Global Mortality Burden of Cirrhosis and Liver Cancer Attributable to Injection Drug Use, 1990–2016: An Age-Period-Cohort and Spatial Autocorrelation Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Age-Period-Cohort Analysis
2.3. Spatial Autocorrelation Analysis
3. Results
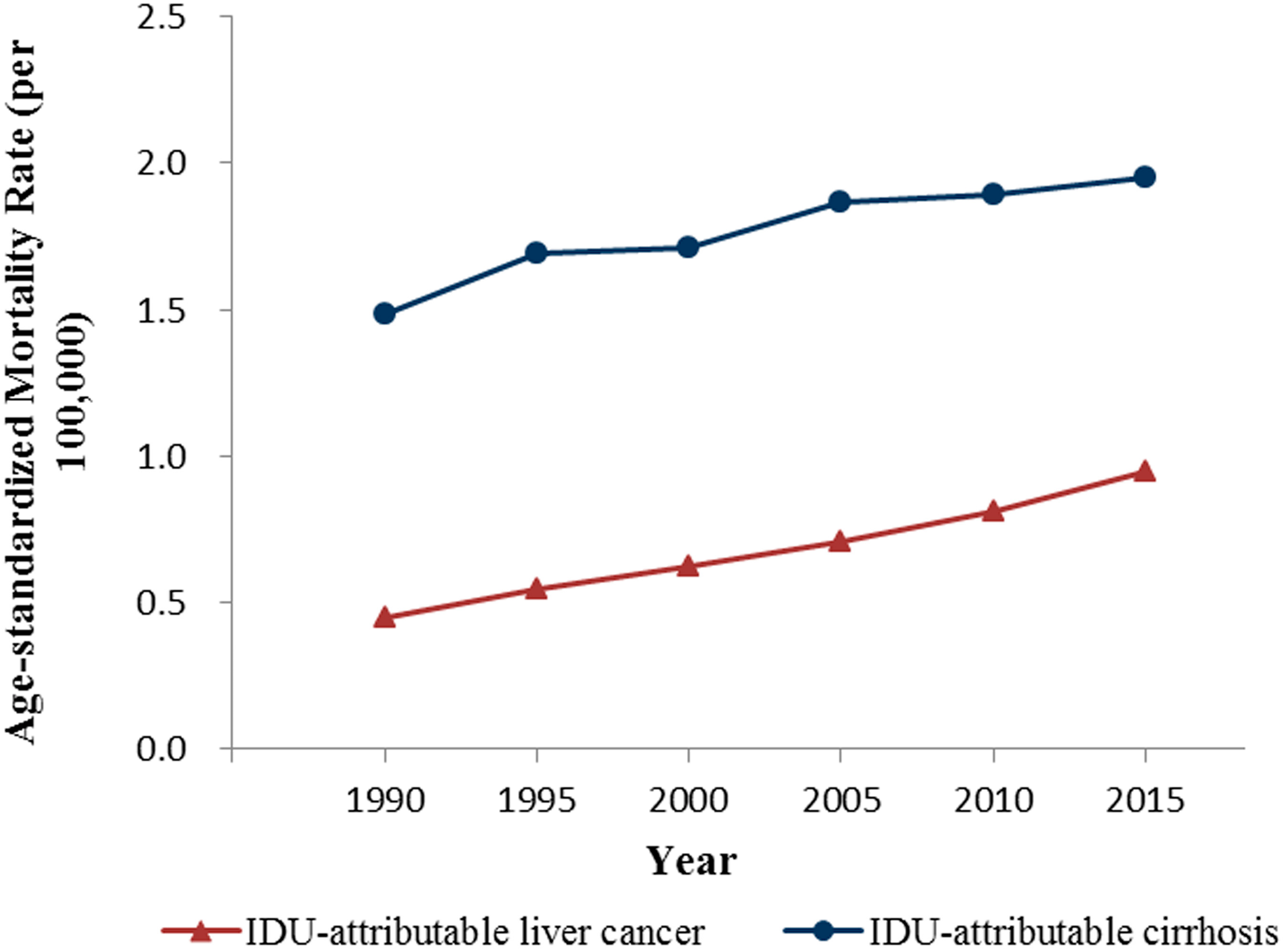
3.1. Global Mortality Trends of Cirrhosis and Liver Cancer Attributable to Injection Drug Use
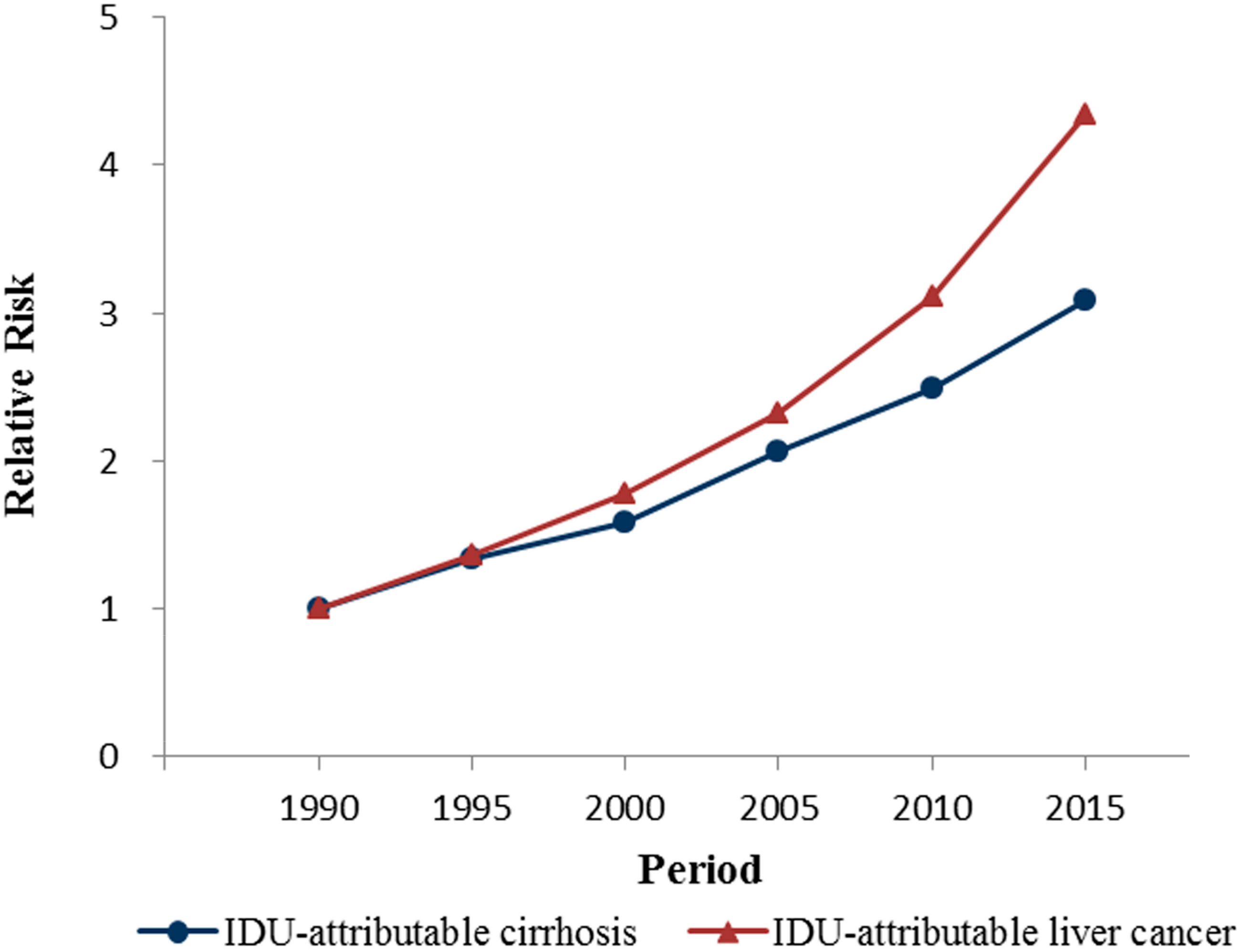
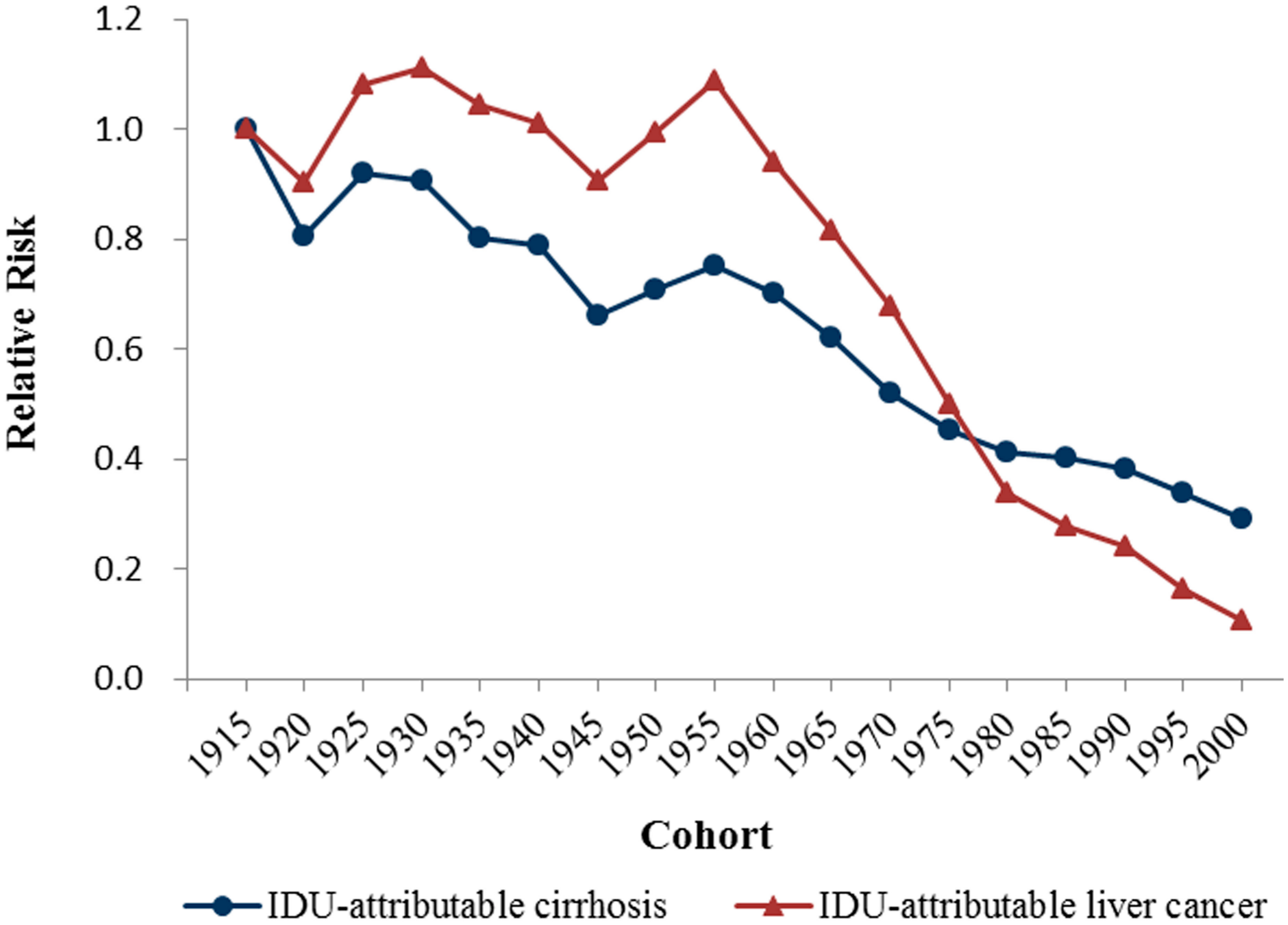
3.2. The Results of Age-Period-Cohort Model Analysis
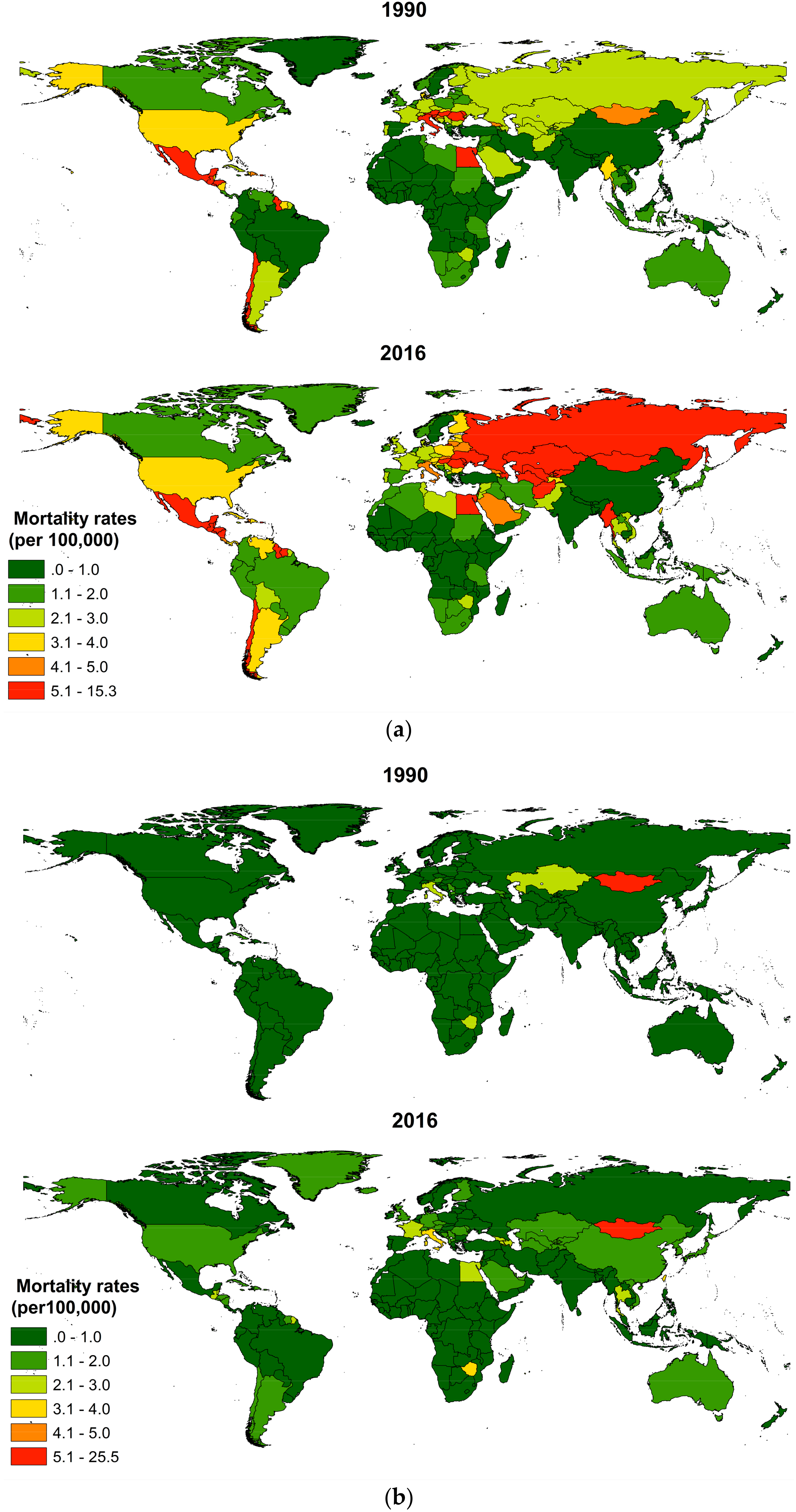
3.3. Country-Level Mortality of IDU-Attributable Cirrhosis and IDU-Attributable Liver Cancer from 1990 to 2016
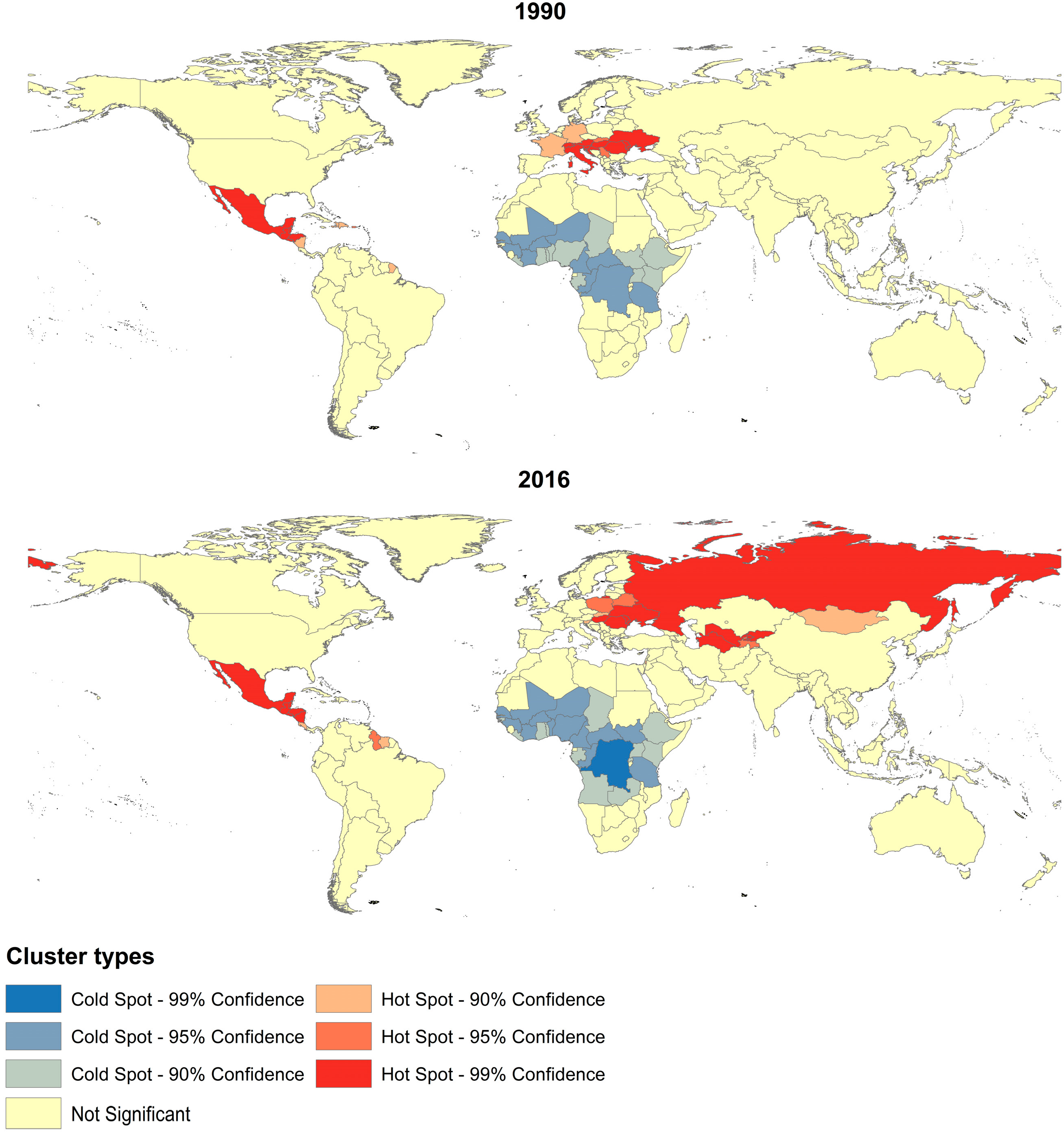
3.4. The Results of Spatial Autocorrelation
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Chen, C.Y.; Lin, K.M. Health consequences of illegal drug use. Curr. Opin. Psychiatry 2009, 22, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Roy, E.; Arruda, N.; Bruneau, J.; Jutras-Aswad, D. Epidemiology of Injection Drug Use: New Trends and Prominent Issues. Can. J. Psychiatry 2016, 61, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Kleinman, S.H.; Busch, M.P. The risks of transfusion-transmitted infection: Direct estimation and mathematical modelling. Best Pract. Res. Clin. Haematol. 2000, 13, 631–649. [Google Scholar] [CrossRef] [PubMed]
- Bravo, Z.J.; Loza, M.C.; Lopez-Alcalde, J. Isolation as a strategy for controlling the transmission of hepatitis C virus (HCV) infection in haemodialysis units. Cochrane Database Syst. Rev. 2016, CD006420. [Google Scholar] [CrossRef]
- McMahon, J.M.; Tortu, S. A potential hidden source of hepatitis C infection among noninjecting drug users. J. Psychoact. Drugs 2003, 35, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Lanini, S.; Easterbrook, P.J.; Zumla, A.; Ippolito, G. Hepatitis C: Global epidemiology and strategies for control. Clin. Microbiol. Infect. 2016, 22, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Daw, M.A.; El-Bouzedi, A.A.; Ahmed, M.O.; Dau, A.A.; Agnan, M.M.; Drah, A.M. Geographic integration of hepatitis C virus: A global threat. World J. Virol. 2016, 5, 170–182. [Google Scholar] [CrossRef] [PubMed]
- Prati, D. Transmission of hepatitis C virus by blood transfusions and other medical procedures: A global review. J. Hepatol. 2006, 45, 607–616. [Google Scholar] [CrossRef] [PubMed]
- Alter, M.J. Epidemiology of hepatitis C virus infection. World J. Gastroenterol. 2007, 13, 2436–2441. [Google Scholar] [CrossRef] [PubMed]
- Bussink, C.; Macdonald, D.; Carpentier, C.; Niaz, K.; Dávalos, L.M.; Pietschmann, T.; Davis, P.; Raithelhuber, M.; Durán-Martínez, A.; Saloga, C.W.; et al. World Drug Report 2016; United Nations Office on Drugs and Crime: Vienna, Austria, 2016. [Google Scholar]
- Nelson, P.K.; Mathers, B.M.; Cowie, B.; Hagan, H.; Des Jarlais, D.; Horyniak, D.; Degenhardt, L. Global epidemiology of hepatitis B and hepatitis C in people who inject drugs: Results of systematic reviews. Lancet 2011, 378, 571–583. [Google Scholar] [CrossRef]
- Perz, J.F.; Armstrong, G.L.; Farrington, L.A.; Hutin, Y.J.; Bell, B.P. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J. Hepatol. 2006, 45, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Dore, G.J.; Freeman, A.J.; Law, M.; Kaldor, J.M. Is severe liver disease a common outcome for people with chronic hepatitis C? J. Gastroenterol. Hepatol. 2002, 17, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Degenhardt, L.; Charlson, F.; Stanaway, J.; Larney, S.; Alexander, L.T.; Hickman, M.; Cowie, B.; Hall, W.D.; Strang, J.; Whiteford, H.; et al. Estimating the burden of disease attributable to injecting drug use as a risk factor for HIV, hepatitis C, and hepatitis B: Findings from the Global Burden of Disease Study 2013. Lancet Infect. Dis. 2016, 16, 1385–1398. [Google Scholar] [CrossRef]
- Colombo, M.; Maisonneuve, P. Controlling liver cancer mortality on a global scale: Still a long way to go. J. Hepatol. 2017, 67, 216–217. [Google Scholar] [CrossRef] [PubMed]
- Kao, J.H. Hepatitis B vaccination and prevention of hepatocellular carcinoma. Best Pract. Res. Clin. Gastroenterol. 2015, 29, 907–917. [Google Scholar] [CrossRef] [PubMed]
- Lim, E.J.; Torresi, J. Prevention of hepatitis C virus infection and liver cancer. Recent Results Cancer Res. 2014, 193, 113–133. [Google Scholar] [CrossRef] [PubMed]
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef]
- Gakidou, E.; Afshin, A.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulle, A.M.; Abera, S.F.; Aboyans, V.; et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar] [CrossRef]
- Pesce, G. Mortality rates for chronic lower respiratory diseases in Italy from 1979 to 2010: An age-period-cohort analysis. ERJ Open Res. 2016, 2. [Google Scholar] [CrossRef] [PubMed]
- Kupper, L.L.; Janis, J.M.; Karmous, A.; Greenberg, B.G. Statistical age-period-cohort analysis: A review and critique. J. Chronic Dis. 1985, 38, 811–830. [Google Scholar] [CrossRef]
- Holford, T.R. The estimation of age, period and cohort effects for vital rates. Biometrics 1983, 39, 311–324. [Google Scholar] [CrossRef] [PubMed]
- Holford, T.R. Understanding the effects of age, period, and cohort on incidence and mortality rates. Annu. Rev. Public Health 1991, 12, 425–457. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, P.S.; Anderson, W.F. Age-period-cohort models in cancer surveillance research: Ready for prime time? Cancer Epidemiol. Biomark. Prev. 2011, 20, 1263–1268. [Google Scholar] [CrossRef] [PubMed]
- Mason, K.O.; Mason, W.M.; Winsborough, H.H. Some Methodological Issues in Cohort Analysis of Archival Data. Am. Sociol. Assoc. 1973, 38, 242–258. [Google Scholar] [CrossRef]
- Robertson, C.; Gandini, S.; Boyle, P. Age-period-cohort models: A comparative study of available methodologies. J. Clin. Epidemiol. 1999, 52, 569–583. [Google Scholar] [CrossRef]
- Yang, Y. A Methodological Comparison of Age-Period-Cohort Models: The Intrinsic Estimator and Conventional Generalized Linear Models. Sociol. Methodol. 2004, 34, 75–110. [Google Scholar] [CrossRef]
- Yang, Y. The intrinsic estimator for age-period-cohort analysis: What it is and how to use it. Am. J. Sociol. 2008, 113, 1697–1736. [Google Scholar] [CrossRef]
- Robinson, T.P. Spatial statistics and geographical information systems in epidemiology and public health. Adv. Parasitol. 2000, 47, 81–128. [Google Scholar] [PubMed]
- Rosenberg, M. The bearing correlogram: A new method of analyzing directional spatial autocorrelation. Geogr. Anal. 2000, 3, 267–278. [Google Scholar] [CrossRef]
- Moran, P.A. Notes on continuous stochastic phenomena. Biometrika 1950, 37, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Getis, A. The analysis of spatial association by use of distance statistics. Geogr. Anal. 1992, 24, 189–206. [Google Scholar] [CrossRef]
- Westbrook, R.H.; Dusheiko, G. Natural history of hepatitis C. J. Hepatol. 2014, 61, S58–S68. [Google Scholar] [CrossRef] [PubMed]
- Bialecki, E.S.; Di Bisceglie, A.M. Clinical presentation and natural course of hepatocellular carcinoma. Eur. J. Gastroenterol. Hepatol. 2005, 17, 485–489. [Google Scholar] [CrossRef] [PubMed]
- Hughes, P.H.; Rieche, O. Heroin epidemics revisited. Epidemiol. Rev. 1995, 17, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Gfroerer, J.; Brodsky, M. The incidence of illicit drug use in the United States, 1962–1989. Br. J. Addict. 1992, 87, 1345–1351. [Google Scholar] [CrossRef] [PubMed]
- Geraghty, J. Drug policy, intravenous drug use, and heroin addiction in the UK. Br. J. Nurs. 2011, 20, 878–884. [Google Scholar] [CrossRef] [PubMed]
- Suwanwela, C.; Poshyachinda, V. Drug abuse in Asia. Bull. Narc. 1986, 38, 41–53. [Google Scholar] [PubMed]
- Skaftason, J.F.; Kristinsson, J.; Johannesson, T. Injection medicines: Historical notes on their use and development, with special reference to Icelandic conditions. Laeknabladid 2011, 97, 169–174. [Google Scholar] [PubMed]
- Steigmann, F.; Hyman, S.; Goldbloom, R. Infectious hepatitis (homologous serum type) in drug addicts. Gastroenterology 1950, 15, 642–646. [Google Scholar] [PubMed]
- Appelbaum, E.; Kalkstein, M. Artificial transmission of viral hepatitis among intravenous diacetylmorphine addicts. J. Am. Med. Assoc. 1951, 147, 222–224. [Google Scholar] [CrossRef] [PubMed]
- Cardon, P.V.; Beck, E.M. The recent occurrence of hepatitis among drug addicts of New York City. J. Med. 1952, 52, 1037–1038. [Google Scholar]
- Choo, Q.L.; Kuo, G.; Weiner, A.J.; Overby, L.R.; Bradley, D.W.; Houghton, M. Isolation of a cDNA clone derived from a blood-borne non-A, non-B viral hepatitis genome. Science 1989, 244, 359–362. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, P.G.; Hill, D.A.; Appleyard, K.; Taylor, A.; Hutchinson, S.; Goldberg, D.J. Prevalence of antibodies to hepatitis C virus, HIV and human T-cell leukaemia/lymphoma viruses in injecting drug users in Tayside, Scotland, 1993–1997. Epidemiol. Infect. 2001, 126, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Crofts, N. Going where the epidemic is: Epidemiology and control of hepatitis C among injecting drug users. Aust. Fam. Phys. 2001, 30, 420–425. [Google Scholar]
- Samuel, M.C.; Doherty, P.M.; Bulterys, M.; Jenison, S.A. Association between heroin use, needle sharing and tattoos received in prison with hepatitis B and C positivity among street-recruited injecting drug users in New Mexico, USA. Epidemiol. Infect. 2001, 127, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Roy, K.; Hay, G.; Andragetti, R.; Taylor, A.; Goldberg, D.; Wiessing, L. Monitoring hepatitis C virus infection among injecting drug users in the European Union: A review of the literature. Epidemiol. Infect. 2002, 129, 577–585. [Google Scholar] [CrossRef] [PubMed]
- Metlay, G. Federalizing medical campaigns against alcoholism and drug abuse. Milbank Q. 2013, 91, 123–162. [Google Scholar] [CrossRef] [PubMed]
- Thokala, P.; Simpson, E.L.; Tappenden, P.; Stevens, J.W.; Dickinson, K.; Ryder, S.; Harrison, P. Ledipasvir-Sofosbuvir for Treating Chronic Hepatitis C: A NICE Single Technology Appraisal-An Evidence Review Group Perspective. Pharmacoeconomics 2016, 34, 741–750. [Google Scholar] [CrossRef] [PubMed]
- Alavi, M.; Raffa, J.D.; Deans, G.D.; Lai, C.; Krajden, M.; Dore, G.J.; Tyndall, M.W.; Grebely, J. Continued low uptake of treatment for hepatitis C virus infection in a large community-based cohort of inner city residents. Liver Int. 2014, 34, 1198–1206. [Google Scholar] [CrossRef] [PubMed]
- Iversen, J.; Grebely, J.; Topp, L.; Wand, H.; Dore, G.; Maher, L. Uptake of hepatitis C treatment among people who inject drugs attending Needle and Syringe Programs in Australia, 1999-2011. J. Viral Hepat. 2014, 21, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Grebely, J.; Robaeys, G.; Bruggmann, P.; Aghemo, A.; Backmund, M.; Bruneau, J.; Byrne, J.; Dalgard, O.; Feld, J.J.; Hellard, M.; et al. Recommendations for the management of hepatitis C virus infection among people who inject drugs. Int. J. Drug Policy 2015, 26, 1028–1038. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.H.; Genberg, B.L.; Astemborski, J.; Kavasery, R.; Kirk, G.D.; Vlahov, D.; Strathdee, S.A.; Thomas, D.L. Limited uptake of hepatitis C treatment among injection drug users. J. Community Health 2008, 33, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Grebely, J.; Dore, G.J. Can hepatitis C virus infection be eradicated in people who inject drugs? Antiviral Res. 2014, 104, 62–72. [Google Scholar] [CrossRef] [PubMed]
- Papatheodoridis, G.V.; Lampertico, P.; Manolakopoulos, S.; Lok, A. Incidence of hepatocellular carcinoma in chronic hepatitis B patients receiving nucleos (t) ide therapy: A systematic review. J. Hepatol. 2010, 53, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Liaw, Y.F.; Leung, N.; Kao, J.H.; Piratvisuth, T.; Gane, E.; Han, K.H.; Guan, R.; Lau, G.K.; Locarnini, S. Asian-Pacific consensus statement on the management of chronic hepatitis B: A 2008 update. Hepatol. Int. 2008, 2, 263–283. [Google Scholar] [CrossRef] [PubMed]
- Lingala, S.; Ghany, M.G. Natural History of Hepatitis C. Gastroenterol. Clin. 2015, 44, 717–734. [Google Scholar] [CrossRef] [PubMed]
- Are, C.; Meyer, B.; Stack, A.; Ahmad, H.; Smith, L.; Qian, B.; Song, T.; Chowdhury, S. Global trends in the burden of liver cancer. J. Surg. Oncol. 2017, 115, 591–602. [Google Scholar] [CrossRef] [PubMed]
- Pateria, P.; de Boer, B.; MacQuillan, G. Liver abnormalities in drug and substance abusers. Best Pract. Res. Clin. Gastroenterol. 2013, 27, 577–596. [Google Scholar] [CrossRef] [PubMed]
- Vitcheva, V. Cocaine toxicity and hepatic oxidative stress. Curr. Med. Chem. 2012, 19, 5677–5682. [Google Scholar] [CrossRef] [PubMed]
- Vandelli, C.; Piaggi, V.; Battilani, R.; Cariani, E.; Sirotti, M.A. Relationship between HBV markers and heroin as a cause of liver injury in drug addicts. Drug Alcohol Depend. 1984, 14, 129–133. [Google Scholar] [CrossRef]
- Winters, K.C.; Lee, C.Y. Likelihood of developing an alcohol and cannabis use disorder during youth: Association with recent use and age. Drug Alcohol Depend. 2008, 92, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Moss, H.B.; Chen, C.M.; Yi, H.Y. Early adolescent patterns of alcohol, cigarettes, and marijuana polysubstance use and young adult substance use outcomes in a nationally representative sample. Drug Alcohol Depend. 2014, 136, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Degenhardt, L.; Stockings, E.; Patton, G.; Hall, W.D.; Lynskey, M. The increasing global health priority of substance use in young people. Lancet Psychiatry 2016, 3, 251–264. [Google Scholar] [CrossRef]
- Maher, L.; Li, J.; Jalaludin, B.; Chant, K.G.; Kaldor, J.M. High hepatitis C incidence in new injecting drug users: A policy failure? J. Public Health 2007, 31, 30–35. [Google Scholar] [CrossRef]
- Hahn, J.A.; Page-Shafer, K.; Lum, P.J.; Bourgois, P.; Stein, E.; Evans, J.L.; Busch, M.P.; Tobler, L.H.; Phelps, B.; Moss, A.R. Hepatitis C virus seroconversion among young injection drug users: Relationships and risks. J. Infect. Dis. 2002, 186, 1558–1564. [Google Scholar] [CrossRef] [PubMed]
- Leaning, J.; Guha-Sapir, D. Natural disasters, armed conflict, and public health. J. Med. 2013, 369, 1836–1842. [Google Scholar] [CrossRef] [PubMed]
- Al, G.N.; Dresden, E.; Keeney, G.B.; Warren, N. Status of women and infants in complex humanitarian emergencies. J. Midwifery Womens Health 2004, 49, 7–13. [Google Scholar] [CrossRef]
- Maher, L. Hepatitis B vaccination and injecting drug use: Narrowing the efficacy-effectiveness gap. Int. J. Drug Policy 2008, 19, 425–428. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidance on Prevention of Viral Hepatitis B and C among People Who Inject Drugs; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- MacArthur, G.J.; van Velzen, E.; Palmateer, N.; Kimber, J.; Pharris, A.; Hope, V.; Taylor, A.; Roy, K.; Aspinall, E.; Goldberg, D.; et al. Interventions to prevent HIV and Hepatitis C in people who inject drugs: A review of reviews to assess evidence of effectiveness. Int. J. Drug Policy 2014, 25, 34–52. [Google Scholar] [CrossRef] [PubMed]
- Brettle, R.P. Infection and injection drug use. J. Infect. 1992, 25, 121–131. [Google Scholar] [CrossRef]
- Des Jarlais, D.C.; Friedman, S.R.; Choopanya, K.; Vanichseni, S.; Ward, T.P. International epidemiology of HIV and AIDS among injecting drug users. Aids 1992, 6, 1053–1068. [Google Scholar] [CrossRef] [PubMed]
- Bucardo, J.; Brouwer, K.C.; Magis-Rodriguez, C.; Ramos, R.; Fraga, M.; Perez, S.G.; Patterson, T.L.; Strathdee, S.A. Historical trends in the production and consumption of illicit drugs in Mexico: Implications for the prevention of blood borne infections. Drug Alcohol Depend. 2005, 79, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Hajarizadeh, B.; Grebely, J.; Dore, G.J. Epidemiology and natural history of HCV infection. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 553–562. [Google Scholar] [CrossRef] [PubMed]
- Mathers, B.M.; Degenhardt, L.; Ali, H.; Wiessing, L.; Hickman, M.; Mattick, R.P.; Myers, B.; Ambekar, A.; Strathdee, S.A. HIV prevention, treatment, and care services for people who inject drugs: A systematic review of global, regional, and national coverage. Lancet 2010, 375, 1014–1028. [Google Scholar] [CrossRef]
- Pierce, R.D.; Hegle, J.; Sabin, K.; Agustian, E.; Johnston, L.G.; Mills, S.; Todd, C.S. Strategic information is everyone’s business: Perspectives from an international stakeholder meeting to enhance strategic information data along the HIV Cascade for people who inject drugs. Harm Reduct. J. 2015, 12, 41. [Google Scholar] [CrossRef] [PubMed]
- Platt, L.; Minozzi, S.; Reed, J.; Vickerman, P.; Hagan, H.; French, C.; Jordan, A.; Degenhardt, L.; Hope, V.; Hutchinson, S.; et al. Needle syringe programmes and opioid substitution therapy for preventing hepatitis C transmission in people who inject drugs. Cochrane Database Syst. Rev. 2017, 9, D12021. [Google Scholar] [CrossRef] [PubMed]
- Feeney, E.R.; Chung, R.T. Antiviral treatment of hepatitis C. BMJ 2014, 348, g3308. [Google Scholar] [CrossRef] [PubMed]
- Kohli, A.; Shaffer, A.; Sherman, A.; Kottilil, S. Treatment of hepatitis C: A systematic review. JAMA 2014, 312, 631–640. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, R.; Burns, A.; Rodden, D.; Chang, F.; Chaum, M.; Garcia, N.; Bollipalli, N.; Niemz, A. Diagnosis and Management of Hepatitis C Virus Infection. J. Lab. Autom. 2015, 20, 519–538. [Google Scholar] [CrossRef] [PubMed]
- McGowan, C.E.; Fried, M.W. Barriers to hepatitis C treatment. Liver Int. 2012, 32, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Rizzetto, M. Hepatitis D: Thirty years after. J. Hepatol. 2009, 50, 1043–1050. [Google Scholar] [CrossRef] [PubMed]
- Farci, P. Delta hepatitis: An update. J. Hepatol. 2003, 39, S212–S219. [Google Scholar] [CrossRef]
- Hadler, S.C.; De Monzon, M.; Ponzetto, A.; Anzola, E.; Rivero, D.; Mondolfi, A.; Bracho, A.; Francis, D.P.; Gerber, M.A.; Thung, S.; et al. Delta virus infection and severe hepatitis. An epidemic in the Yucpa Indians of Venezuela. Ann. Int. Med. 1984, 100, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Govindarajan, S.; Chin, K.P.; Redeker, A.G.; Peters, R.L. Fulminant B viral hepatitis: Role of delta agent. Gastroenterology 1984, 86, 1417–1420. [Google Scholar] [PubMed]
- Saracco, G.; Rosina, F.; Brunetto, M.R.; Amoroso, P.; Caredda, F.; Farci, P.; Piantino, P.; Bonino, F.; Rizzetto, M. Rapidly progressive HBsAg-positive hepatitis in Italy. The role of hepatitis delta virus infection. J. Hepatol. 1987, 5, 274–281. [Google Scholar] [CrossRef]
- Fattovich, G.; Boscaro, S.; Noventa, F.; Pornaro, E.; Stenico, D.; Alberti, A.; Ruol, A.; Realdi, G. Influence of hepatitis delta virus infection on progression to cirrhosis in chronic hepatitis type B. J. Infect. Dis. 1987, 155, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Romeo, R.; Del, N.E.; Rumi, M.; Russo, A.; Sangiovanni, A.; de Franchis, R.; Ronchi, G.; Colombo, M. A 28-year study of the course of hepatitis Delta infection: A risk factor for cirrhosis and hepatocellular carcinoma. Gastroenterology 2009, 136, 1629–1638. [Google Scholar] [CrossRef] [PubMed]
- Hughes, S.A.; Wedemeyer, H.; Harrison, P.M. Hepatitis delta virus. Lancet 2011, 378, 73–85. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Liver Cancer Mortality-IDU | Cirrhosis Mortality-IDU | ||||
|---|---|---|---|---|---|---|
| Moran’s I | Z Score | p | Moran’s I | Z Score | p | |
| 1990 | 0.10 | 2.21 | 0.027 | 0.55 | 8.96 | <0.001 |
| 1995 | 0.11 | 2.40 | 0.016 | 0.60 | 9.79 | <0.001 |
| 2000 | 0.10 | 2.30 | 0.021 | 0.66 | 10.66 | <0.001 |
| 2005 | 0.07 | 1.93 | 0.054 | 0.66 | 10.59 | <0.001 |
| 2010 | 0.06 | 1.80 | 0.072 | 0.63 | 10.20 | <0.001 |
| 2016 | 0.06 | 1.93 | 0.054 | 0.64 | 10.26 | <0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.; Zhang, Y.; Luo, L.; Meng, R.; Yu, C. Global Mortality Burden of Cirrhosis and Liver Cancer Attributable to Injection Drug Use, 1990–2016: An Age-Period-Cohort and Spatial Autocorrelation Analysis. Int. J. Environ. Res. Public Health 2018, 15, 170. https://doi.org/10.3390/ijerph15010170
Yang J, Zhang Y, Luo L, Meng R, Yu C. Global Mortality Burden of Cirrhosis and Liver Cancer Attributable to Injection Drug Use, 1990–2016: An Age-Period-Cohort and Spatial Autocorrelation Analysis. International Journal of Environmental Research and Public Health. 2018; 15(1):170. https://doi.org/10.3390/ijerph15010170
Chicago/Turabian StyleYang, Jin, Yunquan Zhang, Lisha Luo, Runtang Meng, and Chuanhua Yu. 2018. "Global Mortality Burden of Cirrhosis and Liver Cancer Attributable to Injection Drug Use, 1990–2016: An Age-Period-Cohort and Spatial Autocorrelation Analysis" International Journal of Environmental Research and Public Health 15, no. 1: 170. https://doi.org/10.3390/ijerph15010170