Evaluation of Regional Vulnerability to Disasters by People of Ishikawa, Japan: A Cross Sectional Study Using National Health Insurance Data

Abstract
:1. Background and Purpose of the Study
1.1. Current State of Disaster-Vulnerable Persons
1.2. Purpose of This Study
- (i).
- The National Health Insurance Database, which contains a massive amount of medical data (hereinafter, “National health insurance data”), was used to determine the number of disaster-vulnerable persons in neighborhood units. In addition, from among the chronic illnesses described in the previous section as urgent challenges in the Great East Japan Earthquake, the diseases analyzed in this study were those requiring dialysis, such as ischemic heart disease, cerebrovascular disease and chronic renal disease.
- (ii).
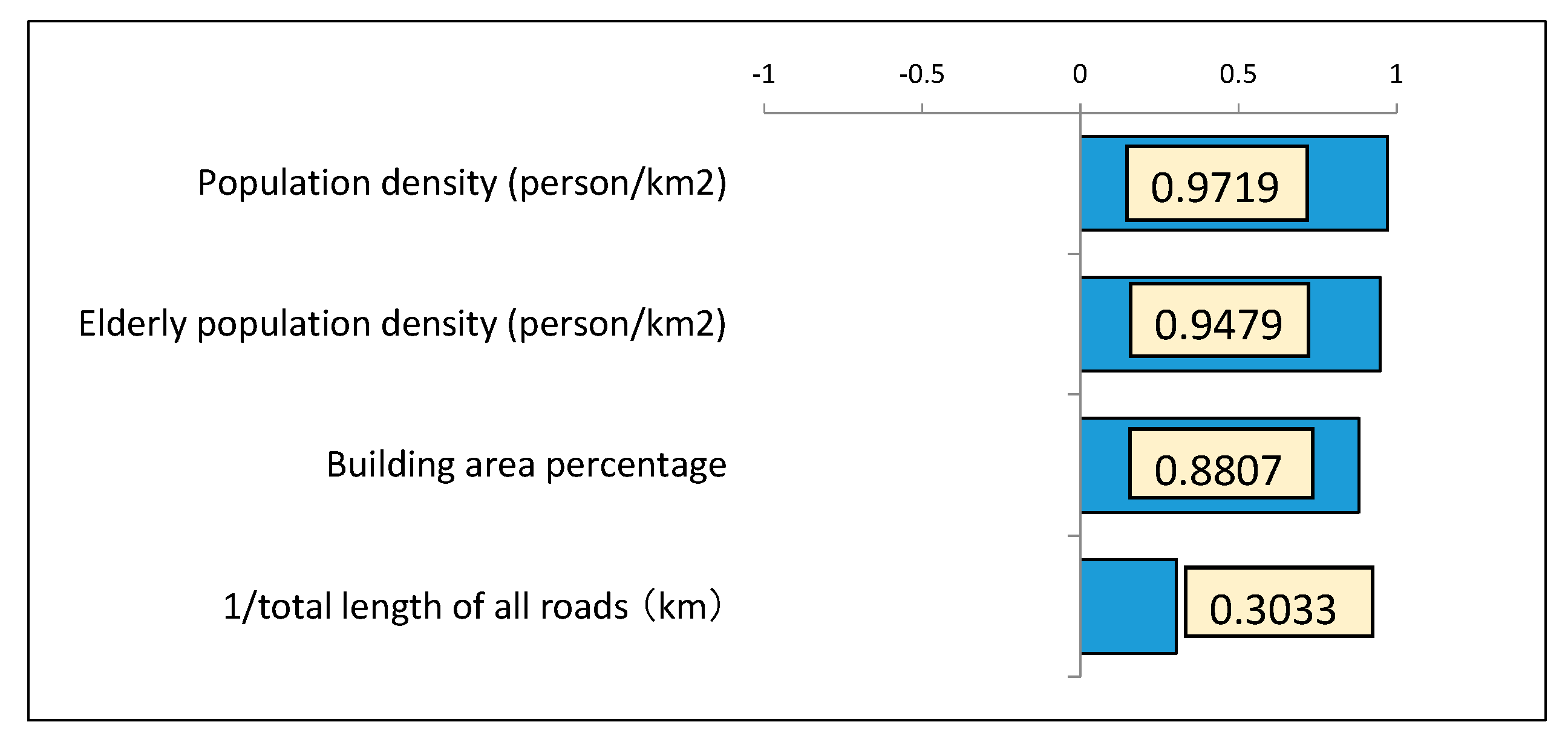
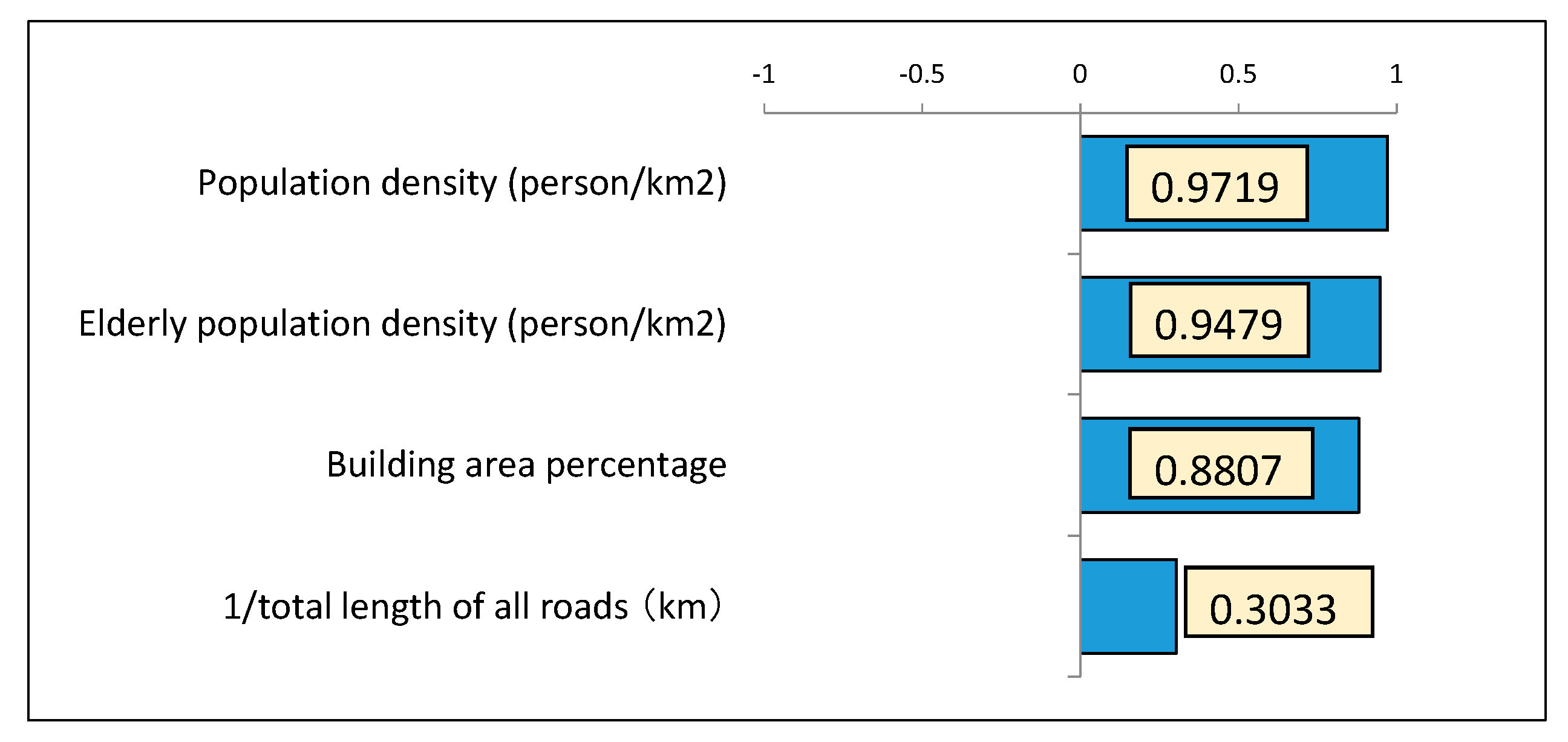
- With the units used to analyze the devastation severity set to neighborhood units, a quantitative analysis of the “external force” of the earthquake vibrations and the “vulnerability” of the neighborhood areas were quantitatively analyzed to evaluate the devastation. The “external force” of the earthquake vibrations was calculated using the value of the measured earthquake intensity from the earthquake vibration prediction map in the J-SHIS (Japan Seismic Hazard Information Station) earthquake hazard station that specified the earthquake source fault [4]. A neighborhood area’s “vulnerability” to earthquake damage was calculated using GIS and principal component analysis. The four surrogate variables during an earthquake disaster used when performing the principal component analysis were “population density (persons/km2)”, “elderly population density (persons/km2)”, “percentage of neighborhood area comprising building area”, and “the total length of roads in the neighborhood area (km)”.
- (iii).
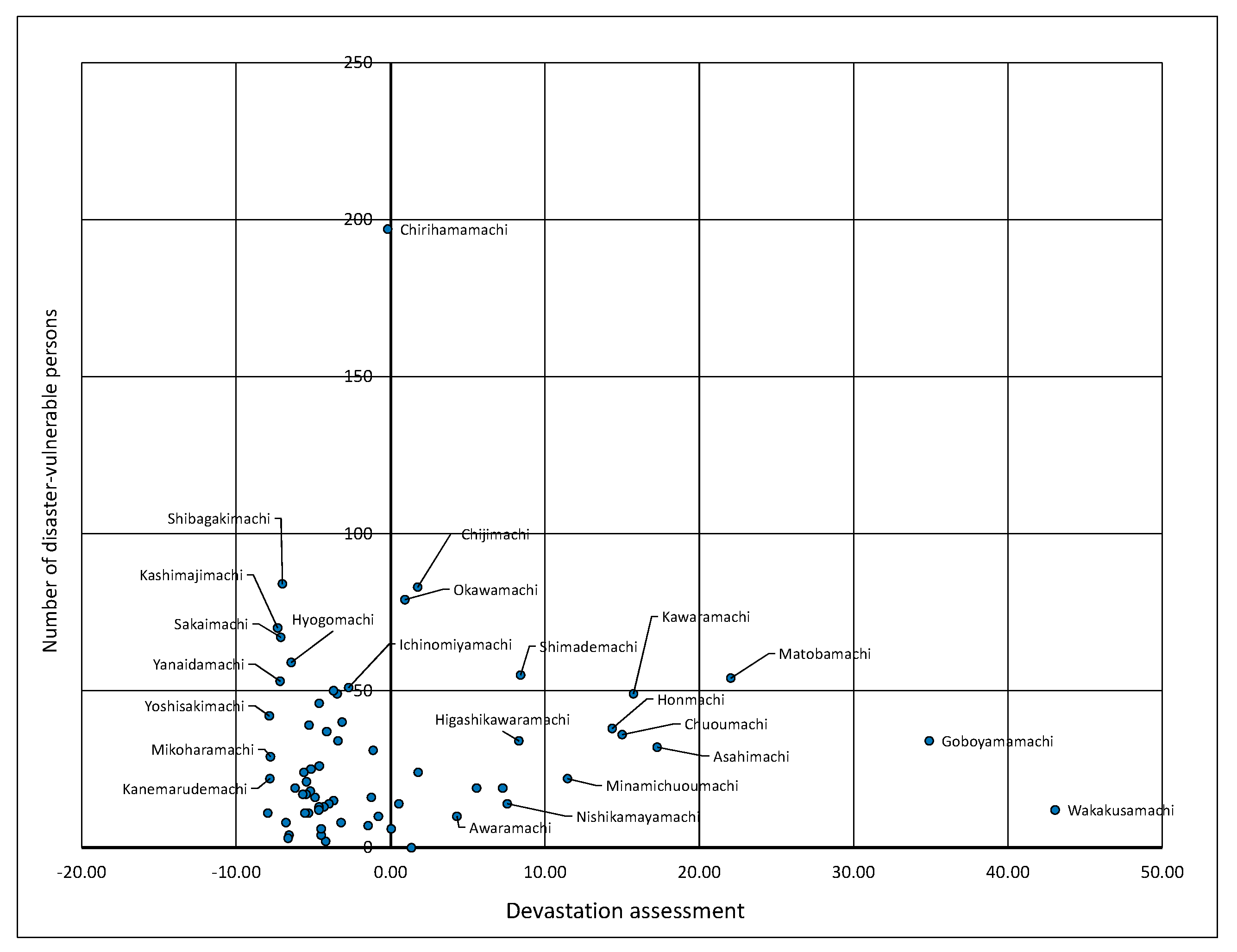
- From the results of (i), and (ii), it was possible to determine a detailed number of disaster-vulnerable persons living in the neighborhood region and the severity of the devastation by which they might be affected.
2. Previous Studies
2.1. Previous Studies on Disaster-Vulnerable Persons
2.2. Previous Studies of Disaster-Vulnerable Persons Using Massive Healthcare Data
2.3. Previous Studies on Evaluating Devastation in Natural Disasters
2.4. Actual State of Devastation Due to the East Japan Earthquake
2.5. Positioning of the Present Study Considering Previous Studies/Reports
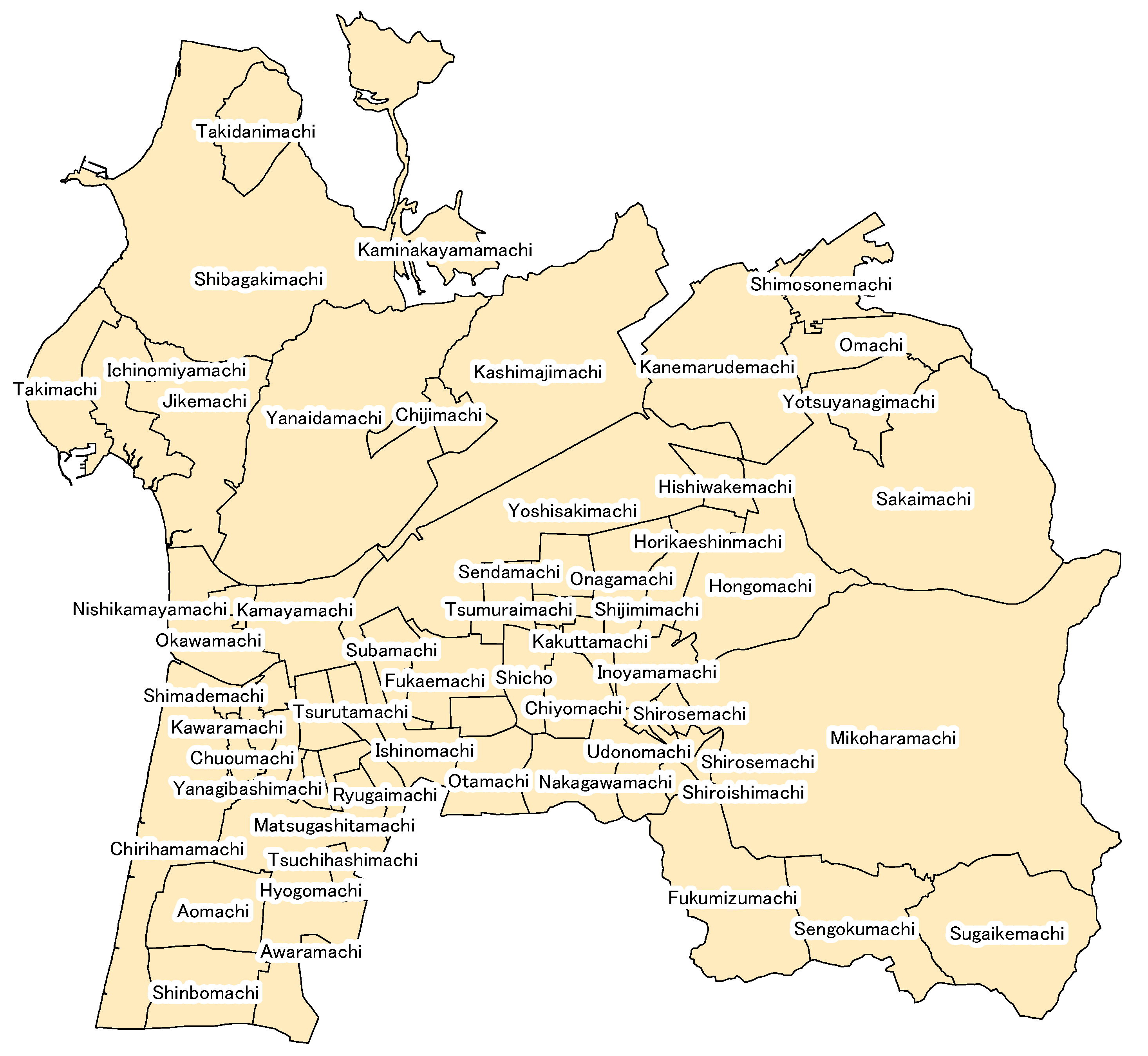
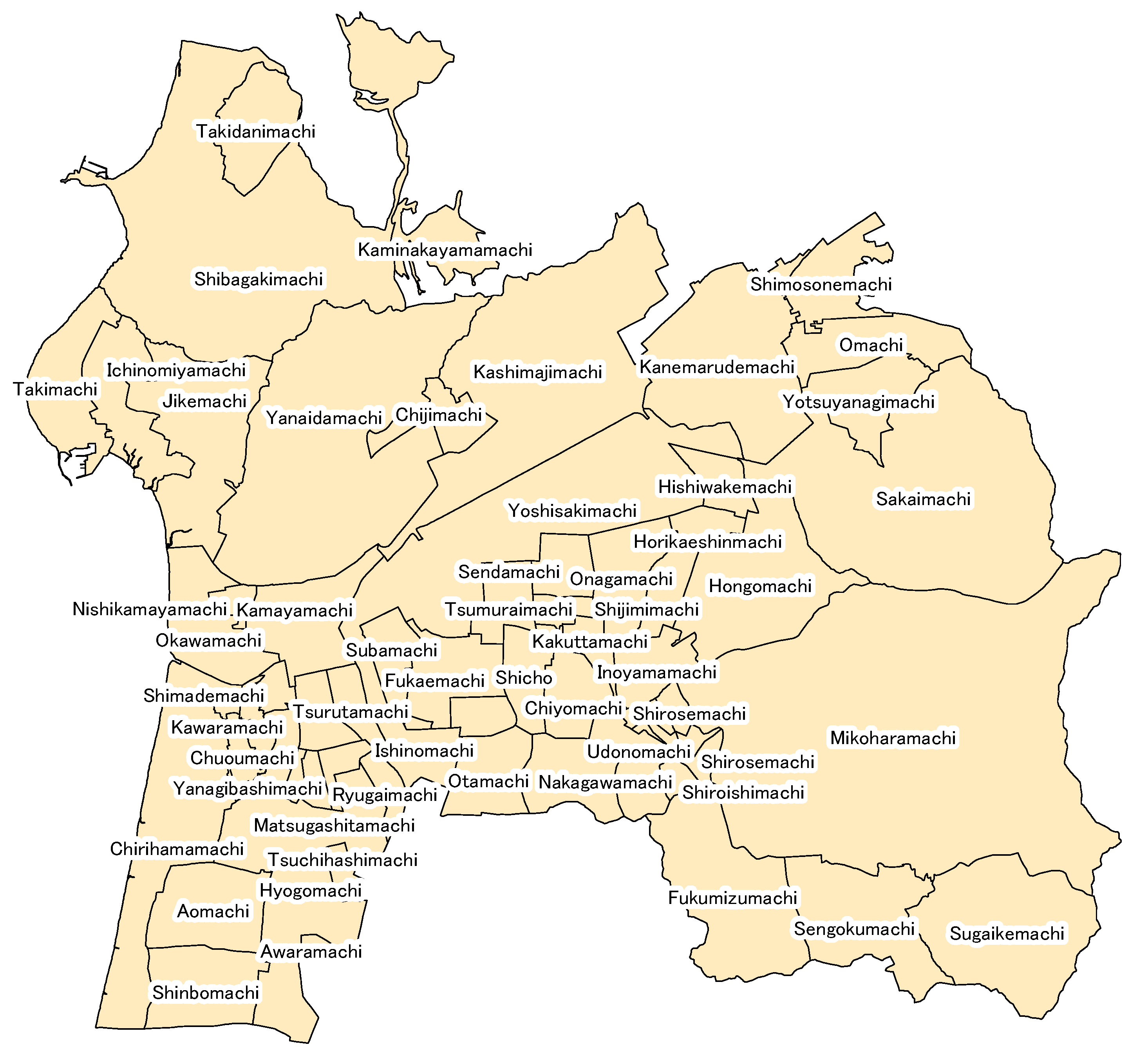
3. Analyzed Regions/Overview of Hakui City in Ishikawa Prefecture
4. Summary of National Health Insurance Data and Calculation of Disaster-Vulnerable Persons
4.1. Summary of National Health Insurance Data
4.2. Establishment of the Diseases to Be Analyzed and Calculation Results
5. Devastation Assessment Considering Regional Vulnerability
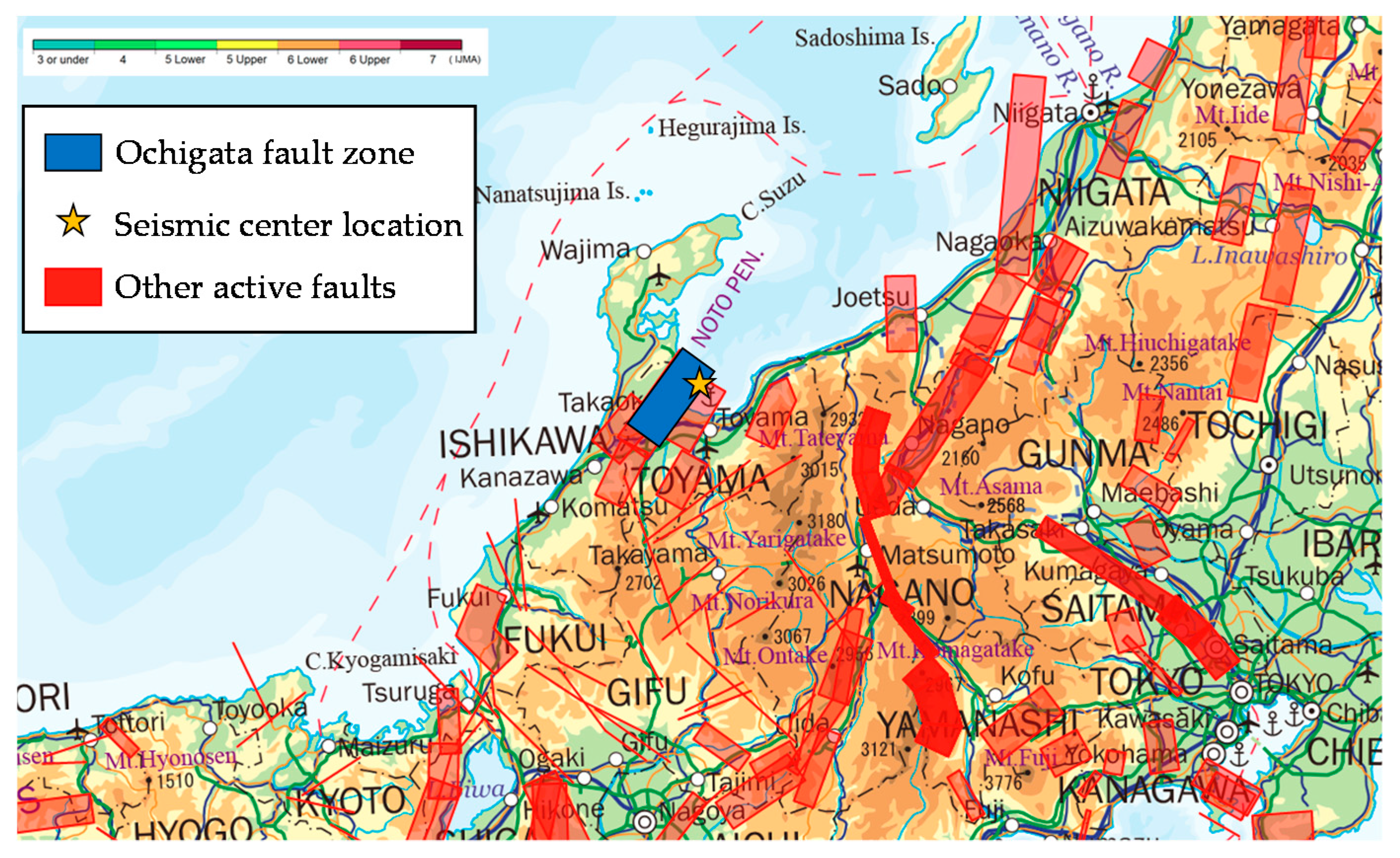
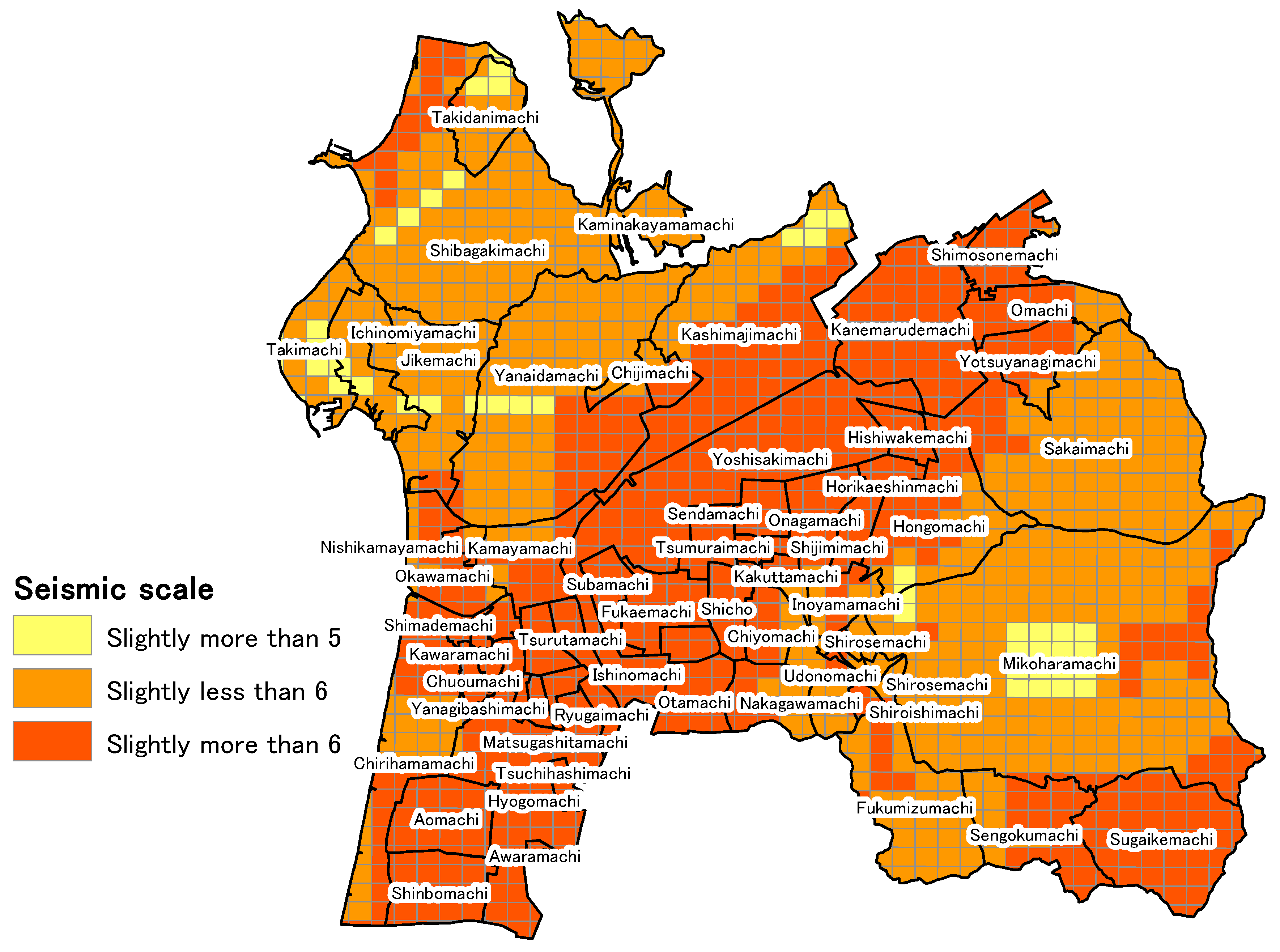
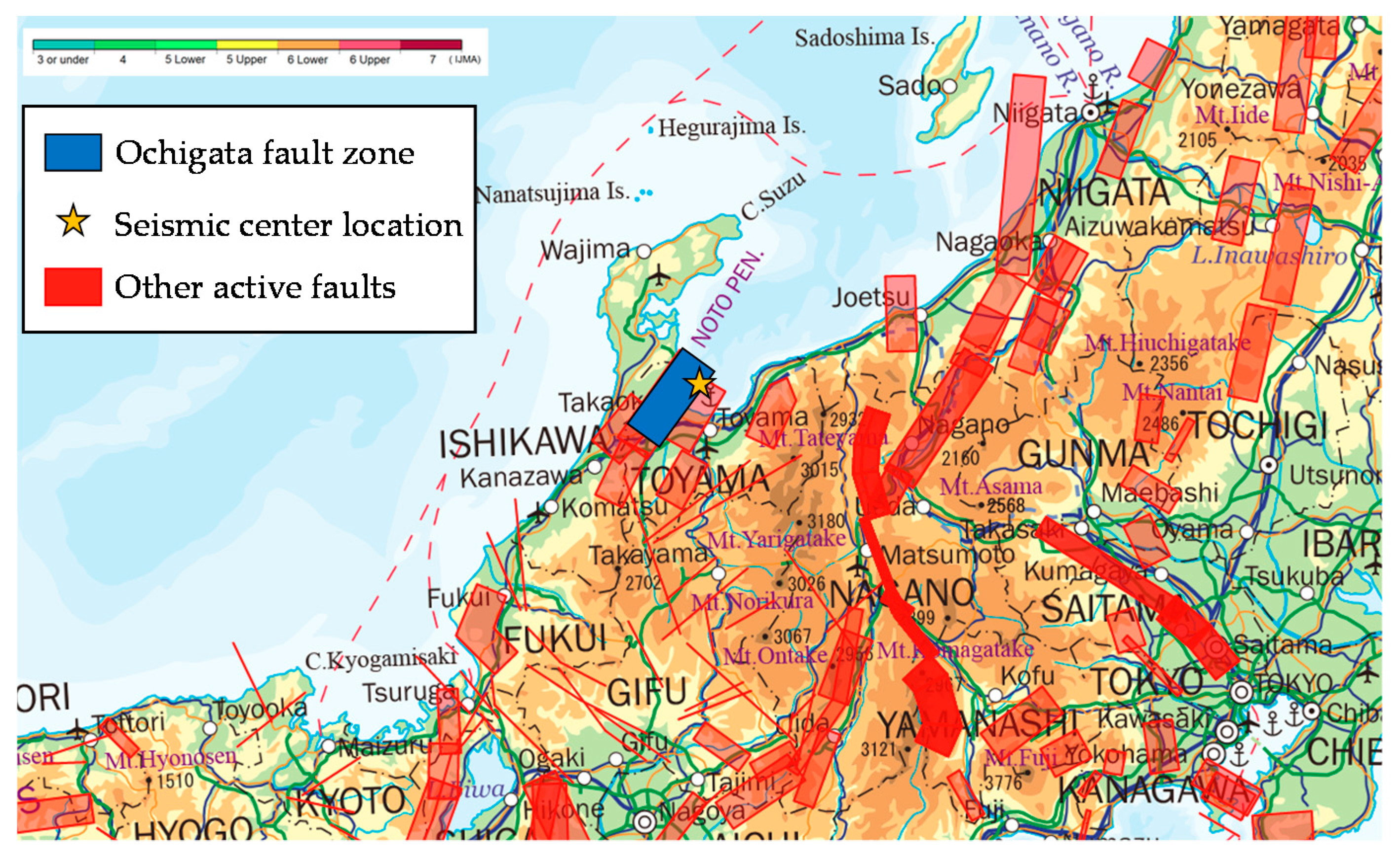
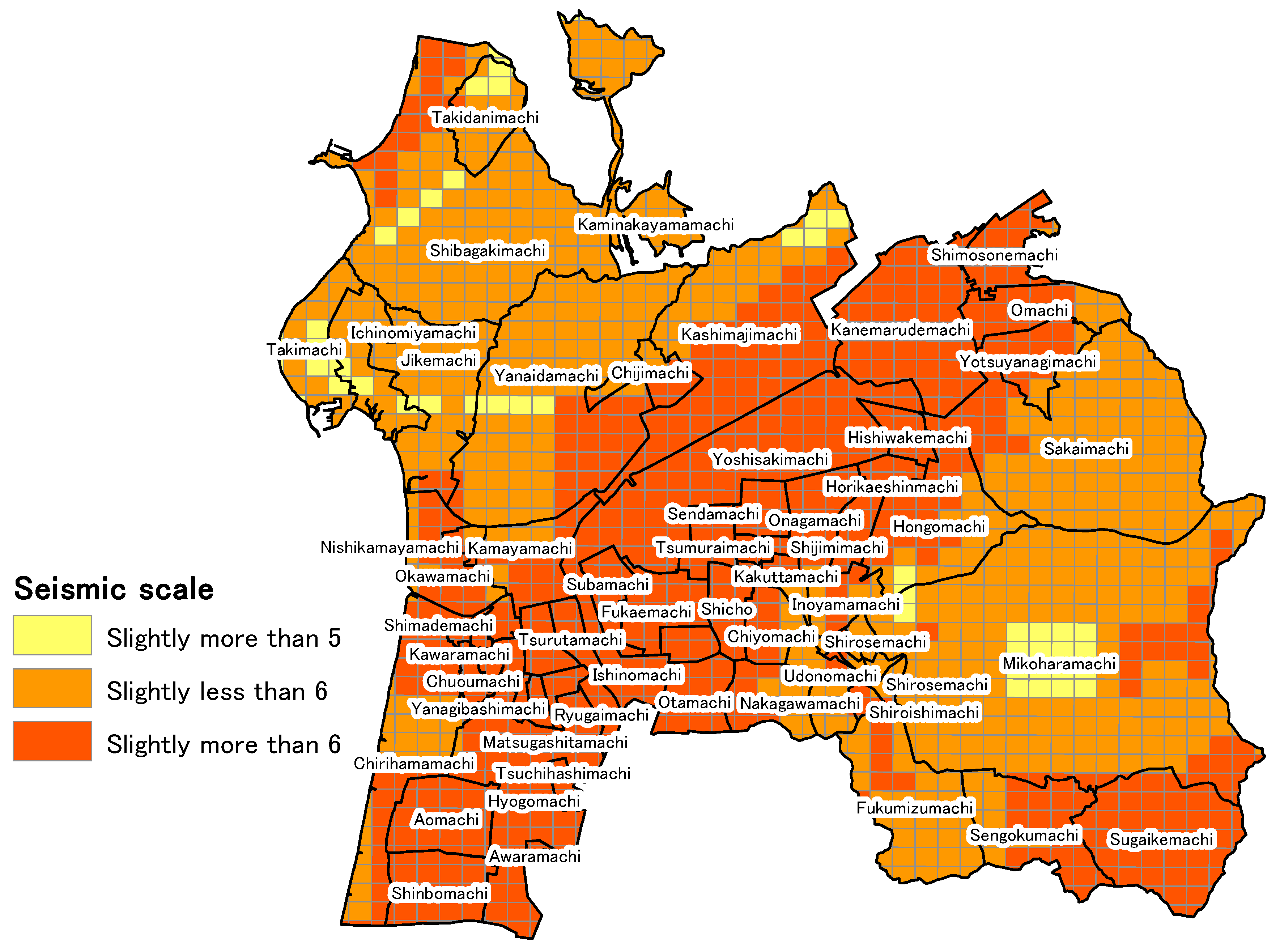
5.1. Calculation of the External Force of Earthquake Vibrations
5.2. Quantitative Evaluation of Earthquake “Vulnerability”
5.3. Quantitative Evaluation of Earthquake “Vulnerability” According to the Principal Component Analysis
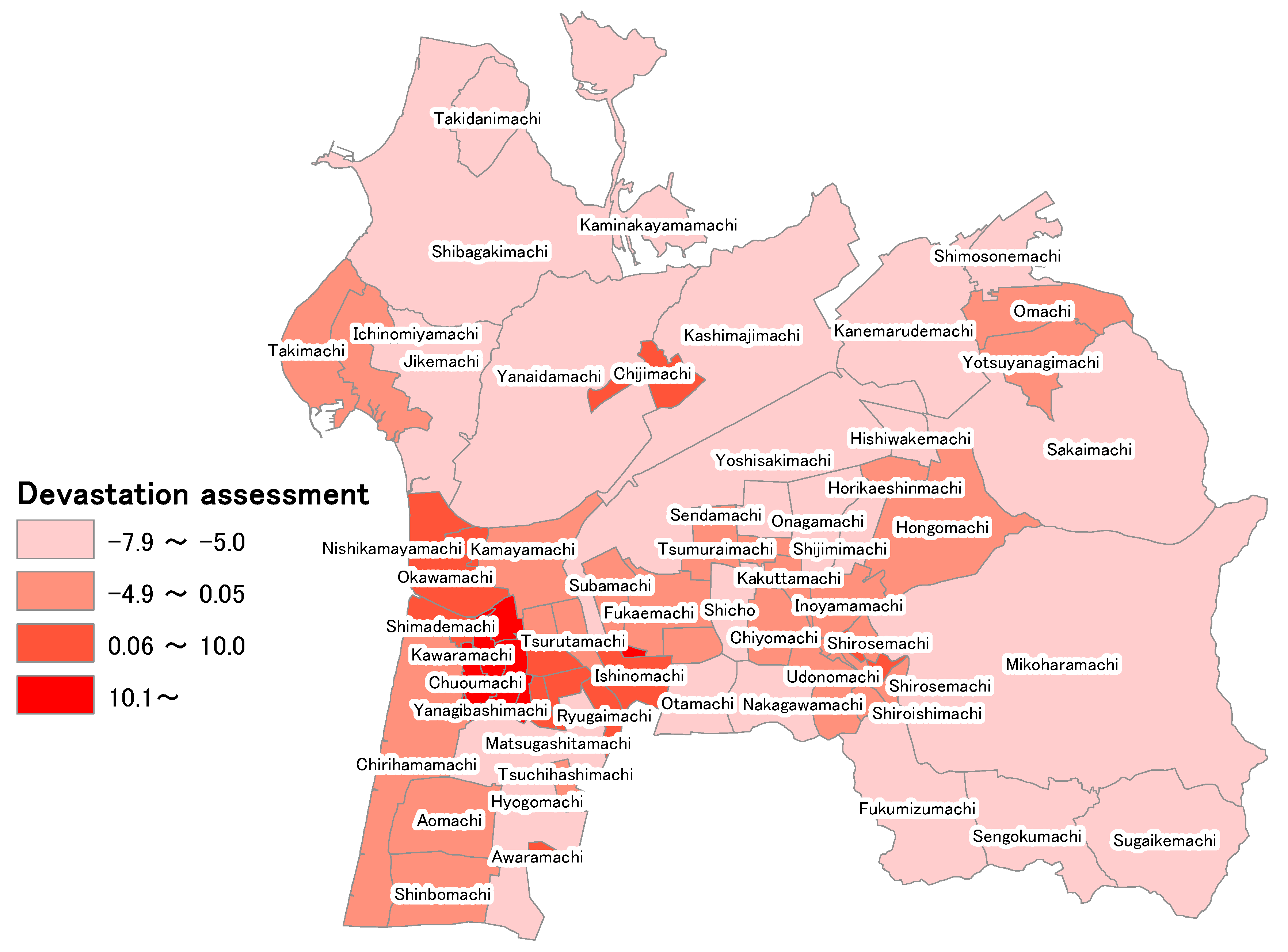
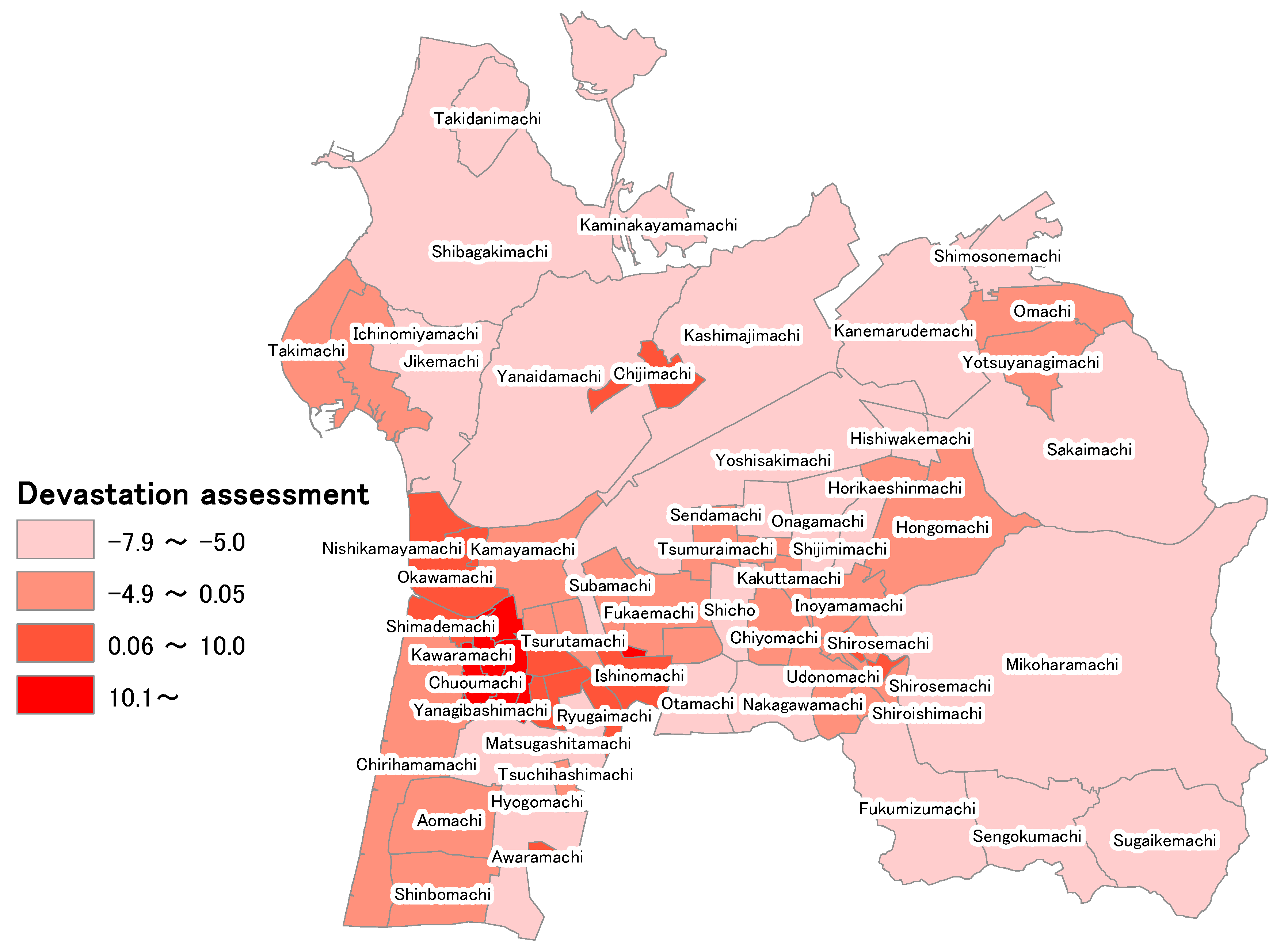
5.4. “Devastation Assessment” Calculated from External Force and Vulnerability
6. Future Topics
7. Conclusions
Author Contributions
Conflicts of Interest
References
- 2011 Disaster Prevention White Paper, Reference 6. Available online: http://www.bousai.go.jp/kaigirep/hakusho (accessed on 10 December 2017).
- National Diet Library Digital Collections: Medical Treatment and Nursing in Disaster Areas—Current State and Issues after the Great East Japan Earthquake. Available online: http://www.ndl.go.jp/jp/diet/publication/issue/pdf/0713.pdf (accessed on 10 December 2017).
- Disaster Countermeasures Basic Law. Available online: http://www.bousai.go.jp/taisaku/kihonhou/index.html (accessed on 10 December 2017).
- J-SHIS Earthquake Hazard Station. Available online: http://www.j-shis.bosai.go.jp (accessed on 10 December 2017).
- Nanba, Y.; Furukawa, Y. Study related to Determination of the Present State of Disaster-Vulnerable Persons and Evacuation During Disasters—A Case Study Targeting the Central Region of East Hiroshima City. Rep. Kinki Univ. Eng. 2006, 40, 41–46. [Google Scholar]
- Miki, S.; Hori, E.; Moriyama, S.; Hasemi, Y. Study of Tsunami Evacuation Behavior of Area Residents in the Great East Japan Earthquake, Report Collection of the Architectural Institute of Japan in Tohoku. Struct. Syst. 2016, 79, 149–152. [Google Scholar]
- Ito, K.; Watanabe, A.; Hosoda, T.; Sugiyama, C. Analysis of the Present Physical and Mental State of Disaster-Vulnerable Persons in Model School Districts, Study of the Establishment and Capacity of Evacuation Facilities for Disaster-Vulnerable Persons in Cities A and B (Part 1). Summ. Tech. Pap. Annu. Meet. Arch. Inst. Jpn. 2005, E-1, 299–300. [Google Scholar]
- Sugiyama, C.; Watanabe, A.; Hosoda, T.; Ito, K. Estimate of the Number of Disaster-Vulnerable Persons in Model School Districts by Evacuation Facility, Study of the Establishment and Capacity of Evacuation Facilities for Disaster-Vulnerable Persons in Cities A and B (Part 2). Summ. Tech. Pap. Annu. Meet. Arch. Inst. Jpn. 2005, E-1, 301–302. [Google Scholar]
- Watanabe, A.; Hosoda, T.; Ito, K.; Sugiyama, C. Estimate of the Number of Disaster-Vulnerable Persons in Model School Districts by Evacuation Facility, Analysis of the Capacity of Evacuation Facilities for Disaster-Vulnerable Persons, Study of the Establishment and Capacity of Evacuation Facilities for Disaster-Vulnerable Persons in Cities A and B (Part 3). Summ. Tech. Pap. Annu. Meet. Arch. Inst. Jpn. 2005, E-1, 303–304. [Google Scholar]
- Tamamori, Y.; Fujiu, M.; Nakayama, S.; Takayama, J.; Nishino, T.; Sagae, M.; Yanagihara, K.; Hirako, K. Evacuation Simulation of Disaster-Vulnerable Persons During a Large-Scale Earthquake—Using the National Health Insurance Database. Rep. Collect. Jpn. Soc. Civil Eng. F6 (Saf. Probl.) Feature Issue 2016, 72, 157–164. [Google Scholar]
- Morisaki, Y.; Fujiu, M.; Takayama, J.; Nakayama, S.; Nishino, T.; Sagae, M.; Yanagihara, K.; Hirako, K. Discussion of Evacuation Facilities that Disaster-Vulnerable Persons with Serious Diseases Can Use in a Large-Scale Earthquake—Using the National Health Insurance Database of Hatoyama-machi. Rep. Collect. Jpn. Soc. Civ. Eng. 2017. under review. [Google Scholar]
- Ikenaga, T.; Ohara, M. Comprehensive Natural Disaster Risk Analysis Considering the Future Population Reduction. Mon. J. Inst. Ind. Sci. 2014, 66, 397–402. [Google Scholar]
- Sobu, S.; Fujimura, S. Disaster Prevention Countermeasures for Patients with Refractory Diseases from the Perspective of Actual Devastation in the Great East Japan Earthquake. J. Fac. Nurs. Iwate Prefect. Univ. 2013, 15, 37–48. [Google Scholar]
- National Diet Library. Issue Brief Number 708; National Diet Library: Tokyo, Japan, 2011; p. 23. [Google Scholar]
- Hakui City 2015 Statistics. Available online: http://www.city.hakui.ishikawa.jp/sypher/www/service/detail.jsp?id=6952 (accessed on 13 December 2017).
- e-Stat National Census 2015. Available online: http://www.e-stat.go.jp/SG1/estat/GL08020101.do?_toGL08020101_&tstatCode=000001080615&requestSender=search (accessed on 14 December 2017).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Target Disease | Number of Patients |
|---|---|
| Patients diagnosed with ischemic heart disease | 1276 |
| Patients diagnosed with cerebrovascular disease | 1036 |
| Patients diagnosed as requiring dialysis | 56 |
| Patients with at least 1 of these 3 diseases | 1985 |
| Neighborhood Region | Population Density (persons/km2) | Elderly Population Density (persons/km2) | Building Area Percentage | 1/Total Length of All Roads (km) | First Principal Component Score | Mean Measured Seismic Intensity | Devastation Assessment | Number of Disaster Vulnerable Persons |
|---|---|---|---|---|---|---|---|---|
| Wakakusamachi | 4.35 | 3.53 | 4.21 | −0.68 | 7.14 | 6.03 | 43.06 | 12 |
| Goboyamamachi | 4.03 | 3.53 | 2.61 | −0.68 | 5.83 | 5.99 | 34.90 | 34 |
| Matobamachi | 1.88 | 3.19 | 1.46 | −0.64 | 3.69 | 5.98 | 22.05 | 54 |
| Asahimachi | 1.62 | 1.98 | 1.31 | −0.53 | 2.86 | 6.03 | 17.28 | 32 |
| Kawaramachi | 1.44 | 1.69 | 1.48 | −0.57 | 2.61 | 6.04 | 15.74 | 49 |
| Chuoumachi | 0.96 | 1.16 | 2.40 | −0.55 | 2.52 | 5.97 | 15.01 | 36 |
| Honmachi | 2.11 | 2.64 | −0.79 | −0.62 | 2.39 | 6.02 | 14.37 | 38 |
| Minamichuoumachi | 0.84 | 0.45 | 2.01 | −0.46 | 1.93 | 5.96 | 11.47 | 22 |
| Shimademachi | 1.10 | 1.23 | 0.21 | −0.51 | 1.42 | 5.94 | 8.43 | 55 |
| Higashikawaramachi | 0.97 | 0.92 | 0.59 | −0.57 | 1.38 | 6.05 | 8.32 | 34 |
| Nishikamayamachi | −0.04 | −0.08 | 2.33 | −0.41 | 1.28 | 5.91 | 7.57 | 14 |
| Kamishirosemachi | 0.17 | 0.12 | 0.01 | 0.90 | 1.25 | 5.81 | 7.28 | 19 |
| Matsugashitamachi | 0.79 | 0.41 | 0.36 | −0.55 | 0.93 | 5.99 | 5.58 | 19 |
| Awaramachi | 0.11 | 0.36 | 0.08 | −0.52 | 0.72 | 6.02 | 4.30 | 10 |
| Ishinomachi | 0.17 | −0.27 | 0.85 | −0.52 | 0.30 | 6.02 | 1.79 | 24 |
| Chijimachi | 0.19 | 0.37 | 0.16 | −0.53 | 0.31 | 5.74 | 1.77 | 83 |
| Yanagibashimachi | −0.35 | −0.49 | 1.17 | −0.35 | 0.23 | 6.01 | 1.36 | 0 |
| Okawamachi | 0.23 | 0.07 | 0.20 | −0.44 | 0.16 | 5.88 | 0.94 | 79 |
| Ryugaimachi | 0.54 | −0.27 | −0.09 | −0.53 | 0.09 | 5.99 | 0.55 | 14 |
| Tsurutamachi | −0.29 | −0.53 | 1.00 | −0.48 | 0.01 | 6.01 | 0.05 | 6 |
| Chirihamamachi | 0.17 | 0.13 | −0.12 | −0.41 | −0.03 | 5.88 | −0.18 | 197 |
| Tsuchihashimachi | −0.20 | 0.00 | −0.08 | −0.53 | −0.13 | 6.01 | −0.78 | 10 |
| Inoyamamachi | −0.16 | −0.09 | −0.07 | 0.03 | −0.19 | 5.83 | −1.12 | 31 |
| Horikaeshinmachi | −0.38 | −0.29 | 0.22 | −0.28 | −0.20 | 6.23 | −1.24 | 16 |
| Higashimatobamachi | −0.10 | −0.34 | −0.03 | −0.52 | −0.24 | 6.03 | −1.45 | 7 |
| Ichinomiyamachi | −0.30 | −0.31 | −0.03 | −0.36 | −0.49 | 5.54 | −2.71 | 51 |
| Shinbomachi | −0.32 | −0.37 | −0.06 | −0.19 | −0.53 | 5.95 | −3.13 | 40 |
| Kakuttamachi | −0.54 | −0.54 | −0.47 | 0.44 | −0.54 | 5.88 | −3.19 | 8 |
| Yotsuyanagimachi | −0.34 | −0.36 | −0.19 | −0.02 | −0.58 | 5.88 | −3.39 | 34 |
| Omachi | −0.34 | −0.31 | −0.17 | −0.37 | −0.58 | 5.93 | −3.45 | 49 |
| Takimachi | −0.32 | −0.23 | −0.43 | −0.42 | −0.68 | 5.44 | −3.68 | 50 |
| Shirosemachi | −0.53 | −0.45 | −0.42 | 0.34 | −0.64 | 5.80 | −3.69 | 15 |
| Chiyomachi | −0.39 | −0.45 | −0.21 | −0.32 | −0.67 | 5.95 | −3.98 | 14 |
| Aomachi | −0.41 | −0.46 | −0.13 | −0.28 | −0.69 | 6.01 | −4.13 | 37 |
| Shiroishimachi | −0.56 | −0.54 | −0.73 | −0.07 | −0.71 | 5.88 | −4.19 | 2 |
| Tsumuraimachi | −0.35 | −0.31 | −0.47 | −0.46 | −0.72 | 6.00 | −4.31 | 13 |
| Uwaemachi | −0.40 | −0.44 | −0.54 | −0.47 | −0.74 | 6.04 | −4.49 | 4 |
| Mitsuyamachi | −0.42 | −0.44 | −0.60 | −0.17 | −0.75 | 6.02 | −4.49 | 6 |
| Kamayamachi | −0.45 | −0.49 | −0.21 | −0.32 | −0.77 | 5.95 | −4.60 | 26 |
| Hongomachi | −0.47 | −0.35 | −0.44 | 1.27 | −0.78 | 5.92 | −4.61 | 46 |
| Udonomachi | −0.57 | −0.51 | −0.64 | 1.09 | −0.80 | 5.76 | −4.63 | 13 |
| Subamachi | −0.30 | −0.38 | −0.53 | −0.52 | −0.78 | 5.97 | −4.64 | 12 |
| Fukaemachi | −0.42 | −0.52 | −0.33 | −0.27 | −0.82 | 5.97 | −4.88 | 16 |
| Shimosonemachi | −0.44 | −0.44 | −0.43 | −0.45 | −0.86 | 5.98 | −5.14 | 25 |
| Sendamachi | −0.46 | −0.37 | −0.56 | −0.41 | −0.85 | 6.11 | −5.19 | 18 |
| Jikemachi | −0.56 | −0.53 | −0.31 | −0.27 | −0.94 | 5.64 | −5.27 | 39 |
| Shijimimachi | −0.53 | −0.51 | −0.69 | 0.36 | −0.85 | 6.21 | −5.31 | 11 |
| Shicho | −0.43 | −0.41 | −0.63 | −0.40 | −0.91 | 5.98 | −5.44 | 21 |
| Otamachi | −0.49 | −0.48 | −0.41 | −0.49 | −0.91 | 6.03 | −5.46 | 17 |
| Hishiwakemachi | −0.52 | −0.45 | −0.74 | 0.01 | −0.89 | 6.20 | −5.54 | 11 |
| Onagamachi | −0.51 | −0.48 | −0.54 | 0.08 | −0.91 | 6.15 | −5.60 | 24 |
| Takidanimachi | −0.58 | −0.51 | −0.57 | −0.05 | −1.01 | 5.59 | −5.68 | 17 |
| Nakagawamachi | −0.53 | −0.49 | −0.68 | −0.29 | −1.06 | 5.84 | −6.18 | 19 |
| Hyogomachi | −0.52 | −0.53 | −0.58 | −0.44 | −1.07 | 5.99 | −6.43 | 59 |
| Sengokumachi | −0.69 | −0.65 | −0.83 | 3.62 | −1.11 | 5.91 | −6.56 | 4 |
| Kaminakayamamachi | −0.67 | −0.63 | −0.81 | 0.27 | −1.16 | 5.70 | −6.63 | 3 |
| Fukumizumachi | −0.67 | −0.62 | −0.77 | 2.34 | −1.18 | 5.75 | −6.76 | 8 |
| Shibagakimachi | −0.63 | −0.59 | −0.74 | 0.38 | −1.25 | 5.62 | −7.00 | 84 |
| Sakaimachi | −0.64 | −0.60 | −0.78 | 1.99 | −1.25 | 5.67 | −7.10 | 67 |
| Yanaidamachi | −0.63 | −0.59 | −0.71 | −0.27 | −1.25 | 5.71 | −7.14 | 53 |
| Kashimajimachi | −0.61 | −0.56 | −0.78 | −0.10 | −1.25 | 5.84 | −7.31 | 70 |
| Mikoharamachi | −0.69 | −0.66 | −0.88 | 5.02 | −1.37 | 5.68 | −7.78 | 29 |
| Kanemarudemachi | −0.63 | −0.59 | −0.79 | −0.33 | −1.28 | 6.09 | −7.81 | 22 |
| Yoshisakimachi | −0.62 | −0.61 | −0.80 | −0.21 | −1.29 | 6.08 | −7.84 | 42 |
| Sugaikemachi | −0.69 | −0.65 | −0.89 | 1.64 | −1.32 | 6.03 | −7.94 | 11 |
| Average | 0.06 | 30.54 |
| Primary Component | Eigen Value | Contribution Ration | Cumulative Contribution Ratio |
|---|---|---|---|
| 1 | 2.711 | 67.77% | 67.77% |
| 2 | 0.941 | 23.53% | 91.30% |
| 3 | 0.317 | 7.92% | 99.22% |
| 4 | 0.031 | 0.78% | 100.00% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujiu, M.; Morisaki, Y.; Takayama, J.; Yanagihara, K.; Nishino, T.; Sagae, M.; Hirako, K. Evaluation of Regional Vulnerability to Disasters by People of Ishikawa, Japan: A Cross Sectional Study Using National Health Insurance Data. Int. J. Environ. Res. Public Health 2018, 15, 507. https://doi.org/10.3390/ijerph15030507
Fujiu M, Morisaki Y, Takayama J, Yanagihara K, Nishino T, Sagae M, Hirako K. Evaluation of Regional Vulnerability to Disasters by People of Ishikawa, Japan: A Cross Sectional Study Using National Health Insurance Data. International Journal of Environmental Research and Public Health. 2018; 15(3):507. https://doi.org/10.3390/ijerph15030507
Chicago/Turabian StyleFujiu, Makoto, Yuma Morisaki, Junichi Takayama, Kiyoko Yanagihara, Tatsuya Nishino, Masahiko Sagae, and Kohei Hirako. 2018. "Evaluation of Regional Vulnerability to Disasters by People of Ishikawa, Japan: A Cross Sectional Study Using National Health Insurance Data" International Journal of Environmental Research and Public Health 15, no. 3: 507. https://doi.org/10.3390/ijerph15030507