Addressing Suicide Risk According to Different Healthcare Professionals in Spain: A Qualitative Study

 , , and
, , and 
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Inclusion Criteria
- Healthcare professional belonging to one of the four groups selected for the study: psychiatrists, psychologists, primary care physicians, and emergency medicine physicians.
- Professional experience in the area of suicide.
- Age between 18 and 65 years.
2.3. Recruitment
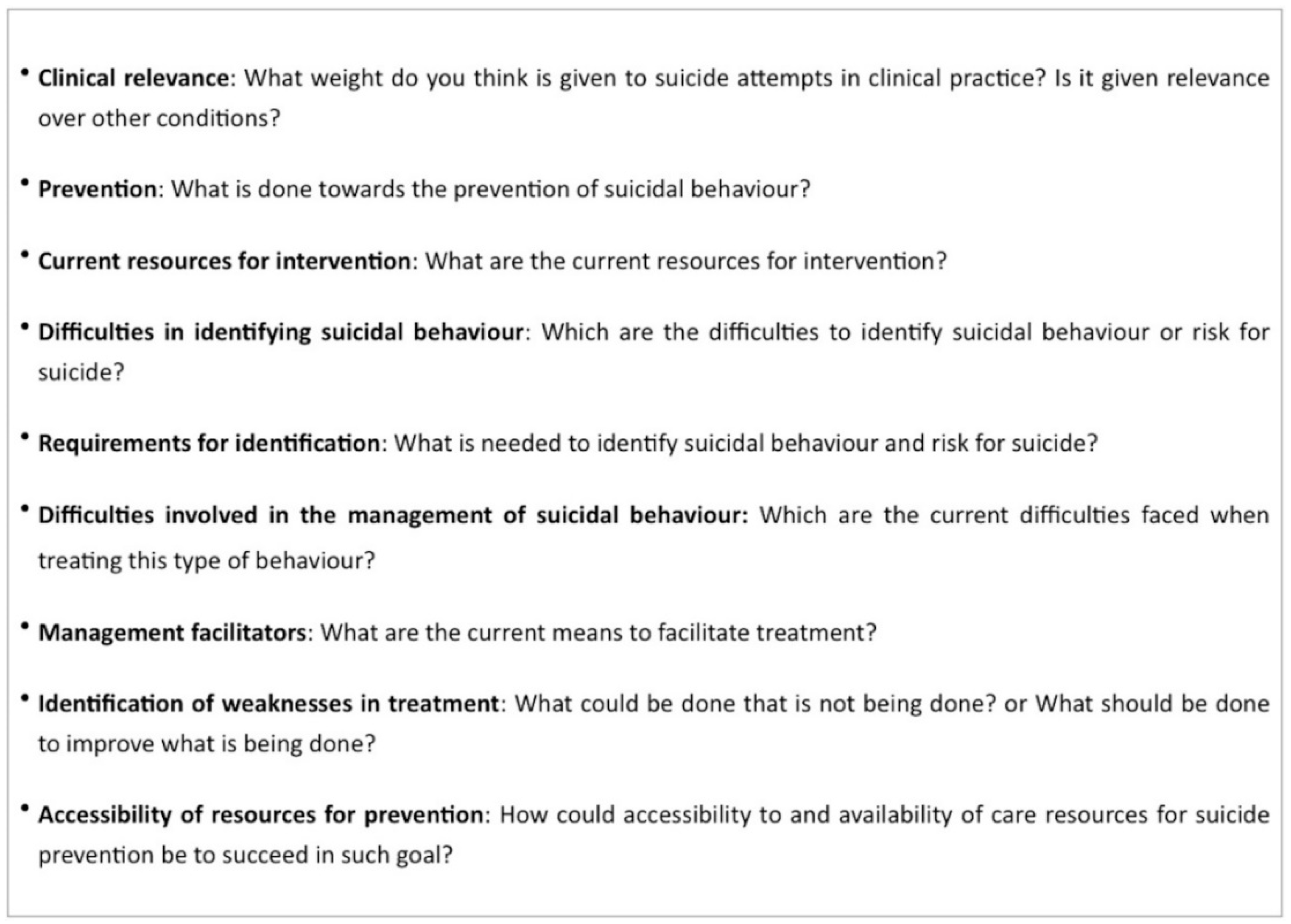
2.4. Procedure
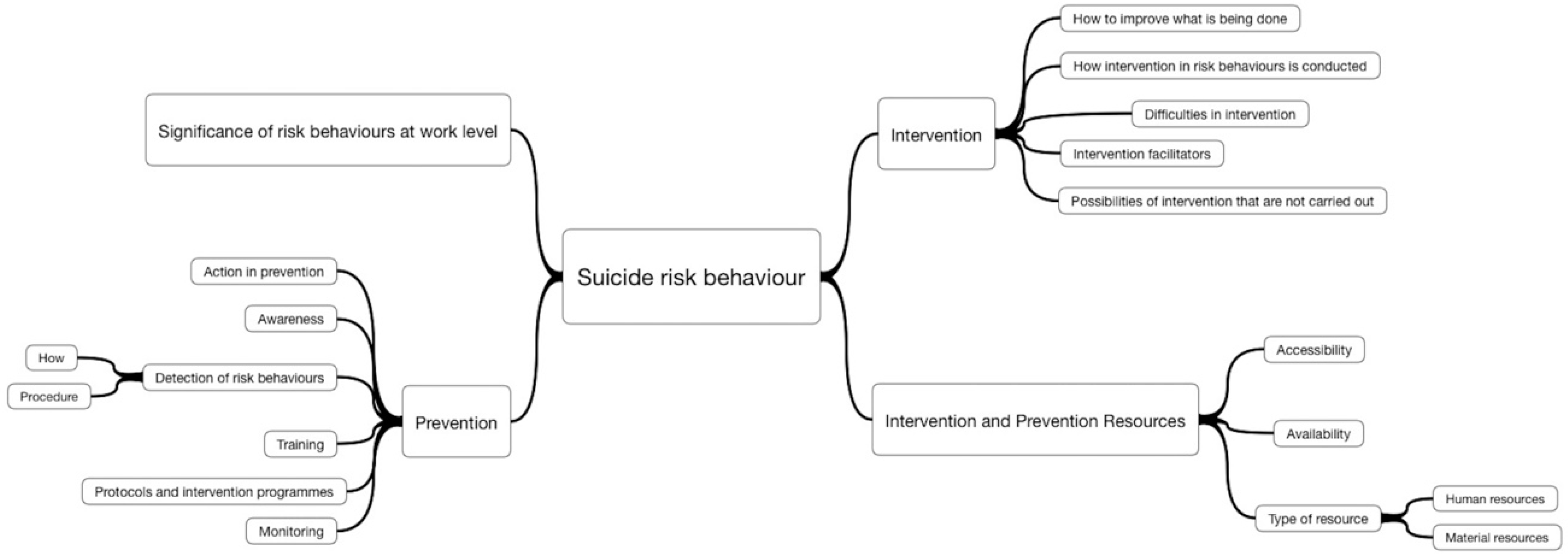
2.5. Analysis
3. Results
3.1. Most Representative Words
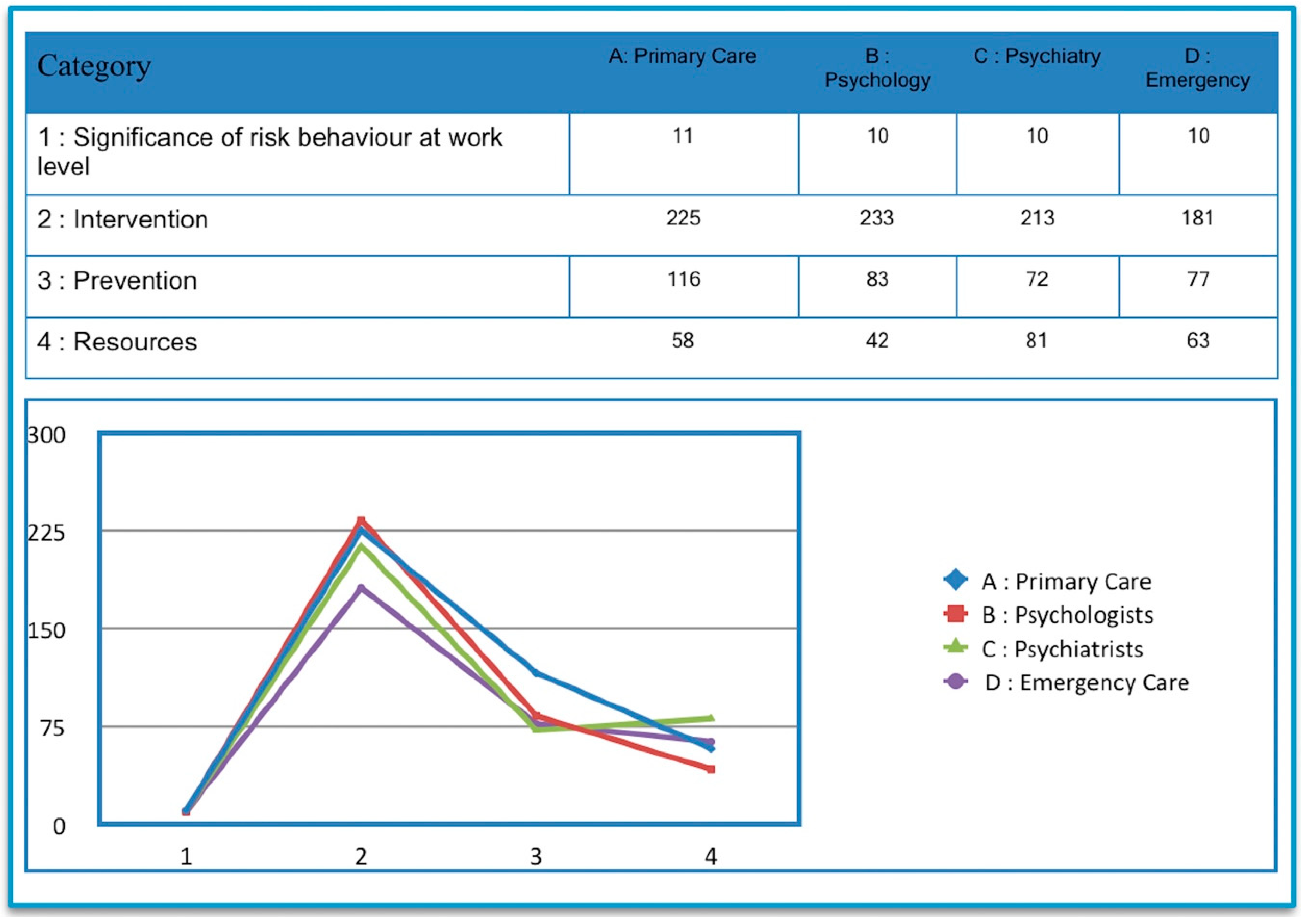
3.2. Category Profile
3.2.1. Emergency Physicians
3.2.2. Psychiatrists
3.2.3. Psychologists
3.2.4. Primary Care Physicians
4. Discussion
5. Conclusions
5.1. Primary Care Physicians
- Need for more time to address patients at risk for suicide.
- Easier access to and communication with the mental health network.
- Availability of immediate or within 24 h referral.
- Lack of training in the management of suicidal behavior.
5.2. Emergency Care Physicians
- Lack of awareness of their role in the detection of risk for suicide in patients who seek attention at emergency care facilities for reasons of general somatic issues.
- They focus their response on handling the risk for death to later refer the patient to psychiatric services.
5.3. Mental Health Care Physicians
- High demand, especially in self-harming behaviors that require a specific approach.
- Give more priority to psychotherapeutic interventions and improve the availability and role of clinical psychologists in the management of suicidal behavior.
- Need for the implementation of specific programs to address suicidal behavior: group therapy, etc.
- Accessibility should be an important part of intervention.
- Importance of the role of a community support network, especially involving home care by nursing professionals.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Preventing Suicide: A Global Imperative; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Kovess-Masfety, V.; Boyd, A.; Haro, J.M.; Bruffaerts, R.; Villagut, G.; Lepine, J.P.; Gasquet, I.; Alonso, J. High and low suicidality in Europe: A fine-grained comparison of France and Spain within the ESEMeD surveys. J. Affect. Disord. 2011, 133, 247–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silverman, M.M.; Berman, A.L.; Sanddal, N.D.; O’Carroll, P.W.; Joiner, T.E. Rebuilding the tower of Babel: A revised nomenclature for the study of suicide and suicidal behaviors. Part 1: Background, rationale, and methodology. Suicide Life Threat. Behav. 2007, 37, 248–263. [Google Scholar] [CrossRef] [PubMed]
- Schaffer, A.; Sinyor, M.; Kurdyak, P.; Vigod, S.; Sareen, J.; Reis, C.; Green, D.; Bolton, J.; Rhodes, A.; Grigoriadis, S.; et al. Population-based analysis of health care contacts among suicide decedents: Identifying opportunities for more targeted suicide prevention strategies. World Psychiatry 2016, 15, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Steeg, S.; Haigh, M.; Webb, R.T.; Kapur, N.; Awenat, Y.; Gooding, P.; Pratt, D.; Cooper, J. The exacerbating influence of hopelessness on other known risk factors for repeat self-harm and suicide. J. Affect. Disord. 2016, 190, 522–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neeleman, J. Beyond risk theory: Suicidal behavior in its social and epidemiological context. Crisis 2002, 23, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, J.D.; Franklin, J.C.; Fox, K.R.; Bentley, K.H.; Kleiman, E.M.; Chang, B.P.; Nock, M.K. Self-injurious thoughts and behaviors as risk factors for future suicide ideation, attempts, and death: A meta-analysis of longitudinal studies. Psychol. Med. 2015, 46, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Borges, G.; Nock, M.K.; Haro Abad, J.M.; Hwang, I.; Sampson, N.A.; Alonso, J.; Andrade, L.H.; Angermeyer, M.C.; Beautrais, A.; Bromet, E.; et al. Twelve-month prevalence of and risk factors for suicide attempts in the World Health Organization World Mental Health Surveys. J. Clin. Psychiatry 2010, 71, 1617–1628. [Google Scholar] [CrossRef] [PubMed]
- Foster, T.; Gillespie, K.; McClelland, R. Mental disorders and suicide in Northern Ireland. Br. J. Psychiatry 1997, 170, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Oldham, J.M. Borderline personality disorder and suicidality. Am. J. Psychiatry 2006, 163, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Osborn, D.; Levy, G.; Nazareth, I.; King, M. Suicide and severe mental illnesses. Cohort study within the UK general practice research database. Schizophr. Res. 2008, 99, 134–138. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Borges, G.; Walters, E.E. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Arch. Gen. Psychiatry 1999, 56, 617–626. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K.; Houston, K.; Haw, C.; Townsend, E.; Harriss, L. Comorbidity of axis I and axis II disorders in patients who attempted suicide. Am. J. Psychiatry 2003, 160, 1494–1500. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.K.; Kessler, R.C. Prevalence of and risk factors for suicide attempts versus suicide gestures: Analysis of the National Comorbidity Survey. J. Abnorm. Psychol. 2006, 115, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Neeleman, J.; de Graaf, R.; Vollebergh, W. The suicidal process; prospective comparison between early and later stages. J. Affect. Disord. 2004, 82, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Runeson, B.S.; Beskow, J.; Waern, M. The suicidal process in suicides among young people. Acta Psychiatr. Scand. 1996, 93, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K.; Casanas, I.C.C.; Haw, C.; Saunders, K. Risk factors for suicide in individuals with depression: A systematic review. J. Affect. Disord. 2013, 147, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Coryell, W.; Kriener, A.; Butcher, B.; Nurnberger, J.; McMahon, F.; Berrettini, W.; Fiedorowicz, J. Risk factors for suicide in bipolar I disorder in two prospectively studied cohorts. J. Affect. Disord. 2016, 190, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Schaffer, A.; Isometsa, E.T.; Azorin, J.M.; Cassidy, F.; Goldstein, T.; Rihmer, Z.; Sinyor, M.; Tondo, L.; Moreno, D.H.; Turecki, G.; et al. A review of factors associated with greater likelihood of suicide attempts and suicide deaths in bipolar disorder: Part II of a report of the International Society for Bipolar Disorders Task Force on Suicide in Bipolar Disorder. Aust. N. Z. J. Psychiatry 2015, 49, 1006–1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dransart, D.A.; Gutjahr, E.; Gulfi, A.; Didisheim, N.K.; Seguin, M. Patient suicide in institutions: Emotional responses and traumatic impact on Swiss mental health professionals. Death Stud. 2014, 38, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Gulfi, A.; Castelli Dransart, D.A.; Heeb, J.L.; Gutjahr, E. The Impact of Patient Suicide on the Professional Practice of Swiss Psychiatrists and Psychologists. Acad. Psychiatry 2016, 40, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Castelli Dransart, D.A.; Heeb, J.L.; Gulfi, A.; Gutjahr, E.M. Stress reactions after a patient suicide and their relations to the profile of mental health professionals. BMC Psychiatry 2015, 15, 265. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.R.; Silva, C.; Covington, D.W.; Joiner, T.E. An assessment of suicide-related knowledge and skills among health professionals. Health Psychol. 2014, 33, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Saunders, K.E.; Hawton, K.; Fortune, S.; Farrell, S. Attitudes and knowledge of clinical staff regarding people who self-harm: A systematic review. J. Affect. Disord. 2012, 139, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Gale, T.M.; Hawley, C.J.; Butler, J.; Morton, A.; Singhal, A. Perception of Suicide Risk in Mental Health Professionals. PLoS ONE 2016, 11, e0149791. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, G.; Forghieri, M.; Ferrari, S.; Pingani, L.; Coppola, P.; Colombini, N.; Rigatelli, M.; Neimeyer, R.A. Suicide intervention skills in health professionals: A multidisciplinary comparison. Arch. Suicide Res. 2008, 12, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Mirick, R.; McCauley, J.; Bridger, J.; Berkowitz, L. Continuing Education on Suicide Assessment and Crisis Intervention: What Can We Learn About the Needs of Mental Health Professionals in Community Practice? Commun. Ment. Health J. 2016, 52, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Gaffney, P.; Russell, V.; Collins, K.; Bergin, A.; Halligan, P.; Carey, C.; Coyle, S. Impact of patient suicide on front-line staff in Ireland. Death Stud. 2009, 33, 639–656. [Google Scholar] [CrossRef] [PubMed]
- Rothes, I.A.; Henriques, M.R.; Leal, J.B.; Lemos, M.S. Facing a patient who seeks help after a suicide attempt: The difficulties of health professionals. Crisis 2014, 35, 110–122. [Google Scholar] [CrossRef] [PubMed]
- Hitosugi, M.; Nagai, T.; Tokudome, S. A voluntary effort to save the youth suicide via the Internet in Japan. Int. J. Nurs. Stud. 2007, 44, 157. [Google Scholar] [CrossRef] [PubMed]
- De Leo, D.; Draper, B.M.; Snowdon, J.; Kolves, K. Contacts with health professionals before suicide: Missed opportunities for prevention? Compr. Psychiatry 2013, 54, 1117–1123. [Google Scholar] [CrossRef] [PubMed]
- Fedyszyn, I.E.; Erlangsen, A.; Hjorthoj, C.; Madsen, T.; Nordentoft, M. Repeated suicide attempts and suicide among individuals with a first emergency department contact for attempted suicide: A prospective, nationwide, Danish register-based study. J. Clin. Psychiatry 2016, 77, 832–840. [Google Scholar] [CrossRef] [PubMed]
- Fhaili, M.N.; Flynn, N.; Dowling, S. Experiences of suicide bereavement: A qualitative study exploring the role of the GP. Br. J. Gen. Pract. 2016, 66, e92–e98. [Google Scholar] [CrossRef] [PubMed]
- Younes, N.; Melchior, M.; Turbelin, C.; Blanchon, T.; Hanslik, T.; Chee, C.C. Attempted and completed suicide in primary care: Not what we expected? J. Affect. Disord. 2015, 170, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Petrik, M.L.; Gutierrez, P.M.; Berlin, J.S.; Saunders, S.M. Barriers and facilitators of suicide risk assessment in emergency departments: A qualitative study of provider perspectives. Gen. Hosp. Psychiatry 2015, 37, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Egan, R.; Sarma, K.M.; O’Neill, M. Factors influencing perceived effectiveness in dealing with self-harming patients in a sample of emergency department staff. J. Emerg. Med. 2012, 43, 1084–1090. [Google Scholar] [CrossRef] [PubMed]
- Simon, R.I. Behavioral risk assessment of the guarded suicidal patient. Suicide Life Threat. Behav. 2008, 38, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Geekie, J.; Read, J.; Renton, J.; Harrop, C. Do English mental health services know whether they followed N.I.C.E. guidelines with patients who killed themselves? Psychol. Psychother. 2017, 90, 797–800. [Google Scholar] [CrossRef] [PubMed]
- Roush, J.F.; Brown, S.L.; Jahn, D.R.; Mitchell, S.M.; Taylor, N.J.; Quinnett, P.; Ries, R. Mental Health Professionals’ Suicide Risk Assessment and Management Practices. Crisis 2018, 39, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Goldney, R.D. Suicide prevention: The role of the psychiatrist. Aust. N. Z. J. Psychiatry 2016, 50, 95–96. [Google Scholar] [CrossRef] [PubMed]
- Baca-Garcia, E.; Diaz-Sastre, C.; Resa, E.G.; Blasco, H.; Conesa, D.B.; Saiz-Ruiz, J.; de Leon, J. Variables associated with hospitalization decisions by emergency psychiatrists after a patient’s suicide attempt. Psychiatr. Serv. 2004, 55, 792–797. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, P.; Helgesson, G.; Titelman, D.; Sjostrand, M.; Juth, N. Skepticism towards the Swedish vision zero for suicide: Interviews with 12 psychiatrists. BMC Med. Ethics 2018, 19, 26. [Google Scholar] [CrossRef] [PubMed]
- Scocco, P.; Toffol, E.; Pilotto, E.; Riccardo, P.; Pavan, L. How the psychiatrists of a mental health department managed their patients before an attempted suicide. Psychiatry Clin. Neurosci. 2009, 63, 706–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finlayson, M.; Simmonds, J. Workplace Responses and Psychologists’ Needs Following Client Suicide. Omega (Westport) 2017. [Google Scholar] [CrossRef] [PubMed]
- Hagen, J.; Hjelmeland, H.; Knizek, B.L. Connecting with suicidal patients in psychiatric wards: Therapist challenges. Death Stud. 2017, 41, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Hepp, U.; Wittmann, L.; Schnyder, U.; Michel, K. Psychological and psychosocial interventions after attempted suicide: An overview of treatment studies. Crisis 2004, 25, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Calati, R.; Courtet, P. Is psychotherapy effective for reducing suicide attempt and non-suicidal self-injury rates? Meta-analysis and meta-regression of literature data. J. Psychiatr. Res. 2016, 79, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Forkmann, T.; Brakemeier, E.L.; Teismann, T.; Schramm, E.; Michalak, J. The Effects of Mindfulness-Based Cognitive Therapy and Cognitive Behavioral Analysis System of Psychotherapy added to Treatment as Usual on suicidal ideation in chronic depression: Results of a randomized-clinical trial. J. Affect. Disord. 2016, 200, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Groth, T.; Boccio, D.E. Psychologists’ Willingness to Provide Services to Individuals at Risk of Suicide. Suicide Life Threat. Behav. 2018. [Google Scholar] [CrossRef] [PubMed]
- Munoz-Sanchez, J.L.; Delgado, C.; Sanchez-Prada, A.; Perez-Lopez, M.; Franco-Martin, M.A. Use of New Technologies in the Prevention of Suicide in Europe: An Exploratory Study. JMIR Ment. Health 2017, 4, e23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munoz-Sanchez, J.L.; Delgado, C.; Parra-Vidales, E.; Franco-Martin, M. Facilitating Factors and Barriers to the Use of Emerging Technologies for Suicide Prevention in Europe: Multicountry Exploratory Study. JMIR Ment. Health 2018, 5, e7. [Google Scholar] [CrossRef] [PubMed]
- Whitley, R.; Crawford, M. Qualitative research in psychiatry. Can. J. Psychiatry 2005, 50, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Whitley, R. Introducing psychiatrists to qualitative research: A guide for instructors. Acad. Psychiatry 2009, 33, 252–255. [Google Scholar] [CrossRef] [PubMed]
- Fairman, N.; Thomas, L.P.; Whitmore, S.; Meier, E.A.; Irwin, S.A. What did I miss? A qualitative assessment of the impact of patient suicide on hospice clinical staff. J. Palliat. Med. 2014, 17, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Michail, M.; Tait, L. Exploring general practitioners’ views and experiences on suicide risk assessment and management of young people in primary care: A qualitative study in the UK. BMJ Open 2016, 6, e009654. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Elo, S.; Kyngas, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Scheerder, G.; Reynders, A.; Andriessen, K.; Van Audenhove, C. Suicide intervention skills and related factors in community and health professionals. Suicide Life Threat. Behav. 2010, 40, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Rothes, I.A.; Henriques, M.R. Health Professionals’ Explanations of Suicidal Behaviour: Effects of Professional Group, Theoretical Intervention Model, and Patient Suicide Experience. Omega (Westport) 2017, 76, 141–168. [Google Scholar] [CrossRef] [PubMed]
- Stene-Larsen, K.; Reneflot, A. Contact with primary and mental health care prior to suicide: A systematic review of the literature from 2000 to 2017. Scand. J. Public Health 2017. [Google Scholar] [CrossRef] [PubMed]
- Sudak, D.; Roy, A.; Sudak, H.; Lipschitz, A.; Maltsberger, J.; Hendin, H. Deficiencies in suicide training in primary care specialties: A survey of training directors. Acad. Psychiatry 2007, 31, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Vannoy, S.D.; Tai-Seale, M.; Duberstein, P.; Eaton, L.J.; Cook, M.A. Now what should I do? Primary care physicians’ responses to older adults expressing thoughts of suicide. J. Gen. Intern. Med. 2011, 26, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Bocquier, A.; Pambrun, E.; Dumesnil, H.; Villani, P.; Verdoux, H.; Verger, P. Physicians’ characteristics associated with exploring suicide risk among patients with depression: A French panel survey of general practitioners. PLoS ONE 2013, 8, e80797. [Google Scholar] [CrossRef] [PubMed]
- Saini, P.; Chantler, K.; Kapur, N. General practitioners’ perspectives on primary care consultations for suicidal patients. Health Soc. Care Commun. 2016, 24, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Leavey, G.; Mallon, S.; Rondon-Sulbaran, J.; Galway, K.; Rosato, M.; Hughes, L. The failure of suicide prevention in primary care: Family and GP perspectives—A qualitative study. BMC Psychiatry 2017, 17, 369. [Google Scholar] [CrossRef] [PubMed]
- Suokas, J.; Suominen, K.; Lonnqvist, J. The attitudes of emergency staff toward attempted suicide patients: A comparative study before and after establishment of a psychiatric consultation service. Crisis 2009, 30, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Giacchero Vedana, K.G.; Magrini, D.F.; Zanetti, A.C.G.; Miasso, A.I.; Borges, T.L.; Dos Santos, M.A. Attitudes towards suicidal behaviour and associated factors among nursing professionals: A quantitative study. J. Psychiatr. Ment. Health Nurs. 2017, 24, 651–659. [Google Scholar] [CrossRef] [PubMed]
- McCabe, R.; Sterno, I.; Priebe, S.; Barnes, R.; Byng, R. How do healthcare professionals interview patients to assess suicide risk? BMC Psychiatry 2017, 17, 122. [Google Scholar] [CrossRef] [PubMed]
- Reuveni, I.; Pelov, I.; Reuveni, H.; Bonne, O.; Canetti, L. Cross-sectional survey on defensive practices and defensive behaviours among Israeli psychiatrists. BMJ Open 2017, 7, e014153. [Google Scholar] [CrossRef] [PubMed]
- Jones, H.; Cipriani, A. Improving access to treatment for mental health problems as a major component of suicide prevention strategy. Aust. N. Z. J. Psychiatry 2016, 50, 176–178. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Lee, M.S.; Hong, J.Y. Determinants of Mental Health Care Utilization in a Suicide High-risk Group with Suicidal Ideation. J. Prev. Med. Public Health 2016, 49, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Roelands, M.; Deschepper, R.; Bilsen, J. Psychiatric Consultation and Referral of Persons Who Have Attempted Suicide. Crisis 2017, 38, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Pirkola, S.; Sund, R.; Sailas, E.; Wahlbeck, K. Community mental-health services and suicide rate in Finland: A nationwide small-area analysis. Lancet 2009, 373, 147–153. [Google Scholar] [CrossRef]
- Miklowitz, D.J.; Taylor, D.O. Family-focused treatment of the suicidal bipolar patient. Bipolar Disord. 2006, 8, 640–651. [Google Scholar] [CrossRef] [PubMed]
- Joe, S.; Bryant, H. Evidence-Based Suicide Prevention Screening in Schools. Child. Sch. 2007, 29, 219–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawton, K.; Witt, K.G.; Salisbury, T.L.T.; Arensman, E.; Gunnell, D.; Hazell, P.; Townsend, E.; van Heeringen, K. Psychosocial interventions following self-harm in adults: A systematic review and meta-analysis. Lancet Psychiatry 2016, 3, 740–750. [Google Scholar] [CrossRef]
- Meerwijk, E.L.; Parekh, A.; Oquendo, M.A.; Allen, I.E.; Franck, L.S.; Lee, K.A. Direct versus indirect psychosocial and behavioural interventions to prevent suicide and suicide attempts: A systematic review and meta-analysis. Lancet Psychiatry 2016, 3, 544–554. [Google Scholar] [CrossRef]
- Cox, G.; Hetrick, S. Psychosocial interventions for self-harm, suicidal ideation and suicide attempt in children and young people: What? How? Who? and Where? Evid. Based Ment. Health 2017, 20, 35–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinstein, S.M.; Cruz, R.A.; Isaia, A.R.; Peters, A.T.; West, A.E. Child- and Family-Focused Cognitive Behavioral Therapy for Pediatric Bipolar Disorder: Applications for Suicide Prevention. Suicide Life Threat. Behav. 2017. [Google Scholar] [CrossRef] [PubMed]
- Gilat, I.; Tobin, Y.; Shahar, G. Offering support to suicidal individuals in an online support group. Arch. Suicide Res. 2011, 15, 195–206. [Google Scholar] [CrossRef] [PubMed]



© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Sánchez, J.-L.; Sánchez-Gómez, M.C.; Martín-Cilleros, M.V.; Parra-Vidales, E.; De Leo, D.; Franco-Martín, M.A. Addressing Suicide Risk According to Different Healthcare Professionals in Spain: A Qualitative Study. Int. J. Environ. Res. Public Health 2018, 15, 2117. https://doi.org/10.3390/ijerph15102117
Muñoz-Sánchez J-L, Sánchez-Gómez MC, Martín-Cilleros MV, Parra-Vidales E, De Leo D, Franco-Martín MA. Addressing Suicide Risk According to Different Healthcare Professionals in Spain: A Qualitative Study. International Journal of Environmental Research and Public Health. 2018; 15(10):2117. https://doi.org/10.3390/ijerph15102117
Chicago/Turabian StyleMuñoz-Sánchez, Juan-Luis, María Cruz Sánchez-Gómez, María Victoria Martín-Cilleros, Esther Parra-Vidales, Diego De Leo, and Manuel A. Franco-Martín. 2018. "Addressing Suicide Risk According to Different Healthcare Professionals in Spain: A Qualitative Study" International Journal of Environmental Research and Public Health 15, no. 10: 2117. https://doi.org/10.3390/ijerph15102117