60 (0.001) |
| Body Weight | BMI | Waist Circumference | Handgrip Strength | Percent Body Fat | VO2peak # | |
|---|---|---|---|---|---|---|
| Run There and Back | −0.40 ± 0.10 ‡ | −0.07 ± 0.01 ‡ | −0.24 ± 0.04 ‡ | 0.16 ± 0.08 * | −0.15 ± 0.03 ‡ | 0.10 ± 0.03 ‡ |
| Hop | −0.33 ± 0.10 ‡ | −0.06 ± 0.01 ‡ | −0.20 ± 0.04 ‡ | 0.13 ± 0.08 | −0.12 ± 0.03 ‡ | 0.10 ± 0.02 ‡ |
| Overhand Throw | 0.11 ± 0.12 | 0.01 ± 0.18 | 0.26 ± 0.05 | 0.18 ± 0.09 * | −0.01 ± 0.03 | 0.60 ± 0.03 * |
| Kick Ball | 0.13 ± 0.10 | 0.01 ± 0.01 | 0.01 ± 0.04 | 0.19 ± 0.07 ‡ | −0.01 ± 0.03 | 0.05 ± 0.03 * |
| Balance Walk Backwards | −0.25 ± 0.1 * | −0.04 ± 0.02 ‡ | −0.15 ± 0.50 ‡ | 0.17 ± 0.14 * | −0.10 ± 0.30 ‡ | 0.06 ± 0.03 * |
| Average Score | −0.30 ± 0.4 * | −0.06 ± 0.02 ‡ | −0.24 ± 0.06 ‡ | 0.33 ± 0.11 ‡ | −0.15 ± 0.04 ‡ | 0.15 ± 0.03 |
| Body Weight | BMI | Waist Circumference | Handgrip Strength | Percent Body Fat | VO2peak # | |||
|---|---|---|---|---|---|---|---|---|
| Lateral Bound | −6.51 ± 2.90 * | −1.10 ± 20.50 * | −2.90 ± 1.30 * | 2.44 ± 2.26 | −1.86 ± 0.82 * | 1.22 ± 0.81 | ||
| Plank | −6.32 ± 1.80 ‡ | −1.02 ± 0.28 ‡ | −3.41 ± 0.80 ‡ | 3.00 ± 1.44 * | −2.02 ± 0.51 ‡ | 1.41 ± 0.45 ‡ | ||
| Circuit | −6.90 ± 1.60 ‡ | −1.04 ± 0.25 ‡ | −3.46 ± 0.71 ‡ | 2.90 ± 1.31 * | −196 ± 0.45 ‡ | 1.65 ± 0.38 ‡ | ||
| Run, Stop, Return | −11.30 ± 2.40 ‡ | −2.00 ± 0.40 ‡ | −6.30 ± 1.05 ‡ | 5.54 ± 1.97 ‡ | −4.22 ± 0.64 ‡ | 2.91 ± 0.64 ‡ | ||
| Throw and Catch | 1.32 ± 2.40 | −0.05 ± 0.40 | 0.77 ± 1.10 | 4.50 ± 1.66 ‡ | −0.48 ± 0.66 | 0.17 ± 0.61 | ||
| Kicks | 0.64 ± 2.35 | −0.04 ± 0.40 | −0.80 ± 1.10 | 4.75 ± 1.81 ‡ | −0.84 ± 0.66 | 1.71 ± 0.60 ‡ | ||
| Average Score | −10.24 ± 3.86 ‡ | −2.00 ± 0.58 ‡ | −5.91 ± 1.71 ‡ | 8.42 ± 2.71 ‡ | −4.20 ± 1.00 ‡ | 3.10 ± 0.72 ‡ | ||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Comeau, M.E.; Bouchard, D.R.; Levesque, C.; Jonhson, M.J.; Rioux, B.V.; Mayo, A.; Sénéchal, M. Association between Functional Movements Skills and Health Indicators in Children Aged between 9 and 12 Years Old. Int. J. Environ. Res. Public Health 2017, 14, 1010. https://doi.org/10.3390/ijerph14091010
Comeau ME, Bouchard DR, Levesque C, Jonhson MJ, Rioux BV, Mayo A, Sénéchal M. Association between Functional Movements Skills and Health Indicators in Children Aged between 9 and 12 Years Old. International Journal of Environmental Research and Public Health. 2017; 14(9):1010. https://doi.org/10.3390/ijerph14091010
Chicago/Turabian StyleComeau, Megan E., Danielle R. Bouchard, Cindy Levesque, Michel J. Jonhson, Brittany V. Rioux, Andrea Mayo, and Martin Sénéchal. 2017. "Association between Functional Movements Skills and Health Indicators in Children Aged between 9 and 12 Years Old" International Journal of Environmental Research and Public Health 14, no. 9: 1010. https://doi.org/10.3390/ijerph14091010