Commonalities between Disaster and Climate Change Risks for Health: A Theoretical Framework


Abstract
:1. Introduction
2. Defining Common Concepts in Disaster and Climate Change Risks to Health
3. Direct Health Impact Pathways
4. Indirect Health Impact Pathways
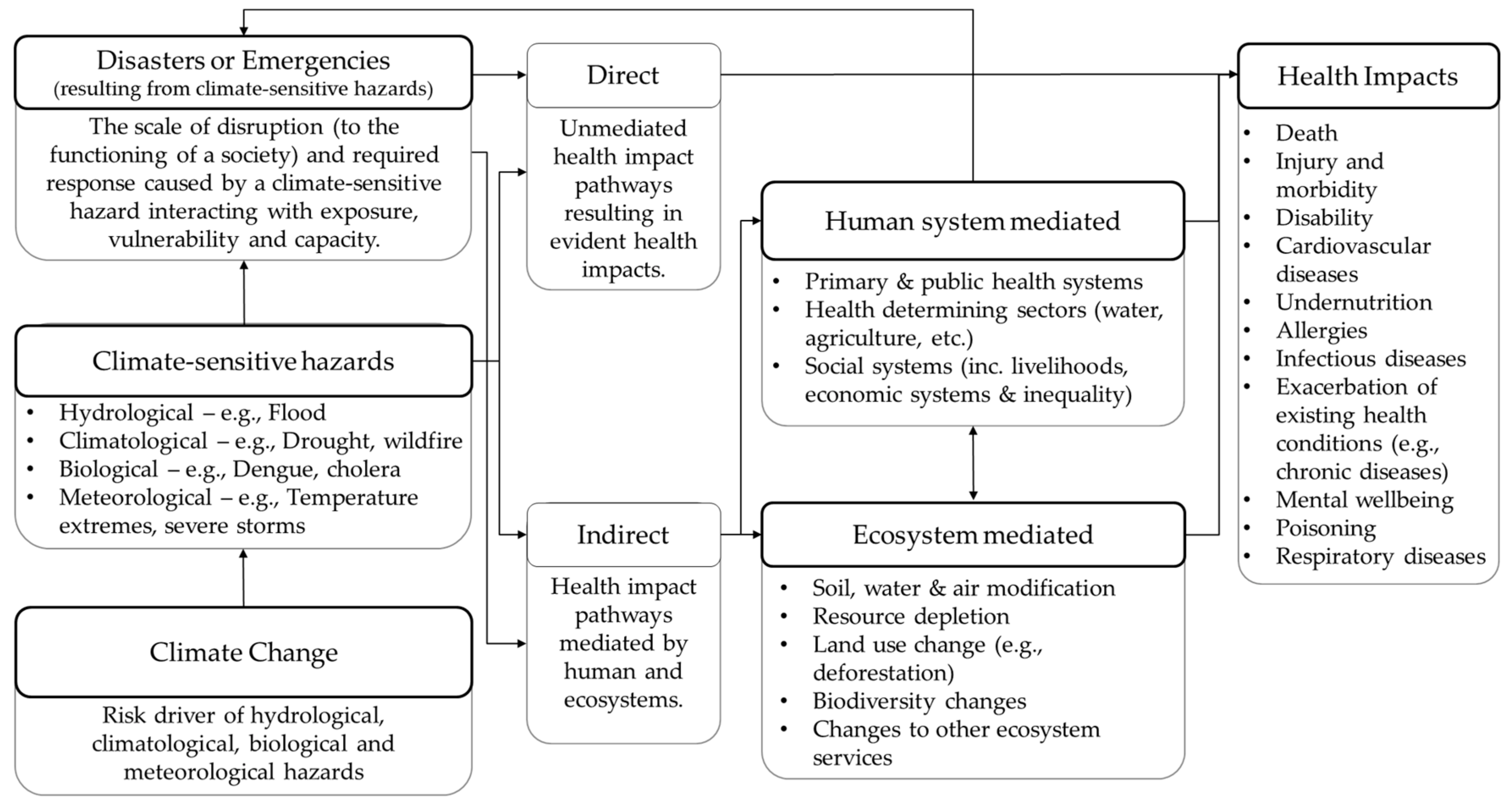
5. Framework for Understanding Commonalities in Health Risks of Climate Change and Climate-Sensitive Disasters
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Aitsi-Selmi, A.; Murray, V. Protecting the health and well-being of populations from disasters: Health and health care in the Sendai framework for disaster risk reduction 2015–2030. Prehosp. Disaster Med. 2016, 31, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Murray, V.; Aitsi-Selmi, A.; Blanchard, K. The role of public health within the United Nations post-2015 framework for disaster risk reduction. Int. J. Disaster Risk Sci. 2015, 6, 28–37. [Google Scholar] [CrossRef]
- United Nations International Strategy for Disaster Risk Reduction (UNISDR). Fact Sheet: Health in the Context of the Sendai Framework for Disaster Risk Reduction; United Nations International Strategy for Disaster Risk Reduction: Geneva, Switzerland, 2016. [Google Scholar]
- Maini, R.; Clarke, L.; Blanchard, K.; Murray, V. The Sendai Framework for Disaster Risk Reduction and its indicators—Where does health fit in? Int. J. Disaster Risk Sci. 2017, 8, 150–155. [Google Scholar] [CrossRef]
- Climate and Development Knowledge Network. Managing Climate Extremes and Disasters in the Health Sector: Lessons from the IPCC Srex Report; Climate and Development Knowledge Network: London, UK, 2012. [Google Scholar]
- Watts, N.; Amann, M.; Ayeb-Karlsson, S.; Belesova, K.; Bouley, T.; Boykoff, M.; Byass, P.; Cai, W.; Campbell-Lendrum, D.; Chambers, J. The Lancet Countdown on health and climate change: From 25 years of inaction to a global transformation for public health. Lancet 2018, 391, 581–630. [Google Scholar] [CrossRef]
- Vogel, L. Climate change is already making us sick. Can. Med. Assoc. 2017, 189, E1428–E1429. [Google Scholar] [CrossRef] [PubMed]
- Centre for Research on the Epidemiology of Disasters. Annual Disaster Statistical Review 2016—The Numbers and Trends; Centre for Research on the Epidemiology of Disasters: Brussels, Belgium, 2017. [Google Scholar]
- Keim, M.E.; Abrahams, J. Health and disaster. In Handbook of Hazards and Disaster Risk Reduction; Wisner, B., Gaillard, J.C., Kelman, I., Eds.; Routledge: Abingdon, UK, 2012. [Google Scholar]
- Chan, E.Y.Y. Public Health Humanitarian Responses to Natural Disasters; Routledge: Abingdon, UK, 2017. [Google Scholar]
- Keim, M.E. Building human resilience: The role of public health preparedness and response as an adaptation to climate change. Am. J. Prev. Med. 2008, 35, 508–516. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Health and Disaster Risk—A Contribution by the United Nations to the Consultation Leading to the Third UN World Conference on Disaster Risk Reduction; United Nations: New York, NY, USA, 2014. [Google Scholar]
- Phalkey, R.; Louis, V. Two hot to handle: How do we manage the simultaneous impacts of climate change and natural disasters on human health? Eur. Phys. J. Spec. Top. 2016, 225, 443–457. [Google Scholar] [CrossRef]
- Intergovernmental Panel on Climate Change (IPCC). Climate Change 2014: Impacts, Adaptation, and Vulnerability: Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; IPCC: Geneva, Switzerland, 2014; Volume 1. [Google Scholar]
- Ebi, K.L.; Hess, J.J. The past and future in understanding the health risks of and responses to climate variability and change. Int. J. Biometeorol. 2017, 1–10. [Google Scholar] [CrossRef] [PubMed]
- McMichael, A.J. Globalization, climate change, and human health. N. Engl. J. Med. 2013, 368, 1335–1343. [Google Scholar] [CrossRef] [PubMed]
- Noji, E.K. Disasters: Introduction and state of the art. Epidemiol. Rev. 2005, 27, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Raich, M.; Adler, C.; Stühlinger, V.; Lorenzoni, N.; Duschek, S. Impacts of disasters on health system performance, security and health protection. Sustain. Dev. 2015, 168, 1111–1121. [Google Scholar]
- Morris, G.P.; Reis, S.; Beck, S.A.; Fleming, L.E.; Adger, W.N.; Benton, T.G.; Depledge, M.H. Scoping the proximal and distal dimensions of climate change on health and wellbeing. Environ. Health 2017, 16, 116. [Google Scholar] [CrossRef] [PubMed]
- Turner, L.R.; Alderman, K.; Connell, D.; Tong, S. Motivators and barriers to incorporating climate change-related health risks in environmental health impact assessment. Int. J. Environ. Res. Public Health 2013, 10, 1139–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shoaf, K.I.; Rottman, S.J. Public health impact of disasters. Aust. J. Emerg. Manag. 2000, 15, 58. [Google Scholar]
- Overseas Development Institute. A Comparative Overview of Resilience Measurement Frameworks: Analysing Indicators and Approaches; Overseas Development Institute: London, UK, 2017. [Google Scholar]
- McMichael, A.J. Planetary Overload: Global Environmental Change and the Health of the Human Species; Cambridge University Press: Cambridge, UK, 1993. [Google Scholar]
- McMichael, A.J.; Woodruff, R.E.; Hales, S. Climate change and human health: Present and future risks. Lancet 2006, 367, 859–869. [Google Scholar] [CrossRef]
- World Health Organization. Our Planet, Our Health: Report of the Who Commission on Health and Environment; World Health Organization: Geneva, Switzerland, 1992. [Google Scholar]
- IPCC. Managing the Risks of Extreme Events and Disasters to Advance Climate Change Adaptation. A Special Report of Working Groups I and II of the Intergovernmental Panel on Climate Change; Cambridge University Press: Cambridge, UK, 2012. [Google Scholar]
- Watts, N.; Adger, W.N.; Agnolucci, P.; Blackstock, J.; Byass, P.; Cai, W.; Chaytor, S.; Colbourn, T.; Collins, M.; Cooper, A.; et al. Health and climate change: Policy responses to protect public health. Lancet 2015, 386, 1861–1914. [Google Scholar] [CrossRef]
- Dar, O.; Buckley, E.J.; Rokadiya, S.; Huda, Q.; Abrahams, J. Integrating health into disaster risk reduction strategies: Key considerations for success. Am. J. Public Health 2014, 104, 1811–1816. [Google Scholar] [CrossRef] [PubMed]
- Haines, A.; Kovats, R.S.; Campbell-Lendrum, D.; Corvalan, C. Climate change and human health: Impacts, vulnerability and public health. Public Health 2006, 120, 585–596. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Strengthening Health Resilience to Climate Change: Technical Briefing for the World Heath Organization Conference on Health and Climate; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organization. Operational Framework for Building Climate Resilient Health Systems; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Aitsi-Selmi, A.; Egawa, S.; Sasaki, H.; Wannous, C.; Murray, V. The Sendai framework for disaster risk reduction: Renewing the global commitment to people’s resilience, health, and well-being. Int. J. Disaster Risk Sci. 2015, 6, 164–176. [Google Scholar] [CrossRef]
- Aitsi-Selmi, A.; Murray, V. The Sendai framework: Disaster risk reduction through a health lens. Bull. World Health Organ. 2015, 93, 362. [Google Scholar] [CrossRef] [PubMed]
- UNFCCC. Adoption of the Paris Agreement. In Proceedings of the Conference of the Parties, Twenty First Session, Paris, France, 30 November–11 December 2015. [Google Scholar]
- UNISDR. Sendai Framework for Disaster Risk Reduction: 2015–2030; UNISDR: Geneva, Switzerland, 2015. [Google Scholar]
- Dietzel, A. The Paris Agreement—Protecting the human right to health? Glob. Policy 2017. [Google Scholar] [CrossRef]
- United Nations General Assembly. Report of the Open-Ended Intergovernmental Expert Working Group on Indicators and Terminology Relating to Disaster Risk Reduction; United Nations General Assembly: New York, NY, USA, 2016. [Google Scholar]
- IPCC. Climate Change 2014: Synthesis Report. Contribution of Working Groups I, II and III to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; IPCC: Geneva, Switzerland, 2014; Volume 1, p. 151. [Google Scholar]
- UNISDR. Terminology on Disaster Risk Reduction; UNISDR: Geneva, Switzerland, 2009. [Google Scholar]
- Adger, W.N. Vulnerability. Glob. Environ. Chang. 2006, 16, 268–281. [Google Scholar] [CrossRef]
- Wisner, B.; Blaikie, P.; Cannon, T.; Davis, I. At Risk: Natural Hazards, People’s Vulnerability and Disasters, 2nd ed.; Routledge: London, UK, 2004. [Google Scholar]
- Alwang, J.; Siegel, P.B.; Jorgensen, S.L. Vulnerability: A View from Different Disciplines; Social Protection Discussion Paper Series; The World Bank: New York, NY, USA, 2001. [Google Scholar]
- McEntire, D.A. Triggering agents, vulnerabilities and disaster reduction: Towards a holistic paradigm. Disaster Prev. Manag. Int. J. 2001, 10, 189–196. [Google Scholar] [CrossRef]
- Scovronick, N.; Sera, F.; Acquaotta, F.; Garzena, D.; Fratianni, S.; Wright, C.Y.; Gasparrini, A. The association between ambient temperature and mortality in South Africa: A time-series analysis. Environ. Res. 2018, 161, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Peng, M.; Wang, L.; Yu, C. Association of diurnal temperature range with daily mortality in England and wales: A nationwide time-series study. Sci. Total Environ. 2018, 619, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Vardoulakis, S.; Dear, K.; Hajat, S.; Heaviside, C.; Eggen, B.; McMichael, A.J. Comparative assessment of the effects of climate change on heat-and cold-related mortality in the United Kingdom and Australia. Environ. Health Perspect. 2014, 122, 1285–1292. [Google Scholar] [CrossRef] [PubMed]
- Noji, E.K. The Public Health Consequences of Disasters; Oxford University Press: Oxford, UK, 1996. [Google Scholar]
- Waring, S.C.; Brown, B.J. The threat of communicable diseases following natural disasters: A public health response. Disaster Manag. Response 2005, 3, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Norris, F.H.; Friedman, M.J.; Watson, P.J.; Byrne, C.M.; Diaz, E.; Kaniasty, K. 60,000 disaster victims speak: Part I. An empirical review of the empirical literature, 1981–2001. Psychiatry 2002, 65, 207–239. [Google Scholar] [CrossRef] [PubMed]
- Goldmann, E.; Galea, S. Mental health consequences of disasters. Annu. Rev. Public Health 2014, 35, 169–183. [Google Scholar] [CrossRef] [PubMed]
- North, C.S.; Pfefferbaum, B. Mental health response to community disasters: A systematic review. JAMA 2013, 310, 507–518. [Google Scholar] [CrossRef] [PubMed]
- Yusa, A.; Berry, P.; J Cheng, J.; Ogden, N.; Bonsal, B.; Stewart, R.; Waldick, R. Climate change, drought and human health in Canada. Int. J. Environ. Res. Public Health 2015, 12, 8359–8412. [Google Scholar] [CrossRef] [PubMed]
- UNFCCC. Human Health and Adaptation: Understanding Climate Impacts on Health and Opportunities for Action; Synthesis Paper by the Secretariat; Advice; UNFCCC: Bonn, Germany, 2017; Volume 46, pp. 8–18. [Google Scholar]
- Phung, D.; Huang, C.; Rutherford, S.; Chu, C.; Wang, X.; Nguyen, M. Climate change, water quality, and water-related diseases in the mekong delta basin: A systematic review. Asia Pac. J. Public Health 2015, 27, 265–276. [Google Scholar] [CrossRef] [PubMed]
- Rose, J.B.; Epstein, P.R.; Lipp, E.K.; Sherman, B.H.; Bernard, S.M.; Patz, J.A. Climate variability and change in the united states: Potential impacts on water-and foodborne diseases caused by microbiologic agents. Environ. Health Perspect. 2001, 109, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, K.S.; LePrevost, C.E. Climate justice in rural southeastern United States: A review of climate change impacts and effects on human health. Int. J. Environ. Res. Public Health 2016, 13, 189. [Google Scholar] [CrossRef] [PubMed]
- Toloo, G.S.; FitzGerald, G.; Tong, S. Managing health risks of extreme weather events: Need for a systematic approach. Aust. N. Z. J. Public Health 2014, 38, 90–91. [Google Scholar] [CrossRef] [PubMed]
- Curtis, S.; Fair, A.; Wistow, J.; Val, D.V.; Oven, K. Impact of extreme weather events and climate change for health and social care systems. Environ. Health 2017, 16, 128. [Google Scholar] [CrossRef] [PubMed]
- Lechat, M.F. The epidemiology of disasters. Proc. R. Soc. Med. 1976, 69, 421–426. [Google Scholar] [PubMed]
- PAHO. Natural Disasters: Protecting the Public's Health; Pan American Health Organisation: Washington, DC, USA, 2000. [Google Scholar]
- Noji, E.K. Public health issues in disasters. Crit. Care Med. 2005, 33, S29–S33. [Google Scholar] [CrossRef] [PubMed]
- Paterson, J.; Berry, P.; Ebi, K.L.; Varangu, L. Health care facilities resilient to climate change impacts. Int. J. Environ. Res. Public Health 2014, 11, 13097–13116. [Google Scholar] [CrossRef] [PubMed]
- Ardalan, A.; Mowafi, H.; Homa Yousefi, K. Impacts of natural hazards on primary health care facilities of Iran: A 10-year retrospective survey. PLoS Curr. 2013, 5. [Google Scholar] [CrossRef] [PubMed]
- Sellers, S.; Ebi, K.L. Climate change and health under the shared socioeconomic pathway framework. Int. J. Environ. Res. Public Health 2017, 15, 3. [Google Scholar] [CrossRef] [PubMed]
- Filho, W.L.; Al-Amin, A.Q.; Nagy, G.J.; Azeiteiro, U.M.; Wiesböck, L.; Ayal, D.Y.; Morgan, E.A.; Mugabe, P.; Aparicio-Effen, M.; Fudjumdjum, H.; et al. A comparative analysis of climate-risk and extreme event-related impacts on well-being and health: Policy implications. J. Environ. Res. Public Health 2018, 15, 331. [Google Scholar] [CrossRef] [PubMed]
- Kelman, I.; Kelman, I. Linking disaster risk reduction, climate change, and the sustainable development goals. Disaster Prev. Manag. Int. J. 2017, 26, 254–258. [Google Scholar] [CrossRef]
- McMichael, A.J.; Lindgren, E. Climate change: Present and future risks to health, and necessary responses. J. Internal Med. 2011, 270, 401–413. [Google Scholar] [CrossRef] [PubMed]
- CRED. General Classification of Hazards. Available online: http://www.emdat.be/classification (accessed on 18 January 2018).
- Kovats, R.S.; Hajat, S. Heat stress and public health: A critical review. Annu. Rev. Public Health 2008, 29, 41–55. [Google Scholar] [CrossRef] [PubMed]
- Manguvo, A.; Mafuvadze, B. The impact of traditional and religious practices on the spread of Ebola in West Africa: Time for a strategic shift. Pan Afr. Med. J. 2015, 22 (Suppl. 1), 9. [Google Scholar]
- Tucker, C.J.; Wilson, J.M.; Mahoney, R.; Anyamba, A.; Linthicum, K.; Myers, M.F. Climatic and ecological context of the 1994–1996 Ebola outbreaks. Photogramm. Eng. Remote Sens. 2002, 68, 147–152. [Google Scholar]
- Alexander, K.A.; Sanderson, C.E.; Marathe, M.; Lewis, B.L.; Rivers, C.M.; Shaman, J.; Drake, J.M.; Lofgren, E.; Dato, V.M.; Eisenberg, M.C. What factors might have led to the emergence of Ebola in West Africa? PLoS Negl. Trop. Dis. 2015, 9, e0003652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinzon, J.E.; Wilson, J.M.; Tucker, C.J.; Arthur, R.; Jahrling, P.B.; Formenty, P. Trigger events: Enviroclimatic coupling of Ebola hemorrhagic fever outbreaks. Am. J. Trop. Med. Hyg. 2004, 71, 664–674. [Google Scholar] [PubMed]
- Talukder, M.R.R.; Rutherford, S.; Huang, C.; Phung, D.; Islam, M.Z.; Chu, C. Drinking water salinity and risk of hypertension: A systematic review and meta-analysis. Arch. Environ. Occup. Health 2017, 72, 126–138. [Google Scholar] [CrossRef] [PubMed]
- Vineis, P.; Chan, Q.; Khan, A. Climate change impacts on water salinity and health. J. Epidemiol. Glob. Health 2011, 1, 5–10. [Google Scholar] [CrossRef] [PubMed]
- United Nations. United Nations Framework Convention on Climate Change; United Nations: New York, NY, USA, 1992. [Google Scholar]


{kind=link}
| Disaster | Climate Change | Common Elements | |
|---|---|---|---|
| Term | The interaction of a hazard with exposure, vulnerability and capacity resulting in serious disruption, losses and impacts to a community [37]. | Changes in climate mean and/or variability that persist over long periods [38]. | |
| Risk | Potential interaction of hazard, exposure, vulnerability and capacity that present the possibility for losses or impacts on a population and elements of a society [37]. | The result of the interaction of vulnerability (including capacity), exposure and hazard [26,38]. | Interaction of vulnerability (including capacity), hazard and exposure. |
| Exposure | Elements of communities, infrastructure, organisations or systems that are located within the proximity of a hazard, thus potentially subject to damage and loss [37]. | Existence of elements of human and ecosystems in places and settings which could be adversely affected by climate change [38]. | Presence of system elements in locations which will be potentially impacted by hazards. |
| Hazard | An event (geophysical, hydrological, climatological, biological, meteorological, technological or human induced) that has the potential to cause losses to human and ecosystems [37]. | Natural or human-induced events that have the potential to occur in the future and impact exposed and vulnerable aspects of a system [26]. | Interaction of hazard with exposure and vulnerability. |
| Vulnerability | “Susceptibility of an individual, a community, assets or systems to the impacts of hazards” [37] (p. 24), caused by economic, social, physical and environmental factors [37,39,40,41,42,43]. | Potential to be adversely affected, including factors such as susceptibility, predisposition and capacity [26,38]. | Susceptibility to potential adverse effects. |
| Capacity | Ability of individuals, communities, organisations and systems to access and use the skills and resources to reduce or manage disaster risk [37,39]. | Individual, community, societal, or organizational strengths, attributes, and resources that enable responses to change [26,38]. | Use of resources and skills to address risks. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banwell, N.; Rutherford, S.; Mackey, B.; Street, R.; Chu, C. Commonalities between Disaster and Climate Change Risks for Health: A Theoretical Framework. Int. J. Environ. Res. Public Health 2018, 15, 538. https://doi.org/10.3390/ijerph15030538
Banwell N, Rutherford S, Mackey B, Street R, Chu C. Commonalities between Disaster and Climate Change Risks for Health: A Theoretical Framework. International Journal of Environmental Research and Public Health. 2018; 15(3):538. https://doi.org/10.3390/ijerph15030538
Chicago/Turabian StyleBanwell, Nicola, Shannon Rutherford, Brendan Mackey, Roger Street, and Cordia Chu. 2018. "Commonalities between Disaster and Climate Change Risks for Health: A Theoretical Framework" International Journal of Environmental Research and Public Health 15, no. 3: 538. https://doi.org/10.3390/ijerph15030538