Economic Conditions May Contribute to Increased Violence toward Children: A Nationwide Population-Based Analysis of Pediatric Injuries in Taiwanese Emergency Departments

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database
2.2. Study Population
2.3. Statistical Analysis
3. Results
3.1. Incidences of Accidental Injuries
3.2. Temporal Trend of Accidental Injuries
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Jeng, M.J.; Lee, Y.S.; Tsao, P.C.; Yang, C.-F.; Luo, Y.-C.; Soong, W.-J. A 10-year population-based nationwide descriptive analysis of pediatric emergency care. BMC Pediatr. 2014, 14, 100. [Google Scholar] [CrossRef] [PubMed]
- Alonge, O.; Khan, U.R.; Hyder, A.A. Our shrinking globe: Implications for child unintentional injuries. Pediatr. Clin. N. Am. 2016, 63, 167–181. [Google Scholar] [CrossRef] [PubMed]
- Armon, K.; Stephenson, T.; Gabriel, V.; MacFaul, R.; Eccleston, P.; Werneke, U.; Smith, S. Determining the common medical presenting problems to an accident and emergency department. Arch. Dis. Child. 2001, 84, 390–392. [Google Scholar] [CrossRef] [PubMed]
- Younesian, S.; Mahfoozpour, S.; Ghaffari Shad, E.; Kariman, H.; Hatamabadi, H.R. Unintentional home injury prevention in preschool children; a study of contributing factors. Emergency 2016, 4, 72–77. [Google Scholar] [PubMed]
- Vogel, L.D.; Vongsachang, H.; Pirrotta, E.; Holmes, J.F.; Sherck, J.; Newton, C.; D’Souza, P.; Spain, D.A.; Wang, N.E. Variations in pediatric trauma transfer patterns in Northern California pediatric trauma centers (2001–2009). Acad. Emerg. Med. 2014, 21, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- Health Statistics II. Ministry of Health and Welfare. 2009. Available online: http://www.mohw.gov.tw/EN/Ministry/Statistic.aspx?f_list_no=474 (assessed on 1 February 2017).
- Gielen, A.C.; McDonald, E.M.; Shields, W. Unintentional home injuries across the life span: Problems and solutions. Annu. Rev. Public Health 2015, 36, 231–253. [Google Scholar] [CrossRef] [PubMed]
- Kemp, A.; Sibert, J. Childhood accidents: Epidemiology, trends, and prevention. J. Accid. Emerg. Med. 1997, 14, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Lu, T.H.; Lee, M.C.; Chou, M.C. Trends in injury mortality among adolescents in Taiwan, 1965-94. Inj. Prev. 1998, 4, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Kurup, S.P.S.; Padankatti, S.; Thomas, K. Accidental injuries in the Pediatric Emergency Department. Int. J. Emerg. Med. 2014, 7 (Suppl. 1), P9. [Google Scholar] [CrossRef]
- Ferraz-Torres, M.; Belzunegui-Otano, T.; Martinez-Garcia, O.; Iriarte-Cerdán, L.; Salgado-Reguero, E. Epidemiological characteristics and overall burden of accidental injuries in navarra, spain: Epidemiology of injuries in children. J. Trauma Nurs. 2016, 23, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.Y.; Wiznia, D.H.; Averbukh, L.; Dai, F.; Leslie, M.P. The economic impact of helmet use on motorcycle accidents: A systematic review and meta-analysis of the literature from the past 20 years. Traffic Inj. Prev. 2015, 16, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Liang, C.C.; Liu, H.T.; Rau, C.S.; Hsu, S.-Y.; Hsieh, H.-Y.; Hsieh, C.-H. Motorcycle-related hospitalization of adolescents in a Level I trauma center in southern Taiwan: A cross-sectional study. BMC Pediatr. 2015, 15, 105. [Google Scholar] [CrossRef] [PubMed]
- Niederdeppe, J.; Avery, R.; Miller, E.N. Alcohol-control public service announcements (PSAs) and drunk-driving fatal accidents in the United States, 1996–2010. Prev. Med. 2017, 99, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Scott, D.; Siskind, V. Patterns of injury in hospitalized one-year-old children: Analysis by trimester of age using coded data and textual description. Int. J. Environ. Res. Public Health 2016, 13, 674. [Google Scholar] [CrossRef] [PubMed]
- Dismuke, C.E.; Bishu, K.G.; Fakhry, S.; Walker, R.J.; Egede, L.E. Clinical factors and expenditures associated with ICD-9-CM coded trauma for the U.S. population: A nationally representative study. Acad. Emerg. Med. 2017, 24, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.Y.; Liu, J.M.; Chang, F.W.; Chang, H.; Cheng, K.C.; Yeh, C.L.; Wei, Y.F.; Hsu, R.J. Scabies increased the risk and severity of COPD: A nationwide population-based study. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 2171–2178. [Google Scholar]
- American Hospital Association; American Medical Record Association; Health Care Financing Administration; National Center for Health Statistics. ICD-9-CM coding and reporting official guidelines. J. Am. Med. Rec. Assoc. 1990, 61, 1–17. [Google Scholar]
- Lu, Y.L.; Chien, W.C.; Lin, F.H.; Chiu, Y.-L.; Pai, L.; Chang, Y.-T.; Villarreal, D.S.; Pan, C.-H.; Chang, S.-C.; Lin, K.H.; et al. Long-term trends in child and youth injury mortality in Taiwan, 1989–2007. J. Med. Sci. 2015, 35, 147–156. [Google Scholar]
- Chien, W.C.; Pai, L.; Chu, C.M.; Kao, S.; Tsai, S.H. Trends in child and adolescent injury mortality in Taiwan, 1986–2006. Taiwan J. Public Health 2010, 29, 22–32. [Google Scholar]
- Allareddy, V.; Anderson, I.M.; Lee, M.K.; Allareddy, V.; Rampa, S.; Nalliah, R.P. Hospital-based emergency department visits in children with motor vehicle traffic accidents: Estimates from the nationwide emergency department sample. World J. Pediatr. 2015, 11, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Cummings, P.; Rivara, F.P.; Olson, C.M.; Smith, K.M. Changes in traffic crash mortality rates attributed to use of alcohol, or lack of a seat belt, air bag, motorcycle helmet, or bicycle helmet, United States, 1982–2001. Inj. Prev. 2006, 12, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.M.; Liao, C.M. Inpatient expenditures on alcohol-attributed diseases and alcohol tax policy: A nationwide analysis in Taiwan from 1996 to 2010. Public Health 2014, 128, 977–984. [Google Scholar] [CrossRef] [PubMed]
- Benjamin Neelon, S.E.; Duffey, K.; Slining, M.M. Regulations to promote healthy sleep practices in child care. Pediatrics 2014, 134, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Sumner, S.A.; Mercy, J.A.; Dahlberg, L.L.; Hillis, S.D.; Klevens, J.; Houry, D. Violence in the United States: Status, challenges, and opportunities. JAMA 2015, 314, 478–488. [Google Scholar] [CrossRef] [PubMed]
- Bossarte, R.M.; Simon, T.R.; Barker, L. Characteristics of homicide followed by suicide incidents in multiple states, 2003-04. Inj. Prev. 2006, 12 (Suppl. 2), ii33–ii38. [Google Scholar] [CrossRef] [PubMed]
- Michas, G.; Varytimiadi, A.; Micha, R. The Greek financial crisis and homicide rates: Another reason to worry. J. Epidemiol. Community Health 2013, 67, 1073. [Google Scholar] [CrossRef] [PubMed]
- Khang, Y.H.; Lynch, J.W.; Kaplan, G.A. Impact of economic crisis on cause-specific mortality in South Korea. Int. J. Epidemiol. 2005, 34, 1291–1301. [Google Scholar] [CrossRef] [PubMed]
- Torrubiano-Dominguez, J.; Vives-Cases, C.; San-Sebastian, M.; Sanz-Barbero, B.; Goicolea, I.; Álvarez-Dardet, C. No effect of unemployment on intimate partner-related femicide during the financial crisis: A longitudinal ecological study in Spain. BMC Public Health 2015, 15, 990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fragkouli, K.; Boumba, V.; Vougiouklakis, T. Survey of medico-legal investigation of homicide in the region of Epirus (Northwest Greece). J. Forensic Leg. Med. 2016, 37, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Kim, D. The associations between U.S. state and local social spending, income inequality, and individual all-cause and cause-specific mortality: The national longitudinal mortality study. Prev. Med. 2016, 84, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Bacci, S.; Pigini, C.; Seracini, M.; Minelli, L. Employment condition, economic deprivation and self-evaluated health in Europe: Evidence from EU-SILC 2009–2012. Int. J. Environ. Res. Public Health 2017, 14, 143. [Google Scholar] [CrossRef] [PubMed]
- Tsouvelas, G.; Kontaxakis, V.; Giotakos, O.; Konstantakopoulos, G.; Kontaxaki, M.I.; Papaslanis, T. Financial crisis and criminality in Greece: 2008 vs. 2011. Psychiatriki 2016, 27, 54–57. [Google Scholar] [PubMed]
- Horton, R. The global financial crisis: An acute threat to health. Lancet 2009, 373, 355–356. [Google Scholar] [CrossRef]
- National Bureau of Statistics; Taiwan. National Statistics. 2002–2009. Available online: http://engstatgovtw/mpasp?mp=5 (assessed on 1 February 2017).
- Kondilis, E.; Giannakipoulos, S.; Gavana, M.; Ierodiakonou, I.; Waitzkin, H.; Benos, A. Economic crisis, restrictive policies, and the population’s health and health care: The Greek case. Am. J. Public Health 2013, 103, 973–979. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Homicide rates among persons aged 10–24 years—United States, 1981–2010. Morb. Mortal. Wkly. Rep. 2013, 62, 545–548. [Google Scholar]
- Abrahams, N.; Mathews, S.; Lombard, C.; Martin, L.J.; Jewkes, R. Sexual homicides in South Africa: A national cross-sectional epidemiological study of adult women and children. PLoS ONE 2017, 12, e0186432. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Injury Type | Patient Number Incidence/1000,000 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Year | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | |
| Cause | |||||||||
| Unintentional Injuries | 565 | 503 | 419 | 306 | 305 | 269 | 223 | 240 | |
| (E800–E949) | 2061.83 | 1955.17 | 1765.44 | 1346.78 | 1426.52 | 1342.15 | 1196.80 | 1392.10 | |
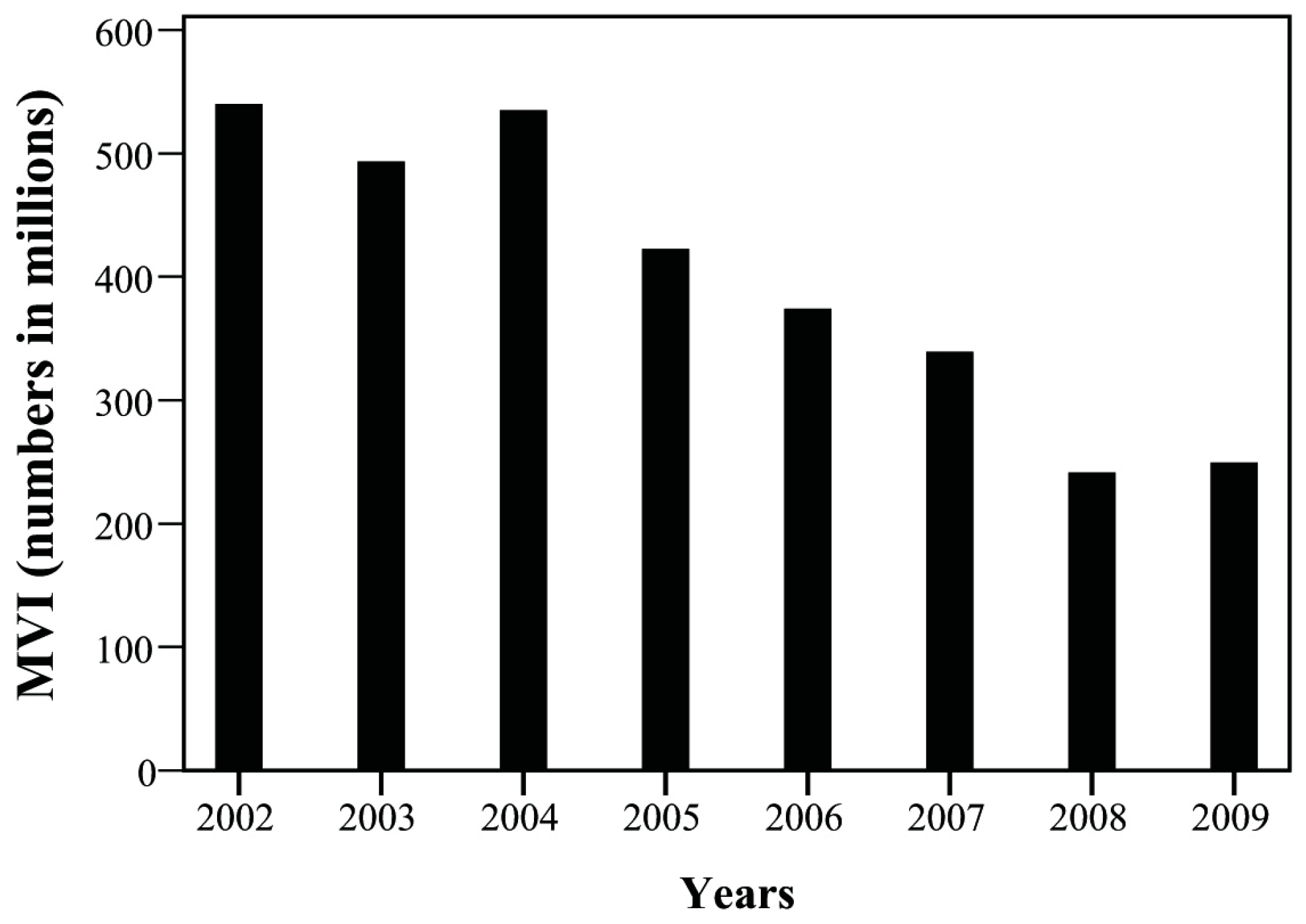
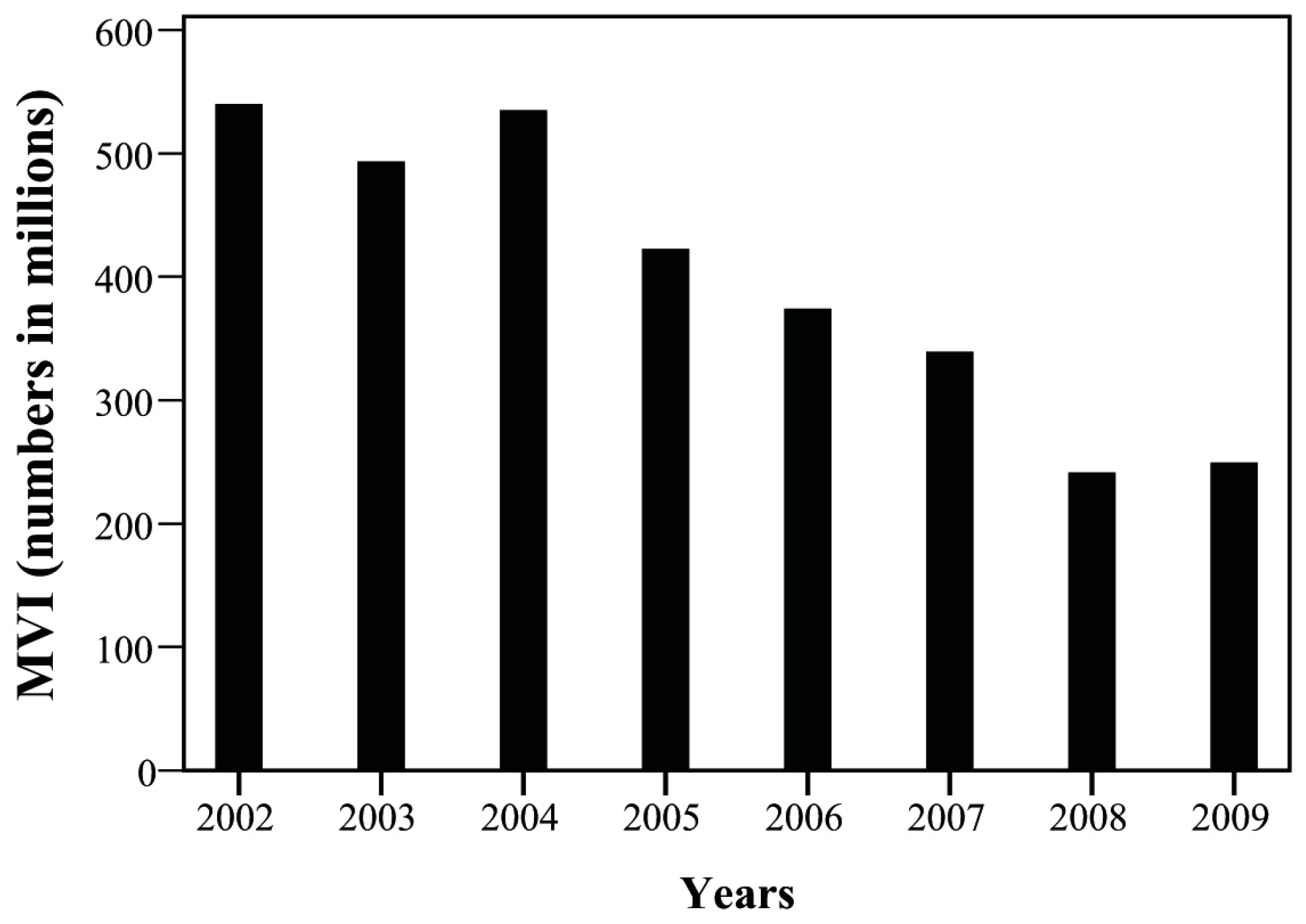
| MVI * | 148 | 127 | 127 | 96 | 80 | 68 | 45 | 43 | |
| (E810–E819) | 540.09 | 493.65 | 535.11 | 422.52 | 374.17 | 339.28 | 241.51 | 249.42 | |
| Poisoning | 5 | 7 | 5 | 3 | 5 | 1 | 4 | 3 | |
| (E850–E869) | 18.25 | 27.21 | 21.07 | 13.20 | 23.39 | 4.99 | 21.47 | 17.40 | |
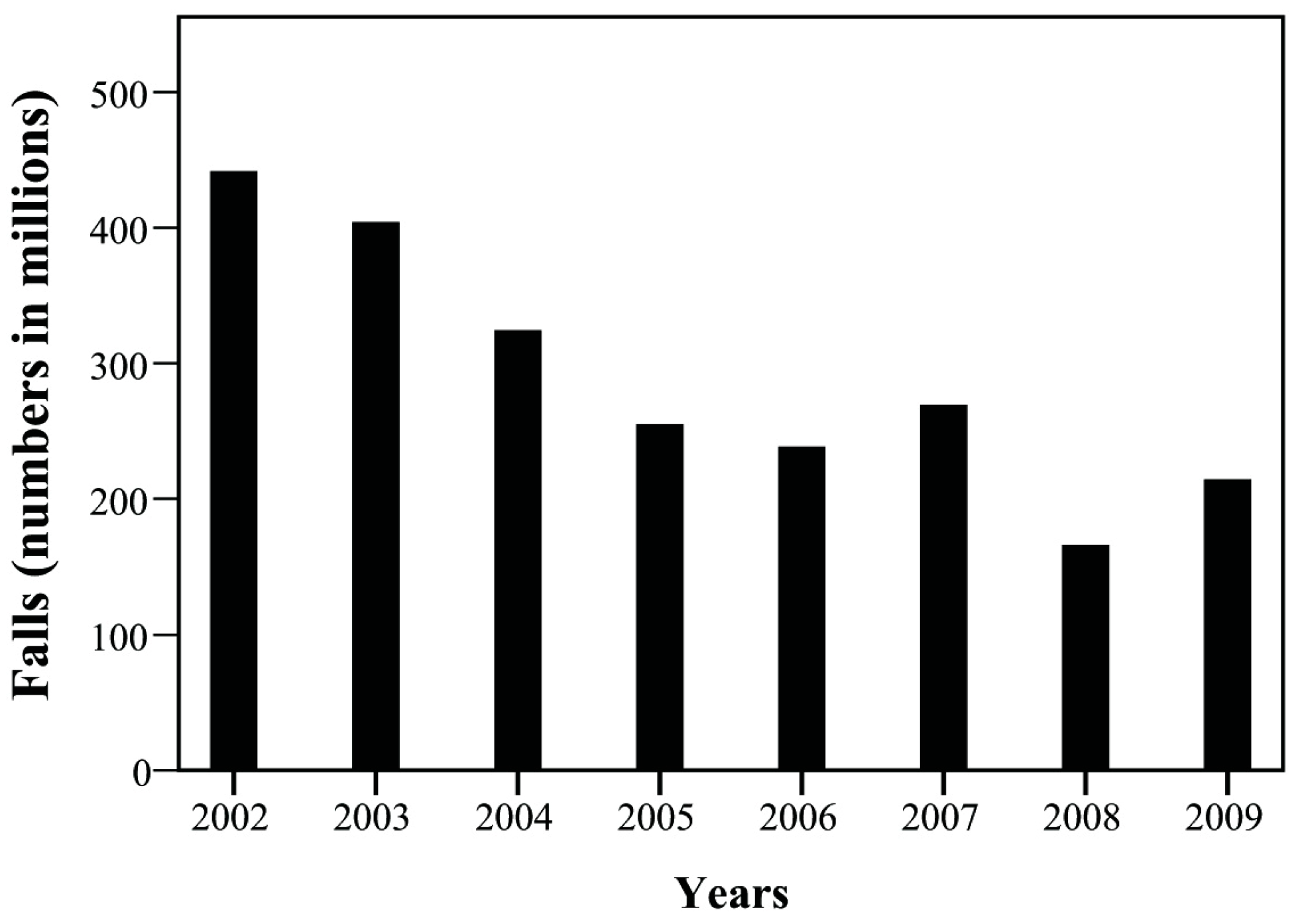
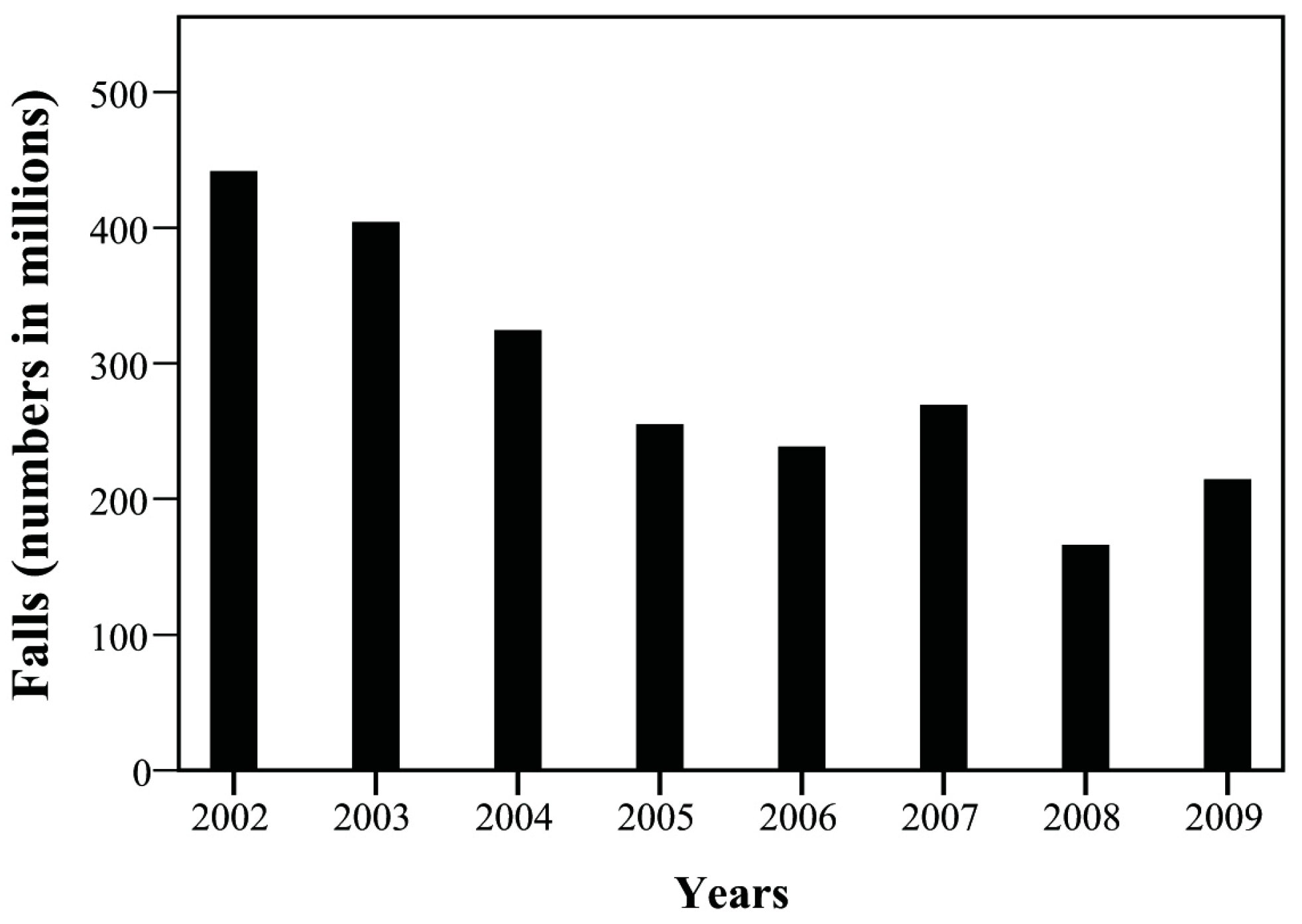
| Falls | 121 | 104 | 77 | 58 | 51 | 54 | 31 | 37 | |
| (E880–E888) | 441.56 | 404.25 | 324.44 | 255.27 | 238.53 | 269.43 | 166.37 | 214.61 | |
| Fire and Flames | 4 | 2 | 0 | 0 | 1 | 1 | 1 | 0 | |
| (E890–E899) | 14.60 | 7.77 | 0 | 0 | 4.68 | 4.99 | 5.37 | 0 | |
| Drowning | 1 | 1 | 0 | 2 | 0 | 1 | 1 | 1 | |
| (E910) | 3.65 | 3.89 | 0 | 8.80 | 0 | 4.99 | 5.37 | 5.80 | |
| Suffocation | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | |
| (E911–E913) | 0 | 3.89 | 4.21 | 0 | 4.68 | 0 | 0 | 0 | |
| Cut Injuries | 25 | 18 | 10 | 4 | 8 | 5 | 14 | 11 | |
| (E920) | 91.23 | 69.97 | 42.13 | 17.6 | 37.42 | 24.95 | 75.14 | 63.80 | |
| Other | 59 | 61 | 33 | 20 | 21 | 14 | 7 | 12 | |
| (E916–E928) | 215.31 | 237.11 | 139.04 | 88.02 | 98.22 | 69.85 | 37.57 | 69.60 | |
| Intentional Injuries | 73 | 43 | 49 | 38 | 48 | 63 | 60 | 50 | |
| (E950–E999) | 266.40 | 167.14 | 206.46 | 167.25 | 224.50 | 314.33 | 322.01 | 290.02 | |
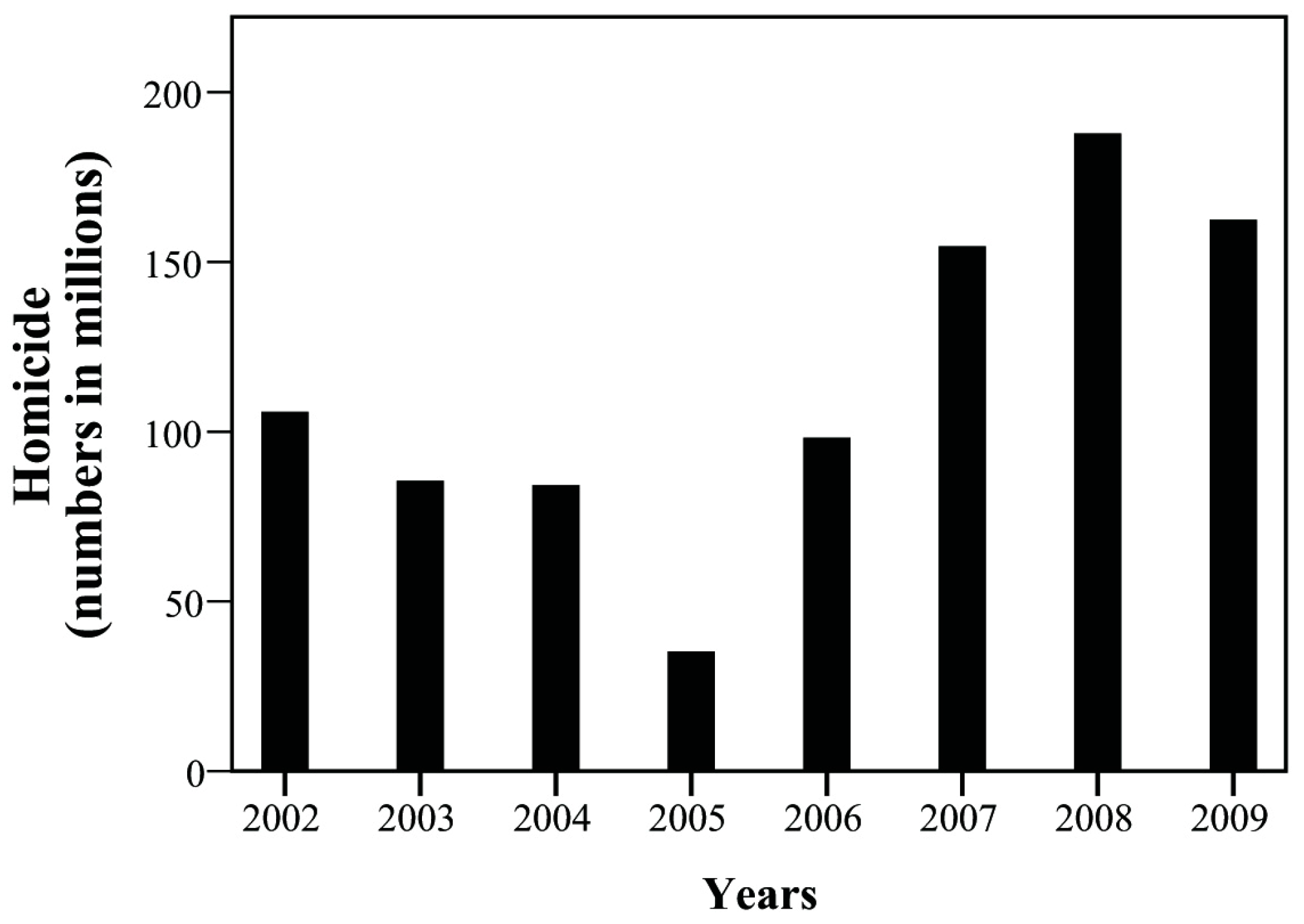
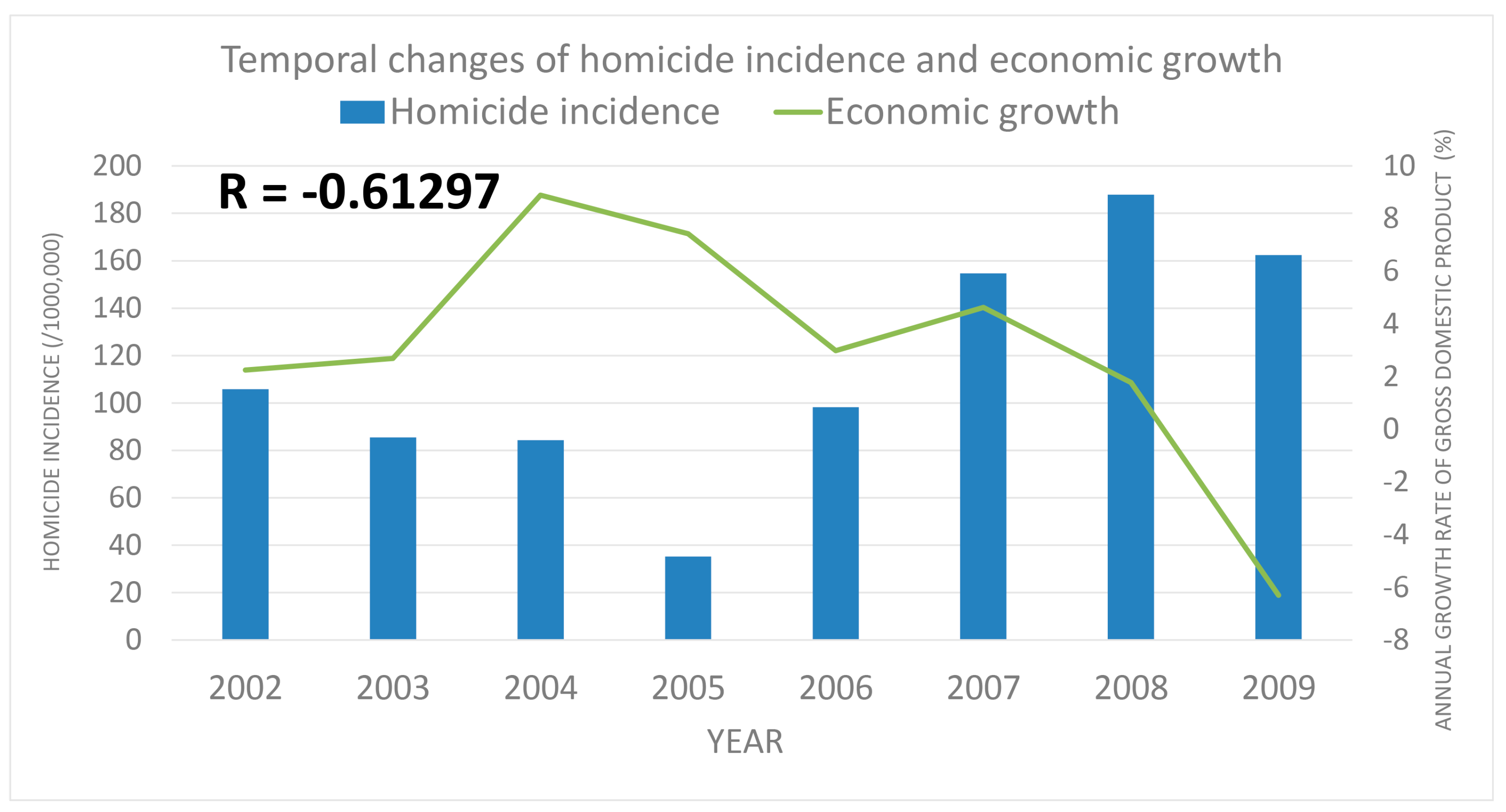
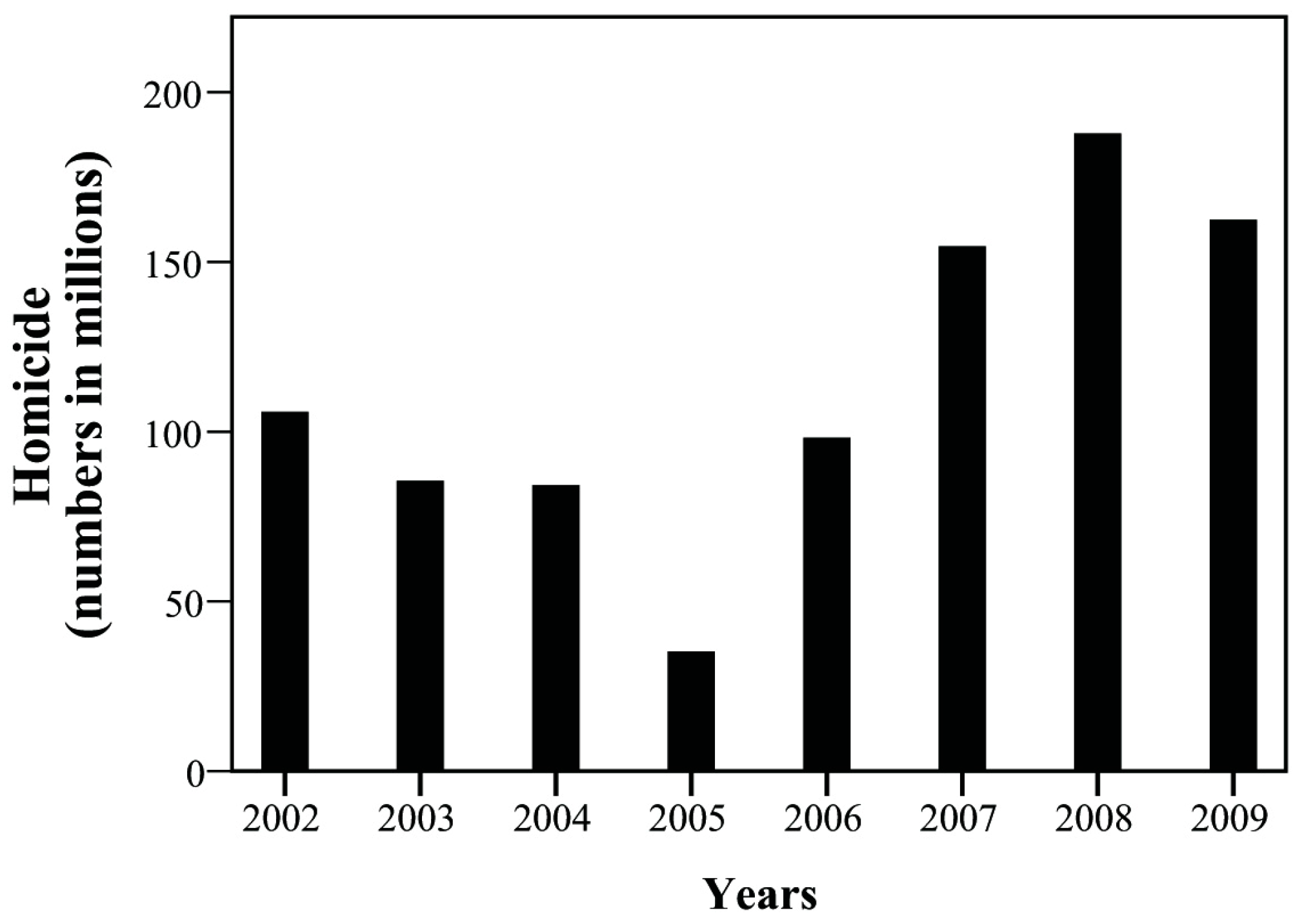
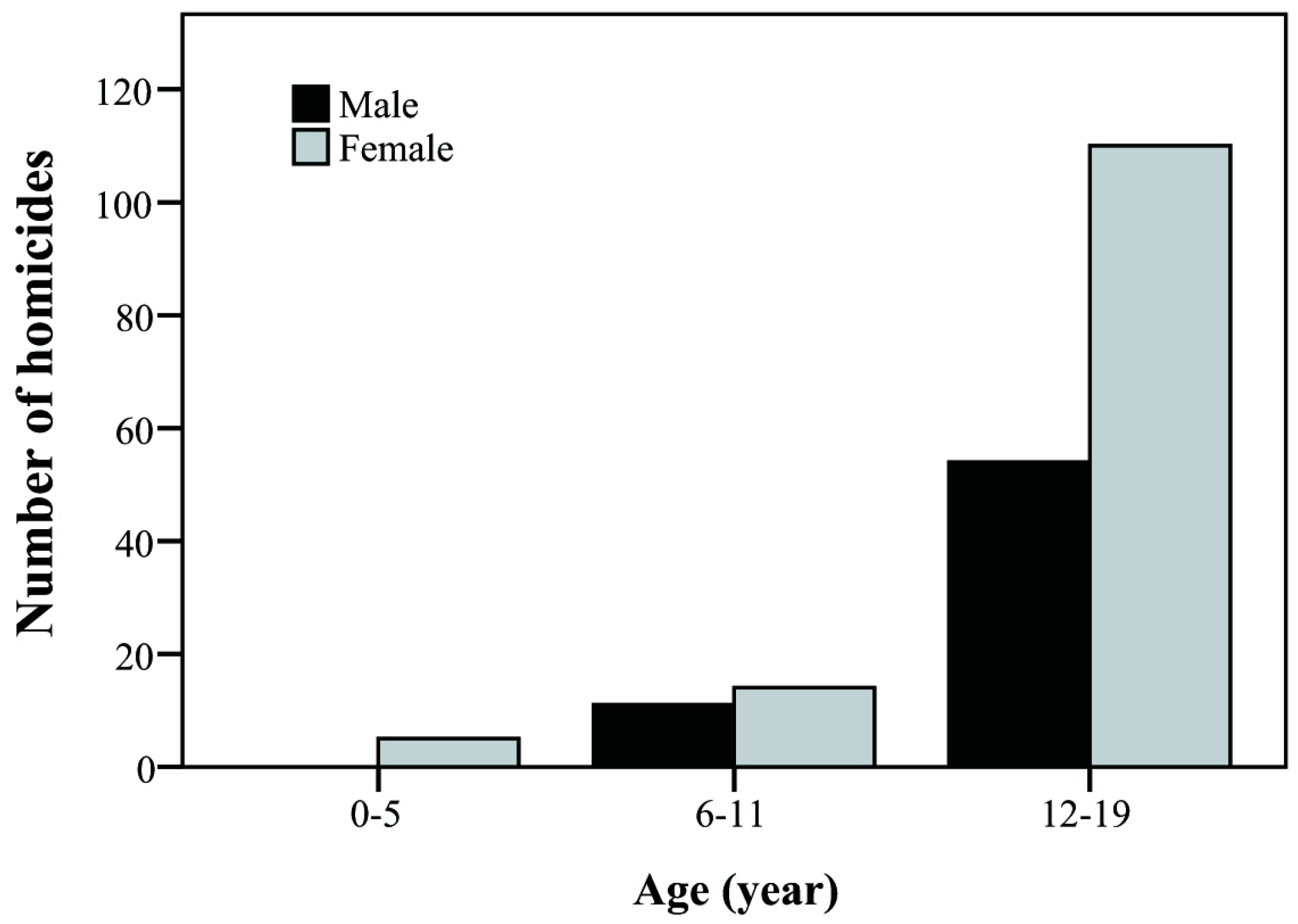
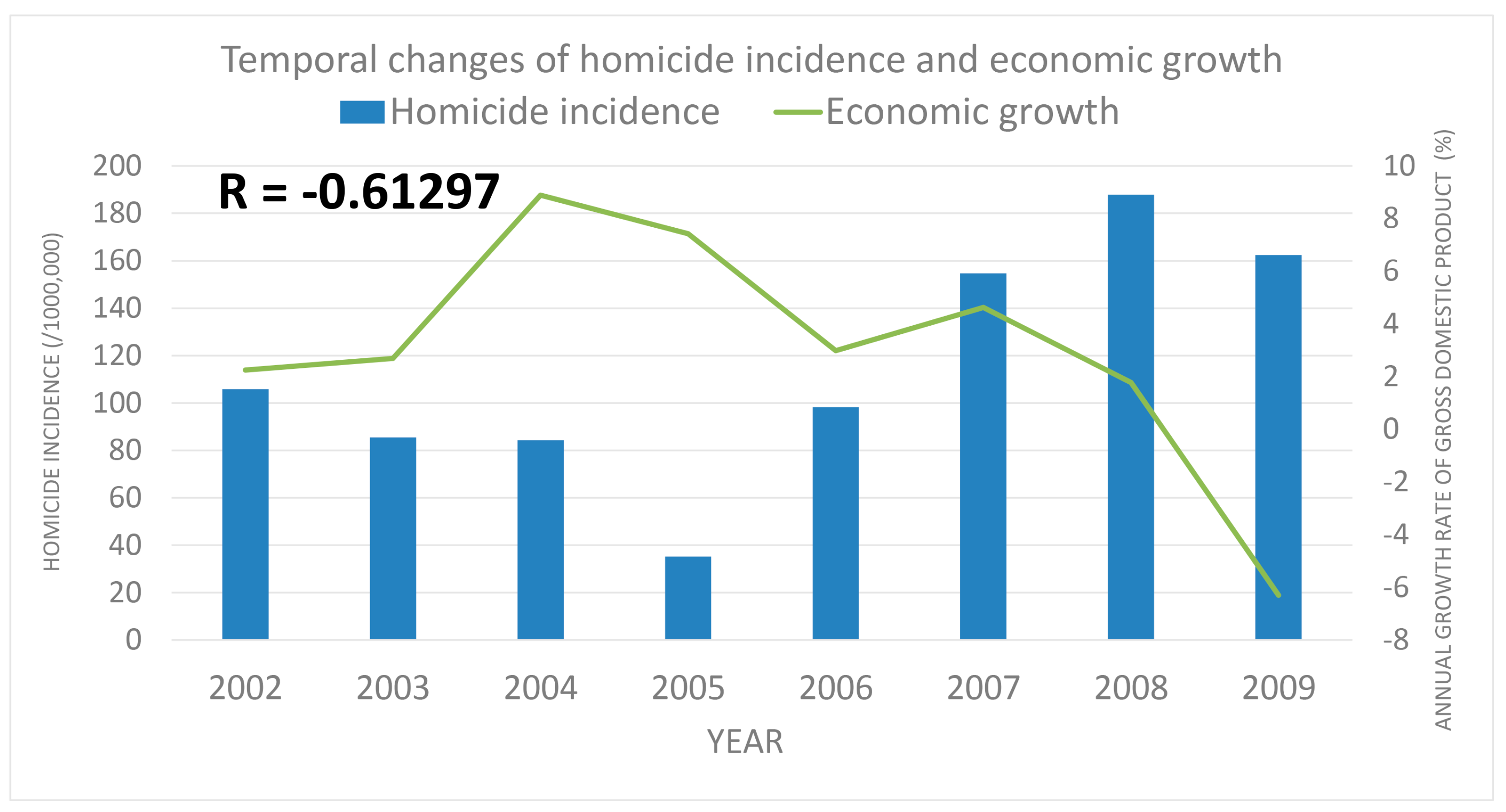
| Homicide | 29 | 22 | 20 | 8 | 21 | 31 | 35 | 28 | |
| (E950-E959) | 105.83 | 85.51 | 84.27 | 35.21 | 98.22 | 154.67 | 187.84 | 162.41 | |
| Suicide | 3 | 2 | 4 | 3 | 5 | 7 | 3 | 3 | |
| (E960–E969) | 10.95 | 7.77 | 16.85 | 13.20 | 23.39 | 34.93 | 16.10 | 17.40 | |
| Other | 41 | 19 | 25 | 27 | 22 | 25 | 22 | 19 | |
| (E980–E989) | 149.62 | 73.85 | 105.34 | 118.83 | 102.90 | 124.73 | 118.07 | 110.21 | |
| Year | Economic Growth (%) | Per Capita Gross Domestic Product | Per Capita National Income | ||
|---|---|---|---|---|---|
| Value (NTD *) | Annual Growth Rate (%) | Value (NTD *) | Annual Growth Rate (%) | ||
| 2002 | 5.57 | 13,750 | 2.25 | 12,270 | 2.8 |
| 2003 | 4.12 | 14,120 | 2.69 | 12,642 | 3.03 |
| 2004 | 6.51 | 15,388 | 8.89 | 13,735 | 8.65 |
| 2005 | 5.42 | 16,532 | 7.43 | 14,602 | 6.31 |
| 2006 | 5.62 | 17,026 | 2.99 | 14,974 | 2.55 |
| 2007 | 6.52 | 17,814 | 4.63 | 15,401 | 2.85 |
| 2008 | 0.7 | 18,131 | 1.78 | 15,388 | −0.08 |
| 2009 | −1.57 | 16,988 | −6.3 | 14,398 | −6.43 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.-P.; Hsu, R.-J.; Wu, M.-H.; Peng, C.-C.; Chang, S.-T.; Lei, W.-T.; Yeh, T.-L.; Liu, J.-M.; Lin, C.-Y. Economic Conditions May Contribute to Increased Violence toward Children: A Nationwide Population-Based Analysis of Pediatric Injuries in Taiwanese Emergency Departments. Int. J. Environ. Res. Public Health 2018, 15, 182. https://doi.org/10.3390/ijerph15020182
Liu Y-P, Hsu R-J, Wu M-H, Peng C-C, Chang S-T, Lei W-T, Yeh T-L, Liu J-M, Lin C-Y. Economic Conditions May Contribute to Increased Violence toward Children: A Nationwide Population-Based Analysis of Pediatric Injuries in Taiwanese Emergency Departments. International Journal of Environmental Research and Public Health. 2018; 15(2):182. https://doi.org/10.3390/ijerph15020182
Chicago/Turabian StyleLiu, Yueh-Ping, Ren-Jun Hsu, Mei-Hwan Wu, Chun-Chih Peng, Shu-Ting Chang, Wei-Te Lei, Tzu-Lin Yeh, Jui-Ming Liu, and Chien-Yu Lin. 2018. "Economic Conditions May Contribute to Increased Violence toward Children: A Nationwide Population-Based Analysis of Pediatric Injuries in Taiwanese Emergency Departments" International Journal of Environmental Research and Public Health 15, no. 2: 182. https://doi.org/10.3390/ijerph15020182