Are Perceived and Objective Distances to Fresh Food and Physical Activity Resources Associated with Cardiometabolic Risk?

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
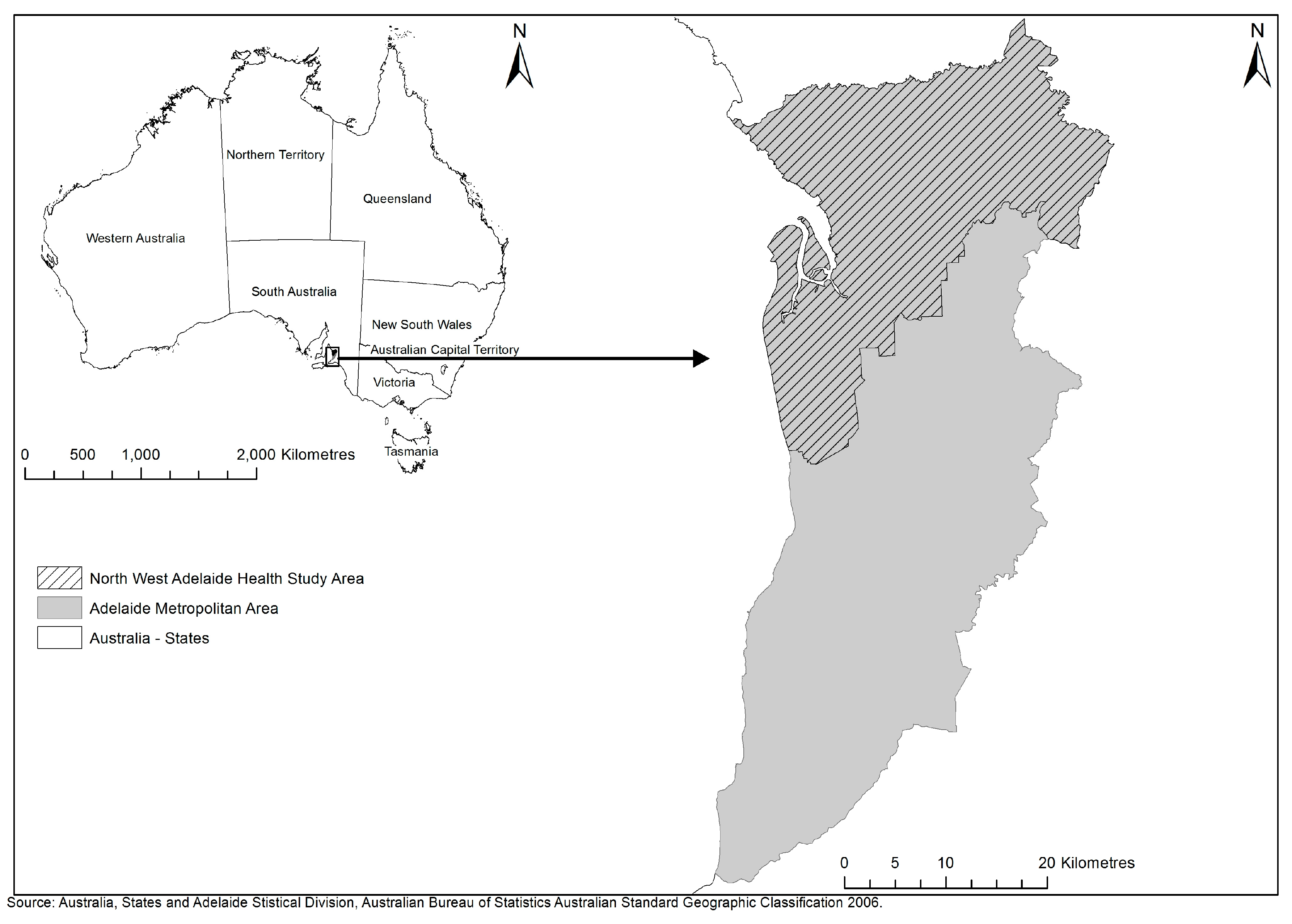
2.1. Study Context
2.2. Sample
2.3. Measures
2.3.1. Outcome Variable
2.3.2. Independent Variables
Resident Perceptions of Fruit and Vegetable Retailers and Public Open Space
Objectively Assessed Fruit and Vegetable Retailers and Public Open Space
Discordance between Perceived and Objective Distances (Overestimation of Distances) to Fruit and Vegetable Retailers and Public Open Space
2.3.3. Mediators
2.3.4. Covariates
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Alberti, K.G.M.M.; Zimmet, P.; Shaw, J. The metabolic syndrome—A new worldwide definition. Lancet 2005, 366, 1059–1062. [Google Scholar] [CrossRef]
- Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z. The metabolic syndrome. Lancet 2005, 365, 1415–1428. [Google Scholar] [CrossRef]
- Daniel, M.; Moore, S.; Kestens, Y. Framing the biosocial pathways underlying associations between place and cardiometabolic disease. Health Place 2008, 14, 117–132. [Google Scholar] [CrossRef] [PubMed]
- Diez Roux, A.V.; Evenson, K.R.; McGinn, A.P.; Brown, D.G.; Moore, L.; Brines, S.; Jacobs, D.R., Jr. Availability of recreational resources and physical activity in adults. Am. J. Public Health 2007, 97, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Giles-Corti, B.; Donovan, R.J. Socioeconomic status differences in recreational physical activity levels and real and perceived access to a supportive physical environment. Prev. Med. 2002, 35, 601–611. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Leslie, E.; Giles-Corti, B.; Owen, N. Physical activity for recreation or exercise on neighbourhood streets: Associations with perceived environmental attributes. Health Place 2009, 15, 1058–1063. [Google Scholar] [CrossRef] [PubMed]
- Giles-Corti, B.; Broomhall, M.H.; Knuiman, M.; Collins, C.; Douglas, K.; Ng, K.; Lange, A.; Donovan, R.J. Increasing walking—How important is distance to, attractiveness, and size of public open space? Am. J. Prev. Med. 2005, 28, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Rose, D.; Richards, R. Food store access and household fruit and vegetable use among participants in the US food stamp program. Public Health Nutr. 2004, 7, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Blitstein, J.L.; Snider, J.; Evans, W.D. Perceptions of the food shopping environment are associated with greater consumption of fruits and vegetables. Public Health Nutr. 2012, 15, 1124–1129. [Google Scholar] [CrossRef] [PubMed]
- Morland, K.; Wing, S.; Diez Roux, A. The contextual effect of the local food environment on residents’ diets: The atherosclerosis risk in communities study. Am. J. Public Health 2002, 92, 1761–1767. [Google Scholar] [CrossRef] [PubMed]
- Inagami, S.; Cohen, D.A.; Finch, B.K.; Asch, S.M. You are where you shop: Grocery store locations, weight, and neighborhoods. Am. J. Prev. Med. 2006, 31, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Morland, K.B.; Evenson, K.R. Obesity prevalence and the local food environment. Health Place 2009, 15, 491–495. [Google Scholar] [CrossRef] [PubMed]
- Lopez, R.P. Neighborhood risk factors for obesity. Obesity 2007, 15, 2111–2119. [Google Scholar] [CrossRef] [PubMed]
- Morland, K.; Diez Roux, A.V.; Wing, S. Supermarkets, other food stores, and obesity: The atherosclerosis risk in communities study. Am. J. Prev. Med. 2006, 30, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Cerin, E.; Frank, L.D.; Sallis, J.F.; Saelens, B.E.; Conway, T.L.; Chapman, J.E.; Glanz, K. From neighborhood design and food options to residents’ weight status. Appetite 2011, 56, 693–703. [Google Scholar] [CrossRef] [PubMed]
- Paquet, C.; Coffee, N.T.; Haren, M.T.; Howard, N.J.; Adams, R.J.; Taylor, A.W.; Daniel, M. Food environment, walkability, and public open spaces are associated with incident development of cardio-metabolic risk factors in a biomedical cohort. Health Place 2014, 28, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Brown, B.B.; Yamada, I.; Smith, K.R.; Zick, C.D.; Kowaleski-Jones, L.; Fan, J.X. Mixed land use and walkability: Variations in land use measures and relationships with BMI, overweight, and obesity. Health Place 2009, 15, 1130–1141. [Google Scholar] [CrossRef] [PubMed]
- Stafford, M.; Cummins, S.; Ellaway, A.; Sacker, A.; Wiggins, R.D.; Macintyre, S. Pathways to obesity: Identifying local, modifiable determinants of physical activity and diet. Soc. Sci. Med. 2007, 65, 1882–1897. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.C.; Kim, S.; Gonzalez, A.A.; MacLeod, K.E.; Winkleby, M.A. Socioeconomic and food-related physical characteristics of the neighbourhood environment are associated with body mass index. J. Epidemiol. Community Health 2007, 61, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Daniel, M.; Paquet, C.; Auger, N.; Zang, G.; Kestens, Y. Association of fast-food restaurant and fruit and vegetable store densities with cardiovascular mortality in a metropolitan population. Eur. J. Epidemiol. 2010, 25, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Boehmer, T.K.; Hoehner, C.M.; Deshpande, A.D.; Brennan Ramirez, L.K.; Brownson, R. Perceived and observed neighborhood indicators of obesity among urban adults. Int. J. Obes. 2007, 31, 968–977. [Google Scholar] [CrossRef] [PubMed]
- Auchincloss, A.H.; Diez Roux, A.V.; Mujahid, M.S.; Shen, M.; Bertoni, A.G.; Carnethon, M.R. Neighborhood resources for physical activity and healthy foods and incidence of type 2 diabetes mellitus: The multi-ethnic study of atherosclerosis. Arch. Intern. Med. 2009, 169, 1698–1704. [Google Scholar] [CrossRef] [PubMed]
- Auchincloss, A.H.; Diez Roux, A.V.; Brown, D.G.; Erdmann, C.A.; Bertoni, A.G. Neighborhood resources for physical activity and healthy foods and their association with insulin resistance. Epidemiology 2008, 19, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Auchincloss, A.H.; Mujahid, M.S.; Shen, M.; Michos, E.D.; Whitt-Glover, M.C.; Diez Roux, A.V. Neighborhood health-promoting resources and obesity risk (the multi-ethnic study of atherosclerosis). Obesity 2013, 21, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Christine, P.J.; Auchincloss, A.H.; Bertoni, A.G.; Carnethon, M.R.; Sánchez, B.N.; Moore, K.; Adar, S.D.; Horwich, T.B.; Watson, K.E.; Diez Roux, A.V. Longitudinal associations between neighborhood physical and social environments and incident type 2 diabetes mellitus: The multi-ethnic study of atherosclerosis (MESA). JAMA Intern. Med. 2015, 175, 1311–1320. [Google Scholar] [CrossRef] [PubMed]
- Lovasi, G.S.; Grady, S.; Rundle, A. Steps forward: Review and recommendations for research on walkability, physical activity and cardiovascular health. Public Health Rev. 2012, 33, 484–506. [Google Scholar] [CrossRef] [PubMed]
- Chaix, B. Geographic life environments and coronary heart disease: A literature review, theoretical contributions, methodological updates, and a research agenda. Annu. Rev. Public Health 2009, 30, 81–105. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Moudon, A.V. Objective versus subjective measures of the built environment, which are most effective in capturing associations with walking? Health Place 2010, 16, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Paquet, C.; Daniel, M.; Kestens, Y.; Leger, K.; Gauvin, L. Field validation of listings of food stores and commercial physical activity establishments from secondary data. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 58. [Google Scholar] [CrossRef] [PubMed]
- Liese, A.D.; Colabianchi, N.; Lamichhane, A.P.; Barnes, T.L.; Hibbert, J.D.; Porter, D.E.; Nichols, M.D.; Lawson, A.B. Validation of 3 food outlet databases: Completeness and geospatial accuracy in rural and urban food environments. Am. J. Epidemiol. 2010, 172, 1324–1333. [Google Scholar] [CrossRef] [PubMed]
- Lake, A.A.; Burgoine, T.; Greenhalgh, F.; Stamp, E.; Tyrrell, R. The foodscape: Classification and field validation of secondary data sources. Health Place 2010, 16, 666–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosler, A.S.; Dharssi, A. Identifying retail food stores to evaluate the food environment. Am. J. Prev. Med. 2010, 39, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Cummins, S.; Macintyre, S. Are secondary data sources on the neighbourhood food environment accurate? Case-study in Glasgow, UK. Prev. Med. 2009, 49, 527–528. [Google Scholar] [CrossRef] [PubMed]
- Boone, J.E.; Gordon-Larsen, P.; Stewart, J.D.; Popkin, B.M. Validation of a GIS facilities database: Quantification and implications of error. Ann. Epidemiol. 2008, 18, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Sharkey, J.R.; Horel, S. Neighborhood socioeconomic deprivation and minority composition are associated with better potential spatial access to the ground-truthed food environment in a large rural area. J. Nutr. 2008, 138, 620–627. [Google Scholar] [CrossRef] [PubMed]
- Zandbergen, P.A.; Green, J.W. Error and bias in determining exposure potential of children at school locations using proximity-based GIS techniques. Environ. Health Perspect. 2007, 115, 1363–1370. [Google Scholar] [CrossRef] [PubMed]
- Saarinen, T.F. Environmental perception. In Perspectives on Environment; Manners, I., Mikesell, M., Eds.; Association of American Geographers, Commission on College Geography: Washington, DC, USA, 1974. [Google Scholar]
- Boehmer, T.K.; Hoehner, C.M.; Wyrwich, K.W.; Brennan Ramirez, L.K.; Brownson, R. Correspondence between perceived and observed measures of neighborhood environmental supports for physical activity. J. Phys. Act. Health 2006, 3, 22–36. [Google Scholar] [CrossRef]
- McArthur, L.Z.; Baron, R.M. Toward an ecological theory of social perception. Psychol. Rev. 1983, 90, 215–238. [Google Scholar] [CrossRef]
- Cummins, S. Neighbourhood food environment and diet: Time for improved conceptual models? Prev. Med. 2007, 44, 196–197. [Google Scholar] [CrossRef] [PubMed]
- Ball, K.; Jeffery, R.W.; Crawford, D.A.; Roberts, R.J.; Salmon, J.; Timperio, A.F. Mismatch between perceived and objective measures of physical activity environments. Prev. Med. 2008, 47, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Blacksher, E.; Lovasi, G.S. Place-focused physical activity research, human agency, and social justice in public health: Taking agency seriously in studies of the built environment. Health Place 2012, 18, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Saelens, B.E.; Sallis, J.F.; Frank, L.D. Environmental correlates of walking and cycling: Findings from the transportation, urban design, and planning literatures. Ann. Behav. Med. 2003, 25, 80–91. [Google Scholar] [CrossRef] [PubMed]
- McCormack, G.R.; Cerin, E.; Leslie, E.; Du Toit, L.; Owen, N. Objective versus perceived walking distances to destinations. Environ. Behav. 2008, 40, 401–425. [Google Scholar] [CrossRef]
- Duncan, M.J.; Spence, J.C.; Mummery, W.K. Perceived environment and physical activity: A meta-analysis of selected environmental characteristics. Int. J. Behav. Nutr. Phys. Act. 2005, 2, 11. [Google Scholar] [CrossRef] [PubMed]
- Owen, N.; Humpel, N.; Leslie, E.; Bauman, A.; Sallis, J.F. Understanding environmental influences on walking; Review and research agenda. Am. J. Prev. Med. 2004, 27, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Bowen, D.J.; Barrington, W.E.; Beresford, S.A.A. Identifying the effects of environmental and policy change interventions on healthy eating. Annu. Rev. Public Health 2015, 36, 289–306. [Google Scholar] [CrossRef] [PubMed]
- Kremers, S.P.; de Bruijn, G.J.; Visscher, T.L.; van Mechelen, W.; de Vries, N.K.; Brug, J. Environmental influences on energy balance-related behaviors: A dual-process view. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 9. [Google Scholar] [CrossRef] [PubMed]
- Montello, D.R. A conceptual model of the cognitive processing of environmental distance information. In Spatial Information Theory; Hornsby, K.S., Claramunt, C., Denis, M., Ligozat, G., Eds.; Springer: Berlin/Heidelberg, Germany, 2009; Volume 5756, pp. 1–17. [Google Scholar]
- Caspi, C.E.; Kawachi, I.; Subramanian, S.V.; Adamkiewicz, G.; Sorensen, G. The relationship between diet and perceived and objective access to supermarkets among low-income housing residents. Soc. Sci. Med. 2012, 75, 1254–1262. [Google Scholar] [CrossRef] [PubMed]
- Gebel, K.; Bauman, A.; Sugiyama, T.; Owen, N. Mismatch between perceived and objectively assessed neighborhood walkability attributes: Prospective relationships with walking and weight gain. Health Place 2011, 17, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics (ABS). Adelaide: A Social Atlas—2006 Census of Population and Housing; ABS: Canberra, Australia, 2008.
- Grant, J.F.; Chittleborough, C.R.; Taylor, A.W.; Dal Grande, E.; Wilson, D.H.; Phillips, P.J.; Adams, R.J.; Cheek, J.; Price, K.; Gill, T.K.; et al. The North West Adelaide health study: Detailed methods and baseline segmentation of a cohort for selected chronic diseases. Epidemiol. Perspect. Innov. 2006, 3, 4. [Google Scholar] [CrossRef] [PubMed]
- Grant, J.F.; Taylor, A.W.; Ruffin, R.E.; Wilson, D.H.; Phillips, P.J.; Adams, R.J.; Price, K. The North West Adelaide Health Study Team. Cohort profile: The North West Adelaide health study (NWAHS). Int. J. Epidemiol. 2009, 38, 1479–1486. [Google Scholar] [CrossRef] [PubMed]
- Cameron, A.J.; Zimmet, P.Z.; Shaw, J.E.; Alberti, K.G.M.M. The metabolic syndrome: In need of a global mission statement. Diabet. Med. 2009, 26, 306–309. [Google Scholar] [CrossRef] [PubMed]
- Carroll, S.J.; Niyonsenga, T.; Coffee, N.T.; Taylor, A.W.; Daniel, M. Does physical activity mediate the associations between local-area descriptive norms, built environment walkability, and glycosylated hemoglobin? Int. J. Environ. Res. Public Health 2017, 14, 953. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. The IDF Consensus Worldwide Definition of the Metabolic Syndrome; International Diabetes Federation: Brussels, Belgium, 2006. [Google Scholar]
- Leslie, E.; Saelens, B.; Frank, L.; Owen, N.; Bauman, A.; Coffee, N.; Hugo, G. Residents’ perceptions of walkability attributes in objectively different neighbourhoods: A pilot study. Health Place 2005, 11, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Saelens, B.E.; Sallis, J.F.; Black, J.B.; Chen, D. Neighborhood-based differences in physical activity: An environment scale evaluation. Am. J. Public Health 2003, 93, 1552–1558. [Google Scholar] [CrossRef] [PubMed]
- Planning, S.A. Community Information: 2007 Retail Database; Department of Planning, Transport and Infrastructure: Adelaide, Australia, 2008.
- Australian Bureau of Statistics (ABS). Are We Building on Smaller Blocks? ABS: Canberra, Australia, 2004.
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R., Jr.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of physical activities: An update of activity codes and met intensities. Med. Sci. Sports Exerc. 2000, 32, S498–S504. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics (ABS). National Health Survey: Users Guide, 2001; ABS: Canberra, Australia, 2003.
- Yaroch, A.L.; Tooze, J.; Thompson, F.E.; Blanck, H.M.; Thompson, O.M.; Colón-Ramos, U.; Shaikh, A.; McNutt, S.; Nebeling, L.C. Evaluation of three short dietary instruments to assess fruit and vegetable intake: The national cancer institute’s food attitudes and behaviors (fab) survey. J. Acad. Nutr. Diet. 2012, 112, 1570–1577. [Google Scholar] [CrossRef] [PubMed]
- Brown, W.J.; Trost, S.G.; Bauman, A.; Mummery, K.; Owen, N. Test-retest reliability of four physical activity measures used in population surveys. J. Sci. Med. Sport 2004, 7, 205–215. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics (ABS). Basic Community Profile Datapack (First/Second Release), Australia 2006; ABS: Canberra, Australia, 2007.
- Chaix, B.; Leal, C.; Evans, D. Neighborhood-level confounding in epidemiologic studies: Unavoidable challenges, uncertain solutions. Epidemiology 2010, 21, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics (ABS). Australian Statistical Geography Standard (ASGS): Volume 3—Non ABS Structures; ABS: Canberra, Australia, 2011.
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Selig, J.P.; Preacher, K.J. Monte Carlo Method for Assessing Mediation: An Interactive Tool for Creating Confidence Intervals for Indirect Effects. Available online: http://quantpsy.org/medmc/medmc.htm (accessed on 7 November 2017).
- Hayes, A.F. Beyond baron and kenny: Statistical mediation analysis in the new millennium. Commun. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Mobley, L.R.; Root, E.D.; Finkelstein, E.A.; Khavjou, O.; Farris, R.P.; Will, J.C. Environment, obesity, and cardiovascular disease risk in low-income women. Am. J. Prev. Med. 2006, 30, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Gebel, K.; Bauman, A.; Owen, N. Correlates of non-concordance between perceived and objective measures of walkability. Ann. Behav. Med. 2009, 37, 228–238. [Google Scholar] [CrossRef] [PubMed]
- Paquet, C.; Orschulok, T.P.; Coffee, N.T.; Howard, N.J.; Hugo, G.; Taylor, A.W.; Adams, R.J.; Daniel, M. Are accessibility and characteristics of public open spaces associated with a better cardiometabolic health? Landsc. Urban Plan 2013, 118, 70–78. [Google Scholar] [CrossRef]
- Nelson, N.M.; Woods, C.B. Obesogenic environments: Are neighbourhood environments that limit physical activity obesogenic? Health Place 2009, 15, 917–924. [Google Scholar] [CrossRef] [PubMed]
- Giles-Corti, B.; Bull, F.; Knuiman, M.; McCormack, G.; Van Niel, K.; Timperio, A.; Christian, H.; Foster, S.; Divitini, M.; Middleton, N.; et al. The influence of urban design on neighbourhood walking following residential relocation: Longitudinal results from the reside study. Soc. Sci. Med. 2013, 77, 20–30. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Individual Characteristics | Mean (SD)/n (%) |
|---|---|
| Age (years) | 56.6 (14.3) |
| Gender (n (%)) | |
| Male | 675 (45.3%) |
| Female | 816 (54.7%) |
| Education level (n (%)) | |
| Less than bachelor degree | 1298 (87.1%) |
| Bachelor degree or higher | 193 (12.9%) |
| Annual household income(AUD$) (n (%)) | |
| Less than $20,001 | 397 (26.6%) |
| $20,001 to $60,000 | 700 (47.0%) |
| More than $60,000 | 394 (26.4%) |
| Duration at current residence (years) | 20.3 (13.9) |
| Fruit and vegetable intake (number of serves per day) | 4.2 (1.9) |
| Physical activity score (total energy expenditure (METS)) | 1709.3 (3119.4) |
| Metabolic syndrome (n (%)) | 552 (37.0%) |
| Central obesity (n (%)) | 1064 (71.4%) |
| Hypertension (n (%)) | 878 (58.9%) |
| Dyslipidaemia (n (%)) | 700 (47.0%) |
| Prediabetes/Diabetes (n (%)) | 729 (48.9%) |
| Area Characteristics | Mean (SD)/n (%) |
| Area-level median weekly household income (AUD$) | 851.38 (200.4) |
| Distance to the nearest FVR (m) | 1164.6 (881.1) |
| Distance to the nearest POS (m) | 241.9 (300.5) |
| Nearest FVR: Perceived distance overestimated objective distance (n (%)) | 561 (37.6%) |
| Nearest FVR: Perceived distance matched objective distance (n (%)) | 628 (42.1%) |
| Nearest POS: Perceived distance overestimated objective distance (n (%)) | 728 (48.8%) |
| Nearest POS: Perceived distance matched objective distance (n (%)) | 699 (46.9%) |
| Cardiometabolic Outcomes | Objective Distance (n = 1491) | Perceived Distance (n = 1491) | Overestimated Distance (n = 1189) a | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Metabolic syndrome | ||||||
| Model 1 | 1.08 (0.96, 1.23) | 0.197 | 1.11 (1.01, 1.22) | 0.036 | 1.10 (0.86, 1.42) | 0.449 |
| Model 2 | 1.02 (0.89, 1.18) | 0.774 | 1.10 (0.98, 1.22) | 0.093 | - | - |
| Model 3 | 1.03 (0.89, 1.18) | 0.713 | 1.10 (0.98, 1.22) | 0.103 | 1.08 (0.84, 1.40) | 0.539 |
| Central obesity | ||||||
| Model 1 | 1.11 (0.97, 1.26) | 0.118 | 1.09 (0.98, 1.20) | 0.098 | 1.22 (0.93, 1.59) | 0.148 |
| Model 2 | 1.07 (0.92, 1.24) | 0.407 | 1.06 (0.94, 1.19) | 0.326 | - | - |
| Model 3 | 1.07 (0.92, 1.24) | 0.386 | 1.06 (0.94, 1.19) | 0.342 | 1.21 (0.93, 1.59) | 0.157 |
| Hypertension | ||||||
| Model 1 | 0.98 (0.86, 1.12) | 0.763 | 1.13 (1.02, 1.25) | 0.022 | 1.37 (1.03, 1.82) | 0.029 |
| Model 2 | 0.87 (0.75, 1.02) | 0.089 | 1.19 (1.05, 1.34) | 0.005 | - | - |
| Model 3 | 0.88 (0.75, 1.02) | 0.099 | 1.19 (1.05, 1.34) | 0.005 | 1.36 (1.02, 1.80) | 0.034 |
| Dyslipidaemia | ||||||
| Model 1 | 1.08 (0.96, 1.22) | 0.176 | 1.08 (0.98, 1.18) | 0.108 | 1.14 (0.89, 1.45) | 0.300 |
| Model 2 | 1.04 (0.91, 1.19) | 0.532 | 1.06 (0.95, 1.17) | 0.284 | - | - |
| Model 3 | 1.05 (0.92, 1.20) | 0.501 | 1.06 (0.95, 1.17) | 0.298 | 1.13 (0.88, 1.44) | 0.342 |
| Prediabetes/Diabetes | ||||||
| Model 1 | 1.03 (0.91, 1.16) | 0.658 | 0.99 (0.90, 1.09) | 0.868 | 0.82 (0.63, 1.07) | 0.139 |
| Model 2 | 1.05 (0.91, 1.21) | 0.543 | 0.97 (0.87, 1.09) | 0.653 | - | - |
| Model 3 | 1.05 (0.91, 1.21) | 0.515 | 0.97 (0.87, 1.09) | 0.635 | 0.82 (0.63, 1.06) | 0.126 |
| Cardiometabolic Outcomes | Objective Distance (n = 1491) | Perceived Distance (n = 1491) | Overestimated Distance (n = 1427) | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Metabolic syndrome | ||||||
| Model 1 | 0.92 (0.73, 1.16) | 0.463 | 1.08 (0.99, 1.18) | 0.097 | 1.22 (0.97, 1.55) | 0.120 |
| Model 2 | 0.87 (0.69, 1.10) | 0.251 | 1.09 (1.00, 1.20) | 0.060 | - | - |
| Model 3 | 0.87 (0.69, 1.10) | 0.248 | 1.09 (0.99, 1.20) | 0.067 | 1.21 (0.96, 1.53) | 0.114 |
| Central obesity | ||||||
| Model 1 | 0.99 (0.79, 1.25) | 0.953 | 1.04 (0.94, 1.15) | 0.478 | 1.13 (0.88, 1.44) | 0.337 |
| Model 2 | 0.97 (0.76, 1.23) | 0.794 | 1.04 (0.94, 1.16) | 0.451 | - | - |
| Model 3 | 0.97 (0.76, 1.23) | 0.807 | 1.04 (0.94, 1.15) | 0.475 | 1.12 (0.87, 1.43) | 0.369 |
| Hypertension | ||||||
| Model 1 | 0.91 (0.72, 1.16) | 0.453 | 1.12 (1.01, 1.25) | 0.036 | 1.43 (1.12, 1.84) | 0.005 |
| Model 2 | 0.84 (0.66, 1.07) | 0.161 | 1.15 (1.03, 1.28) | 0.016 | - | - |
| Model 3 | 0.84 (0.66, 1.07) | 0.166 | 1.14 (1.02, 1.28) | 0.018 | 1.42 (1.11, 1.83) | 0.006 |
| Dyslipidaemia | ||||||
| Model 1 | 0.80 (0.65, 1.00) | 0.051 | 1.05 (0.96, 1.15) | 0.292 | 1.26 (1.01, 1.58) | 0.039 |
| Model 2 | 0.77 (0.62, 0.96) | 0.023 | 1.08 (0.98, 1.18) | 0.112 | - | - |
| Model 3 | 0.77 (0.62, 0.96) | 0.023 | 1.07 (0.98, 1.18) | 0.123 | 1.25 (1.00, 1.57) | 0.048 |
| Prediabetes/Diabetes | ||||||
| Model 1 | 1.07 (0.85, 1.34) | 0.566 | 0.99 (0.90, 1.09) | 0.907 | 0.99 (0.78, 1.26) | 0.942 |
| Model 2 | 1.08 (0.85, 1.36) | 0.530 | 0.99 (0.89, 1.09) | 0.780 | - | - |
| Model 3 | 1.08 (0.85, 1.36) | 0.525 | 0.99 (0.89, 1.09) | 0.766 | 0.99 (0.78, 1.25) | 0.922 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baldock, K.L.; Paquet, C.; Howard, N.J.; Coffee, N.T.; Taylor, A.W.; Daniel, M. Are Perceived and Objective Distances to Fresh Food and Physical Activity Resources Associated with Cardiometabolic Risk? Int. J. Environ. Res. Public Health 2018, 15, 224. https://doi.org/10.3390/ijerph15020224
Baldock KL, Paquet C, Howard NJ, Coffee NT, Taylor AW, Daniel M. Are Perceived and Objective Distances to Fresh Food and Physical Activity Resources Associated with Cardiometabolic Risk? International Journal of Environmental Research and Public Health. 2018; 15(2):224. https://doi.org/10.3390/ijerph15020224
Chicago/Turabian StyleBaldock, Katherine L., Catherine Paquet, Natasha J. Howard, Neil T. Coffee, Anne W. Taylor, and Mark Daniel. 2018. "Are Perceived and Objective Distances to Fresh Food and Physical Activity Resources Associated with Cardiometabolic Risk?" International Journal of Environmental Research and Public Health 15, no. 2: 224. https://doi.org/10.3390/ijerph15020224