Differences between Dual Users and Switchers Center around Vaping Behavior and Its Experiences Rather than Beliefs and Attitudes


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Procedure
2.4. Statistical Analyses
3. Results
3.1. Demographics
3.2. Smoking Behavior
3.3. E-cig use
3.4. Behavioral, Cognitive and Attitudinal Aspects
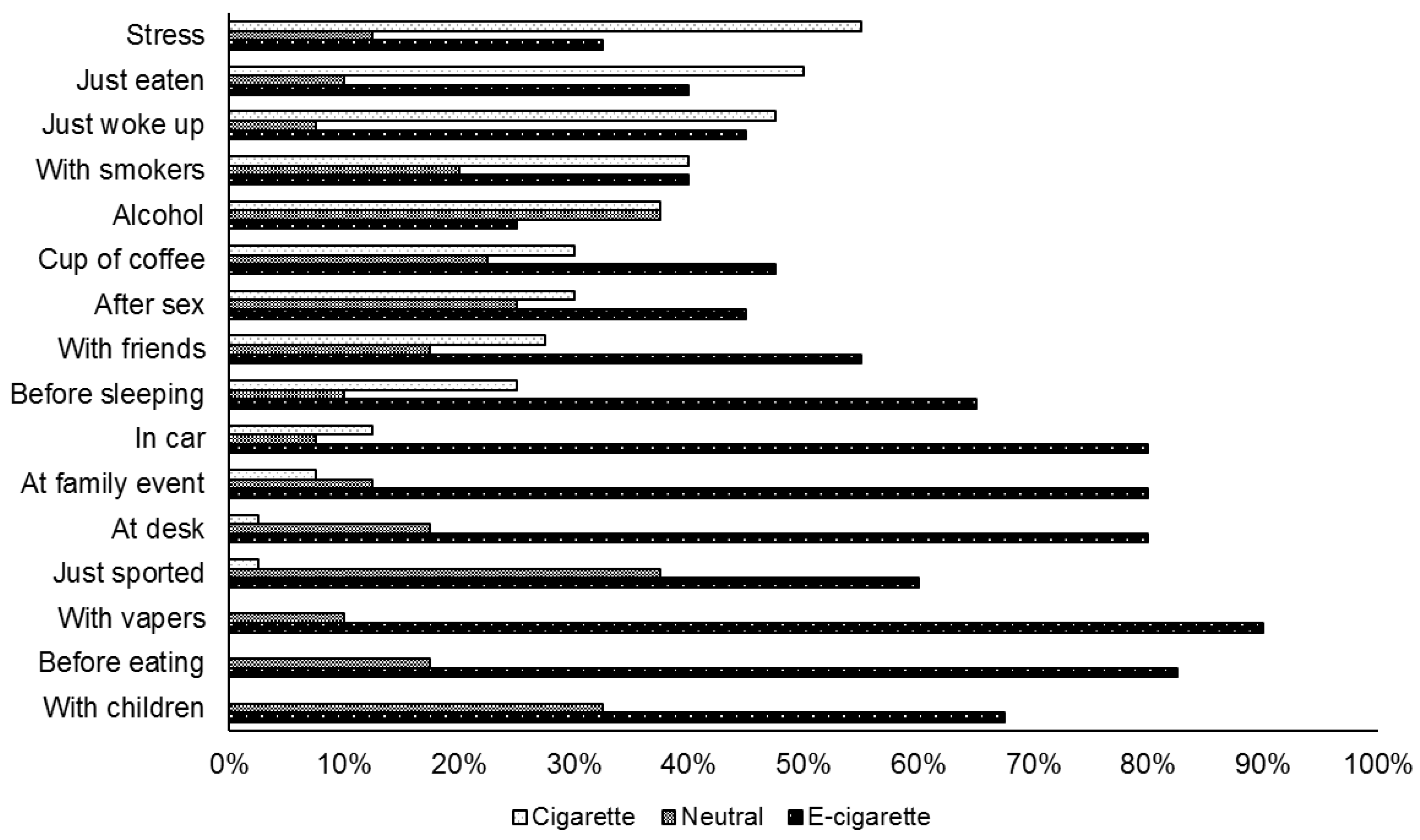
3.5. Situations
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Special Eurobarometer 458: Attitudes of Europeans towards Tobacco and Electronic Cigarettes. Available online: http://ec.europa.eu/commfrontoffice/publicopinion/index.cfm/Survey/getSurveyDetail/instruments/SPECIAL/surveyKy/2146 (accessed on 6 June 2017).
- Jamal, A.; Homa, D.M.; O’Connor, E.; Babb, S.D.; Caraballo, R.S.; Singh, T.; Sean Hu, S.; King, B.A. Current cigarette smoking among adults—United States, 2005–2014. MMWR Morb. Mortal. Wkly. Rep. 2015, 64, 1233–1240. [Google Scholar] [CrossRef] [PubMed]
- Inoue-Choi, M.; Liao, L.M.; Reyes-Guzman, C.; Hartge, P.; Caporaso, N.; Freedman, N.D. Association of long-term, low-intensity smoking with all-cause and cause-specific mortality in the National Institutes of health-AARP diet and health study. JAMA Intern. Med. 2016, 177, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Pirie, K.; Peto, R.; Reeves, G.K.; Green, J.; Beral, V. The 21st century hazards of smoking and benefits of stopping: A prospective study of one million women in the UK. Lancet 2013, 381, 133–141. [Google Scholar] [CrossRef]
- ASH. Factsheet: Use of Electronic Cigarettes (Vapourisers) among Adults in Great Britain. Action on Smoking and Health. Available online: http://ash.org.uk/information-and-resources/fact-sheets/use-of-electronic-cigarettes-vapourisers-among-adults-in-great-britain/ (accessed on 22 May 2017).
- West, R.; Beard, E.; Brown, J. Trends in Electronic Cigarette Use in England. Smoking in England. Available online: http://www.smokinginengland.info/latest-statistics/ (accessed on 24 May 2017).
- Schoenborn, C.A.; Clarke, T.C. QuickStats: Percentage of adults who ever used an e-cigarette and percentage who currently use e-cigarettes, by age group—National Health Interview Survey, United States, 2016. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 892. [Google Scholar] [CrossRef]
- Farsalinos, K.E.; Poulas, K.; Voudris, V.; Le Houezec, J. Electronic cigarette use in the European Union: Analysis of a representative sample of 27 460 Europeans from 28 countries. Addiction 2016, 111, 2032–2040. [Google Scholar] [CrossRef] [PubMed]
- Farsalinos, K.E.; Romagna, G.; Tsiapras, D.; Kyrzopoulos, S.; Voudris, V. Characteristics, perceived side effects and benefits of electronic cigarette use: A worldwide survey of more than 19 000 consumers. Int. J. Environ. Res. Public Health 2014, 11, 4356–4373. [Google Scholar] [CrossRef] [PubMed]
- Rodu, B. 2016 CDC Data Shows E-Cigarette Use Declines Again. Available online: https://rodutobaccotruth.blogspot.be/2017/09/2016-cdc-data-shows-e-cigarette-use.html (accessed on 13 October 2017).
- Farsalinos, K.E.; Romagna, G.; Voudris, V. Factors associated with dual use of tobacco and electronic cigarettes: A case control study. Int. J. Drug Policy 2015, 26, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, K.; Kuhn, S.; Reimer, J. Electronic cigarettes in Germany: Patterns of use and perceived health improvement. Eur. Addict. Res. 2017, 23, 136–147. [Google Scholar] [CrossRef] [PubMed]
- Rass, O.; Pacek, L.R.; Johnson, P.S.; Johnson, M.W. Characterizing use patterns and perceptions of relative harm in users of electronic and tobacco cigarettes. Exp. Clin. Psychopharmacol. 2015, 23, 494–503. [Google Scholar] [CrossRef] [PubMed]
- Pokhrel, P.; Herzog, T.A.; Muranaka, N.; Regmi, S.; Fagan, P. Contexts of cigarette and e-cigarette use among dual users: A qualitative study. BMC Public Health 2015, 15. [Google Scholar] [CrossRef] [PubMed]
- Fagerström, K. Determinants of tobacco use and renaming the FTND to the Fagerström Test for Cigarette Dependence. Nicotine Tob. Res. 2012, 14, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Qualtrics. Qualtrics; [Computer Software]; Qualtrics: Provo, Utah, 2016. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows; Version 24.0; [Computer Software]; IBM Corp.: Armonk, NY, USA, 2016. [Google Scholar]
- Stichting Tegen Kanker. Rookgedrag in België 2017. Available online: http://www.kanker.be/sites/default/files/stichting_tegen_kanker_-_enquete_rookgedrag_2017_1.pdf (accessed on 9 November 2017).
- Etter, J.F.; Bullen, C. A longitudinal study of electronic cigarette users. Addict. Behav. 2014, 29, 491–494. [Google Scholar] [CrossRef] [PubMed]
- Etter, J.F. Electronic cigarette: A longitudinal study of regular vapers. Nicotine Tob. Res. 2017. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, L.R.; Simmons, V.N.; Sutton, S.K.; Drobes, D.J.; Quinn, G.P.; Meade, C.D.; Unrod, M.; Brandon, K.O.; Harrell, P.T.; Eissenberg, T.; et al. A randomized controlled trial of a smoking cessation self-help intervention for dual users of tobacco cigarettes and e-cigarettes: Intervention development and research design. Contemp. Clin. Trials 2017, 60, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Mckeganey, N.; Dickson, T. Why don’t more smokers switch to using e-cigarettes: The views of confirmed smokers. Int. J. Environ. Res. Public Health 2017, 14, 647. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Total | Dual user | Switcher | Statistic | p-value |
|---|---|---|---|---|---|
| Age a | 42.57 (11.23) | 39.25 (13.08) | 43.33 (10.66) | t(213) = −2.09 | 0.04 |
| Gender | χ2 (1) = 7.90 | 0.005 | |||
| Man | 75 | 58 | 79 | ||
| Woman | 25 | 43 | 21 | ||
| Ethnicity | 0.12 b | ||||
| Caucasian | 98 | 95 | 98 | ||
| Asian | 0 | 3 | 0 | ||
| Mix ethnicity | 2 | 3 | 2 | ||
| Marital status | 0.10 b | ||||
| Single/unmarried | 20 | 35 | 17 | ||
| Married | 42 | 30 | 45 | ||
| Cohabiting | 31 | 28 | 32 | ||
| Divorced | 5 | 5 | 5 | ||
| Widow(er) | 2 | 3 | 2 | ||
| Highest degree | 0.62 b | ||||
| Primary school | 3 | 8 | 3 | ||
| High school | 47 | 45 | 47 | ||
| Bachelor’s | 40 | 38 | 40 | ||
| University | 9 | 10 | 9 | ||
| Other | 0 | 0 | 1 | ||
| Occupation | 0.08 b | ||||
| Student | 3 | 8 | 2 | ||
| Working part-time | 15 | 20 | 14 | ||
| Working full-time | 62 | 48 | 66 | ||
| Housewife/-man | 8 | 5 | 9 | ||
| Job seeker | 7 | 13 | 6 | ||
| Retired | 5 | 8 | 4 | ||
| Monthly net income | χ2 (5) = 8.43 | 0.13 | |||
| Under 1000 € | 13 | 20 | 11 | ||
| 1000–1500 € | 15 | 15 | 16 | ||
| 1500–2000 € | 29 | 38 | 27 | ||
| 2000–2500 € | 22 | 8 | 25 | ||
| 2500–3000 € | 11 | 13 | 10 | ||
| More than 3000 € | 10 | 8 | 10 |
| Variable | Total | Dual User | Switcher | Statistic | p-Value |
|---|---|---|---|---|---|
| Age start smoking a | 15.03 (2.61) | 14.70 (1.58) | 15.10 (2.79) | t(213) = −0.88 | 0.38 |
| Product used before e-cig use | 0.45 b | ||||
| Filtered cigarettes | 52 | 60 | 50 | ||
| Cigarettes without filter | 0 | 0 | 1 | ||
| Rolling tobacco | 38 | 30 | 39 | ||
| Cigars | 1 | 3 | 1 | ||
| Different products | 9 | 8 | 9 | ||
| How often smoked before e-cig use | 1 b | ||||
| Daily | 98 | 100 | 98 | ||
| Multiple days per week, not daily | 1 | 0 | 2 | ||
| Multiple times per month | 0 | 0 | 1 | ||
| Mean CPD before e-cig use a | 22.24 (12.34) | 22.33 (13.01) | 22.23 (12.22) | t(213) = 0.05 | 0.96 |
| Tried to quit smoking? | 0.27 b | ||||
| Yes | 88 | 83 | 90 | ||
| No | 12 | 18 | 10 | ||
| Mean quit attempts a | 5.07 (4.62) | 7.36 (7.13) | 4.59 (3.75) | t(188) = 3.21 | <0.001 |
| Longest period quitted smoking (months) a | 12.98 (17.14) | 9.15 (14.27) | 13.79 (17.62) | t(188) = −1.42 | 0.16 |
| Time since last cigarette smoked | <0.001 b | ||||
| One day or less | 13 | 68 | 1 | ||
| Between a day and a week | 5 | 20 | 1 | ||
| Between a week and a month | 5 | 10 | 4 | ||
| Between a month and a year | 33 | 3 | 39 | ||
| More than one year | 45 | 0 | 55 | ||
| Cessation aids used quitting smoking | |||||
| NRT | 52 | 56 | 55 | χ2 (1) = 0.79 | 0.37 |
| Medication | 24 | 33 | 32 | χ2 (1) = 1.53 | 0.22 |
| E-cig | 15 | 10 | 11 | 0.54 b | |
| Counseling | 6 | 19 | 17 | χ2 (1) = 3.79 | 0.05 |
| Willpower (no aid) | 58 | 61 | 60 | χ2 (1) = 0.60 | 0.44 |
| Alternative (laser, hypnotherapy, …) | 6 | 9 | 8 | 0.74 b | |
| Cessation aids used longest period quitted smoking | |||||
| NRT | 12 | 5 | 6 | χ2 (1) = 1.82 | 0.18 |
| Medication | 9 | 8 | 8 | χ2 (1) = 0.02 | 0.89 |
| E-cig | 61 | 71 | 69 | χ2 (1) = 2.69 | 0.10 |
| Counseling | 3 | 3 | 3 | χ2 (1) = 0.01 b | 1 |
| Willpower (no aid) | 27 | 18 | 20 | χ2 (1) = 0.79 | 0.38 |
| Alternative (laser, hypnotherapy, …) | 0 | 3 | 2 | χ2 (1) = 0.93 | 1 |
| Product use now | <0.001 b | ||||
| Nothing | 81 | 0 | 100 | ||
| Filtered cigarettes | 15 | 83 | 0 | ||
| Rolling tobacco | 2 | 13 | 0 | ||
| Cigars | 0 | 3 | 0 | ||
| Cannabis | 0 | 3 | 0 | ||
| How often smoking now | χ2 (3) = 194.06 | <0.001 | |||
| Never | 81 | 0 | 100 | ||
| Daily | 9 | 50 | 0 | ||
| Multiple days per week, not daily | 6 | 30 | 0 | ||
| Multiple times per month | 4 | 20 | 0 | ||
| Mean CPD now a | / | 3.92 (5.48) | / | / | / |
| FTCD-score a | / | 3.35 (2.41) | / | / | / |
| Future plans regarding smoking | <0.001 b | ||||
| Do not want to quit completely | 3 | 15 | 0 | ||
| Thinking about quitting, not in next 6 months | 3 | 15 | 0 | ||
| Thinking about quitting, in next 6 months | 6 | 33 | 0 | ||
| Thinking about quitting, in next month | 6 | 33 | 0 | ||
| Thinking about quitting, in next week | 1 | 5 | 0 | ||
| Already quit smoking completely | 81 | 0 | 100.00 |
| Variable | Total | Dual User | Switcher | Statistic | p-Value |
|---|---|---|---|---|---|
| E-cig FTCD-score a | 9.84 (0.51) | 9.80 (0.56) | 9.85 (0.49) | t(213) = −0.58 | 0.56 |
| Started with e-cigs (months) a | 21.81 (19.11) | 17.30 (18.37) | 22.84 (19.18) | t(213) = −1.66 | 0.10 |
| E-cig type | χ2 (2) = 2.80 | 0.25 | |||
| Upgrade needed | 6 | 10 | 5 | ||
| Mixed category | 25 | 30 | 24 | ||
| Up-to-date | 69 | 60 | 71 | ||
| Nicotine level | 0.75 b | ||||
| 0 mg/mL | 11 | 10 | 11 | ||
| 4–8 mg/mL | 63 | 58 | 64 | ||
| 9–16 mg/mL | 23 | 30 | 22 | ||
| 17–24 mg/mL | 3 | 3 | 3 | ||
| Flavor regular use | χ2 (1) = 1.61 | 0.21 | |||
| Tobacco | 27 | 35 | 25 | ||
| Other | 73 | 65 | 75 | ||
| Flavor at e-cig initiation | χ2 (1) = 2.66 | 0.26 | |||
| Tobacco | 68 | 73 | 67 | ||
| Other | 32 | 28 | 33 | ||
| PG/VG proportions | χ2 (2) = 3.68 | 0.16 | |||
| Dominant PG | 27 | 37 | 25 | ||
| 50/50 | 37 | 39 | 37 | ||
| Dominant VG | 36 | 24 | 39 | ||
| How often vaping | 0.34 b | ||||
| Daily | 99 | 98 | 99 | ||
| Multiple days per week, not daily | 1 | 3 | 1 | ||
| Puffs per day | χ2 (3) = 5.71 | 0.13 | |||
| 100 puffs or less | 16 | 25 | 14 | ||
| 101–200 puffs | 34 | 23 | 37 | ||
| 201–300 puffs | 28 | 35 | 27 | ||
| 301 puffs or more | 22 | 18 | 23 | ||
| Mean amount of liquid used (mL/week) | 38.11 (26.36) | 23.65 (15.48) | 41.42 (27.24) | t(213) = −3.98 | <0.001 |
| Future plans regarding vaping | χ2 (2) = 0.05 | 0.97 | |||
| Continue to use as now | 67 | 65 | 67 | ||
| Try to cut back | 27 | 28 | 26 | ||
| Try to cut completely | 7 | 8 | 7 | ||
| Future plans regarding nicotine level | χ2 (2) = 4.07 | 0.13 | |||
| Continue same concentration as now | 27 | 17 | 24 | ||
| Try to cut back | 32 | 44 | 29 | ||
| Switching to zero nicotine | 41 | 39 | 42 | ||
| Reasons to start vaping | |||||
| Smoking is unhealthy | 4.41 (1.02) | 4.43 (0.87) | 4.41 (1.05) | t(213) = 0.11 | 0.91 |
| More advantages than other cessation aids | 4.37 (1.00) | 4.48 (0.72) | 4.34 (1.05) | t(213) = 0.76 | 0.45 |
| To quit smoking completely | 4.10 (1.33) | 3.85 (1.19) | 4.16 (1.36) | t(213) = −1.33 | 0.19 |
| Out of curiosity | 3.38 (1.40) | 3.15 (1.33) | 3.43 (1.41) | t(213) = −1.16 | 0.25 |
| Smoking tobacco cigarettes is too expensive | 3.28 (1.38) | 3.63 (1.44) | 3.20 (1.36) | t(213) = 1.76 | 0.08 |
| Smoking bothered other people | 2.58 (1.36) | 2.45 (1.41) | 2.61 (1.36) | t(213) = −0.67 | 0.50 |
| To vape were smoking is prohibited | 2.46 (1.32) | 2.88 (1.47) | 2.36 (1.27) | t(213) = 2.24 | 0.03 |
| To reduce smoking | 2.34 (1.40) | 3.18 (1.36) | 2.15 (1.34) | t(213) = 4.33 | <0.001 |
| People around me are also vaping | 2.17 (1.67) | 2.48 (1.24) | 2.10 (1.55) | t(213) = 1.83 | 0.07 |
| Reasons to continue vaping | |||||
| Smoking is unhealthy | 4.63 (0.78) | 4.53 (0.85) | 4.66 (0.76) | t(213) = −0.97 | 0.33 |
| More advantages than other cessation aids | 4.58 (0.79) | 4.60 (0.74) | 4.57 (0.80) | t(213) = 0.21 | 0.84 |
| It is pleasant | 4.56 (0.62) | 4.48 (0.55) | 4.58 (0.64) | t(213) = −0.99 | 0.32 |
| Smoking tobacco cigarettes is too expensive | 3.48 (1.27) | 3.68 (1.31) | 3.44 (1.26) | t(213) = 1.06 | 0.29 |
| Smoking bothered other people | 3.39 (1.21) | 3.23 (1.27) | 3.42 (1.91) | t(213) = −0.94 | 0.35 |
| To vape were smoking is prohibited | 2.65 (1.26) | 2.95 (1.50) | 2.58 (1.20) | t(213) = 1.69 | 0.09 |
| People around me are also vaping | 2.27 (1.12) | 2.33 (1.21) | 2.26 (1.10) | t(213) = 0.32 | 0.75 |
| It helps me to smoke less a | / | 4.65 (0.77) | / | / | / |
| To quit smoking completely in time a | / | 4.30 (0.99) | / | / | / |
| To reduce smoking a | / | 2.28 (1.50) | / | / | / |
| To prevent relapsing to smoking a | / | / | 4.24 (1.00) | / | / |
| Variable | Total | Dual User | Switcher | Statistic | p-Value |
|---|---|---|---|---|---|
| Risk perception | 1.86 (0.62) | 1.83 (0.66) | 1.86 (0.61) | t(213) = −0.37 | 0.72 |
| The faster I quit vaping, the better | 2.56 (1.14) | 2.63 (1.30) | 2.54 (1.11) | t(213) = 0.41 | 0.68 |
| Concerns regarding long term health effects e-cig | 2.31 (1.01) | 2.13 (1.02) | 2.35 (1.01) | t(213) = −1.27 | 0.21 |
| Concerns regarding long term e-cig use | 1.95 (0.87) | 1.85 (0.92) | 1.98 (0.86) | t(213) = −0.83 | 0.41 |
| Fear problems with heart and blood vessels | 1.69 (0.74) | 1.73 (0.85) | 1.69 (0.71) | t(213) = 0.30 | 0.76 |
| Fear breathing problems due to e-cig use | 1.65 (0.71) | 1.58 (0.64) | 1.67 (0.72) | t(213) = 0.76 | 0.45 |
| Fear for lung cancer | 1.59 (0.74) | 1.60 (0.87) | 1.59 (0.71) | t(213) = 0.09 | 0.93 |
| E-cig is as harmful as a cigarette | 1.25 (0.50) | 1.28 (0.51) | 1.24 (0.50) | t(213) = 0.40 | 0.69 |
| E-cig efficacy | 4.30 (0.45) | 3.97 (0.56) | 4.37 (0.40) | t(213) = −5.18 | <0.001 |
| Less desire for cigarettes | 4.89 (0.37) | 4.60 (0.67) | 4.96 (0.20) | t(213) = −6.08 | <0.001 |
| Decreased smoking | 4.81 (0.69) | 4.88 (0.34) | 4.79 (0.75) | t(213) = 0.67 | 0.50 |
| After vaping I do not immediately smoke | 4.73 (0.78) | 3.90 (1.34) | 4.93 (0.39) | t(213) = −8.74 | <0.001 |
| No need for cigarette after vaping for a while | 4.70 (0.77) | 4.25 (0.84) | 4.80 (0.72) | t(213) = −4.23 | <0.001 |
| Less desire for nicotine | 4.27 (0.92) | 4.18 (0.93) | 4.30 (0.92) | t(213) = −0.75 | 0.45 |
| Throat hit is comparable | 3.47 (1.08) | 3.00 (1.11) | 3.57 (1.04) | t(213) = −3.09 | 0.002 |
| Act vaping is comparable with smoking | 3.20 (1.24) | 3.00 (1.34) | 3.25 (1.21) | t(213) = −1.16 | 0.25 |
| Practical problems | 1.87 (0.71) | 2.16 (0.74) | 1.80 (0.69) | t(213) = 2.94 | 0.004 |
| Purchasing liquids is difficult | 1.99 (1.26) | 2.18 (1.28) | 1.94 (1.25) | t(213) = 1.06 | 0.29 |
| Battery empty at inconvenient moments | 1.97 (1.00) | 2.48 (1.06) | 1.85 (0.95) | t(213) = 3.65 | <0.001 |
| Inconvenient to carry material of e-cig | 1.92 (0.98) | 2.40 (1.19) | 1.81 (0.89) | t(213) = 3.53 | 0.001 |
| Purchasing e-cig is difficult | 1.92 (1.83) | 2.00 (1.13) | 1.90 (1.20) | t(213) = 0.47 | 0.64 |
| Difficult to not forget anything for using e-cig | 1.89 (0.96) | 2.25 (1.08) | 1.81 (0.91) | t(213) = 2.68 | 0.008 |
| Purchasing coils and other parts is difficult | 1.84 (1.14) | 2.00 (1.16) | 1.81 (1.13) | t(213) = 0.98 | 0.33 |
| Malfunction e-cig | 1.57 (0.79) | 1.85 (0.98) | 1.15 (0.73) | t(213) = 2.49 | 0.01 |
| Social component | 3.33 (0.65) | 3.41 (0.75) | 3.31 (0.62) | t(213) = 0.93 | 0.35 |
| Environment obligates me to vape outside | 4.00 (1.13) | 3.95 (1.32) | 4.01 (1.08) | t(213) = −0.28 | 0.78 |
| Environment still sees me as addicted | 3.65 (0.91) | 3.90 (0.98) | 3.59 (0.89) | t(213) = 1.93 | 0.06 |
| Others see vapor as harmful as cigarette smoke | 3.64 (1.06) | 3.65 (1.15) | 3.63 (1.04) | t(213) = 0.09 | 0.93 |
| I feel obligated to stand outside with smokers | 3.35 (1.30) | 3.38 (1.44) | 3.35 (1.27) | t(213) = 0.12 | 0.91 |
| When vaping, others still consider me as a smoker | 3.34 (1.17) | 3.58 (1.08) | 3.29 (1.83) | t(213) = 1.42 | 0.16 |
| Environment sees switch to e-cig as not positive | 1.98 (0.83) | 2.03 (0.92) | 1.97 (0.81) | t(213) = 0.37 | 0.71 |
| Negative consequences | 1.52 (0.36) | 1.67 (0.42) | 1.49 (0.34) | t(213) = 2.92 | 0.004 |
| More technical problems | 2.75 (1.07) | 2.78 (1.03) | 2.75 (1.09) | t(213) = 0.14 | 0.89 |
| Dry mouth | 2.40 (1.00) | 2.60 (1.03) | 2.35 (0.99) | t(213) = 1.44 | 0.15 |
| Dry throat | 2.10 (0.96) | 2.30 (1.04) | 2.05 (0.94) | t(213) = 1.48 | 0.14 |
| Increased weight | 1.64 (1.01) | 1.50 (0.85) | 1.67 (1.04) | t(213) = −0.99 | 0.33 |
| Coughing | 1.52 (0.70) | 1.83 (0.87) | 1.45 (0.64) | t(213) = 3.09 | 0.002 |
| Bad taste when vaping | 1.51 (0.69) | 1.88 (0.85) | 1.42 (0.62) | t(213) = 3.86 | <0.001 |
| Sore throat | 1.39 (0.62) | 1.63 (0.81) | 1.33 (0.55) | t(213) = 2.77 | 0.006 |
| Worrying about health | 1.37 (0.61) | 1.40 (0.67) | 1.37 (0.60) | t(213) = 0.32 | 0.75 |
| Unpleasant sensation in throat | 1.33 (0.58) | 1.48 (0.72) | 1.30 (0.54) | t(213) = 1.70 | 0.09 |
| Bad physical condition | 1.30 (0.63) | 1.60 (0.87) | 1.23 (0.54) | t(213) = 3.38 | 0.001 |
| Sleeping problems | 1.28 (0.70) | 1.60 (0.96) | 1.21 (0.60) | t(213) = 3.26 | 0.001 |
| Headache | 1.27 (0.54) | 1.33 (0.57) | 1.26 (0.53) | t(213) = 0.72 | 0.47 |
| Increased heart rate or palpitations | 1.24 (0.52) | 1.40 (0.63) | 1.20 (0.48) | t(213) = 2.23 | 0.03 |
| Unpleasant odors when using | 1.23 (0.50) | 1.20 (0.41) | 1.23 (0.52) | t(213) = −0.39 | 0.70 |
| Bad taste | 1.22 (0.55) | 1.28 (0.60) | 1.21 (0.54) | t(213) = 0.72 | 0.47 |
| Breathing problems | 1.21 (0.47) | 1.40 (0.63) | 1.17 (0.42) | t(213) = 2.79 | 0.006 |
| Bad smell | 1.13 (0.37) | 1.23 (0.53) | 1.11 (0.32) | t(213) = 1.72 | 0.09 |
| Positive consequences | 4.20 (0.49) | 3.84 (0.56) | 4.28 (0.43) | t(213) = −5.45 | <0.001 |
| Craving for cigarette is reduced | 4.87 (0.38) | 4.63 (0.59) | 4.93 (0.28) | t(213) = −4.78 | <0.001 |
| Could decrease smoking | 4.71 (0.71) | 4.78 (0.42) | 4.69 (0.76) | t(213) = 0.67 | 0.50 |
| Could quit smoking | 4.59 (0.90) | 3.10 (0.98) | 4.93 (0.39) | t(213) = −19.06 | <0.001 |
| Smell/taste cigarette is less pleasant | 4.54 (0.91) | 4.13 (1.14) | 4.64 (0.82) | t(213) = −3.32 | 0.001 |
| Fresher breath | 4.49 (0.73) | 4.33 (0.69) | 4.53 (0.73) | t(213) = −1.58 | 0.12 |
| More pleasure in vaping than in smoking | 4.38 (0.90) | 4.10 (1.08) | 4.45 (0.84) | t(213) = −2.22 | 0.03 |
| Fitness and health are improved | 4.38 (0.82) | 4.00 (1.01) | 4.47 (0.75) | t(213) = −3.33 | 0.001 |
| Less coughing | 4.36 (0.98) | 4.00 (1.13) | 4.44 (0.92) | t(213) = −2.61 | 0.01 |
| Better breathing | 4.31 (0.83) | 3.88 (0.91) | 4.41 (0.77) | t(213) = −3.78 | <0.001 |
| Improved sense of smell | 4.24 (0.88) | 3.68 (0.97) | 4.37 (0.81) | t(213) = −4.68 | <0.001 |
| Improved taste | 4.24 (0.84) | 3.75 (0.87) | 4.35 (0.80) | t(213) = −4.26 | <0.001 |
| Less disturbing for other people | 3.84 (1.06) | 3.65 (1.25) | 3.89 (1.01) | t(213) = −1.28 | 0.20 |
| More often in a good mood | 3.62 (1.04) | 3.8 (1.09) | 3.65 (1.03) | t(213) = −0.97 | 0.34 |
| Improved sleep quality | 3.58 (1.01) | 3.35 (1.00) | 3.63 (1.01) | t(213) = −1.58 | 0.12 |
| Possible to vape in several places | 3.57 (1.29) | 3.68 (1.42) | 3.55 (1.26) | t(213) = 0.56 | 0.58 |
| Improved appetite | 3.50 (0.98) | 3.00 (0.93) | 3.62 (0.95) | t(213) = −3.72 | <0.001 |
| ‘Addiction’ to cigarettes | 1.76 (1.06) | 3.28 (0.95) | 1.41 (0.72) | t(213) = 13.85 | <0.001 |
| I cannot resist the act of smoking | 1.92 (1.32) | 3.38 (1.08) | 1.58 (1.13) | t(213) = 9.15 | <0.001 |
| Addicted to cigarette at this moment | 1.60 (1.06) | 3.18 (1.08) | 1.23 (0.64) | t(213) = 14.93 | <0.001 |
| I consider my addiction to cigarettes as problematic a | / | 3.53 (1.33) | / | / | / |
| ‘Addiction’ to e-cigs | 3.53 (0.93) | 3.28 (1.09) | 3.59 (0.88) | t(213) = −1.98 | 0.05 |
| Addicted to e-cig at this moment | 3.55 (0.97) | 3.28 (1.15) | 3.62 (0.92) | t(213) = −2.02 | 0.05 |
| I cannot resist the act of vaping | 3.52 (1.02) | 3.28 (1.11) | 3.57 (0.99) | t(213) = −1.67 | 0.10 |
| I consider my addiction to e-cigs as problematic a | 1.83 (0.82) | 2.13 (0.92) | 1.77 (0.79) | t(135) = 1.94 | 0.06 |
| ‘Addiction’ to nicotine | 2.66 (0.94) | 2.93 (0.99) | 2.60 (0.92) | t(213) = 1.97 | 0.05 |
| I am more addicted to nicotine since vaping | 2.00 (1.09) | 2.13 (1.20) | 1.97 (1.06) | t(213) = 0.80 | 0.42 |
| I feel addicted to nicotine | 3.33 (1.18) | 3.73 (1.18) | 3.23 (1.16) | t(213) = 2.10 | 0.02 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adriaens, K.; Van Gucht, D.; Baeyens, F. Differences between Dual Users and Switchers Center around Vaping Behavior and Its Experiences Rather than Beliefs and Attitudes. Int. J. Environ. Res. Public Health 2018, 15, 12. https://doi.org/10.3390/ijerph15010012
Adriaens K, Van Gucht D, Baeyens F. Differences between Dual Users and Switchers Center around Vaping Behavior and Its Experiences Rather than Beliefs and Attitudes. International Journal of Environmental Research and Public Health. 2018; 15(1):12. https://doi.org/10.3390/ijerph15010012
Chicago/Turabian StyleAdriaens, Karolien, Dinska Van Gucht, and Frank Baeyens. 2018. "Differences between Dual Users and Switchers Center around Vaping Behavior and Its Experiences Rather than Beliefs and Attitudes" International Journal of Environmental Research and Public Health 15, no. 1: 12. https://doi.org/10.3390/ijerph15010012