Study of the Relevance of the Quality of Care, Operating Efficiency and Inefficient Quality Competition of Senior Care Facilities

Abstract
:1. Introduction
1.1. Motivations
1.2. Literature Review
1.2.1. Inefficient Quality Competition
1.2.2. Data Envelopment Analyses (DEA)
1.2.3. Metafrontier Efficiency Analysis (MTE)
2. Materials and Methods
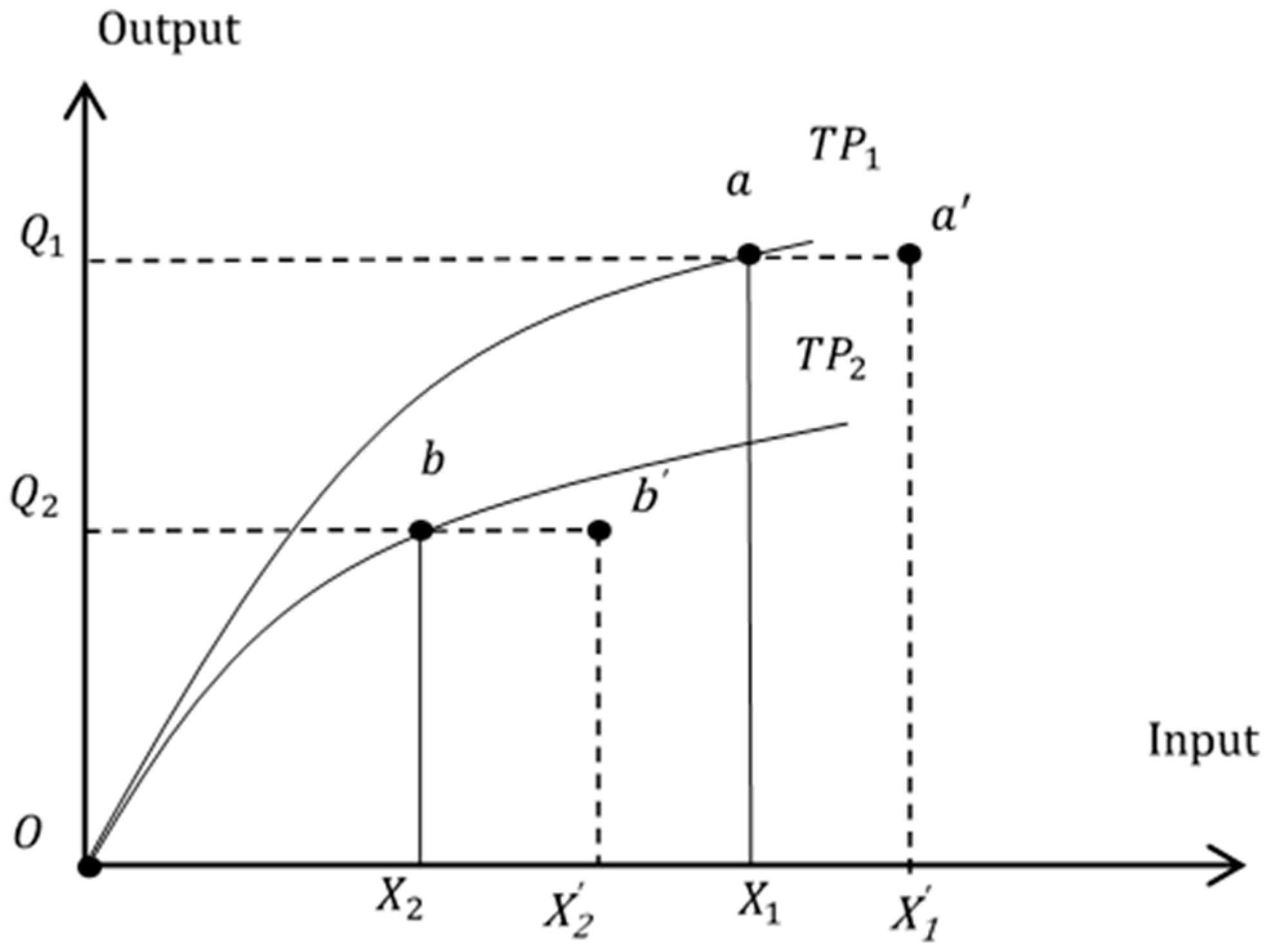
2.1. Technical Efficiency and Null Hypotheses
| H1: The input levels of general care facilities and nursing homes are the same |
| H2: The output levels of general care facilities and nursing homes are the same |
| H3: The productivity of general care facilities and nursing homes are the same |
| H4: The quality of care of general care facilities and nursing homes are the same |
| H5: The technical efficiency of general care facilities and nursing homes are the same |
| H6: Quality of care is positively related to technical efficiency |
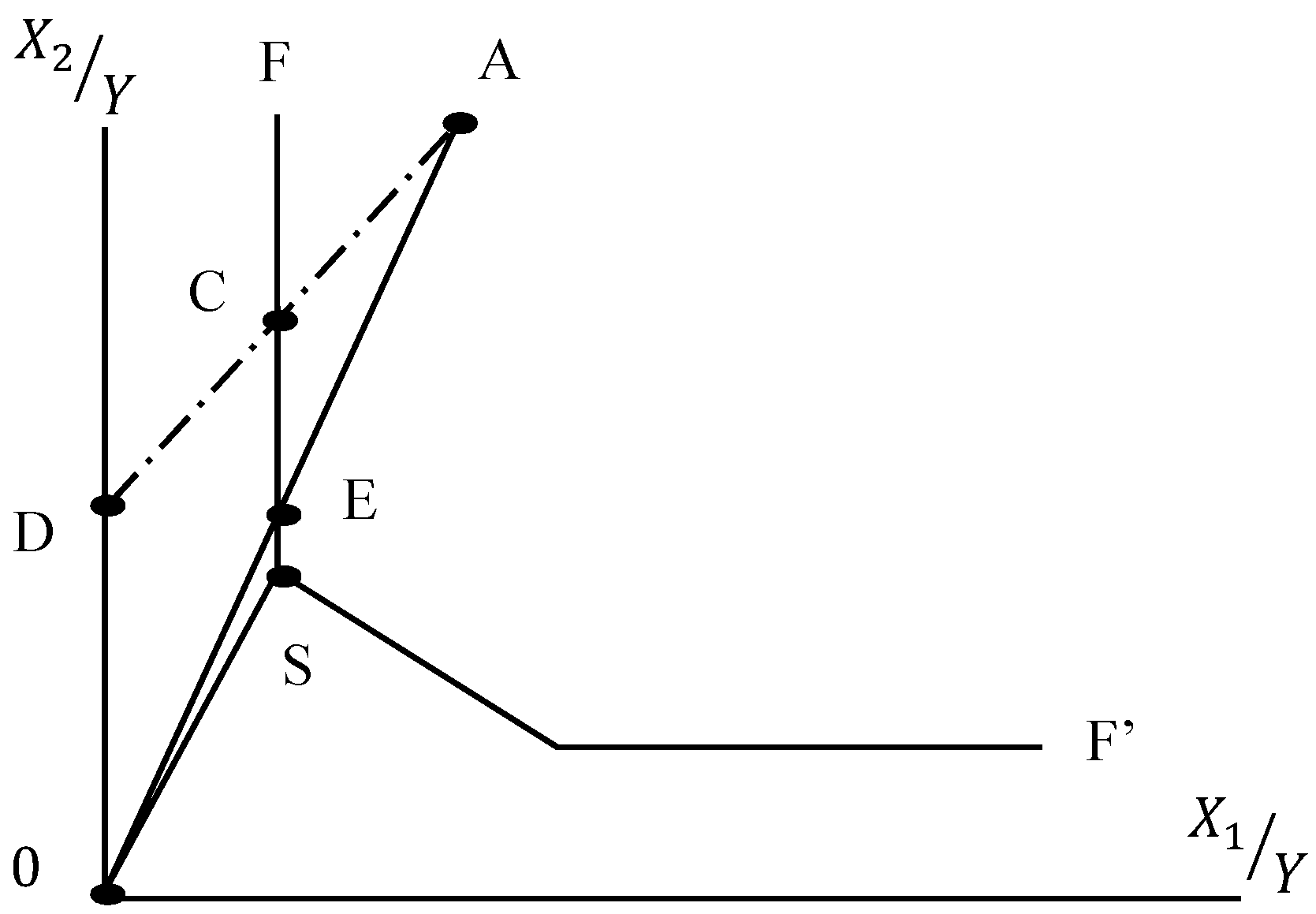
2.2. Data Envelopment Analysis (DEA)
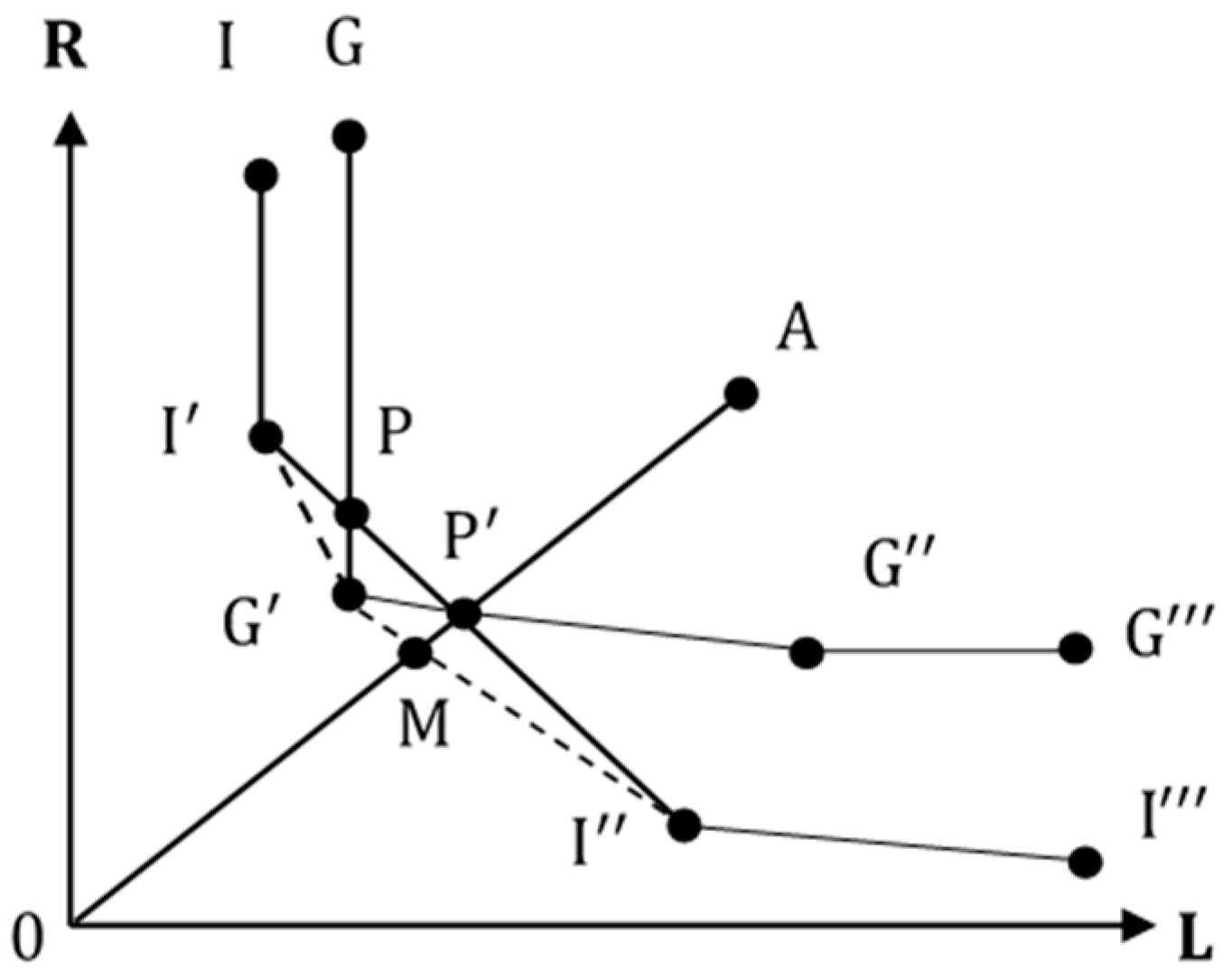
2.3. Metafrontier Efficiency Analysis (MTE)
- Calculate group technical efficiency ) for each facility by means of the EBM DEA model in Equation (5), where represents the technical efficiency of facility i in group j.
- Obtain the technical gap ratio (). is an estimate of the ratio of the efficiency of facility i to the overall efficiency of all facilities. Overall efficiency is obtained by inserting the target input and output values obtained from Step 1 of all groups into Equation (5).
- Calculate the metafrontier efficiency of each facility by combining results from step 1 and 2 by the following equation:
2.4. Iterative Seemingly Unrelated Regression
3. Empirical Results
3.1. Variable and Data Descriptions
3.2. Test of Hypotheses
3.3. Data Envelopment Analysis
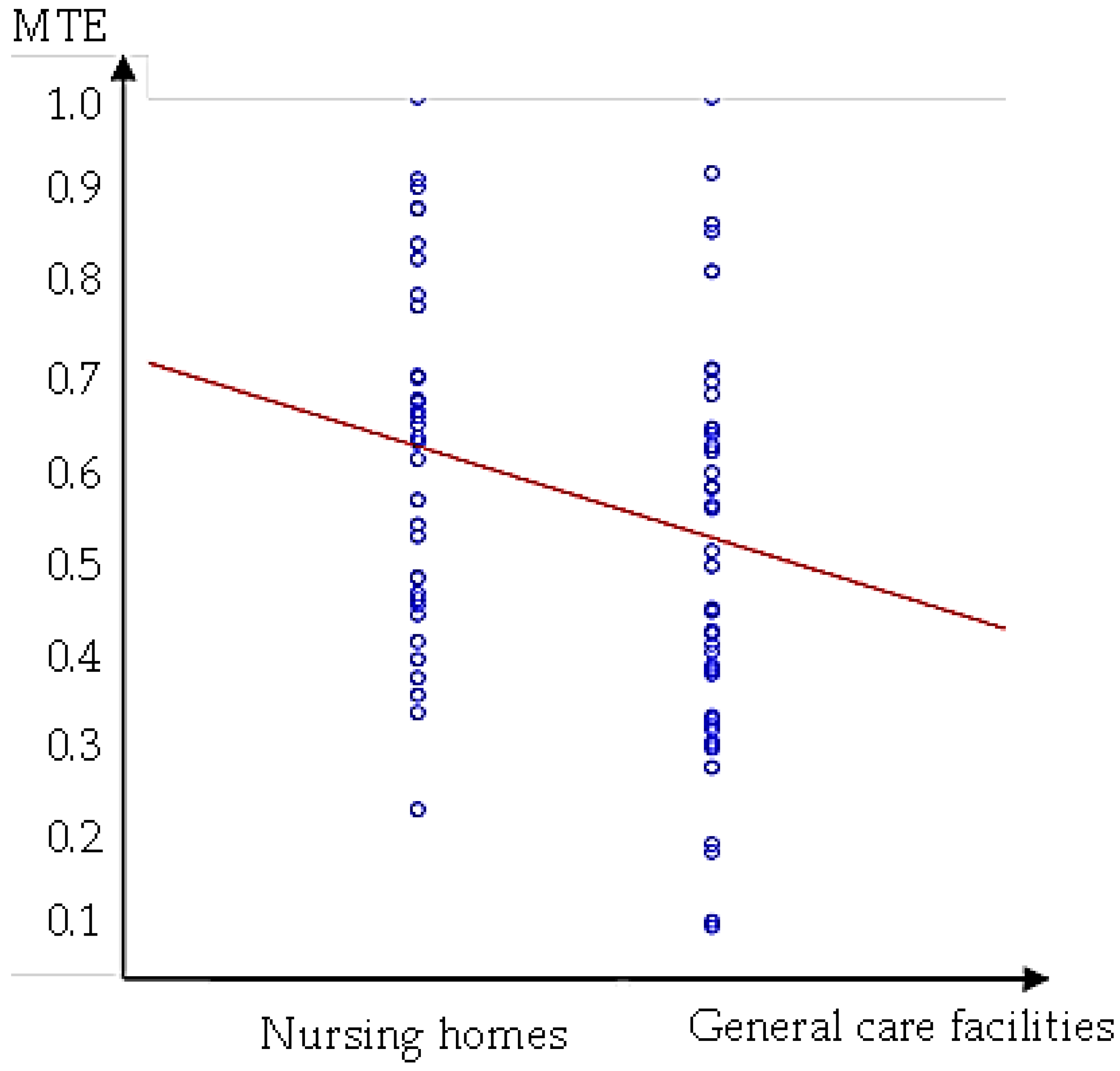
3.4. Metafrontier Efficiency Analysis
3.5. Regression Results
4. Conclusions
- The results of the EBM data envelopment analysis, which allows flexibility to adjust input and output ratios to fit various types of operations, proved to be different from the results of conventional data envelopment analysis. We showed that general care facilities and nursing homes have distinct efficiency frontiers. Therefore, it is necessary to conduct metafrontier efficiency analysis, which allows us to evaluate and compare the operating efficiency across different groups of senior facilities.
- The metafrontier efficiency results showed that there is, on average, room for improvement amounting to 45% for general care facilities and 36% for nursing homes to achieve complete metafrontier efficiency. The operating efficiency of general care facilities, with greater operating scales and better accreditation ratings on average, is inferior to that of nursing homes in Taiwan.
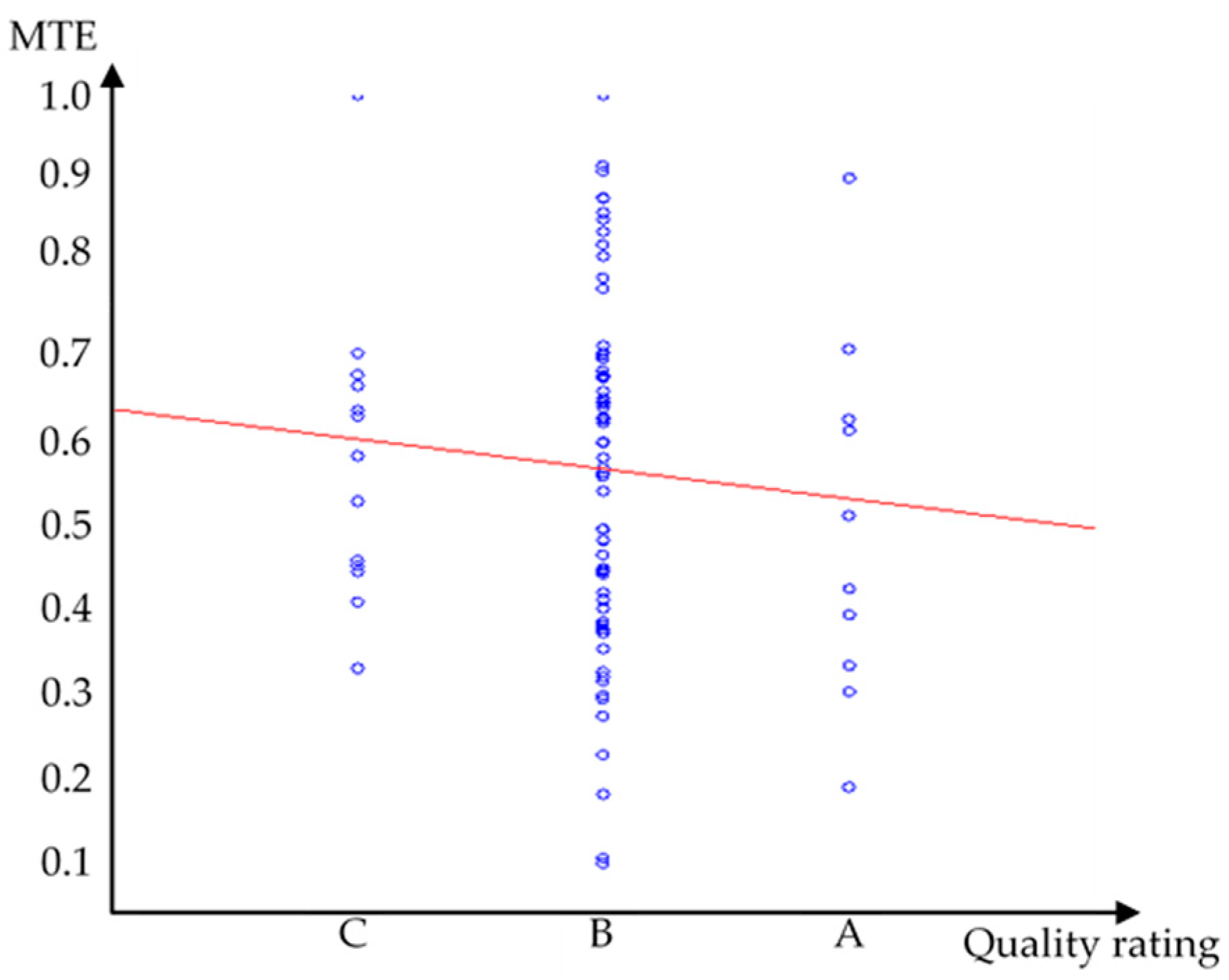
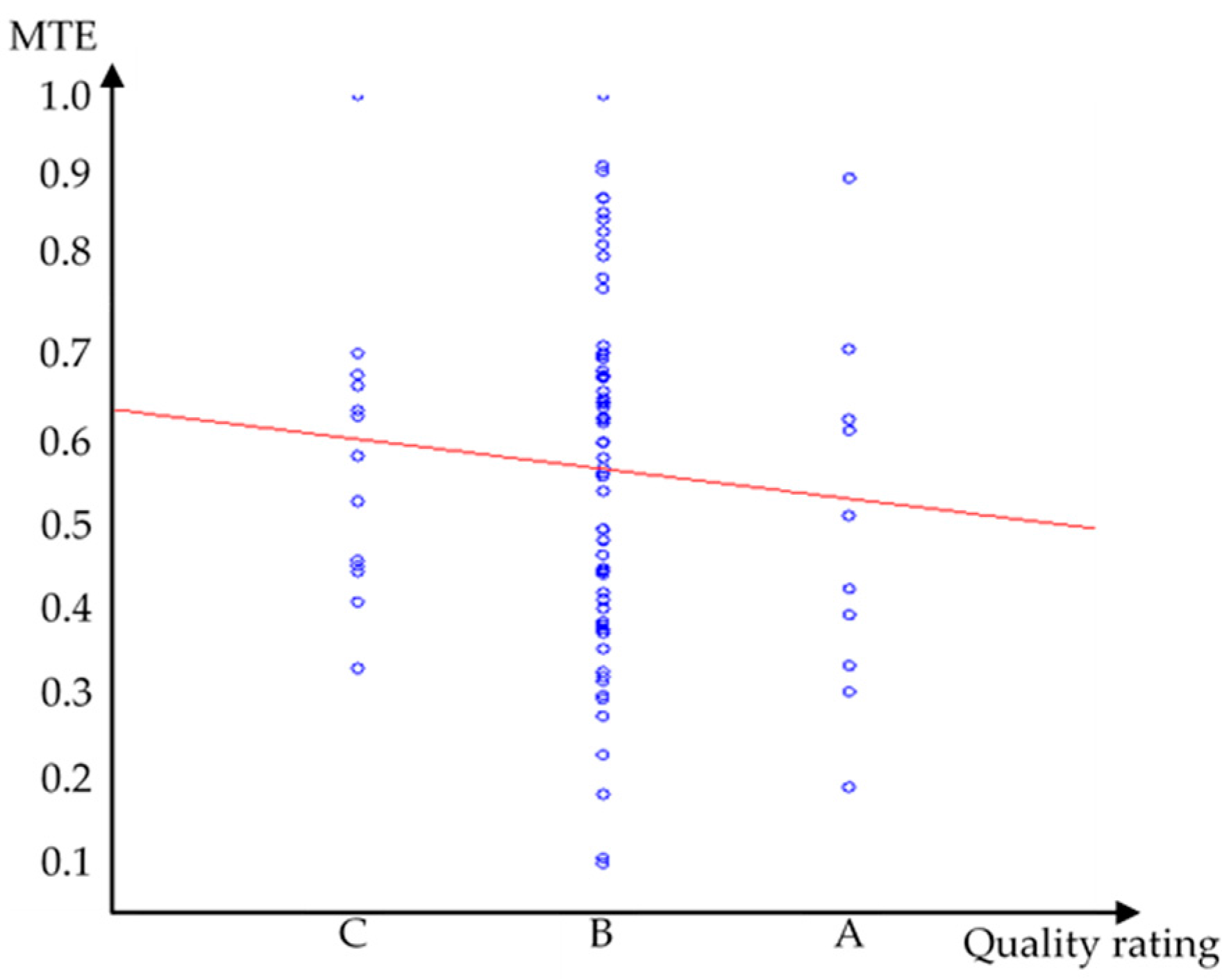
- The results of the regression model indicated that a tradeoff relationship exists between quality of care and metafrontier efficiency among general care facilities. General care facilities are observed to devote more input resources in order to obtain better ratings in the accreditation reports/quality of care; however, metafrontier efficiency is not improved but rather reduced. The inefficiency quality competition hypothesis is sustained for general care facilities. This observation corresponds to the inferior operating efficiency of general care facilities as noted in observation two. However, the same inference cannot be drawn for nursing homes. The small number of observations of nursing homes in the census data might be the reason that the relation between quality and efficiency in the empirical studies was not significant. The relatively small number of nursing homes in Taiwan might be due to two factors in our observations: the relatively small population of the country and the heavy reliance on home/resident care due to cultural concept of the youth bearing the responsibility for caring for the elderly in the family in Taiwan. Especially, the latter factor explains why nursing homes, which care for people who still have self-care ability, are not popular in the senior care system.
- The metafrontier efficiency results also showed that of all benchmark facilities (efficiency value = 1), of the eight facilities with a technical gap ratio = 1 and four facilities with metafrontier efficiency = 1, only one facility is publicly operated. This might be because privately-owned facilities have more financial incentives to achieve operating efficiency than public organizations.
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. Ageing and Health 2015. Available online: http://www.who.int/mediacentre/factsheets/fs404/en/ (accessed on 30 September 2015).
- Population Projections for R. O. C. (Taiwan). Nation Development Council. Available online: http://www.ndc.gov.tw/en/cp.aspx?n=2E5DCB04C64512CC (accessed on 24 August 2016).
- Belleflame, P.; Peitz, M. Asymmetric Information and Overinvestment in Quality. Eur. Econ. Rev. 2014, 66, 127–143. [Google Scholar] [CrossRef]
- Foote, S.B. Managing the Medical Arms Race: Innovation and Public Policy in the Medical Device Industry; University of California Press: London, UK, 1992; ISBN 9780520075917. [Google Scholar]
- James, P. Is the Medical Arms Race still Present in Today's Managed Care Environment? NYU Working Paper SSRN eLibrary; NYU Stern School of Business Research Paper Series: New York, NY, USA, 2002. [Google Scholar]
- White, M.J. The “Arms Race” on American Roads: The Effect of Sport Utility Vehicles and Pickup Trucks on Traffic Safety. J. Law Econ. 2004, 47, 333–355. [Google Scholar] [CrossRef]
- Gritsko, N.; Kozlova, V.; Neilson, W.; Wichmanni, B. The CEO Arms Race. South Econ. J. 2013, 79, 586–599. [Google Scholar] [CrossRef]
- Devers, K.J.; Brewster, H.R.; Casalino, L.P. Changes in Hospital Competitive Strategy: A New Medical Arms Race? Health Serv. Res. 2003, 38, 447–469. [Google Scholar] [CrossRef] [PubMed]
- Berenson, R.A.; Bodenheimer, T.; Pham, H.H. Specialty-Service Lines: Salvos in the New Medical Arms Race. Health Aff. 2006, 25, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Carey, K.; Stefos, T. Controlling for Quality in the Hospital Cost Function. Health Care Manag. Sci. 2011, 14, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Blank Jos, L.T.; Evelien, E. The Impact of Policy on Hospital Productivity: A Time Series Analysis of Dutch Hospitals. Health Care Manag. Sci. 2014, 17, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Trybou, J.; Gemmel, P.; Lieven, A. In the Eye of the Beholder: A Qualitative Study of Mutual Obligations and Areas of Ambiguity in the Hospital–physician Relationship. Int. J. Healthc. Manag. 2015, 8, 126–134. [Google Scholar] [CrossRef]
- Tsai, W.-D.; Li, I.-H. Hospital Nonprice Competition and Market Structure: An Empirical Study of Hospitals’ Acquisition of High-tech Medical Equipment. Acad. Econ. Pap. 2002, 30, 57–78. [Google Scholar]
- Sexton, T.R.; Leiken, A.M.; Sleeper, S.; Coburn, A.F. The Impact of Prospective Reimbursement on Nursing Home Efficiency. Med. Care 1989, 27, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Nyman, J.A.; Bricker, D.L.; Link, D. Technical Efficiency in Nursing Homes. Med. Care 1990, 28, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Fizel, J.L.; Nunnikhoven, T.S. Technical Efficiency of For-profit and Non-profit Nursing Homes. Manag. Decis. Econ. 1992, 13, 429–439. [Google Scholar] [CrossRef]
- Ozcan, Y.A.; Wogen, S.E.; Mau, L.W. Efficiency Evaluation of Skilled Nursing Facilities. J. Med. Syst. 1998, 22, 211–224. [Google Scholar] [CrossRef] [PubMed]
- Rosko, M.D.; Chilingerian, J.A.; Zinn, J.S.; Aaronson, W.E. The Effects of Ownership, Operating Environment, and Strategic Choices on Nursing Home Efficiency. Med. Care 1995, 33, 1001–1021. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-N. Operational Efficiency Analysis of Nursing Homes and Institutions in Taiwan: Data Envelopment Analysis. Taipei Econ. Inq. 2002, 38, 23–56. [Google Scholar]
- Yang, C.-C. The Analysis on Operating Efficiency of Nursing Homes—Application of Environmental Variable-Adjusted DEA. J. Health Sci. 2008, 10, 185–196. [Google Scholar]
- Chang, B.-G.; Huang, T.-H.; Wang, S.-H. Measuring the technical efficiency of H liner shipping company in Taiwan. J. Manag. Sci. 2010, 17, 743–764. [Google Scholar]
- Assaf, A.; Barros, C.P.; Josassen, A. Hotel Efficiency: A Bootstrapped Metafrontier Approach. Int. J. Hosp. Manag. 2010, 47, 468–475. [Google Scholar] [CrossRef]
- Battese, G.E.; Rao, D.S.P. Technology Gap, Efficiency, and a Stochastic Metafrontier Function. Int. J. Bus. Econ. 2002, 1, 87–93. [Google Scholar]
- Battese, G.E.; Rao, D.S.P.; O’Donnell, C.J. A Metafrontier Production Function for Estimation Efficiencies and Technology Gaps for Firms Operating under Different Technologies. J. Prod. Anal. 2004, 21, 91–103. [Google Scholar] [CrossRef]
- Rao, D.S.P. Conference Paper. Metafrontier Frameworks for the Study on Firm-level Efficiencies and Technology Gaps. In Proceedings of the Productivity and Efficiency Seminar, Taipei, Taiwan, 10 March 2006. [Google Scholar]
- Lin, C.H.; Chiu, Y.H.; Huang, C.W. Assessment of Technology Gaps of Tourist Hotels in Productive and Service Processes Using Meta-frontier DEA. Serv. Ind. J. 2012, 32, 2329–2342. [Google Scholar] [CrossRef]
- O’Donnell, C.; Rao, D.S.P.; Battese, G. Metafrontier Frameworks for the Study of Firm-level Efficiencies and Technology Ratios. Empir. Econ. 2008, 34, 231–255. [Google Scholar] [CrossRef]
- Huang, T.-H.; Chang, B.-G.; Chiu, Y.-F. An Examination of Banks’ Efficiency for Six Asian Countries under Metafrontier Cost Function. Acad. Econ. Pap. 2009, 37, 61–100. [Google Scholar]
- Yen, H.-P.; Chang, J.-W. Measuring Cost Efficiencies in Domestic Banks: Application of the Metafrontier Approach. Taipei Econ. Inq. 2011, 47, 147–181. [Google Scholar]
- Huang, C.J.; Huang, T.H.; Liu, N.H. A New Approach to Estimating the Metafrontier Production Function Based on a Stochastic Frontier Framework. J. Prod. Anal. 2014, 42, 241–254. [Google Scholar] [CrossRef]
- Charnes, A.; Cooper, W.W.; Rhodes, E. Measuring the Efficiency of Decision Making Units. Eur. J. Oper. Res. 1978, 2, 429–444. [Google Scholar] [CrossRef]
- Tone, K. A Slacks-based Measure of Efficiency in Data Envelopment Analysis. Eur. J. Oper. Res. 2001, 130, 498–509. [Google Scholar] [CrossRef]
- Tone, K.; Tsutsui, M. An Epsilon-based Measure of Efficiency in DEA—A Third Polo of Technical Efficiency. Eur. J. Oper. Res. 2010, 207, 1554–1563. [Google Scholar] [CrossRef]
- Cooper, W.W.; Seiford, L.M.; Tone, K. A Comprehensive Text with Models, Applications, References and DEA-Solver Software. In Data Envelopment Analysis; Kluwer Academic Publishers: Boston, MA, USA, 2000; ISBN 978-0-387-45283-8. [Google Scholar]
- Zellner, A. An Efficient Method of Estimating Seemingly Unrelated Regressions and Tests for Aggregation Bias. J. Am. Stat. Assoc. 1962, 57, 348–368. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Notation | Unit | Definition |
|---|---|---|---|
| Input variables | |||
| Direct nursing personnel | DSP | People | Nursing personnel, social workers, caregivers and other professionals related to the services provided |
| Indirect personnel | ISP | People | Administrative personnel include administrators, technicians, pharmacists, sanitary personnel, etc. |
| Floor area | FLO | Square meters | Floor area of the buildings |
| Output variables | |||
| Actual accommodation | APE | People | Actual accommodation at the time of accreditation report |
| Variables | Statistics | General Care Facilities | Nursing Homes | Total |
|---|---|---|---|---|
| DSP | Average | 42.596 | 28.949 | 36.747 |
| Maximum | 117.000 | 114.000 | 117.000 | |
| Minimum | 8.000 | 7.000 | 7.000 | |
| Standard deviation | 29.417 | 19.586 | 26.429 | |
| ISP | Average | 13.385 | 7.385 | 10.813 |
| Maximum | 67.000 | 26.000 | 67.000 | |
| Minimum | 2.000 | 1.000 | 1.000 | |
| Standard deviation | 11.264 | 5.413 | 9.653 | |
| FLO | Average | 2.228 | 0.487 | 1.482 |
| Maximum | 10.500 | 4.580 | 10.500 | |
| Minimum | 0.109 | 0.023 | 0.023 | |
| Standard deviation | 2.327 | 0.833 | 2.028 | |
| APE | Average | 152.712 | 78.333 | 120.835 |
| Maximum | 481.000 | 179.000 | 544.000 | |
| Minimum | 10.000 | 17.000 | 20.000 | |
| Standard deviation | 116.589 | 45.969 | 99.824 |
| General Care Facilities | Nursing Homes | t-Test | |
|---|---|---|---|
| Panel A: Means | |||
| DSP | 42.596 | 28.949 | (2.508 **) |
| ISP | 13.385 | 7.385 | (3.068 ***) |
| General care facilities | Nursing homes | t-Test | |
| FLO | 2.228 | 0.487 | (4.459 ***) |
| APE | 152.712 | 78.333 | (3.766 ***) |
| Panel B: Productivity | |||
| DSP/APE | 3.783 | 2.875 | (2.851 ***) |
| ISP/APE | 13.921 | 14.428 | (−0.205 ***) |
| FLO/APE | 141.481 | 392.589 | (−5.352 ***) |
| Ranking | A | B | C |
|---|---|---|---|
| General care facilities | 11.54% | 80.77% | 7.69% |
| Nursing homes | 10.26% | 66.67% | 23.08% |
| Total | 10.99% | 74.73% | 14.29% |
| General Care Facilities | |||
| APE | DSP | ISP | FLO |
| 0.838 | 0.608 | 0.387 | |
| (10.853 ***) | (5.422 ***) | (2.970 ***) | |
| Nursing Homes | |||
| APE | DSP | ISP | FLO |
| 0.659 | 0.362 | 0.436 | |
| (5.326 ***) | (2.360 **) | (2.943 ***) | |
| CCR | SBM | EBM | |
|---|---|---|---|
| General care facilities | |||
| Average | 0.636 | 0.559 | 0.621 |
| F-test | (1.431) | ||
| Medium | 0.656 | 0.546 | 0.641 |
| (2.923) | |||
| Nursing homes | |||
| Average | 0.684 | 0.502 | 0.644 |
| F-test | (8.860 ***) | ||
| Medium | 0.706 | 0.435 | 0.665 |
| (13.608 ***) | |||
| Total | |||
| Average | 0.656 | 0.535 | 0.631 |
| F-test | (7.303 ***) | ||
| Medium | 0.682 | 0.492 | 0.650 |
| (11.810 ***) | |||
| GTE | PTE | |
|---|---|---|
| Average | 0.631 | 0.559 |
| t test | (2.313 **) | |
| Medium | 0.650 | 0.534 |
| (2.659 **) | ||
| GTE | TGR | MTE | |
|---|---|---|---|
| General care facilities | |||
| Average | 0.621 | 0.898 | 0.548 |
| Medium | 0.641 | 0.925 | 0.527 |
| Maximum | 1.000 | 1.000 | 1.000 |
| Minimum | 0.159 | 0.659 | 0.150 |
| Nursing homes | |||
| Average | 0.645 | 0.997 | 0.642 |
| Medium | 0.665 | 1.000 | 0.665 |
| Maximum | 1.000 | 1.000 | 1.000 |
| Minimum | 0.270 | 0.886 | 0.270 |
| Total | |||
| Average | 0.631 | 0.941 | 0.589 |
| Medium | 0.650 | 1.000 | 0.598 |
| Maximum | 0.941 | 1.000 | 1.000 |
| Minimum | 0.159 | 0.659 | 0.150 |
| GTE = 1 | TGR = 1 | MTE = 1 | |
|---|---|---|---|
| General care facilities | 12% | 23% | 6% |
| Nursing homes | 8% | 95% | 5% |
| Technical Efficiency | General Care Facilities | Nursing Homes | |
|---|---|---|---|
| GTE | 0.641 | 0.665 | (0.599) |
| TGR | 0.925 | 1.000 | (5.971 ***) |
| MTE | 0.527 | 0.665 | (2.346 ***) |
| Equation | Log(DSP) | VIF1 | Log(ISP) | VIF2 | Log(FLO) | VIF3 | MTE | VIF4 | |
|---|---|---|---|---|---|---|---|---|---|
| Variable | |||||||||
| CQH general care facilities | 0.023 (0.093) | 2.479 | 0.315 (0.806) | 2.479 | 1.222 ** (2.408) | 2.479 | −0.109 ** (−2.011) | 2.639 | |
| CQM general care facilities | −0.031 (−0.330) | 1.565 | 0.115 (0.744) | 1.565 | 0.698 *** (3.477) | 1.565 | −0.061 *** (−2.768) | 1.774 | |
| CQH nursing homes | 0.348 * (1.664) | 2.958 | 0.298 (0.879) | 2.958 | 0.334 (0.761) | 2.958 | 0.084 * (1.810) | 3.076 | |
| CQM nursing homes | −0.029 (−0.229) | 2.038 | 0.289 (1.431) | 2.038 | 0.297 (1.131) | 2.038 | 0.039 (1.423) | 2.103 | |
| BED | 0.002 (0.768) | 1.109 | −0.003 (−0.839) | 1.109 | −0.033 *** (−7.721) | 1.109 | −0.0006 (−0.975) | 1.849 | |
| LOG (APE) | 0.685 *** (12.392) | 1.320 | 0.582 *** (6.500) | 1.320 | 1.096 *** (9.422) | 1.320 | 0.478 *** (20.153) | 5.077 | |
| LOG (DSP) | −0.306 *** (−12.992) | 3.803 | |||||||
| LOG (ISP) | −0.097 *** (−6.485) | 2.053 | |||||||
| LOG (FLO) | −0.082 *** (−7.272) | 3.850 | |||||||
| CONSTANT | 0.166 (0.637) | −0.649 (−1.537) | −3.567 *** (−6.509) | −0.329 *** (−4.774) | |||||
| RESET F-test (1,80) | 0.462 | 4.079 | 0.004 | 20.141 *** | |||||
| R2 | 0.722 | 0.456 | 0.721 | 0.847 | |||||
| Goodness of fit | LM = 9.314 | System R2 = 0.984 | |||||||
| Mediating Effect | Direct Effect | Total Effect | |
|---|---|---|---|
| CQH (general care facilities) | −0.301 *** (14.688) | −0.025 (0.268) | −0.325 ** (13.859) |
| CQM (general care facilities) | −0.103 ** (4.453) | −0.022 (0.568) | −0.125 ** (5.254) |
| CQH (nursing homes) | −0.163 ** (4.042) | 0.084 * (3.276) | −0.078 (0.718) |
| CQM (nursing homes) | −0.044 (0.819) | 0.039 (2.026) | −0.004 (0.006) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, J.-R.; Chen, C.-Y.; Peng, T.-K. Study of the Relevance of the Quality of Care, Operating Efficiency and Inefficient Quality Competition of Senior Care Facilities. Int. J. Environ. Res. Public Health 2017, 14, 1047. https://doi.org/10.3390/ijerph14091047
Lin J-R, Chen C-Y, Peng T-K. Study of the Relevance of the Quality of Care, Operating Efficiency and Inefficient Quality Competition of Senior Care Facilities. International Journal of Environmental Research and Public Health. 2017; 14(9):1047. https://doi.org/10.3390/ijerph14091047
Chicago/Turabian StyleLin, Jwu-Rong, Ching-Yu Chen, and Tso-Kwei Peng. 2017. "Study of the Relevance of the Quality of Care, Operating Efficiency and Inefficient Quality Competition of Senior Care Facilities" International Journal of Environmental Research and Public Health 14, no. 9: 1047. https://doi.org/10.3390/ijerph14091047