
Job Stress and Presenteeism among Chinese Healthcare Workers: The Mediating Effects of Affective Commitment

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Data Source
2.2. Variables and Instruments
2.3. Statistical Analysis
3. Results
3.1. Demographic Characteristics of Participants
3.2. Correlations between Presenteeism, Challenge Stress, Hindrance Stress, and Affective Commitment
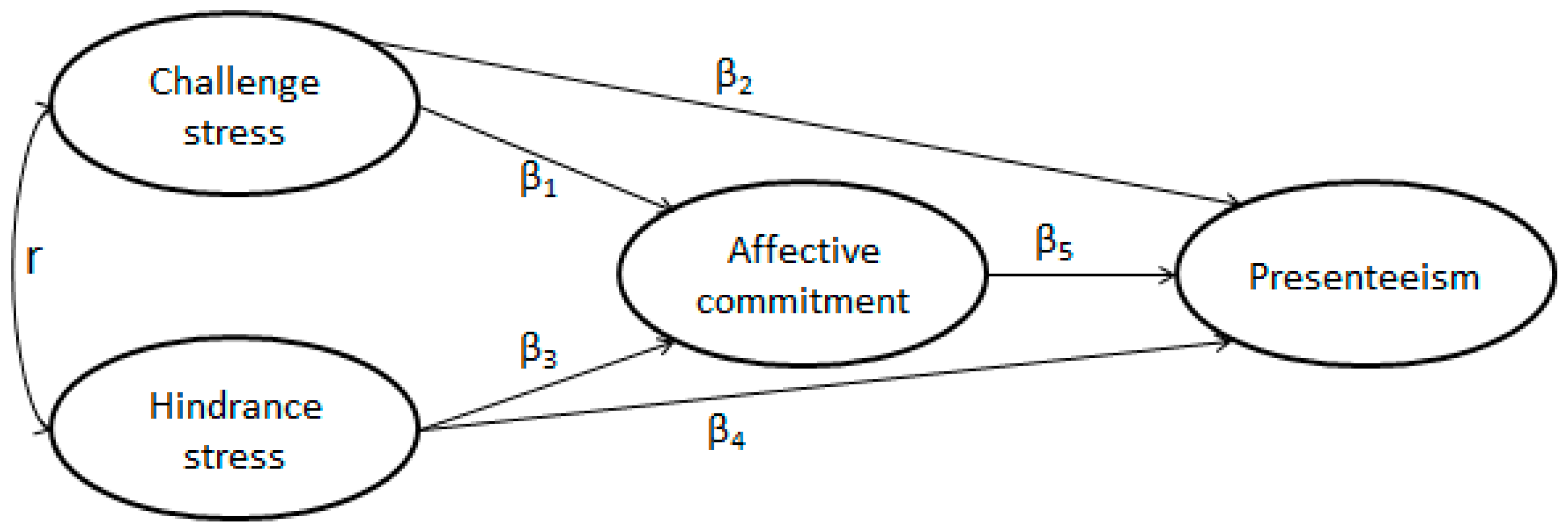
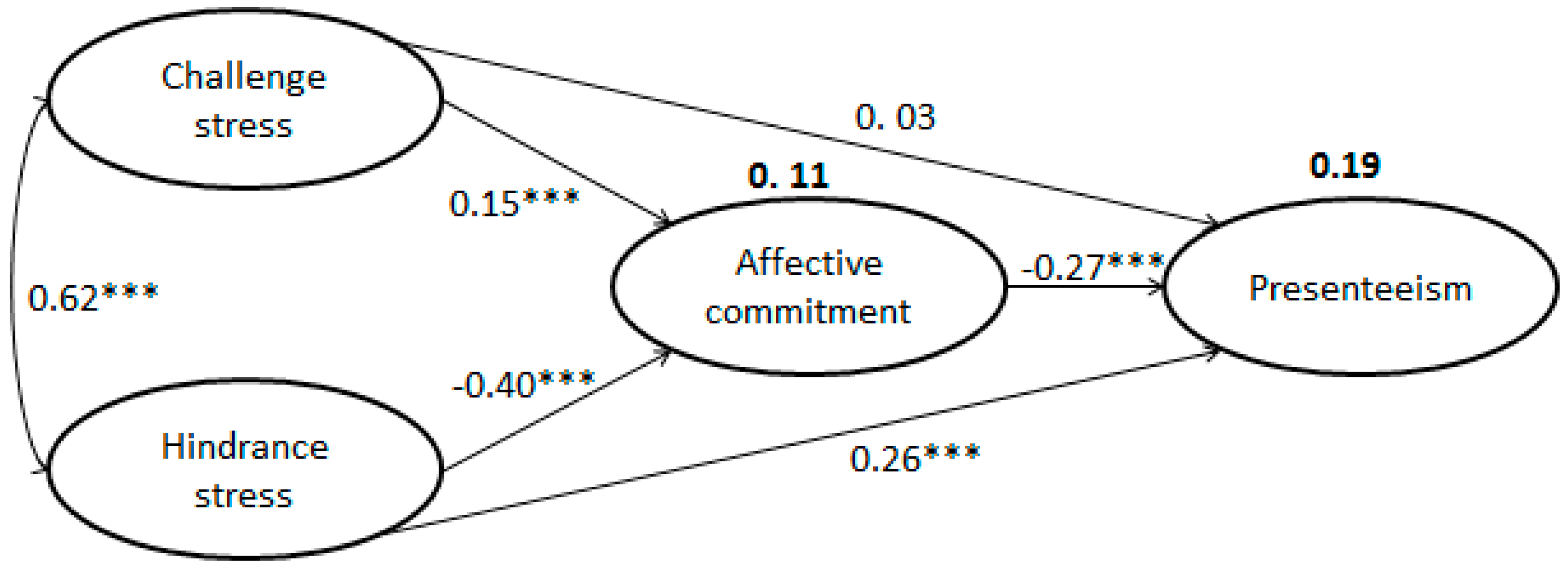
3.3. SEM
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Conflicts of Interest
Funding
References
- Johns, G. Presenteeism in the workplace: A review and research agenda. J. Organ. Behav. 2010, 31, 519–542. [Google Scholar] [CrossRef]
- Aronsson, G.; Gustafsson, K.; Dallner, M. Sick but yet at work. An empirical study of sickness presenteeism. J. Epidemiol. Community Health 2000, 54, 502–509. [Google Scholar] [CrossRef] [PubMed]
- Kivimäki, M.; Head, J.; Ferrie, J.E.; Hemingway, H.; Shipley, M.J.; Vahtera, J.; Marmot, M.G. Working while ill as a risk factor for serious coronary events: Whitehall II study. Am. J. Public Health 2011, 95, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Hemp, P. Presenteeism: At work—But out of it. Harv. Bus. Rev. 2004, 82, 49–58. [Google Scholar] [PubMed]
- Weaver, R. Cost of Presenteeism Surpasses Absenteeism. Available online: http://www.examiner.com/human-capitalin-detroit/cost-of-presenteeism-surpasses-absenteeism (accessed on 9 July 2017).
- Wan, H.C.; Downey, L.A.; Stough, C. Understanding non-work presenteeism: Relationships between emotional intelligence, boredom, procrastination and job stress. Pers. Individ Dif. 2014, 65, 86–90. [Google Scholar] [CrossRef]
- Whitehouse, D. Workplace presenteeism: How behavioral professionals can make a difference. Behav. Healthcare Tomorrow 2005, 14, 32–36. [Google Scholar]
- D’Abate, C.P.; Eddy, E.R. Engaging in personal business on the job: Extending the presenteeism construct. Hum. Resour. Dev. Q. 2007, 18, 361–383. [Google Scholar] [CrossRef]
- Collins, J.J.; Baase, C.M.; Sharda, C.E.; Ozminkowski, R.J.; Nicholson, S.; Billotti, G.M.; Turpin, R.S.; Olson, M.; Berger, M.L. The assessment of chronic health conditions on work performance, absence, and total economic impact for employers. J. Occup. Environ. Med. 2005, 47, 547–557. [Google Scholar] [CrossRef] [PubMed]
- Stewart, W.F.; Ricci, J.A.; Chee, E.; Morganstein, D. Lost productive work time costs from health conditions in the United States: Results from the American productivity audit. J. Occup. Environ. Med. 2003, 45, 1234–1246. [Google Scholar] [CrossRef] [PubMed]
- Pit, S.; Hansen, V. The relationship between lifestyle-, occupational health and work-related factors with presenteeism amongst general practitioners. Arch. Environ. Occup. Health 2016, 71, 49–56. [Google Scholar] [PubMed]
- Yang, T.; Zhu, M.; Xie, X. The determinants of presenteeism: A comprehensive investigation of stress-related factors at work, health, and individual factors among the aging workforce. J. Occup. Health 2015, 58, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Ilmarinen, J.; Rantanen, J. Promotion of work ability during ageing. Am. J. Ind. Med. 1999, 36, 21–23. [Google Scholar] [CrossRef]
- Yang, T.; Shen, Y.M.; Zhu, M.; Liu, Y.; Deng, J.; Chen, Q.; See, L.C. Effects of co-worker and supervisor support on job stress and presenteeism in an aging workforce: A structural equation modelling approach. Int. J. Environ. Res. Public Health 2016, 13, 72. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.; Fisher, G.; Ryan, L.; Clarke, P.; House, J.; Weir, D. Psychosocial and Lifestyle Uestionnaire 2006–2010 Documentation Report Core Section LB; The HRS Psychosocial Working Group: Ann Arbor, MI, USA, 2013. [Google Scholar]
- Hummer, J.; Sherman, B.; Quinn, N. Present and unaccounted for. Occup. Health Saf. 2002, 71, 40–42. [Google Scholar] [PubMed]
- Turpin, R.S.; Ozminkowski, R.J.; Sharda, C.E.; Collins, J.J.; Berger, M.L.; Billotti, G.M.; Baase, C.M.; Olson, M.J.; Nicholson, S. Reliability and validity of the stanford presenteeism scale. J. Occup. Environ. Med. 2004, 46, 1123–1133. [Google Scholar] [CrossRef] [PubMed]
- Macgregor, J.N.; Cunningham, J.B.; Caverley, N. Factors in absenteeism and presenteeism: Life events and health events. Manag. Res. News 2008, 31, 607–615. [Google Scholar] [CrossRef]
- Vänni, K.; Virtanen, P.; Luukkaala, T.; Nygård, C.H. Relationship between perceived work ability and productivity loss. Int. J. Occup. Saf. Ergonom. 2012, 18, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Elstad, J.I.; Vabø, M. Job stress, sickness absence and sickness presenteeism in nordic elderly care. Scand. J. Public Health 2008, 36, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Huff, J.; Ablah, E. Stress and presenteeism among Kansas hospital employees: What stress reduction interventions might hospitals benefit from offering to employees? J. Occup. Environ. Med. 2016, 58, e368–e369. [Google Scholar] [CrossRef] [PubMed]
- Cavanaugh, M.A.; Boswell, W.R.; Roehling, M.V.; Boudreau, J.W. An empirical examination of self-reported work stress among U.S. Managers. J. Appl. Psychol. 2000, 85, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Boswell, W.R.; Olson-Buchanan, J.B.; Lepine, M.A. Relations between stress and work outcomes: The role of felt challenge, job control, and psychological strain. J. Vocat. Behav. 2004, 64, 165–181. [Google Scholar] [CrossRef]
- Wallace, J.C.; Edwards, B.D.; Arnold, T.; Frazier, M.L.; Finch, D.M. Work stressors, role-based performance, and the moderating influence of organizational support. J. Appl. Psychol. 2009, 94, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Lepine, J.A.; Podsakoff, N.P.; Lepine, M.A. A meta-analytic test of the challenge stressor-hindrance stressor framework: An explanation for inconsistent relationships among stressors and performance. Acad. Manag. J. 2005, 48, 764–775. [Google Scholar] [CrossRef]
- Podsakoff, N.P.; Lepine, J.A.; Lepine, M.A. Differential challenge stressor-hindrance stressor relationships with job attitudes, turnover intentions, turnover, and withdrawal behavior: A meta-analysis. J. Appl. Psychol. 2007, 92, 438–454. [Google Scholar] [CrossRef] [PubMed]
- Jourdain, G.; Vézina, M. How psychological stress in the workplace influences presenteeism propensity: A test of the demand–control–support model. Eur. J. Work Organ. Psycol. 2014, 23, 483–496. [Google Scholar] [CrossRef]
- Hansen, C.D.; Andersen, J.H. Going ill to work—What personal circumstances, attitudes and work-related factors are associated with sickness presenteeism? Soc. Sci. Med. 2008, 67, 956–964. [Google Scholar] [CrossRef] [PubMed]
- Cicei, C.C.; Mohorea, L.; Teodoru, A.A. Investigating two predictors of sickness presenteeism on a romanian sample. The case of performance-based self-esteem and overcommitment. Procedia Soc. Behav. Sci. 2013, 78, 325–329. [Google Scholar] [CrossRef]
- Bierla, I.; Huver, B.; Richard, S. New evidence on absenteeism and presenteeism. Int. J. Hum. Resour. Manag. 2013, 24, 1536–1550. [Google Scholar] [CrossRef]
- Mowday, R.T. Reflections on the study and relevance of organizational commitment. Hum. Resour. Manag. Rev. 1998, 8, 387–401. [Google Scholar] [CrossRef]
- Yeh, Y.J.Y.; Ko, J.J.R.; Chang, Y.S.; Chen, C.H.V. Job stress and work attitudes between temporary and permanently employed nurses. Stress Health 2007, 23, 111–120. [Google Scholar] [CrossRef]
- Lu, L.; Siu, O.L.; Lu, C.Q. Does loyalty protect Chinese workers from stress? The role of affective organizational commitment in the greater china region. Stress Health 2010, 26, 161–168. [Google Scholar] [CrossRef]
- Irving, P.G.; Coleman, D.F. The moderating effect of different forms of commitment on role ambiguity-job tension relations. Can. J. Adm. Sci. 2003, 20, 97–106. [Google Scholar] [CrossRef]
- Haar, J.M. Challenge and hindrance stressors in New Zealand: Exploring social exchange theory outcomes. Int. J. Hum. Resour. Manag. 2006, 17, 1942–1950. [Google Scholar] [CrossRef]
- Oxtoby, K. Why doctors need to resist “presenteeism”. BMJ 2015, 351, h6720. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, S.M.; Løvseth, L.T.; Schenckgustafsson, K.; Fridner, A. What makes physicians go to work while sick: A comparative study of sickness presenteeism in four European countries (HOUPE). Swiss Med. Wkly. 2013, 143, w13840. [Google Scholar] [CrossRef] [PubMed]
- Adeolu, J.O.; Yussuf, O.B.; Popoola, O.A. Prevalence and correlates of job stress among junior doctors in the university college hospital, Ibadan. Ann. Ib. Postgrad. Med. 2016, 14, 92–98. [Google Scholar] [PubMed]
- Letvak, S.A.; Ruhm, C.J.; Gupta, S.N. Nurses’ presenteeism and its effects on self-reported quality of care and costs. Am. J. Nurs. 2012, 112, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Lancet, T. Ending violence against doctors in China. Lancet 2012, 379, 1764. [Google Scholar] [CrossRef]
- NHFP Commission. China Health and Family Planning Statistical Digest; Peking Union Medical College Press: Beijing, China, 2015.
- Mowday, R.T.; Steers, R.M.; Porter, L.W. The measurement of organizational commitment. J. Vocat. Behav. 1979, 14, 224–247. [Google Scholar] [CrossRef]
- Yang, T.; Hou, F.; Guo, Y.; Ma, M.; Ye, T.; Deng, J. Studying of the Relationship among Challenge Stress, Hindrance Work Stress and Job Burnout in Medical Staffs of Private Hospitals. Chin. Health Serv. Manag. 2017, 34, 384–387. [Google Scholar]
- Bollen, K.A.; Long, J.S. Testing Structural Equation Models; Sage: Thousand Oaks, CA, USA, 1993. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Fit indices in covariance structure modeling: Sensitivity to models. Sociol. Methodol. 1998, 13, 290–312. [Google Scholar]
- Hayes, A.F. Beyond baron and kenny: Statistical mediation analysis in the new millennium. Commun. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Mackinnon, D.P.; Lockwood, C.M.; Hoffman, J.M.; West, S.G.; Sheets, V. A comparison of methods to test mediation and other intervening variable effects. Psychol. Methods 2002, 7, 83. [Google Scholar] [CrossRef] [PubMed]
- Sobel, M.E. Asymptotic confidence intervals for indirect effects in structural equation models. Sociol. Methodol. 1982, 13, 290–312. [Google Scholar] [CrossRef]
- Vandenberg, R.; Lance, C. A review and synthesis of the measurement invariance literature: Suggestions, practices, and recommendations for organizational research. Organ. Res. Methods 2000, 3, 4–69. [Google Scholar] [CrossRef]
- Cheung, G.W.; Rensvold, R.B. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct. Equ. Model. 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Kyriacou, C.; Sutcliffe, J. Teacher stress: Prevalence, sources, and symptoms. Br. J. Educ. Psychol. 1978, 48, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Liu, Y.; Chen, Q.; Zhu, M.; Deng, J. Challenge or hindrance: Job stress leads to reduction of presenteeism in Chinese context, really? In Proceedings of the 2017 Annual Meeting of Academy of Management, Atlanta, GA, USA, 4–8 August 2017. [Google Scholar]
- Lin, L.; Siu, O.L.; Shi, K.; Bai, X.W. Challenge and hindrance job demands, job resource, and their relationships with vigor and emotional exhaustion. In Proceedings of the International Conference on Management Science and Engineering, Moscow, Russia, 14–16 September 2009. [Google Scholar]
- Homans, G.C. Social behavior as exchange. Am. J. Sociol. 1958, 63, 597–606. [Google Scholar] [CrossRef]
- Gun, M.S.; Choi, Y.H.; Park, K.H. Job stress and presenteeism of clinical nurses. Korean J. Occup. Health Nurs. 2011, 20, 163–171. [Google Scholar] [CrossRef]
- Boles, M.; Pelletier, B.; Lynch, W. The relationship between health risks and work productivity. J. Occup. Environ. Med. 2004, 46, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Ryu, I.S.; Jeong, D.S.; Kim, I.A.; Roh, J.H.; Won, J.U. Association between job stress, psychosocial well-being and presenteeism, absenteeism: Focusing on railroad workers. Korean J. Occup. Environ. Med. 2012, 24, 263–273. [Google Scholar]
- Zheng, X. Stress status and countermeasures of healthcare workers. Chin. J. Public Health 2012, 28, 35–36. [Google Scholar]
- Cheng, H. Occupation Burnout and Its Influence Factors of Clinical Doctors in West Area of China; Nanjing Medical University: Nanjing, China, 2012. [Google Scholar]
- Li, Y.; Lv, H.; Liu, Y. Research advance on job burnout of medical staff. Modern Prev. Med. 2015, 42, 3489–3492. [Google Scholar]
- Yang, T.; Deng, J.; Liu, Y.; Chen, Q.; Chen, Z.; Shen, Y.M. What makes medical staffs from public hospitals to Private hospitals? Work. In Proceedings of the Age, Health and Employment—Evidence from Longitudinal Studies, Wuppertal, Germany, 19–21 September 2016. [Google Scholar]
- Lewis, S.; Cooper, C.L. Balancing the work and family interface: A European perspective. Hum. Resour. Manag. Rev. 1996, 5, 289–305. [Google Scholar] [CrossRef]
- Lancet, T. Violence against doctors: Why china? Why now? What next? Lancet 2014, 383, 1013. [Google Scholar] [CrossRef]
- Listed, N. Chinese doctors are under threat. Lancet 2010, 376, 657. [Google Scholar]
- Huang, Y.; Chen, J.; Lin, P.; Lin, Z.; Jiang, Y. Female doctor’s work stressors and relationship with their metal health. J. Chin. Prev. Med. 2012, 13, 55–58. [Google Scholar]
- Taifor, N.A.; Abdullah, H.S.; Hashim, R. In Incidence and antecedents of presenteeism: The case of a federal government ministry in Malaysia. In Proceedings of the 2011 IEEE Colloquium on Humanities, Science and Engineering, Penang, Malaysia, 5–6 December 2011; pp. 654–659. [Google Scholar]
- Chen, Z.X.; Francesco, A.M. The relationship between the three components of commitment and employee performance in China. J. Vocat. Behav. 2003, 62, 490–510. [Google Scholar] [CrossRef]
- Shen, S.W.; Yuan, Y. The contemporary value and defects of Chinese traditional culture. Sci. Econom. Soc. 2012, 4, 36. [Google Scholar]
- Huang, Q.; Zhang, X.; Tang, Z. Analysis of orientation and training ways of general practitioners. Northwest. Med. Edu. 2016, 24, 743–745. [Google Scholar]
- Wang, Z. On doctors’ responsibilities. Chin. Med. Eth. 2009, 22, 3–4. [Google Scholar]
- Podsakoff, P.M.; MacKenzie, S.B.; Podsakoff, N.P. Sources of method bias in social science research and recommendations on how to control it. Annu. Rev. Psychol. 2012, 63, 539–569. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variables | Items | Mead | SD |
|---|---|---|---|
| Presenteeism (0–10) | P1. How many points would you give your current ability to work? | 2.37 | 1.57 |
| P2. Thinking about the physical demands of your job, how do you rate your current ability to meet those demands? | 2.56 | 1.65 | |
| P3. Thinking about the mental demands of your job, how do you rate your current ability to meet those demands? | 2.75 | 1.79 | |
| P4. Thinking about the interpersonal demands of your job, how do you rate your current ability to meet those demands? | 2.66 | 1.73 | |
| Challenge stress (1–5) | CS1. The number of projects and or assignments I have. | 3.48 | 0.87 |
| CS2. The amount of time I spend at work. | 3.50 | 0.85 | |
| CS3. The volume of work that must be accomplished in the allotted time. | 3.36 | 0.88 | |
| CS4. Time pressures I experience. | 3.45 | 0.88 | |
| CS5. The amount of responsibility I have. | 3.56 | 0.87 | |
| CS6. The scope of responsibility my position entails. | 3.49 | 0.89 | |
| Hindrance stress (1–5) | HS1. The degree to which politics rather than performance affects organizational decisions. | 2.85 | 1.04 |
| HS2. The inability to clearly understand what is expected of me on the job. | 2.38 | 1.05 | |
| HS3. The amount of red tape I need to go through to get my job done. | 3.01 | 1.00 | |
| HS4. The lack of job security I have. | 2.98 | 1.08 | |
| HS5. The degree to which my career seems stalled. | 3.04 | 1.05 | |
| Affective commitment (1–7) | AC1. I am willing to put in a great deal of effort beyond that normally expected in order to help this organization be successful. | 4.63 | 1.49 |
| AC2. I talk up this organization to my friends as a great organization to work for. | 4.81 | 1.49 | |
| AC3. I feel very little loyalty to this organization. (R) | 5.14 | 1.60 | |
| AC4. I would accept almost any type of job assignment in order to keep working for this organization. | 4.17 | 1.61 | |
| AC5. I find that my values and the organization’s values are very similar. | 4.41 | 1.56 | |
| AC6. I am proud to tell others that I am part of this organization. | 4.91 | 1.69 | |
| AC7. I could just as well be working for a different organization as long as the type of work was similar. (R) | 4.22 | 1.54 | |
| AC8. This organization really inspires the very best in me in the way of job performance. | 4.34 | 1.65 | |
| AC9. It would take very little change in my present circumstances to cause me to leave this organization. (R) | 5.19 | 1.46 | |
| AC10. I am extremely glad that I chose this organization to work for over others I was considering at the time I joined. | 5.05 | 1.49 | |
| AC11. There’s not too much to be gained by sticking with this organization indefinitely. (R) | 4.40 | 1.70 | |
| AC12. Often, I find it difficult to agree with this organization’s policies on important matters relating to its employees. (R) | 4.11 | 1.68 | |
| AC13. I really care about the fate of this organization. | 5.41 | 1.41 | |
| AC14. For me, this is the best of all possible organizations for which to work. | 4.90 | 1.50 | |
| AC15. Deciding to work for this organization was a definite mistake on my part. (R) | 4.97 | 1.85 |
| Characteristics | Sample (n = 1392) | Percent (%) |
|---|---|---|
| Sex | ||
| Male | 297 | 21.3% |
| Female | 1037 | 74.5% |
| Age (years) | ||
| ~25 | 189 | 13.6% |
| 25~30 | 538 | 38.6% |
| 31~35 | 302 | 21.7% |
| 36~40 | 128 | 9.2% |
| 41~50 | 138 | 9.9% |
| 51~55 | 40 | 2.9% |
| 56~60 | 8 | 0.6% |
| 60~ | 3 | 0.2% |
| Post | ||
| Clinician | 425 | 30.5% |
| Nurse | 589 | 42.3% |
| Management | 119 | 8.5% |
| medical technicians | 158 | 11.4% |
| Pharmacist | 25 | 1.8% |
| Education | ||
| Under degree | 53 | 3.8% |
| Junior college | 295 | 21.2% |
| Undergraduate | 577 | 41.5% |
| Master | 299 | 21.5% |
| Doctor | 110 | 7.9% |
| Title | ||
| Trainee | 67 | 4.8% |
| Primary | 739 | 53.1% |
| Middle | 384 | 27.6% |
| Senior | 120 | 8.6% |
| Seniority (years) | ||
| ~3 | 341 | 24.5% |
| 3~5 | 355 | 25.5% |
| 6~10 | 307 | 22.1% |
| 11~20 | 193 | 13.9% |
| 20~ | 140 | 10.1% |
| Department | ||
| Physician | 229 | 16.5% |
| Surgeon | 226 | 16.2% |
| Obstetrics/gynecology | 132 | 9.5% |
| Pediatrics | 260 | 18.7% |
| Chinese Medicine | 102 | 7.3% |
| Oncology | 12 | 0.9% |
| Other clinical departments | 84 | 6.0% |
| Medical technology | 181 | 13.0% |
| Administration and Logistics | 90 | 6.5% |
| Variables (Mean (M), SD) | Items | |||
|---|---|---|---|---|
| P | CS | HS | AC | |
| P (2.59, 1.5) | 1 | |||
| CS (3.47, 0.75) | 0.20 ** | 1 | ||
| HS (2.85, 0.81) | 0.32 ** | 0.53 ** | 1 | |
| AC (4.70, 0.93) | −0. 33 ** | −0.09 ** | −0.28 ** | 1 |
| Path | Young (under 30 Years, n = 727) | Old (over 31 Years, n = 619) | Early Career (n = 806) | Mid/Late Career (n = 504) | ||||
|---|---|---|---|---|---|---|---|---|
| β | p Value | β | p Value | β | p Value | β | p Value | |
| CS to AC | 0.13 | ** | 0.17 | * | 0.15 | ** | 0.13 | * |
| HS to AC | −0.40 | *** | −0.41 | *** | −0.44 | *** | −0.38 | *** |
| AC to P | −0.22 | *** | −0.31 | *** | −0.24 | *** | −0.34 | *** |
| CS to P | −0.04 | 0.44 | 0.10 | 0.08 | −0.03 | 0.47 | 0.12 | 0.06 |
| HS to P | 0.31 | *** | 0.21 | *** | 0.29 | *** | 0.20 | ** |
| CS to HS | 0.59 | *** | 0.66 | *** | 0.60 | *** | 0.65 | *** |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, T.; Guo, Y.; Ma, M.; Li, Y.; Tian, H.; Deng, J. Job Stress and Presenteeism among Chinese Healthcare Workers: The Mediating Effects of Affective Commitment. Int. J. Environ. Res. Public Health 2017, 14, 978. https://doi.org/10.3390/ijerph14090978
Yang T, Guo Y, Ma M, Li Y, Tian H, Deng J. Job Stress and Presenteeism among Chinese Healthcare Workers: The Mediating Effects of Affective Commitment. International Journal of Environmental Research and Public Health. 2017; 14(9):978. https://doi.org/10.3390/ijerph14090978
Chicago/Turabian StyleYang, Tianan, Yina Guo, Mingxu Ma, Yaxin Li, Huilin Tian, and Jianwei Deng. 2017. "Job Stress and Presenteeism among Chinese Healthcare Workers: The Mediating Effects of Affective Commitment" International Journal of Environmental Research and Public Health 14, no. 9: 978. https://doi.org/10.3390/ijerph14090978